Paeds · child-safety-and-social-paediatrics
Child maltreatment recognition and response
Also known as Child abuse recognition · Non-accidental injury assessment · Safeguarding recognition and response · Child protection recognition · Maltreatment recognition in paediatrics
Fellowship hub on recognising and responding to child maltreatment across all forms (physical, sexual, emotional, neglect, fabricated or induced illness): global epidemiology and the under-detection gap, the toxic-stress / adverse-childhood-experiences cascade and its buffering adult, presenting patterns and sentinel injuries, the TEN-4-FBCP bruising rule, mimics and differentials, the trauma-informed examination with a body map, the workup (skeletal survey, neuroimaging, ophthalmology, coagulation, STI screen), the parallel recognition-to-response bundle (stabilise, document, report, refer, safeguard), prevention of re-injury, and ANZ/UK/US/Canada guideline structure.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
T.E.N.-4-F.B.C.P. — the bruising rule that demands action
Overview & Definition
A six-week-old baby is brought to the emergency department with a single small bruise on the ear. The parents say it happened when the baby rolled against the cot bar. A registrar documents "minor bruise, likely accidental" and discharges the family. Three months later the baby is admitted with subdural haemorrhages, retinal bleeds and an unresponsive brain. That first ear bruise was a sentinel injury — the most preventable miss in all of paediatrics. Recognising and responding to child maltreatment is the discipline of turning that first bruise into a protected child. [8] [9]
Child maltreatment is any act of commission or omission, by a parent, caregiver or other adult in a relationship of responsibility, trust or power, that results in actual or potential harm to a child's health, survival, development or dignity. Two features make it hard to detect and demanding to manage: the harm usually occurs in private, behind a consistent family account, and the consequences unfold across the whole life course through a biological cascade that an examiner cannot see at the bedside. [1] [2]
The recognition-to-response stance is what this hub topic owns. You are asked to recognise the patterns across all five forms, build the differential that separates abuse from its mimics, examine in a trauma-informed way, order the right workup, and deliver the parallel bundle of stabilise, document, report and refer. This page does not rebuild the dedicated leaves — physical abuse and bruising, abusive head trauma, inflicted fractures, child sexual abuse assessment, neglect, fabricated or induced illness, mandatory reporting, trauma-informed examination, and prevention — it links to them and supplies the framework that holds them together. [2]
Classification
Sort the work by which form of maltreatment is in front of you, because each form has its own patterns, mimics, workup and reporting nuance, and because forms overlap — poly-victimisation is the rule, not the exception. [1] [2]
The five forms are the working taxonomy. Physical abuse is an act of commission causing physical harm — bruises, burns, fractures, abdominal or head injury. Sexual abuse is any sexual activity a child cannot consent to or comprehend, including grooming, contact and non-contact exploitation. Emotional or psychological abuse is a persistent pattern of behaviour that damages a child's emotional development — terrorising, humiliating, rejecting, isolating or corrupting. Neglect is the failure to provide for a child's basic physical, emotional, medical, educational or supervisory needs, and it is an act of omission. Caregiver-fabricated or induced illness is the falsification or induction of illness in a child to fulfil the caregiver's need, not the child's. [1] [10]
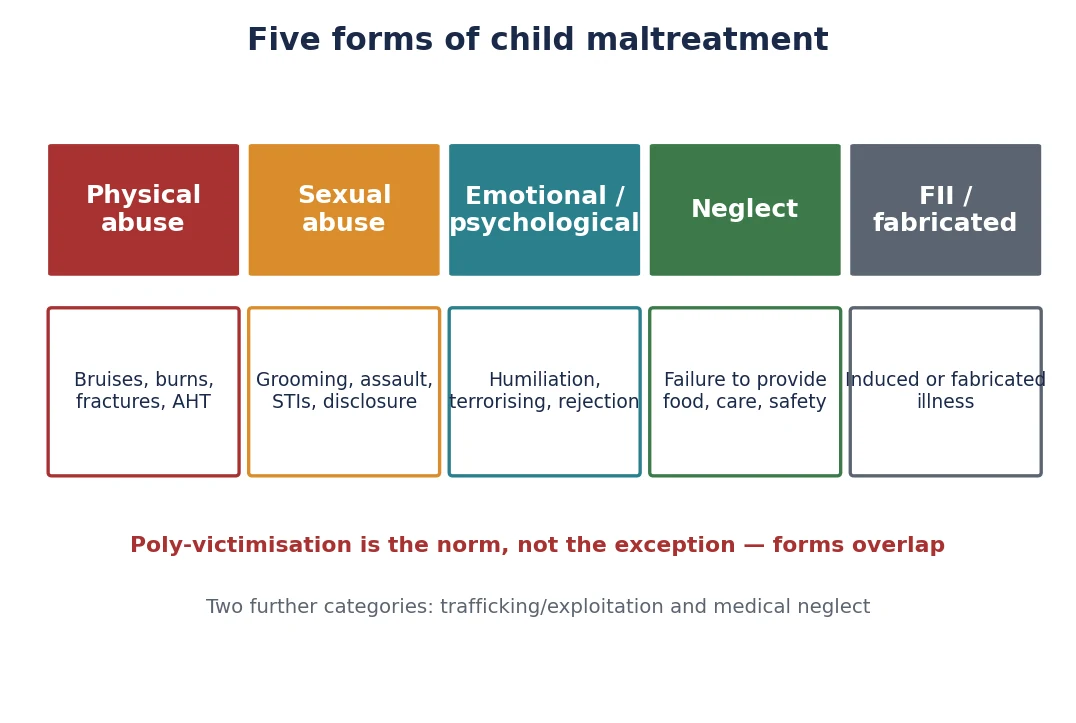
Two further categories are kept in view. Trafficking, exploitation and forced marriage sit alongside the five forms and present with unexplained absences, a controlling adult, and unexplained money or possessions. Medical neglect — the failure to secure necessary medical care for a child — is a specific and common presentation that overlaps with general neglect. Keeping both in mind stops the single-form frame from hiding the whole picture. [1] [2]
