Paeds · child-safety-and-social-paediatrics
Child sexual abuse and assault assessment
Also known as Child sexual abuse assessment · Child sexual assault medical examination · Anogenital examination for suspected abuse · Forensic paediatric examination after sexual assault · CSA medical evaluation
A fellowship approach to the medical assessment of a child or adolescent who may have been sexually abused or assaulted: deciding the tempo from acute to non-acute, conducting the trauma-informed forensic history and ano-genital examination, interpreting normal and abnormal findings against the Adams consensus, ordering the right investigations within the correct time windows, assembling the acute management bundle, and discharging the safeguarding, reporting and follow-up duties.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A seven-year-old is brought to the emergency department at midnight after disclosing that her mother's partner touched her genitals. The triage nurse asks you what happens next. Your job is not to decide in this moment whether abuse occurred. Your job is to run a safe, staged assessment that protects the child, preserves any evidence that is time-limited, treats what can be treated, and hands the diagnosis to the child-protection and police systems that are built to weigh it. [1] [2]
Child sexual abuse is the involvement of a child in sexual activity that they cannot consent to, cannot understand, or cannot refuse, and that violates the laws or social taboos of the society. The medical assessment is one piece of a multi-agency response, and it answers four questions: is the child medically safe now, what examination and investigation are indicated today, what must be preserved before the forensic window closes, and what safety, reporting and follow-up follow from that. [1]
The single most important idea to hold throughout — and the one examiners probe hardest — is that the physical examination is usually normal. In Adams' landmark study of legally confirmed abuse, the majority of children had normal or nonspecific findings, because hymenal tissue heals rapidly and most contact is non-penetrative or delayed before examination. A normal exam therefore never rules out abuse. The history, taken once and well by a trained forensic interviewer, almost always carries more diagnostic weight than the genital findings. [3]
Classification
The first branch in any CSA assessment is the tempo: is this an acute presentation within the forensic evidence window, or a non-acute disclosure? Everything downstream — urgency, setting, what you examine for, whether a forensic kit is taken — follows from that single decision. [1]
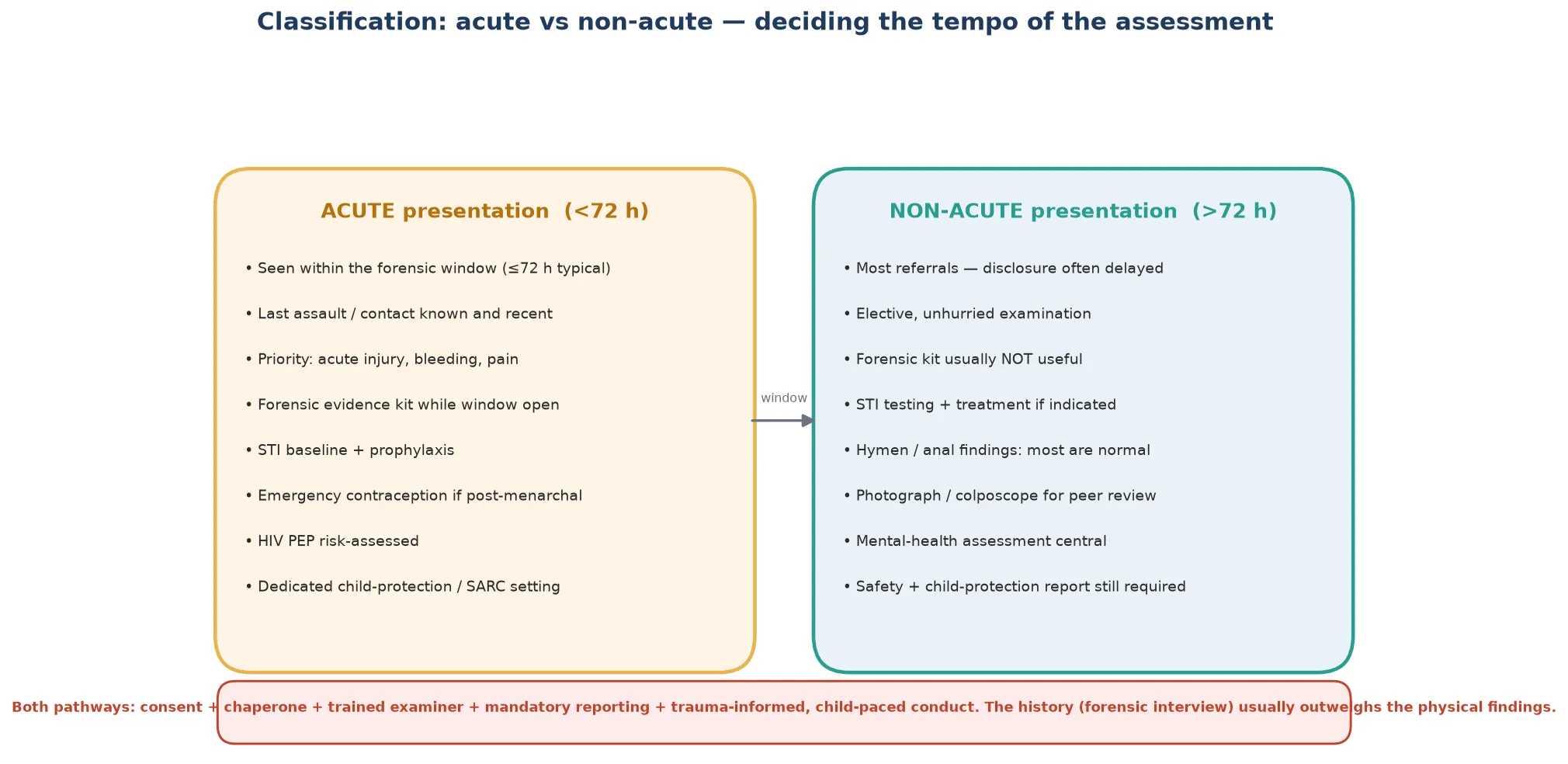
The second useful axis is the type of contact. Non-contact abuse includes exposure to pornography, voyeurism, and being made to watch sexual acts. Contact abuse ranges from fondling and genital touching through to oral, vaginal or anal penetration. Penetrative abuse is the category most likely to leave a specific finding, but it is also the category most likely to be delayed before examination, which is why even penetrative abuse often yields a normal exam. [2]
Acute (<72 h)
Time-critical
- Forensic evidence kit while window open
- Acute injury, bleeding, pain first
- STI baseline + post-exposure prophylaxis
- Emergency contraception if post-menarchal
- Dedicated child-protection / SARC setting
Non-acute
Elective
- Most referrals — disclosure usually delayed
- Unhurried, child-paced examination
- Forensic kit rarely useful
- STI testing + treatment if indicated
- Mental-health and safety planning central
Contact vs non-contact
What happened
- Non-contact: exposure, voyeurism, pornography
- Contact: fondling, oral, genital
- Penetrative: vaginal or anal
- Penetrative most likely to scar — but often delayed
