Paeds · child-safety-and-social-paediatrics
Inflicted abdominal and thoracic injury
Also known as Non-accidental abdominal trauma · Abusive visceral injury · Inflicted truncal injury · Child abuse abdominal injury · Non-accidental thoracic trauma · Hollow viscus injury from abuse · Abusive liver laceration
Fellowship-level coverage of inflicted abdominal and thoracic injury: the hidden high-specificity patterns (posterior rib fractures, duodenal and pancreatic injury), why delay and an inconsistent story matter, the AST/ALT and lipase occult-injury screen, trauma-team care running in parallel with safeguarding, and ANZ/UK/US practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A toddler arrives drowsy with a tender, rigid abdomen and a story of a short fall. The injury is real. The story is not. Inflicted abdominal and thoracic injury is blunt or, rarely, penetrating trunk trauma caused by a caregiver's assault — a kick, a punch, a squeeze, a throw, or a slam into a hard surface. The injury sits inside the body, the child often cannot speak, and the offered mechanism usually under-explains the damage. [1] [2]
Abdominal injury is the second leading cause of death from physical abuse after head injury, and it kills children because we miss it. The viscera that bear the force — liver, duodenum, pancreas, jejunum, mesentery — sit deep and quiet. Perforation may take twenty-four to forty-eight hours to declare itself as peritonitis and sepsis, by which point the child has deteriorated and the history has drifted. The thorax adds its own warning signs: rib fractures, pulmonary contusion, pneumothorax and, rarely, cardiac contusion or great-vessel injury. [1] [5] [6]
This leaf covers inflicted solid-organ, hollow-viscus, pancreatic and thoracic injury as one connected problem. Bruising, sentinel injuries, abusive head trauma and inflicted fractures live in sibling leaves — cross-link them. This page deals with the trunk cavity, the occult-injury screen, and the safeguarding interface that decides whether a child goes home. [1] [9]
Classification
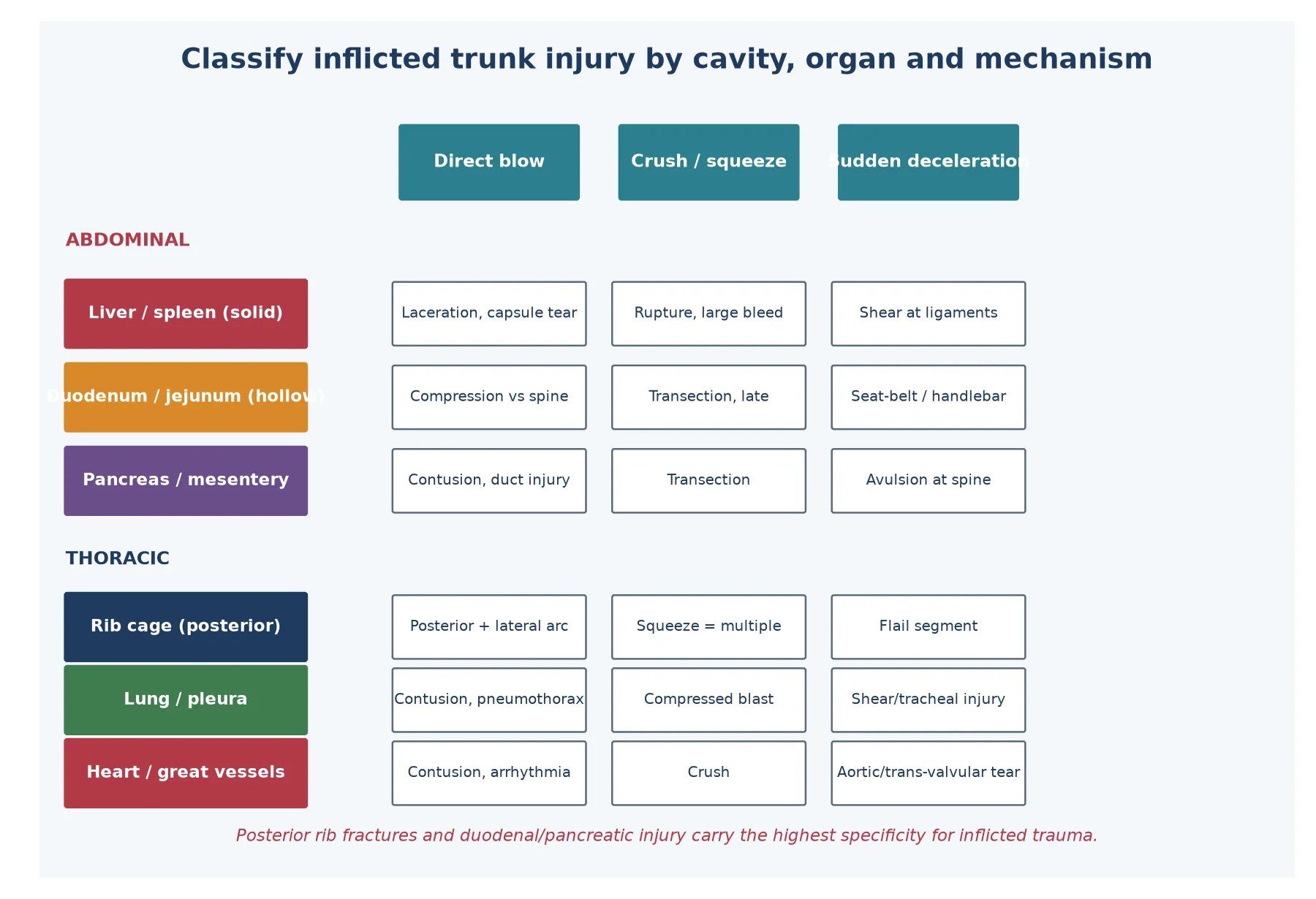
Sort inflicted trunk injury along three axes examiners will probe in turn: which cavity, which organ, and which mechanism. The cavity tells you the immediate threat (bleeding versus breathing). The organ tells you the specificity for abuse — duodenum and pancreas carry far more weight than a simple liver laceration. The mechanism tells you whether the story is even plausible. [1] [2]
Three axes that sort the case
- Abdominal: bleeding, peritonitis, sepsis
- Thoracic: breathing failure, pneumothorax, cardiac
- Both can co-exist from one assault
- Liver/spleen: common, often survivable
- Duodenum/jejunum/pancreas: high specificity for abuse
- Posterior ribs: high specificity in infants
- Direct blow: focused solid-organ injury
- Crush/squeeze: hollow-viscus transection
- Deceleration: mesenteric and shearing injury
Specificity matters because the differential includes genuine accidental trauma. A liver laceration from a clear, high-energy bicycle handlebar impact is not abuse. A duodenal transection in a non-mobile infant with no credible mechanism is abuse until shown otherwise. Hold both possibilities and let the pattern — organ plus mechanism plus history plus other injuries — decide. [2] [15]