The deepest classification question is the one a clinician must answer at the bedside: is this injury abuse, an accident, a mimic, or a cultural practice? A bruise may be inflicted; it may be a Mongolian blue spot; it may be coining or cupping from a traditional remedy; it may be thrombocytopenic purpura. Getting the classification right at this first fork determines the whole downstream response, and it is the question the differential-diagnosis section is built to answer. [6] [2]
Epidemiology & Risk Factors
How common is child maltreatment? Two different answers come back depending on how you ask, and the gap between them is itself the central epidemiological fact. Official, agency-substantiated rates — the figures child-protection systems record — markedly under-estimate true prevalence, because most maltreatment is never reported or substantiated. Self-report surveys of adults recalling childhood show that maltreatment is several-fold more common than agency data suggest, which is why a clinician who waits for an "obvious" case will miss most of them. [1] [5]
Globally, the burden is large. A WHO/CDC systematic review estimated that roughly one billion children aged two to seventeen years experienced past-year violence, and self-report studies put the lifetime prevalence of contact childhood sexual abuse at roughly one in five women and one in thirteen men. High-income country data place physical abuse and neglect among the most common adverse exposures of childhood. [5] [1]
Risk clusters at three levels. Child factors include infancy and prematurity, chronic illness, disability and behaviour that challenges caregivers. Parent or family factors include intimate-partner violence, parental mental illness, parental substance use, social isolation, a caregiver's own history of childhood adversity, and young or single parenthood. Community factors include poverty, housing instability, neighbourhood violence and poor access to support. None of these factors is diagnostic — most families with risk factors never maltreat — but together they raise the index of suspicion and, more importantly, mark where preventive support should go. [1] [4]
The reason any of this matters for prognosis is that maltreatment is strongly associated with later disease and early death in a dose-response pattern: the more forms and the more adversity, the worse the adult outcome. That dose-response is the epidemiological bridge to the mechanism in the next section. [3] [4]
Pathophysiology
Why does maltreatment harm a child for life — and why can one stable adult change that trajectory? The answer is the biology of toxic stress, and it is the mechanism an examiner must hold in mind because it explains why an injury that looks minor can carry lifelong cost, and why intervention is urgent even when the child looks well. [3] [10]
A child's stress response is healthy when it is brief and buffered. When a threat passes and a responsive adult comforts the child, the cortisol and adrenergic surge of "positive" or "tolerable" stress settles and the brain records a safely mastered challenge. Maltreatment removes the buffer: the threat comes from within the caregiving relationship itself, so the stress response stays activated for weeks, months and years. That sustained activation is toxic stress, and it recalibrates the developing hypothalamic-pituitary-adrenal axis, dysregulates the immune system, and alters the architecture of the brain — especially the limbic and prefrontal circuits that govern emotion, attention and impulse. [3] [4]
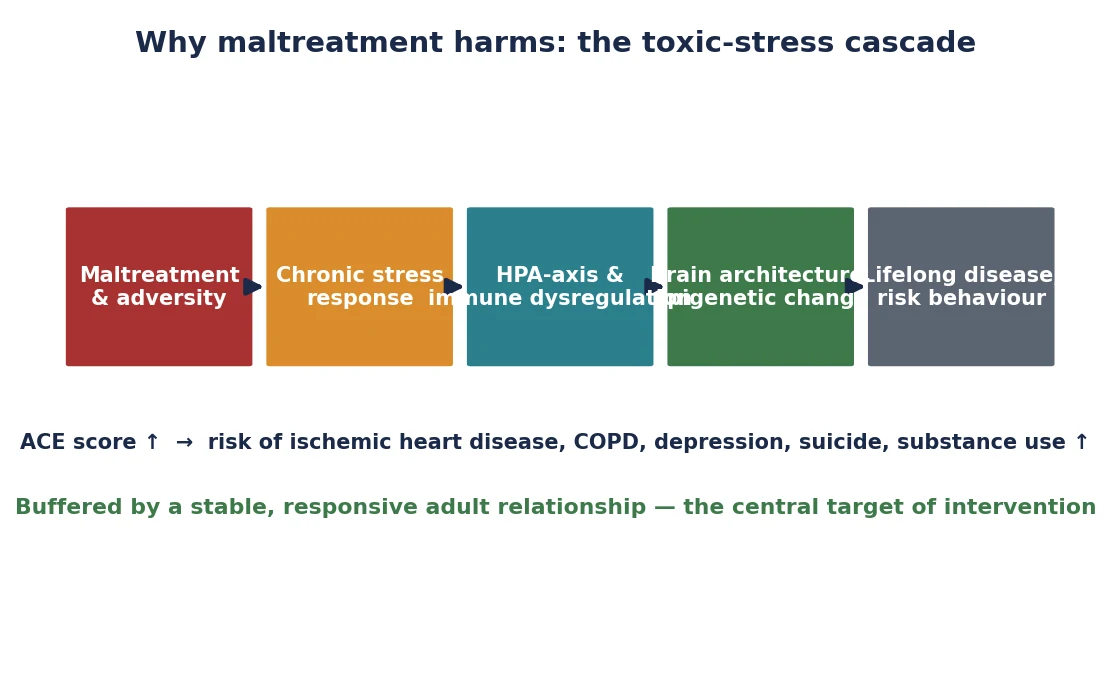
The same cascade produces the adult disease associations that make the ACE literature so consequential. A meta-analysis of the long-term health consequences of abuse and neglect found elevated risks of mental disorder, substance use, sexually transmitted infection, risky sexual behaviour, self-harm and physical disease; the Adverse Childhood Experiences study showed a graded relationship between the ACE score and the leading causes of adult death, including ischaemic heart disease. The mechanism is dose-response: more cumulative adversity, more downstream disease. [10] [3]
The single most important therapeutic implication is that a stable, responsive adult relationship is the buffer that converts toxic stress into tolerable stress. That is why the response to maltreatment is not only to stop the harm but to protect or rebuild that relationship — through placing the child with a safe caregiver, supporting a non-offending parent, and arranging trauma-focused therapy. Mechanism and management meet here: the biology of harm is also the biology of recovery. [3] [4]