A third axis the examiner may press is the relationship to the perpetrator: intra-familial abuse (most common, often chronic and delayed) versus extra-familial and stranger assault, and adolescent sexual assault, which carries its own consent, confidentiality and emergency-contraception decisions. [1]
Epidemiology & Risk Factors
Child sexual abuse is common. Two large meta-analyses converge on a global prevalence of roughly one in five girls and one in eight boys before the age of 18, although rates vary widely with definition and method. The scale of the problem is the reason every general paediatrician must be competent in the assessment, not only the sub-specialist. [10] [11]
Most perpetrators are known to the child — a parent, step-parent, relative, family friend, caregiver or older child — which is why the perpetrator is so often in the waiting room, and why the timing of the interview and the separation of the child from the accompanying adult matter operationally. Stranger assault is less common and more likely to present acutely. [1]
Risk is not evenly distributed. Children with disability, especially those who are non-verbal or have intellectual impairment, face substantially higher risk and face it with fewer ways to disclose. So do children in out-of-home care, young people in youth-justice settings, and those living with parental mental illness or substance use. Recognising these groups lets you make the assessment opportunistic — building a safeguarding review into a foster-care health check or a disability clinic. [1]
Pathophysiology
Understanding why the examination is usually normal is the single most important piece of pathophysiology in this topic, because it is the error that lets abused children be dismissed. The hymen is a thin, oestrogen-sensitive mucosal fold at the vaginal introitus. Its morphology changes with age — delicate and un-oestrogenised before puberty, fuller and redundant under the influence of oestrogen during puberty and beyond. The posterior rim, between the 3 and 9 o'clock positions, is where most specific findings of penetrative trauma are found. [4] [7]
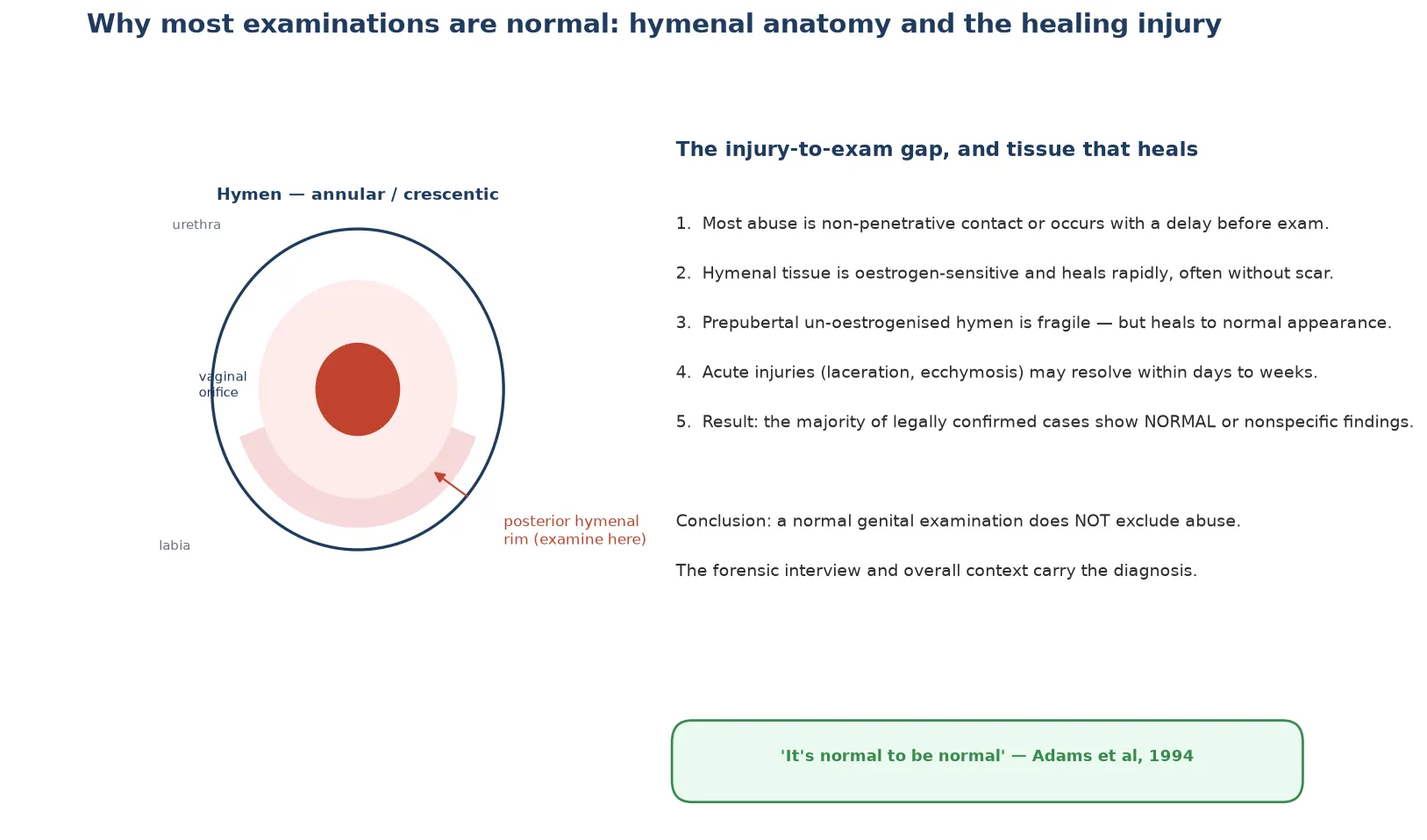
Three forces combine to produce the "normal to be normal" finding. First, most abuse is non-penetrative contact that leaves no lasting mark. Second, even penetrative injury to hymenal and anal tissue heals quickly and often without scarring, particularly in the un-oestrogenised prepubertal child. Third, disclosure is frequently delayed, so by the time the child reaches you the window for an acute finding has passed. The net result is that the majority of legally confirmed cases have a normal or nonspecific examination. [3] [8]
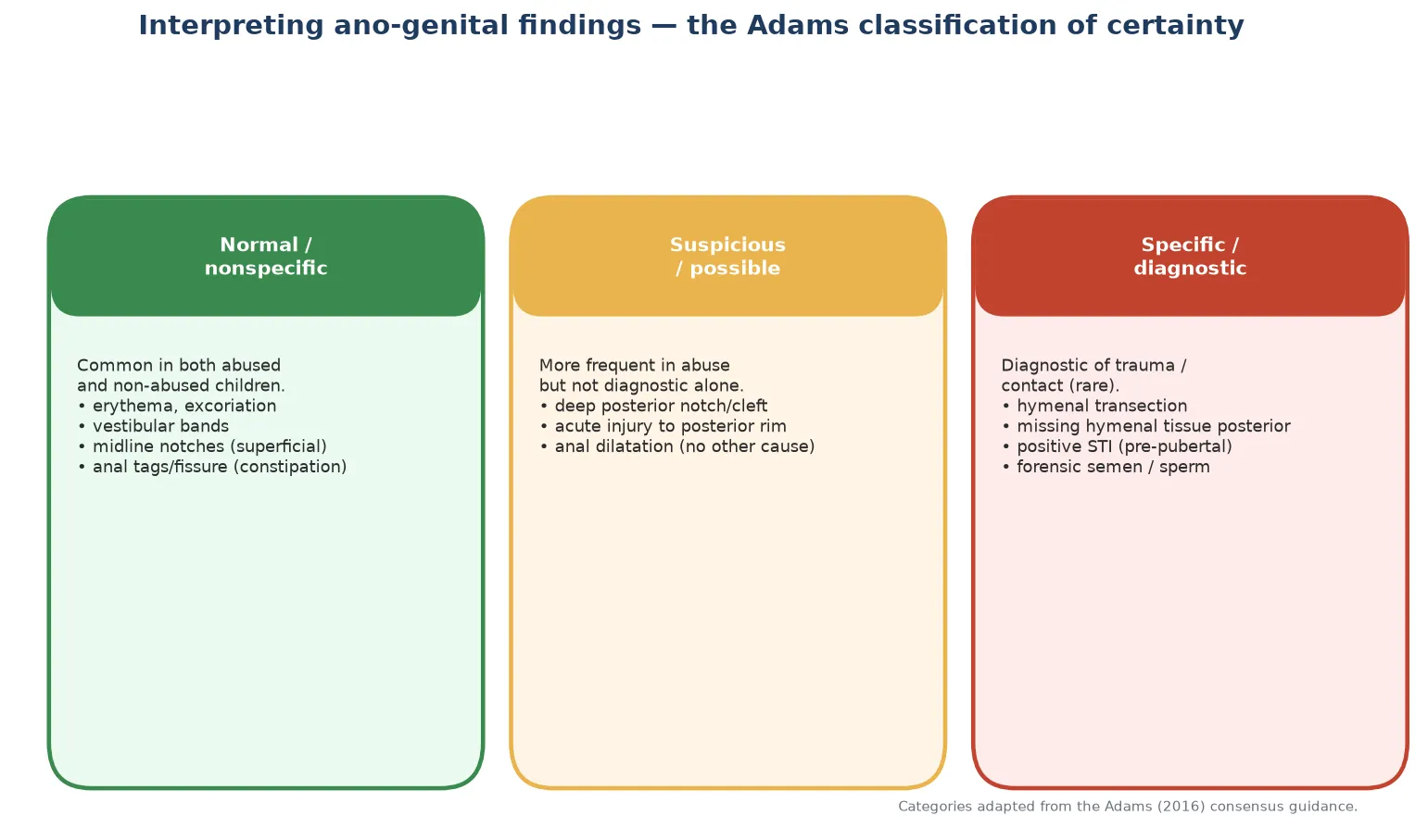
The findings that do persist are the specific findings: a full-thickness transection of the posterior hymenal rim, absence of hymenal tissue between 3 and 9 o'clock, and a fresh deep laceration. These are rare but diagnostic of trauma. They are the exceptions that prove the rule that the exam is usually normal, not a tool to rule abuse out. [1] [4]
Clinical Presentation
Children who have been sexually abused rarely present with a clean, full, immediate disclosure. The more typical picture is a delayed, partial, tentative or retracted statement — a child who hints, asks whether a secret can be kept, then withdraws under pressure. Understanding this presentation prevents the most common bedside error, which is dismissing a tentative disclosure because it sounds uncertain. [1]
Disclosure pattern
How it usually sounds
- Delayed — days, weeks, years after
- Partial or incremental — told in pieces
- Tentative — 'can you keep a secret?'
- Retracted under family pressure
- Triggered by safety education, media, a trusted adult
Behavioural indicators
Non-specific