Epidemiology & Risk Factors
Abdominal injury is uncommon in absolute terms but disproportionate in its lethality. In the United States trauma databank, children with non-accidental trauma are younger, more severely injured, and more likely to die than children with accidental injury of similar anatomical grade. The mortality gap reflects delay: abused children reach care later, sicker, and with a story that misdirects the team. [14] [5]
The risk profile is the risk profile of maltreatment generally. The child is young, pre-verbal, and developmentally unable to escape or report. The household carries the familiar drivers: intimate-partner violence, substance use, mental ill-health, social isolation, financial stress, and a caregiver who was themselves abused. A previous child-protection notification, an unexplained prior injury, or an inconsistent account of the current event should raise the threshold for acceptance, not lower it. [1] [6]
Inflicted abdominal and thoracic injury concentrates in infants and toddlers because the small trunk, thin abdominal wall, large solid organs and horizontal cartilaginous ribs transmit force directly to viscera. A school-age child reporting pain, and able to do so, shifts the presentation toward earlier presentation and accidental mechanism — but does not exclude abuse. [5] [9]
Pathophysiology
A child's trunk fails under three biomechanical loads, and the load predicts the organ. A direct blow — a punch or kick — focuses force through a thin abdominal wall onto a solid organ, lacerating liver or spleen. A crush or squeeze — an adult compressing the abdomen against the spine — pins a mobile hollow viscus, typically the duodenum or jejunum, transecting it. Sudden deceleration — a throw or a fall — generates shear at fixed points such as the ligament of Treitz and the mesenteric root, tearing bowel from its blood supply. [1] [17]
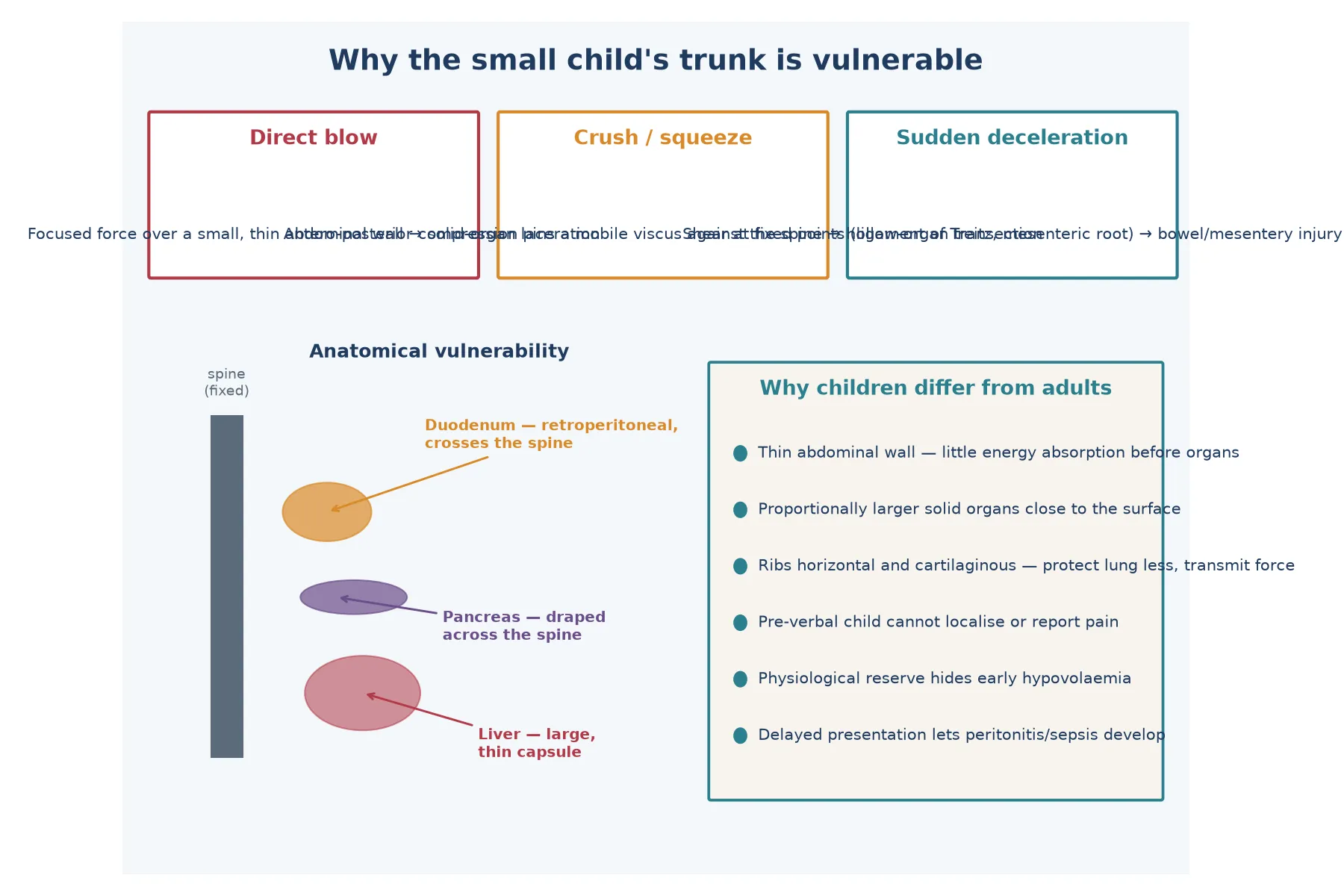
Why children differ from adults
- Little energy absorption before organs
- Force reaches the liver directly
- Duodenum crosses the spine
- Pancreas draped across it
- Crush transects at these points
- Transmits force rather than absorbing it
- Lung contusion without rib fracture is possible
- Posterior rib fractures mark squeeze/grip
The clinical consequence is latency. A liver laceration bleeds now and may shock the child within minutes. A duodenal haematoma obstructs over hours to days. A full-thickness duodenal or jejunal perforation leaks enteric contents, and peritonitis with sepsis builds over twenty-four to forty-eight hours — exactly the window in which a caregiver may attribute deterioration to a 'sudden tummy bug'. The pancreas declares itself late with rising enzymes and a pseudocyst. Recognising latency is recognising abuse. [7] [16] [18]
Clinical Presentation
Presentations divide into three. The acute collapse — shock, pallor, rigid abdomen, sometimes a witnessed assault — is the easy diagnosis and the rare one. The delayed peritonitis — a child brought in 'just getting sick' over one to three days, with abdominal distension, tenderness, vomiting and fever — is the trap; the offered history is a gastrointestinal illness and the real problem is a perforated viscus. The incidental finding — elevated transaminases, lipase or an injury seen on imaging done for another reason — is where a good screen saves a life. [1] [5] [18]