For the acute forms, the mechanism is mechanical. Abusive head trauma injures the infant brain through violent acceleration-deceleration and rotational shear, generating subdural haemorrhage, retinal haemorrhage and diffuse axonal injury. Inflicted fractures and burns follow non-accidental impact and thermal-gradient patterns. Neglect produces failure to thrive through simple caloric deficit. Knowing the mechanism lets you judge whether a stated history is physiologically plausible — and most implausible histories fail this test. [12] [11]
Clinical Presentation
What you will see depends on the form, but a small number of patterns account for most presentations, and recognising them is the examiner's first task. The cardinal rule is that a history that does not fit the injury — in pattern, age or developmental stage — is itself a finding, and a sentinel injury in a non-mobile infant is never "normal". [2] [8]
Physical abuse presents with bruises in non-mobile infants, patterned or staged bruising (a hand-slap, a ligature, an implement), injuries incompatible with the stated mechanism, burns with clear immersion or demarcation lines, and fractures of differing ages. The history is often vague, delayed, or changes between tellers, and the child may be presented for an unrelated complaint. [6] [11]
Abusive head trauma presents as unexplained encephalopathy in an infant — irritability, vomiting, apnoea, seizures, or collapse — with subdural haemorrhage, retinal haemorrhages that are extensive, multilayered and reach the periphery, and often a history of a trivial mechanism such as a short fall. The PredAHT tool combines six features (head/neck bruising, subdural haemorrhage, hypoxic-ischaemic injury, retinal haemorrhage, rib fracture, and long-bone fracture) to estimate the probability of abuse. [12] [14]
Child sexual abuse presents most often as a disclosure by the child — the single most common presentation — and the verbatim disclosure must be recorded without interrogation. Other presentations are behavioural change (regression, sexualised behaviour, withdrawal), anogenital symptoms, a sexually transmitted infection or pregnancy in a pre-pubertal child, and disclosure to a trusted adult days, weeks or years after the event. [13]
Emotional abuse presents as a child who is withdrawn, fearful, avoidant of a caregiver, self-soothing in stereotyped ways, or showing developmental and emotional regression; the signs are subtle and chronic, and the caregiver-child interaction may itself be the most telling observation. Neglect presents as failure to thrive with faltering growth, untreated medical or dental disease, developmental delay, chronic school absence, and inadequately clothed or supervised children. [10] [2]
Caregiver-fabricated or induced illness presents as perplexing, recurring symptoms that do not fit known disease, that resolve when the child is separated from the caregiver, with test results that are abnormal but inconsistent, and a caregiver who is strikingly knowledgeable, over-involved and seeks repeated invasive intervention. The trap is to keep investigating the symptoms rather than the pattern. [2] [14]
The atypical presentations are deliberately examined. A well-looking infant may carry a sentinel injury; a child with disability may disclose only through behavioural change and cannot always be examined in the usual way; and an adolescent's self-harm, substance use or running-away may be the only signal of ongoing sexual or physical abuse. Holding these in mind stops the "looks well" trap. [8] [13]
Differential Diagnosis
The differential is the gate that protects both directions of the error: missing abuse, and falsely accusing a family. The aim is not to list every rare mimic but to separate the common, dangerous and plausible causes by features you can test at the bedside and on investigation. [6] [2]
For bruising, separate inflicted bruising from dermal melanocytosis (Mongolian blue spots — blue-grey, typically over the sacrum and buttocks, unchanged over time, fading over years), from culture-bound practices such as coin rubbing (coining) and cupping used for febrile illness, and from bleeding disorders such as idiopathic thrombocytopenic purpura and Henoch-Schönlein purpura. The discriminating features are site, pattern, the child's mobility, the colour and its evolution, and the platelet count and coagulation screen. [6] [7]