- Sleep disturbance, regression, withdrawal
- New sexualised behaviour beyond developmental norm
- School decline, somatic complaints
- Anxiety, depression, self-harm in adolescents
- Indicators alone never diagnose — but prompt asking
The acute physical presentation is the easy one to recognise: genital bleeding, pain, or visible injury after a disclosed assault, or an adolescent brought in within hours of rape. This presentation triggers the acute pathway and the forensic window. The harder and more common presentation is the non-acute one — the behavioural change, the sleep disturbance, the sexualised behaviour in a young child — where your task is to create the conditions for a disclosure, not to hunt for an injury that has long since healed. [2]
The adolescent presentation deserves a separate mention because it carries consent, confidentiality and contraception decisions that do not arise in the young child. An adolescent may be unsure whether an encounter was consensual, may fear parental discovery, or may be most concerned about pregnancy and infection rather than prosecution. The assessment must hold all of these at once. [1]
Differential Diagnosis
When a child has a genital or anal finding, your job is to separate the inflicted from the accidental and the benign. The differential matters because the wrong label is catastrophic in either direction — missing abuse endangers a child, and over-calling a benign finding destroys a family. The discriminating features are the location of the finding and the history that accompanies it. [1] [7]
Straddle injury
Accidental
- External, anterior, asymmetric
- History of clear fall onto a hard edge (bicycle, playground)
- Injury to labia, perineum, mons — not posterior hymen
- Usually unilateral, bridged
Lichen sclerosus
Mimic
- 'Figure-of-8' pale atrophic plaques
- Pruitus, bleeding, fissuring
- Prepubertal girls; may bruise or bleed
- Blanches with topical steroid — resolves the picture
Vulvovaginitis / UTI
Common mimic
- Discharge, erythema, dysuria
- Poor hygiene, pinworms, irritant
- Nonspecific findings — do not diagnose abuse
- Treat the cause; consider testing if red flags
Anal fissure (constipation)
Common mimic
- Midline, superficial, with hard stools
- Resolves with stool softening
- Distinguish from acute traumatic injury
- Tags and skin tags can follow
Two rules resolve most of the differential. First, location discriminates: inflicted penetrative injury clusters on the posterior hymenal rim and the anal sphincter, whereas accidental injury (straddle) sits externally and anteriorly on the labia, perineum and mons. Second, the history must fit the finding: a straddle history that explains a labial contusion is reassuring; the same finding with no plausible mechanism is not. [4]
The most dangerous mimic to over-call is the normal variant mistaken for a specific finding — a midline posterior notch, a hymenal tag, or a vestibular band. These are common in non-abused children, which is why the comparison studies of girls selected for nonabuse exist: to anchor what is normal before you label anything abnormal. [4] [7]
Clinical & Bedside Assessment
The assessment is trauma-informed and child-paced from the moment the child arrives. The setting is quiet and private; the examiner is competent and supported by a chaperone; the child is told what will happen and given genuine choices where they exist; and every effort is made to minimise the number of times the child must tell their story. Re-traumatisation through repeated interviews and examinations is a real harm, and avoiding it is part of the treatment. [1]
The structured assessment, in order
Safety first — acute injury, bleeding, pain; separate the child from the suspected perpetrator
Consent from the child (age-appropriate) and guardian; explain limits to confidentiality honestly