Thoracic injury adds its own patterns. An infant with respiratory distress and crepitus or a paradoxic chest may have rib fractures or a flail segment. Pulmonary contusion can progress over hours. Pneumothorax and haemothorax present with the usual signs, and a child with a cardiac contusion may develop arrhythmia — serum troponin is the screening marker. Look at the chest as carefully as the abdomen. [12] [13]
Beyond the trunk, the inflicted child often carries more: bruising in non-mobile areas, a sentinel injury, fractures of different ages, or signs of neglect. The trunk injury may be the most visible problem but is rarely the only one. Examine the whole child, and treat the trunk as the door into a full assessment. [1] [11]
Differential Diagnosis
Inflicted versus accidental trunk injury
Genuine medical mimics deserve a hearing but should not become a refuge. A bleeding disorder can bruise; it does not transect a duodenum. Osteogenesis imperfecta can fracture; it does not perforate a jejunum. Volvulus, intussusception and appendicitis cause acute abdomens but with their own time course and no extra injuries. When the pattern is discordant, the answer is a full work-up and a child-protection assessment, not a diagnostic retreat into the rare. [1] [2]
Seat-belt and handlebar injury from a real motor-vehicle or bicycle crash are the classic accidental confounders — a chance to over-call abuse. The discriminating features are a credible, witnessed, high-energy mechanism with a restraint or handlebar sign, age-appropriate reporting, and the absence of injuries of different ages. Carter and colleagues showed that even 'fall' histories conceal inflicted cases, so verify the mechanism rather than accept it. [15] [18]
Clinical & Bedside Assessment
Begin with the injury and the airway, not the suspicion. Run a structured primary survey, expose the child fully, and log-roll. Abdominal examination assesses distension, guarding, rigidity, and seatbelt or handlebar bruising. The thorax is inspected for crepitus, asymmetrical chest movement, and tenderness over ribs. Vital signs and perfusion — capillary refill, level of consciousness — quantify shock before the child decompensates. [5] [14]
The history is taken separately and carefully. Ask each caregiver independently what happened, when, who was present, and what was done afterwards. Note changing details, delay, and any account that under-explains the injury. A trauma-focused history is also a forensic history: document the words used, in quotes where possible, because the record may later support a court statement. Keep the tone neutral and factual. [1] [6]
Examine for the injuries that surround the trunk. Document every bruise and abrasion on a body map, inspect the oral cavity and ears, and look behind the tympanic membranes. Note any sentinel injury from the past — a healed fracture, an old bruise, a torn frenulum. These findings do not compete with the acute problem; they complete the picture that the abdominal injury alone cannot. [1] [11]
Investigations