For fractures, separate inflicted fractures from osteogenesis imperfecta (a family history of fractures, blue sclerae, dentinogenesis imperfecta, wormian skulls), rickets and preterm osteopenia of prematurity (metaphyseal fraying, biochemical vitamin-D deficiency), and accidental injury. The discriminating features are the fracture pattern (classic metaphyseal lesions and posterior rib fractures are highly specific for abuse), the callus age versus the stated timing, the family history, and the metabolic and genetic workup. [2] [9]
For abusive head trauma, separate inflicted head injury from accidental trauma (a credible high-energy mechanism with consistent history), birth-related subdural haemorrhage (resolving in the first weeks of life), metabolic disease such as glutaric aciduria (macrocephaly, frontotemporal atrophy), coagulopathy, and meningitis or encephalitis. The discriminating features are the history, the retinal findings, the pattern and age of the haemorrhage, and the metabolic and infective workup. [12] [14]
For burns, separate inflicted scalds from accidental spills (a splash pattern with cooling-tail dribbles, no clear demarcation line), bullous impetigo and staphylococcal scalded skin (flaccid blisters, positive Nikolsky, no clear immersion geometry), fixed drug eruptions, and cultural practices. The discriminating feature is the geometry — an immersion burn shows a clear fluid line, a glove-and-stocking distribution and no splash, which an accidental spill cannot reproduce. [2] [11]
For failure to thrive, separate neglect from organic disease (coeliac disease, cystic fibrosis, endocrine and metabolic causes) and constitutional or familial short stature. The discriminating test is catch-up growth on a supervised feeding trial, together with the growth-chart trajectory and the elimination of organic disease. [2] [10]
Clinical & Bedside Assessment
The examination must be trauma-informed, unhurried, top-to-toe, and performed by an appropriately trained clinician with consent and a chaperone present. Explain each step to the child and the family, attend to pain first, and never repeat an examination that has already been done well — repeated examinations re-traumatise the child and add nothing. [2]
Document every injury on a body map: the exact site, the measured size and shape, the colour, the pattern, and the stage of healing, and photograph each injury with a scale. A contemporaneous, diagrammed, dated record is the single most powerful piece of evidence you will produce, because it cannot be reconstructed later. Separately record who gave the history and the exact words used in any disclosure. [2] [8]
Examine specifically for the findings that examiners test. Inspect the frenulum, oral cavity, pinna, ears, neck and torso in every pre-mobile infant — a torn frenulum, a bruised pinna or a single trunk bruise in such a child is a sentinel injury. Apply the TEN-4-FBCP rule to any bruise. Measure growth (weight, length or height, head circumference) on validated charts and look for faltering. Assess the developmental and emotional state, the school engagement, and the parent-child interaction. Recognise that a normal examination does not exclude significant abuse — disclosure and history often outweigh physical signs. [6] [8]
Investigations
The workup is tailored to the form and the age, but it rests on a small number of high-yield, time-sensitive tests. The aim is to confirm or exclude occult injury, to exclude mimics, and to generate objective evidence that a future case conference or court can rely on — while never delaying stabilisation or reporting to complete it. [2]
Core physical-abuse workup
Skeletal survey with dedicated, multiple views for any child under two years with suspected physical abuse — a single 'babygram' is never adequate.
Repeat the skeletal survey at 11 to 14 days to reveal occult fractures and clarify callus dating.
Non-contrast CT brain as first-line for suspected abusive head trauma or any infant with altered consciousness; MRI brain once stable for parenchymal and dating detail.
Specialist indirect ophthalmoscopy for retinal haemorrhages in suspected abusive head trauma.
Coagulation screen (full blood count, PT/INR, APTT, fibrinogen, von Willebrand panel) for any bruising to exclude a bleeding diathesis.
Metabolic bone and, when indicated, metabolic genetics workup for unexplained fractures to exclude osteogenesis imperfecta and rickets.
STI screening and forensic specimen collection, by a trained examiner within jurisdictional time windows, for suspected sexual abuse.