Single forensic interview by a trained interviewer (NICHD protocol) — you listen, you do not re-question
General examination including growth, skin, and signs of other maltreatment
Ano-genital examination: supine frog-leg with labial separation then traction; knee-chest position if needed
Colposcopy with photo-documentation for peer review, with explicit consent for the images
Investigations timed to the window (STI, pregnancy, forensic kit)
Safety planning, mandatory report, and disposition before the child leaves
The forensic interview is the heart of the assessment, and the clinician's role in it is constrained. A trained interviewer uses a structured protocol — the NICHD Investigative Interview Protocol is the best-evidenced — that begins with open-ended narrative and only later, if at all, moves to focused questions, avoiding leading or suggestive prompts. The medical clinician should not re-interview the child about the detail of the abuse; one good interview is the goal, because repeated and suggestive questioning both contaminates the evidence and distresses the child. [9]
The genital examination is technique-dependent and must be done by a competent examiner. The standard position is supine frog-leg with the hips abducted. The examiner first inspects the external genitalia, then uses labial separation (gently pulling the labia apart) and labial traction (gently pulling the labia outward and toward the examiner) to visualise the hymenal rim. The knee-chest position is added when the hymen is not adequately seen supine. Colposcopy provides magnification and the means to capture images for peer review. [1] [7]
In Australia and Aotearoa New Zealand, examinations are performed by clinicians with child-protection training, often through a dedicated Sexual Assault Referral Centre (SARC) or a paediatric forensic medical service, with remote peer review where local expertise is limited. Mandatory reporting of reasonable belief of child sexual abuse applies to all registered medical practitioners. [1]
Investigations
Investigations are chosen by the timing of the alleged contact and the child's pubertal stage, not sent as a blanket. Three groups of test apply: sexually transmitted infection (STI) testing, forensic evidence collection, and pregnancy testing in a post-menarchal adolescent. Blood-borne virus testing and repeat serology are timed to incubation and seroconversion windows. [1] [12]
Forensic kit
Only if within window
- Collected when the alleged contact is within the forensic window (typically up to 72 hours)
- Swabs for semen, sperm, DNA; clothing, debris, foreign hair
- Strict chain of custody; consent for the kit and for storage
- Largely unhelpful beyond the window — do not delay acute care for it
STI testing
By age and timing
- Prepubertal: test only if indicated (disclosure, finding, symptoms)
- Adolescent: NAAT for chlamydia, gonorrhoea, trichomonas from relevant sites
- Syphilis, HIV, hepatitis B and C serology baseline; repeat per incubation
- A prepubertal STI, once vertical transmission excluded, is highly concerning
Pregnancy
Post-menarchal
- Urine b-hCG in any post-menarchal adolescent
- Drives emergency contraception decision
- Repeat at follow-up if negative and at risk
The forensic evidence window is short. Most jurisdictions use a window of up to 72 hours for genital swab collection in children, though the yield falls steeply with time, and some protocols narrow this for very young children. The kit never takes priority over resuscitation, analgesia, or the child's immediate safety, and it is collected with explicit consent and a continuous chain of custody. [1] [2]