Laboratory screening is the single highest-yield step after resuscitation, because it finds the injury the history concealed. Draw AST and ALT as a liver-injury screen: values above roughly 80 to 100 U/L after a concerning mechanism warrant abdominal imaging, and the ExSTRA and earlier Lindberg studies built the evidence base for this threshold. Add lipase and amylase for pancreatic injury, a full blood count and lactate for haemorrhage and perfusion, coagulation studies, and a group-and-save or crossmatch. [3] [4] [16]
Imaging is matched to stability. Bedside FAST or eFAST detects free fluid in the unstable child and directs emergency surgery, though it misses solid-organ grade and hollow-viscus injury. A haemodynamically stable child with clinical concern or an abnormal screen should have contrast-enhanced CT of the abdomen and chest, which grades solid-organ injury, identifies hollow-viscus perforation, and reveals rib and vertebral fractures that radiographs under-call. Karmazyn's comparative work confirms CT discriminates abusive from accidental patterns better than clinical assessment alone. [13] [20]
The Skeletal survey is mandatory in every child under two years with suspected physical abuse, and should be considered in older pre-verbal children; it is not optional and it should not wait for surgical clearance. Request a high-detail, two-view skeletal survey with a repeat at two weeks to reveal callus, and include oblique rib views. A chest radiograph supplements the skeletal survey for acute rib fractures. Cardiac troponin screens for cardiac contusion in significant thoracic injury. [11] [12] [19]
The screen that hides behind the obvious
Timing matters as much as the test. Hepatic transaminases fall predictably after blunt liver injury, so a high value on day one that matches a delayed presentation can itself date the injury — Baxter's enzyme-decline work underpins this. A normal early lipase does not exclude pancreatic injury if the mechanism fits; repeat it. Treat the laboratory trajectory as part of the forensic record. [8] [16]
Management — Resuscitation
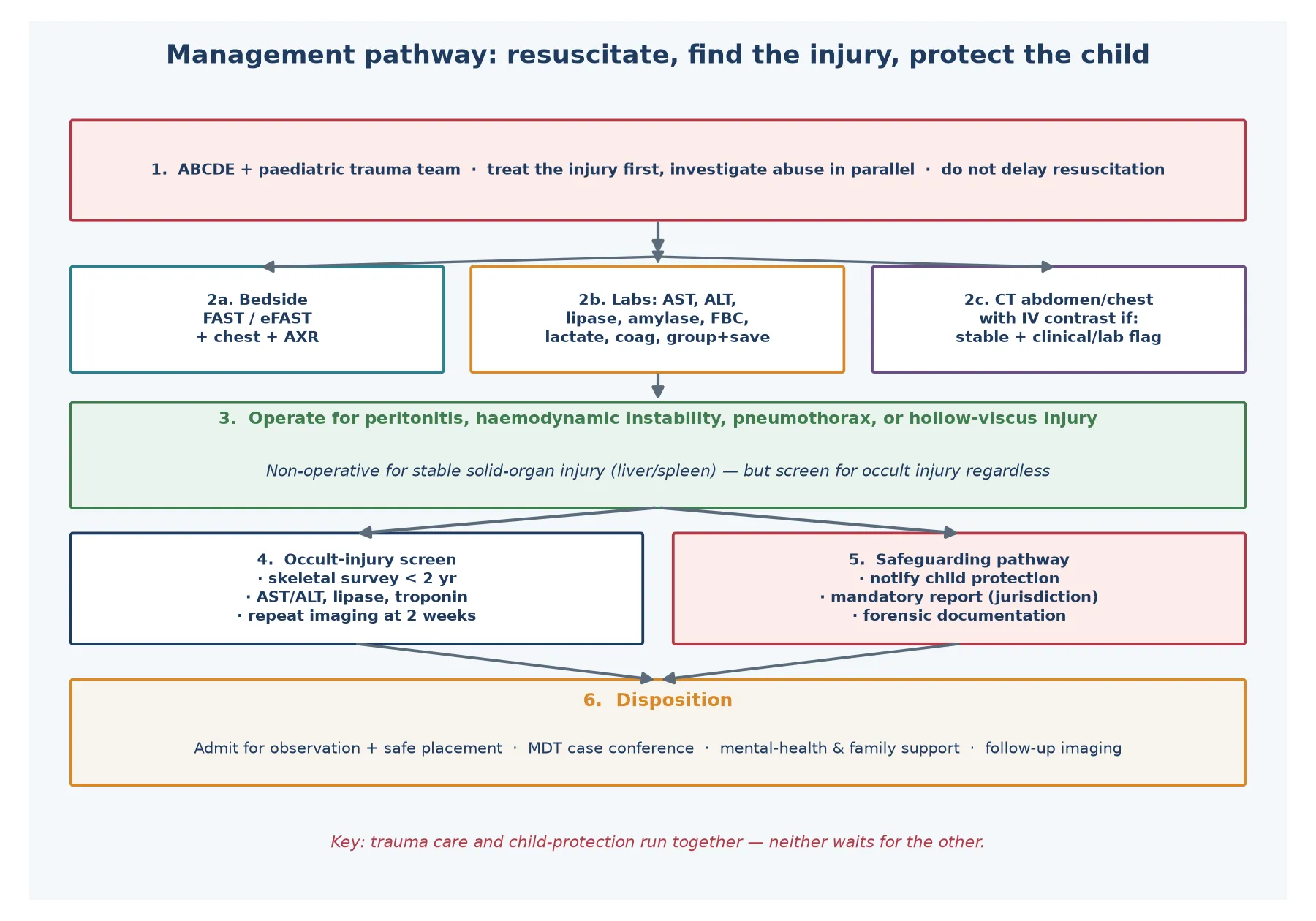
Resuscitate the injury before you investigate the abuse, and start both pathways at once. Hand the child to a paediatric trauma team, follow advanced paediatric life support, and treat airway, breathing and circulation in sequence. Obtain large-bore access, give warmed crystalloid in 10 mL/kg boluses and switch to blood early if shock persists, then titrate to perfusion and lactate. [5] [14]
A rigid abdomen with shock, or free fluid on FAST in an unstable child, is a surgical emergency: activate the operating theatre without waiting for CT. A tension pneumothorax or significant haemothorax is drained immediately. Cardiac arrest after blunt chest trauma in a child with a survivable injury may warrant resuscitative thoracotomy only in highly selected circumstances — this is a retrieval-centre decision, not a ward one. [13] [17]
Do not delay analgesia, antibiotics or blood products for forensic niceties, and do not delay safeguarding for the operating list. Notify the child-protection team while the child is being resuscitated, so that forensic documentation, photography and the multi-disciplinary response run in parallel. Trauma care and child protection are the same resuscitation, applied to the same child. [1] [6]