A skeletal survey with dedicated views of every bone is required for any child under two years with suspected physical abuse, and a single "babygram" is explicitly inadequate because it misses the subtle, highly specific classic metaphyseal and rib fractures. A repeat survey at 11 to 14 days detects fractures that were occult or non-specific on the first study and clarifies the age of callus, which dates the injury. [9] [2]
For suspected abusive head trauma, non-contrast CT brain is the first-line modality for an unstable or acutely encephalopathic infant, and MRI brain is obtained once the child is stable to define parenchymal injury, diffuse axonal injury and the age of haemorrhage. A specialist ophthalmology examination with indirect ophthalmoscopy looks for retinal haemorrhages — extensive, multilayered bleeds reaching the periphery are highly suggestive of abusive head trauma. [12] [14]
The coagulation screen (full blood count, prothrombin time with INR, activated partial thromboplastin time, fibrinogen and a von Willebrand panel) excludes a bleeding diathesis before bruising is attributed to abuse. For unexplained fractures, metabolic biochemistry (calcium, phosphate, alkaline phosphatase, vitamin D) and, when indicated, a metabolic genetics opinion exclude osteogenesis imperfecta and rickets. For suspected sexual abuse, STI screening and forensic specimen collection are performed by a trained examiner within jurisdictional time windows, weighing yield against the child's distress. [6] [13]
Management — Resuscitation
Treat the presenting injury or physiological threat first, using an ABCDE approach, before the abuse assessment dominates your thinking. Analgesia, fluid resuscitation, control of seizures and management of raised intracranial pressure take priority over gathering the history or imaging, because a dead child cannot be protected. [2]
Stabilise and admit any child with abusive head trauma, a significant injury, or failure to thrive, and do not discharge a child who is not safe. The immediate safety decision is binary: is there ongoing risk in the home? If yes, the child does not go home until a child-protection plan is in place — seek a place of safety, involve the statutory agency, and document the reasoning explicitly. [2] [9]
The time-critical forensic step runs in parallel: preserve evidence by not cleaning the child or removing clothing before examination where forensic specimens may be needed, once medical stabilisation permits. Do not bathe the child after a suspected sexual assault before specimens are taken. Evidence is perishable — once washed or discarded it cannot be recovered. [13] [2]
Recognise that recognising and responding to maltreatment is distressing for clinicians too. Engage senior staff, the child-protection team and a debrief early; the documented impact of child-protection work on clinicians — stress, burnout and, for some, secondary trauma — means self-care is part of the response, not an afterthought. [2]
Management — Definitive & Stepwise
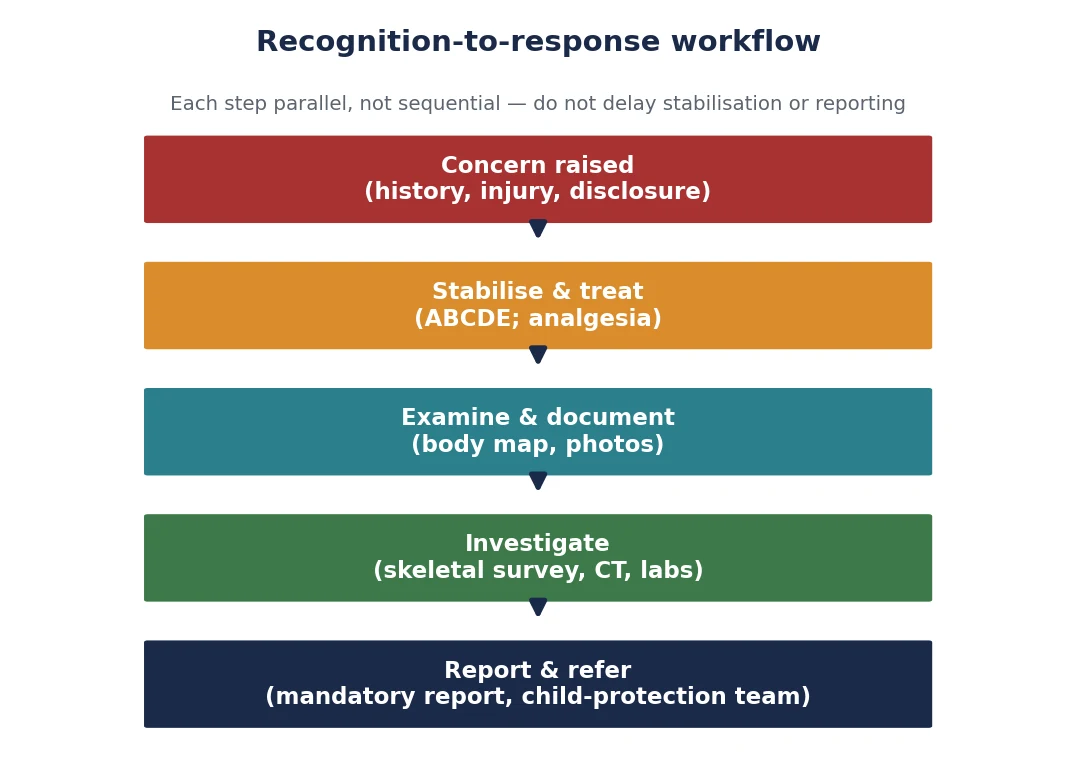
The definitive response is a bundle run in parallel, not a sequence. Stabilise, examine and document, investigate, report, refer, and safeguard — these proceed at the same time, and the two that examiners most often see delayed are documentation (left until "after the workup") and reporting (left until "after certainty"). Neither waits. [2]
Make the mandatory report to the statutory child-protection agency when you form a reasonable belief that a child has suffered, or is at risk of, significant harm, applying your jurisdictional threshold. Whether your jurisdiction imposes mandatory reporting, and for which forms and by whom, varies — know your local statute — but the clinical principle does not: reporting rests on a reasonable belief of risk, not on diagnostic certainty. [2] [9]
Refer to the multidisciplinary child-protection team and arrange a case conference that brings together social work, mental health, primary care, education and, where relevant, law enforcement. The conference builds a single, shared understanding of risk and a single plan, and it is where the medical findings meet the psychosocial context that medicine alone cannot capture. [2]