Interpreting the ano-genital examination uses the Adams consensus classification, which grades findings by how strongly they support a diagnosis of trauma or contact. Most findings fall into the normal or nonspecific group, which are seen in non-abused children; a smaller suspicious group is more frequent after abuse but not diagnostic alone; and a rare specific group — a hymenal transection, absent posterior hymenal tissue, or a positive prepubertal STI — is diagnostic. The classification exists precisely to stop over-reading the nonspecific. [1]
Management — Resuscitation
The first question in the acute presentation is whether the child is medically safe now. Active genital or anal bleeding, a deep laceration, visceral injury, or perineal trauma from a severe assault can be life-threatening and must be addressed before anything forensic. Resuscitation follows the standard paediatric ABCDE approach, with early analgesia, and senior surgical or gynaecology involvement for significant injury. [1]
In the child who is haemodynamically stable and pain-controlled, the acute pathway can proceed in an unhurried but time-aware sequence. The forensic kit is collected only if within the window, the examination is completed, and the post-exposure bundle is assembled. Throughout, the child is kept with a safe, supportive adult and separated from any suspected perpetrator. [1]
Management — Definitive & Stepwise
The acute assault bundle, for a presentation within the forensic window, is the high-yield management stem the examiner will push on. Each element is time-limited and each must carry its agent, route, timing and rationale. The operational source is the CDC Sexually Transmitted Infections Treatment Guidelines, adapted to the child's pubertal stage and the local jurisdiction. [12]
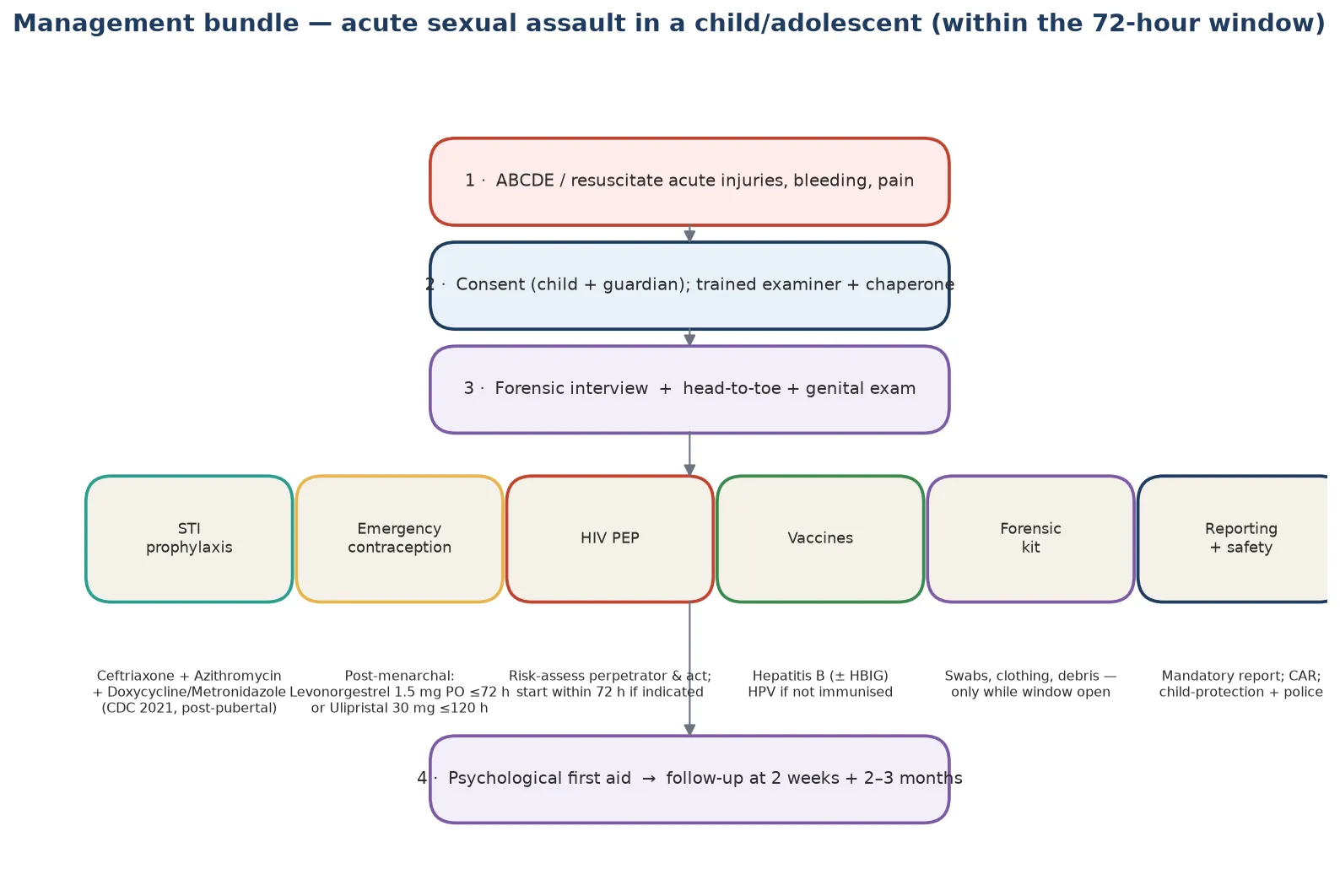
STI prophylaxis for the post-pubertal adolescent follows the CDC post-sexual-assault regimen: ceftriaxone to cover gonorrhoea, azithromycin or doxycycline to cover chlamydia, and metronidazole to cover trichomoniasis, given as empiric post-exposure prophylaxis after the baseline tests are sent. Prepubertal children are not routinely given prophylaxis; they are tested and treated only if an infection is found, because the yield is low and the burden of unnecessary medication in a young child is real. [12]
Emergency contraception (post-menarchal adolescent)
HIV post-exposure prophylaxis is decided by risk assessment of the perpetrator, the act, and the time elapsed. A three-drug antiretroviral regimen is started within 72 hours when the assailant is known or likely to be HIV-positive, or when the exposure is high-risk. The decision is made with infectious-disease or sexual-health input, and the regimen is continued for 28 days with follow-up serology. [12]
Hepatitis B and HPV are covered by vaccination. Hepatitis B vaccine is given to the non-immune child after a documented exposure, with hepatitis B immunoglobulin added when the assailant is known or likely infectious and the child is unimmunised. Catch-up HPV vaccination is offered to eligible adolescents who are not yet immunised. [12]
Psychological first aid, reporting and safety close the bundle. Mandatory reporting of reasonable belief of child sexual abuse is made to child-protection and, where indicated, police. A safety plan is agreed so the child does not return to the alleged perpetrator. Psychological first aid — calm, supportive, non-intrusive — is offered at the first contact, with a clear pathway to trauma-focused therapy, because the long-term harm is largely psychological. [1] [14]
Follow-up examination matters and is often where previously missed findings appear or infections declare. A two-week review checks healing, repeats testing where indicated, and addresses the psychological response; a two-to-three-month review repeats serology for syphilis, HIV and hepatitis, reinforces therapy engagement, and confirms the safety plan is working. [13]