Management — Definitive & Stepwise
Once stable, the child follows a stepwise path. Stabilise and image. A stable child with abdominal signs or an abnormal screen has contrast CT; a stable thoracic injury has targeted chest imaging and troponin. Decide operate versus observe. Operate for peritonitis, hollow-viscus perforation, haemodynamic instability despite resuscitation, or a significant haemothorax or pneumothorax; observe the stable solid-organ liver or spleen injury with serial examination and haemoglobin. [2] [7]
Stepwise definitive care
Stabilise; image with CT (abdomen/chest) if stable, FAST if not
Screen labs: AST, ALT, lipase, tropanin, FBC, lactate, coag, group-and-save
Operate for peritonitis, perforation or instability; observe stable solid-organ injury
Occult-injury screen: skeletal survey under two years, repeat at two weeks
Activate safeguarding: child-protection team, mandatory reporting, forensic documentation
Disposition: safe placement, MDT case conference, follow-up imaging and mental-health support
Hollow-viscus and pancreatic injuries usually need surgery or interventional endoscopy. A duodenal haematoma may resolve with nasogastric decompression and nutrition, but a full-thickness perforation or transection requires repair or resection; pancreatic injury ranges from conservative management of a contusion to drainage or resection for ductal disruption, and a pseudocyst may develop weeks later. Solid-organ injury follows the modern principle of non-operative management when the child is stable and monitored. [7] [16] [17]
The safeguarding step is definitive care, not an afterthought. Once the child is stable, notify child protection, file the mandatory report required by your jurisdiction, and convene or feed into a multi-disciplinary case conference. Document injuries, photograph where indicated, and write a clear, factual medical statement. The disposition must guarantee a safe place for the child to recover — admission, alternative carer, or inpatient paediatric ward pending placement — never simply discharge to the index household. [1] [6]
Specific Subtypes & Scenarios
Liver and spleen are the commonest solid-organ injuries and the most survivable. They bleed now, declare themselves with shock and abdominal signs, and most stable injuries are managed non-operatively with serial observation. A liver laceration in an infant with a 'short fall' still demands a full abuse work-up because the mechanism, not the organ, raises the concern. [2] [8]
Duodenum and jejunum are the high-specificity hollow-viscus injuries. A duodenal haematoma presents with bilious vomiting and obstruction; a perforation or transection presents with peritonitis, often late. Sowrey's series reminds us that duodenal injury in the very young is abuse until proven otherwise — the viscus is retroperitoneal and requires real force to injure. Jejunal perforation from small-bowel trauma behaves similarly. [7] [18]
Pancreas is the great pretender. A contusion may be asymptomatic; ductal injury develops a pseudocyst over weeks; and pancreatic injury from abuse is well described in the forensic literature. Unexplained pancreatitis or a pseudocyst in a young child without a credible mechanism demands a child-protection assessment. [16]