Build a written safety plan that specifies who the child will live with, the supervision arrangements, any no-contact conditions, and the follow-up review date; arrange supervised contact if needed. Arrange trauma-focused therapy for the child and support for the non-offending caregiver, because the buffering-adult mechanism is where the biology of harm meets the biology of recovery. Arrange close medical, developmental and mental-health follow-up, and a repeat skeletal survey where indicated, documenting the plan and handing over explicitly to the named professionals who carry it. [2] [3]
Specific Subtypes & Scenarios
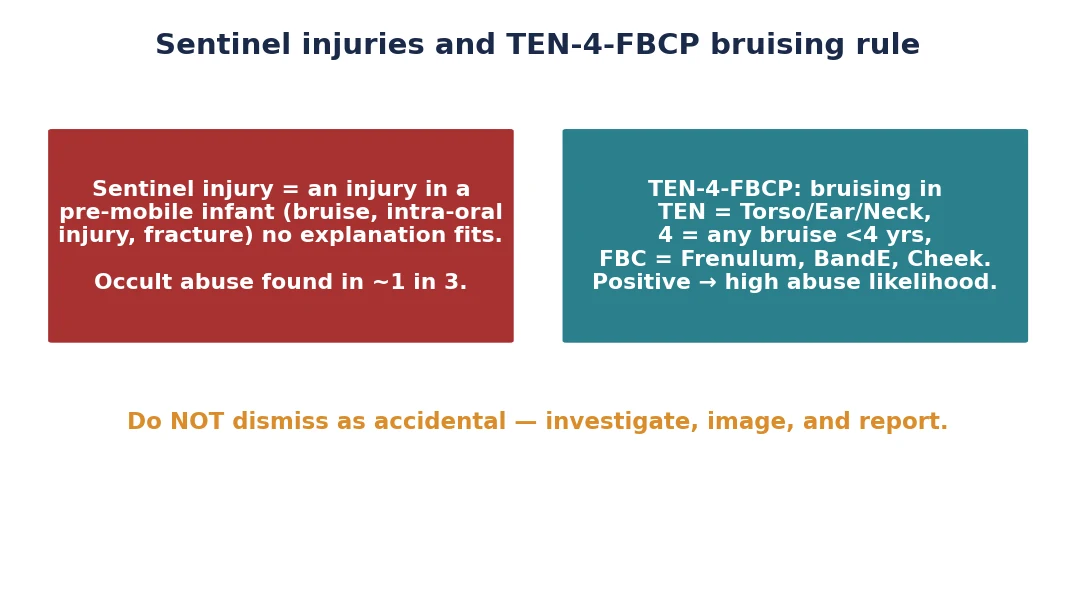
A sentinel injury in a pre-mobile infant is the scenario examiners reward most. Investigate with a skeletal survey and coagulation screen, examine fully, and report; roughly one in three such infants has occult abuse found, and the sentinel injury may be the last warning before a fatal event. The error to name and avoid is the "minor bruise, likely accidental" discharge. [8] [9]
Suspected abusive head trauma demands a full trauma-team response: stabilisation and neuroprotection, control of seizures and raised intracranial pressure, non-contrast CT brain and then MRI, specialist ophthalmology, a skeletal survey, coagulation and metabolic workup, and admission to a monitored bed. Apply the PredAHT features to estimate the probability of abuse and document the reasoning, while excluding the metabolic and coagulopathic mimics. [12] [14]
Child sexual abuse follows a disclosure-led, examiner-trained forensic pathway within the jurisdictional time window, with STI prophylaxis and emergency contraception as indicated by the assessment, and a trauma-informed aftercare plan. Record the verbatim disclosure, do not interrogate, and do not delay emergency contraception or HIV post-exposure prophylaxis where indicated by the assessment. [13]
Neglect with failure to thrive is managed with a supervised feeding trial (often requiring admission to demonstrate catch-up growth), assessment of the developmental impact, a home and needs assessment, and a structured family-support and review plan. The recovery of growth on a feeding trial is both diagnostic and the first therapeutic step. [2] [10]
Caregiver-fabricated or induced illness is managed by objective verification of the reported findings, separation and observation of the child, review of historical records across centres, and a child-protection referral. The cardinal rule is not to confront the caregiver before safeguarding is in place, because confrontation can precipitate escalation or flight. [2] [14]
Children with disability are over-represented among maltreated children and often cannot disclose verbally. Recognise behavioural change, sleep disturbance and unexplained injury as the equivalent of disclosure; adapt the examination and communication to the child; and hold a higher index of suspicion rather than attributing distress to the disability. [1] [13]
Complications & Pitfalls
Missing a sentinel injury is the most preventable failure in paediatrics, and it may precede a fatal or disabling event. Examine every pre-mobile infant fully, document on a body map, and never write off a single bruise as accidental in a child who does not yet move independently. [8] [9]
Accepting an implausible history is the parallel failure. A history that does not fit the injury's age, pattern or the child's developmental stage is itself a finding — document the discrepancy explicitly, and do not let a confident, fluent account override the physiology. Conversely, premature labelling and racial or cultural bias cause the opposite harm: mistaking a Mongolian spot, coining, cupping or a cultural dressing for abuse damages a family and erodes trust. Verify the mimic before concluding, and use a second opinion where doubt remains. [6] [2]
Delaying the mandatory report to complete the workup is a recurring and serious pitfall. Reporting is triggered by a reasonable belief of risk, not by diagnostic certainty — report first, and complete the skeletal survey and the rest of the workup in parallel. Failing to document contemporaneously, or to use a body map, means an injury that could have been defended later cannot be. Confounding a bleeding disorder with abuse (or vice versa) is avoided by ordering the coagulation screen before attributing bruising. [2] [9]
Secondary traumatising the child through repeated examinations is a pitfall that is easy to cause and entirely avoidable. Coordinate a single examination by a trained clinician, share the findings between teams, and do not re-examine for the sake of completeness. [2] [13]
Prognosis & Disposition