Specific Subtypes & Scenarios
Acute penetrative assault in an adolescent is the scenario most likely to appear as an OSCE or short-answer stem. The candidate must run the acute bundle in order — resuscitation, consent and chaperone, examination, forensic kit, STI prophylaxis, emergency contraception, HIV PEP risk assessment, hepatitis B vaccination, reporting and safety — while holding the adolescent's confidentiality and consent rights. The presence of a controlling accompanying adult who refuses to leave the room is itself a red flag that warrants private, adolescent-only time. [12] [1]
Chronic non-acute abuse in a prepubertal child with a normal exam is the most common real-world scenario and the trap in the exam. The disclosure is the diagnosis; the normal exam is expected and changes nothing. The candidate who concludes "no abuse because no findings" has failed the question. The task is the forensic interview, a careful examination to document the (normal) baseline, STI testing where indicated, safety, and the mandatory report. [3] [8]
The non-verbal or disabled child carries higher baseline risk and cannot give a verbal history. The assessment leans harder on behavioural change, on examination, and on the accounts of carers, while recognising that the threshold to investigate is lower, not higher, when the child cannot speak. Communication aids and a familiar carer are part of making the examination tolerable. [1]
The adolescent where consensual and assault histories coexist is a reasoning test. Consent, intoxication, coercion, age of the partner and the law all bear on whether the encounter was assault, and the medical management — emergency contraception, STI prophylaxis, HIV PEP — proceeds on the basis of the sexual exposure regardless of how it is ultimately characterised. [1]
Male victims and child-perpetrated or peer assault are easily missed because of lower suspicion. Male victims may present with anal findings or with disclosure of being made to perform or receive acts; the examination and the acute bundle follow the same principles, with attention to anal injury and its mimics such as constipation. Child-perpetrated abuse still requires a safeguarding response, focused on both children. [1]
Complications & Pitfalls
The most common harm a poor assessment adds is re-traumatisation — a child made to retell the abuse to examiner after examiner until the telling itself becomes the injury. Defending a single trained forensic interview and a single competent examination, with photo-documentation so the finding never has to be re-found, is how you stop the assessment from compounding the abuse it set out to investigate. [9]
False-negative trap
Most dangerous
- Normal exam used to 'rule out' abuse
- Misses the majority who are normal
- Disclosure carries the diagnosis
- Always pair a normal exam with the history and context
Missed window
Time-critical
- Forensic kit not collected within the window
- Emergency contraception or HIV PEP delayed past efficacy
- STI baseline not taken before prophylaxis
- Use a checklist; do not defer for non-urgent reasons
Confidentiality error
Communication
- Promising secrecy you cannot keep
- Telling a parent findings before the child
- Not explaining mandatory reporting upfront
- State the limits of confidentiality before the interview
Over-reading
Differential
- Calling a normal variant a specific finding
- Misattributing straddle injury or lichen sclerosus
- Destroying a family with a mislabel
- Anchor to the non-abuse comparison studies
Missed infection, missed pregnancy, and a mishandled chain of custody are the procedural pitfalls that can be avoided with a checklist and a protocol. The chain of custody, in particular, must be unbroken from collection to the laboratory, because a broken chain can render otherwise valid evidence inadmissible and can fail the child in the courtroom. [1]