Rib fractures and the thorax are the signature skeletal marker of trunk abuse. Posterior rib fractures, caused by an adult squeeze that levers the rib head against the transverse process, are highly specific; their positive predictive value for abuse in an infant is around 95 per cent. Pulmonary contusion, pneumothorax, haemothorax and, rarely, cardiac contusion or great-vessel injury complete the thoracic picture. Otjen's review catalogues the pearls and the pitfalls. [9] [11] [13]
Cardiopulmonary resuscitation and the rib-fracture myth
- Rib fractures are commonly caused by CPR
- Therefore rib fractures do not imply abuse
- Maguire's systematic review: CPR rib fractures are rare and usually anterior/lateral
- Posterior rib fractures remain highly specific for abuse
- CPR does not explain multiple posterior or lateral arc fractures
Cardiac contusion and commotio cordis are rarer but lethal. Serum troponin I screens for myocardial injury in significant blunt chest trauma, and a blunt blow to the precordium can produce sudden arrhythmic arrest even without structural damage — the child who survives the chest impact but arrests minutes later needs both cardiac and safeguarding assessment. [12]
Complications & Pitfalls
The first pitfall is accepting the history. A short fall, a sibling, or a 'funny turn' offered for a serious trunk injury deflects the team from imaging and screening. Anchor your thinking to the injury pattern and the occult-injury screen, not to the carer's account. [1] [15]
The second pitfall is the normal early abdomen. Perforation and pancreatic injury mature over hours to days; a soft abdomen on arrival does not exclude a transected viscus. Admit, observe, and re-examine; repeat lipase and lactate; and image when the picture evolves. Discharging a child with an evolving peritonitis because the initial examination was soft is a recurring, avoidable death. [7] [16]
Three errors that lose children
- Treating a hollow-viscus perforation as gastroenteritis for forty-eight hours. 2. Forgetting the skeletal survey in a child under two because the surgical problem dominated. 3. Discharging a stable liver laceration to the index household before the child-protection assessment was complete. [1] [7] [11]
The third pitfall is separating the surgery from the safeguarding. The operating list is not a reason to defer child-protection notification; the child-protection investigation is not a reason to defer surgery. Run both concurrently, and ensure safe placement is part of the discharge plan from the moment of admission. [1] [6]
Prognosis & Disposition
Mortality tracks severity and delay. Children with inflicted trunk injury die more often than those with accidental injury of the same grade because they present later and sicker. Survival after a stable solid-organ injury managed non-operatively is excellent; survival after a delayed perforation with septic shock is guarded and depends on the quality of retrieval, surgical and intensive care. [6] [14]