The protective factor with the strongest evidence is a stable, responsive adult relationship, and intervention is designed to protect or rebuild it. Where the child cannot remain safely at home, placement with kin or a foster family preserves the relational buffer better than an institutional setting, and trauma-focused therapy supports recovery in both the child and the non-offending caregiver. [3] [4]
Recurrence is common when the child returns to an unchanged environment, and re-injury after a sentinel event may be fatal — which is why a written safety plan, supervised contact conditions and a fixed follow-up date are not optional. The long-term prognosis follows the dose-response curve of cumulative adversity: more forms and more adversity predict worse adult mental and physical health, but timely recognition and consistent support improve the trajectory. [3] [10]
Disposition spans medical admission for safety and treatment, place-of-safety placement when home is unsafe, and structured outpatient follow-up for developmental, mental-health and medical needs. The safety-net is explicit: a written follow-up plan, engagement of primary care and school, and a clear re-presentation pathway for the family so that deterioration is caught early. [2]
Special Populations
The very young, the disabled and the already-disadvantaged carry the highest risk of both maltreatment and being missed, and each group needs a deliberately adjusted approach. Infants under one year have the highest rates of severe and fatal abuse and the lowest threshold for a skeletal survey and admission — a single bruise in a non-mobile infant is a sentinel injury. Children with disability or chronic illness are over-represented among maltreated children, often cannot disclose verbally, and may show only behavioural change, sleep disturbance or unexplained injury; hold a higher index of suspicion and adapt examination and communication rather than attributing distress to the disability. [1] [13]
Aboriginal and Torres Strait Islander, Māori and other Indigenous children require culturally safe, trauma-informed care that addresses structural determinants and historical context; do not conflate socioeconomic disadvantage with risk, and apply the same objective, evidence-based recognition while engaging Indigenous health workers and family. Children in out-of-home care and refugee or asylum-seeking children carry high baseline adversity, so screen actively for past and ongoing abuse and unmet health need at every contact. Adolescents require a careful balance of confidentiality and mandatory reporting, and disclosure, self-harm, substance use and running-away may be the only signal of ongoing sexual or physical abuse; manage consent and sexual-health needs directly. [2] [5]
In Australia and New Zealand, mandatory reporting statutes vary by state and territory in their scope and in which professions are mandated, but the RACP and the colleges hold all paediatricians to a duty to report a reasonable belief of significant harm. Notify the statutory child-protection authority, involve the hospital child-protection unit, and arrange a case conference coordinated with social work. [2]
Evidence, Guidelines & Regional Differences
The causal chain from maltreatment to adult disease now rests on large meta-analytic evidence. The long-term-outcomes meta-analysis confirmed elevated risks of mental disorder, substance use, self-harm and physical disease after physical abuse, emotional abuse and neglect, and the Adverse Childhood Experiences study established a graded relationship between the ACE score and the leading adult causes of death. Global prevalence and the under-detection gap are documented in the WHO/CDC systematic review of past-year violence against children. [10] [3] [5]
Validated decision tools have moved recognition from intuition toward rule-based practice. The TEN-4-FBCP bruising clinical decision rule, validated in a multicentre study, identifies bruising patterns that carry a high likelihood of abuse and demand evaluation; the PredAHT abusive-head-trauma prediction tool combines six clinical and imaging features to estimate the probability of abuse. Both tools raise the index of suspicion where it should be raised and supply objective support for the report. [7] [12]
TEN-4-FBCP multicentre validation
Population: Young children with bruising evaluated for suspected abuse across multiple centres
Key finding
The TEN-4-FBCP rule discriminated abusive from non-abusive bruising with high sensitivity; a positive rule substantially raised the likelihood of confirmed abuse.