The "virginity" myth — the belief that an intact hymen proves virginity or that its absence proves intercourse — has no place in modern practice and must be actively countered, because it drives both family coercion and harmful practices. Hymenal morphology is variable in non-abused children, and even penetration does not reliably alter it. [4] [7]
Prognosis & Disposition
The long-term consequences of child sexual abuse are predominantly mental and behavioural, and they are substantial. A systematic review and meta-analysis of child maltreatment links abuse to higher rates of depressive disorder, anxiety, post-traumatic stress, self-harm and suicide, substance use, and sexual and reproductive problems in adult life. Belief, support and timely trauma-focused therapy modify this trajectory. [14]
Disposition is decided by safety first and by the multi-agency plan. The child must not return to an unsafe placement, which may mean emergency out-of-home care pending investigation. Child-protection and police receive the report and determine the statutory response, while the clinician owns the medical follow-up — the two-week and two-to-three-month reviews, the therapy referral, and the longitudinal relationship that so often falls to the general paediatrician. [1] [13]
What determines a good outcome is less the forensic detail and more whether the child was believed, supported, and kept safe, and whether trauma-focused therapy was accessible. The general paediatrician who holds the child over months and years — not only the clinician who examined them once — is often the most important determinant of recovery. [14]
Special Populations
Adolescents bring the full set of consent, confidentiality and contraception decisions. A mature minor can consent to examination, testing and emergency contraception without parental involvement; the limits of confidentiality (mandatory reporting) are stated before the interview; and the acute bundle is delivered in full. Youth-friendly, non-judgemental conduct is part of the treatment. [1]
Children with disability, especially non-verbal children, are at higher baseline risk and disclose less. The threshold to investigate is lower, the examination is adapted to the child's communication and sensory needs, and a familiar carer and communication aids are used. Behavioural change may be the only signal. [1]
Out-of-home care, youth-justice, Aboriginal and Torres Strait Islander, Māori, and refugee or migrant children carry intersecting risks of higher exposure and lower access. The assessment must be culturally safe, interpreter-mediated where needed, and connected to the child's community and care network. Recognising intergenerational trauma and avoiding re-traumatisation are part of competent care for these groups. [1]
Gender- and sexually-diverse young people may have specific concerns about confidentiality, body and identity that affect disclosure and follow-up. A respectful, affirming approach increases the chance of disclosure and engagement. [1]
Evidence, Guidelines & Regional Differences
The operational evidence base for this topic is the Adams consensus guidance, most recently updated in 2016, which sets out the approach to examination, the interpretation of findings, and the follow-up. The CDC Sexually Transmitted Infections Treatment Guidelines, 2021, provide the post-exposure prophylaxis regimens and the timing of testing. These two sources, with the local child-protection statute, are the framework a fellowship candidate should name. [1] [12]