Disposition serves two goals: safe recovery and safe placement. Admit every child with a significant inflicted trunk injury, even if non-operative, for observation, occult-injury screening, and child-protection assessment. Do not discharge to the index household before the multi-disciplinary case conference agrees the destination. Arrange follow-up imaging for solid-organ healing and pancreatic pseudocyst surveillance, and link the family to mental-health and developmental support. [1] [19]
The longer-term prognosis is the prognosis of maltreatment: recurrence, developmental harm, and the mental-health sequelae of chronic trauma. A single admission is an intervention point for the whole family. Use it to connect the child and the non-offending carers to sustained support, and to close the loop with child protection and primary care. [1] [11]
Special Populations
Pre-verbal infants and toddlers are the core group. They cannot report pain, their injuries declare late, and their rib cages and viscera are anatomically vulnerable. Apply the lowest threshold for imaging, screening and skeletal survey here. [9] [11]
Children with disability and medical complexity are at elevated risk of maltreatment and may communicate pain atypically. A gastrostomy, a feeding tube or a tracheostomy adds both mechanism and diagnostic noise; interpret signs carefully and screen generously. [1]
Aboriginal and Torres Strait Islander, Māori, migrant and refugee families require culturally safe, non-stigmatising practice that does not equate disadvantage with risk. Use trained interpreters, engage Aboriginal health practitioners or cultural support workers, and recognise that colonisation, racism and intergenerational trauma shape both risk and the experience of child-protection services. [1]
Children in out-of-home care, and those in remote settings face delayed presentation and fragmented records. A child arriving from care with an unexplained injury needs a thorough, trauma-informed assessment and coordination between the agencies holding their history. Rural and remote practice compounds delay — retrieval and local safeguarding planning must start early. [1] [14]
Evidence, Guidelines & Regional Differences
The evidence base is observational and systematic-review led. Maguire's systematic review of abusive visceral injuries established the range and recognition of inflicted abdominal injury, and remains the foundational synthesis. Wood's comparison of inflicted and accidental abdominal injuries defined the discriminating clinical features, while Trokel's two studies quantified the patient and injury characteristics and the outcomes of abusive abdominal injury. [1] [2] [5] [6]
The occult-injury screen rests on the ExSTRA-era and earlier Lindberg transaminase studies, which validated AST and ALT as a liver-injury screen in suspected abuse, and on Kemp's and Maguire's systematic reviews of fracture patterns and CPR-related rib injuries. The American College of Radiology Appropriateness Criteria set the imaging standard for suspected physical abuse, including the mandatory skeletal survey under two years. [3] [4] [10] [11] [19]
Lindberg, ExSTRA network (2013)
Key finding
Hepatic transaminases are a feasible, low-risk screen for clinically occult liver injury in children evaluated for physical abuse, supporting routine AST/ALT alongside the skeletal survey.
Practice change
Draw AST and ALT on any child undergoing an abuse work-up; image when the screen is abnormal.