Practice change
Apply the rule to any bruise in a young child: a positive result mandates full evaluation, not reassurance.
The regional guideline structure is consistent in principle and varies in statute. In ANZ, the RACP provides child-protection guidance and each jurisdiction sets its own mandatory-reporting law and threshold. In the UK, the RCPCH child-protection evidence base and the "Working Together" statutory framework set the standard, and all healthcare staff are expected to report. In the US, the AAP child-abuse-pediatrics specialty and state-by-state mandated-reporter laws apply. In Canada, the RCPSC holds a child-maltreatment competency and each province imposes a duty to report. In every region the clinical trigger is the same: a reasonable belief of significant harm. [2] [5]
The controversies are real and must be managed with objectivity, multidisciplinary review and adherence to evidence. They include the appropriate threshold and age limit for a skeletal survey, the interpretation of classic metaphyseal and rib fractures, the limits of dating bruises, the competing risks of false accusation and missed abuse, and the boundary between a perplexing genuine illness and fabricated or induced illness. The defence against each is the same: a calm, documented, evidence-based assessment shared with a multidisciplinary team. [9] [14]
Exam Pearls
- The most common presentation of child sexual abuse is a disclosure by the child — believe it, record it verbatim, and do not interrogate. [13]
- A bruise in a non-mobile infant is never normal — it is a sentinel injury until proven otherwise. [8]
- TEN-4-FACESp: Torso, Ear, Neck bruising in a child under 4 years; any bruise under 4 months; Frenulum, Angle of jaw, Cheeks, Eyelids, Subconjunctivae, patterned — a positive rule means evaluate for abuse. [7]
- Retinal haemorrhages that are extensive, multilayered and reaching the periphery are highly suggestive of abusive head trauma. [12]
- A single babygram is never an adequate skeletal survey; order dedicated views and repeat at 11 to 14 days. [9]
- Mongolian spots are blue-grey, usually over the sacrum and buttocks, do not change colour, and fade over years — distinct from a fresh bruise. [6]
- Reporting rests on a reasonable belief of risk, not on diagnostic certainty — report first, complete the workup in parallel. [2]
- The single most protective factor against the toxic-stress cascade is a stable, responsive adult relationship. [3]
References
- [1]Gilbert R; Widom CS; Browne K; et al Burden and consequences of child maltreatment in high-income countries. Lancet, 2009.PMID 19056114
- [2]Gilbert R; Kemp A; Thoburn J; et al Recognising and responding to child maltreatment. Lancet, 2009.PMID 19056119
- [3]Felitti VJ; Anda RF; Nordenberg D; et al Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 1998.PMID 9635069
- [4]Hughes K; Bellis MA; Hardcastle KA; et al The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health, 2017.PMID 29253477
- [5]Hillis S; Mercy J; Amobi A; Kress H Global Prevalence of Past-year Violence Against Children: A Systematic Review and Minimum Estimates. Pediatrics, 2016.PMID 26810785
- [6]Pierce MC; Kaczor K; Aldridge S; et al Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics, 2010.PMID 19969620
- [7]Pierce MC; Magana JN; Kaczor K; et al Validation of a Clinical Decision Rule to Predict Abuse in Young Children Based on Bruising Characteristics. JAMA Network Open, 2021.PMID 33852003
- [8]Sheets LK; Leach ME; Koszewski IJ; et al Sentinel injuries in infants evaluated for child physical abuse. Pediatrics, 2013.PMID 23478861
- [9]Lindberg DM; Beaty B; Juarez-Colunga E; et al Testing for Abuse in Children With Sentinel Injuries. Pediatrics, 2015.PMID 26438705
- [10]Norman RE; Byambaa M; De R; et al The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine, 2012.PMID 23209385
- [11]Maguire SA; Upadhyaya M; Evans A; Kemp AM A systematic review of abusive visceral injuries in childhood--their range and recognition. Child Abuse & Neglect, 2013.PMID 23306146
- [12]Cowley LE; Morris CB; Maguire SA; et al Validation of a Prediction Tool for Abusive Head Trauma. Pediatrics, 2015.PMID 26216332
- [13]Adams JA; Kellogg ND; Farst KJ; et al Sexual Abuse in Children: What the General Practice Ob/Gyn Needs to Know. Clinical Obstetrics and Gynecology, 2020.PMID 32366764
- [14]Jenny C; Rieth KG Mild abusive head injury: diagnosis and pitfalls. Child's Nervous System, 2022.PMID 36637470