Regional differences are real and the examiner expects them to be named. In ANZ, examinations are performed through dedicated child-protection and sexual-assault services with remote peer review for rural and remote settings, and mandatory reporting applies to all doctors. In the UK, the RCPCH Child Protection Companion sets the standard, with regional child-protection medicals and mandatory reporting under safeguarding legislation. In the US, child-abuse paediatrics is a recognised sub-specialty, and theAAP and CDC set the prophylaxis and examination standards. [1] [12]
The live controversies are familiar. Who should examine the child, and how far should a non-specialist go? How wide is the forensic window, and does it differ by age and by body site? When is photo-documentation appropriate and what consent does it need? And the limits of the physical examination itself — acknowledged in the "normal to be normal" finding — are a continuing reminder that the history, the context, and the multi-agency judgement, not the exam, usually make the diagnosis. [1] [3]
Exam Pearls
EXAMINE
Other high-yield facts: examine the posterior hymenal rim between 3 and 9 o'clock; the forensic window is short and the kit never trumps resuscitation; emergency contraception options are levonorgestrel up to 72 hours, ulipristal up to 120 hours, and a copper intrauterine device up to 5 days; a prepubertal sexually transmitted infection, once vertical transmission is excluded, is highly concerning; and follow-up at two weeks and two-to-three months is where missed infections and healing findings often emerge. [12] [13]
References
- [1]Adams JA, Kellogg ND, Farst KJ, Harper NS, Palusci VJ, Frasier LD Updated Guidelines for the Medical Assessment and Care of Children Who May Have Been Sexually Abused. Journal of Pediatric and Adolescent Gynecology, 2016.PMID 26220352
- [2]Adams JA Medical evaluation of suspected child sexual abuse: 2011 update. Journal of Child Sexual Abuse, 2011.PMID 21970647
- [3]Adams JA, Harper K, Knudson S, Revilla J Examination findings in legally confirmed child sexual abuse: it's normal to be normal. Pediatrics, 1994.PMID 8065856
- [4]Berenson AB, Heger AH, Hayes JM, Bailey RK, Emans SJ Appearance of the hymen in prepubertal girls. Pediatrics, 1992.PMID 1741209
- [5]Berenson AB Appearance of the hymen at birth and one year of age: a longitudinal study. Pediatrics, 1993.PMID 8464674
- [6]Berenson AB A longitudinal study of hymenal morphology in the first 3 years of life. Pediatrics, 1995.PMID 7700746
- [7]Heger AH, Ticson L, Guerra L, Lister J, Voorhees S, Emans SJ, Muram D Appearance of the genitalia in girls selected for nonabuse: review of hymenal morphology and nonspecific findings. Journal of Pediatric and Adolescent Gynecology, 2002.PMID 11888807
- [8]Heger A, Ticson L, Velasquez O, Bernier R Children referred for possible sexual abuse: medical findings in 2384 children. Child Abuse & Neglect, 2002.PMID 12201160
- [9]Lamb ME, Orbach Y, Hershkowitz I, Esplin PW, Horowitz D A structured forensic interview protocol improves the quality and informativeness of investigative interviews with children: a review of research using the NICHD Investigative Interview Protocol. Child Abuse & Neglect, 2007.PMID 18023872
- [10]Stoltenborgh M, van Ijzendoorn MH, Euser EM, Bakermans-Kranenburg MJ A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreatment, 2011.PMID 21511741
- [11]Barth J, Bermetz L, Heim E, Trelle S, Tonia T The current prevalence of child sexual abuse worldwide: a systematic review and meta-analysis. International Journal of Public Health, 2013.PMID 23178922
- [12]Workowski KA, Bachmann LH, Chan PA Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recommendations and Reports, 2021.PMID 34292926
- [13]Gavril AR, Kellogg ND, Nair P Value of follow-up examinations of children and adolescents evaluated for sexual abuse and assault. Pediatrics, 2012.PMID 22291113
- [14]Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine, 2012.PMID 23209385