Regional practice differs mainly in the medico-legal frame. In Australia and New Zealand, mandatory reporting legislation, state child-protection services and the RACP Child Abuse and Neglect special interest group frame practice; the RCPCH child-protection evidence series and statutory frameworks govern the United Kingdom; and AAP and ACR guidance, together with state-level mandatory reporting, govern the United States. The clinical standard — resuscitate, image, screen, safeguard — is shared across all three. [1] [19]
The live controversy is the optimal imaging strategy. CT radiation must be weighed against the yield of occult injury; recent work continues to refine CT versus radiography for rib-fracture detection and to compare clinical and CT findings in abusive versus accidental abdominal trauma. The principle is stable: image the stable child, use FAST in the unstable child, and never omit the skeletal survey in the under-twos. [13] [20]
Exam Pearls
- Duodenum, pancreas, posterior ribs = high specificity for inflicted trauma. [1] [7]
- AST/ALT > ~80–100 U/L after a concerning mechanism = image the abdomen. [3] [4]
- Rib-fracture PPV for abuse in an infant ≈ 95%; CPR rarely causes rib fractures and not posterior ones. [9] [10]
- Peritonitis can take 24–48 hours to declare; a soft early abdomen does not exclude perforation. [7] [18]
- Skeletal survey is mandatory under two years and should be repeated at two weeks. [11] [19]
- Trauma care and safeguarding run concurrently, not sequentially — neither waits for the other. [1] [6]
- Hepatic transaminase decline can date the injury when presentation is delayed. [8]
- Troponin screens for cardiac contusion after significant blunt chest trauma. [12]
References
- [1]Maguire SA A systematic review of abusive visceral injuries in childhood--their range and recognition Child Abuse Negl, 2013.PMID 23306146
- [2]Wood J Distinguishing inflicted versus accidental abdominal injuries in young children J Trauma, 2005.PMID 16385300
- [3]Lindberg DM Utility of hepatic transaminases in children with concern for abuse Pediatrics, 2013.PMID 23319537
- [4]Lindberg D Utility of hepatic transaminases to recognize abuse in children Pediatrics, 2009.PMID 19620197
- [5]Trokel M Patient and injury characteristics in abusive abdominal injuries Pediatr Emerg Care, 2006.PMID 17047468
- [6]Trokel M Blunt abdominal injury in the young pediatric patient: child abuse and patient outcomes Child Maltreat, 2004.PMID 14871002
- [7]Sowrey L Duodenal injuries in the very young: child abuse? J Trauma Acute Care Surg, 2013.PMID 23271088
- [8]Baxter AL Hepatic enzyme decline after pediatric blunt trauma: a tool for timing child abuse? Child Abuse Negl, 2008.PMID 18945486
- [9]Barsness KA The positive predictive value of rib fractures as an indicator of nonaccidental trauma in children J Trauma, 2003.PMID 12813330
- [10]Maguire S Does cardiopulmonary resuscitation cause rib fractures in children? A systematic review Child Abuse Negl, 2006.PMID 16857258
- [11]Kemp AM Patterns of skeletal fractures in child abuse: systematic review BMJ, 2008.PMID 18832412
- [12]Bennett BL Serum Cardiac Troponin I in the Evaluation of Nonaccidental Trauma J Pediatr, 2015.PMID 26141552
- [13]Otjen JP Pearls and Pitfalls of Thoracic Manifestations of Abuse in Children Semin Ultrasound CT MR, 2022.PMID 35164910
- [14]Rosenfeld EH Understanding non-accidental trauma in the United States: A national trauma databank study J Pediatr Surg, 2020.PMID 31103270
- [15]Carter KW Pediatric abdominal injury patterns caused by falls: A comparison between nonaccidental and accidental trauma J Pediatr Surg, 2016.PMID 26850907
- [16]Callahan K The Pancreas in Child Abuse Acad Forensic Pathol, 2018.PMID 31240040
- [17]Ledbetter DJ Diagnostic and surgical implications of child abuse Arch Surg, 1988.PMID 3415461
- [18]Beckmann KR Small bowel perforation: an unusual presentation for child abuse J Am Osteopath Assoc, 2000.PMID 10979255
- [19]Wootton-Gorges SL ACR Appropriateness Criteria(®) Suspected Physical Abuse-Child J Am Coll Radiol, 2017.PMID 28473090
- [20]Karmazyn B Comparison of clinical and abdominal CT imaging findings in children evaluated for abusive and accidental abdominal trauma Emerg Radiol, 2025.PMID 39708206