Paeds · child-safety-and-social-paediatrics
Inflicted burns and scalds
Also known as Non-accidental burns · Inflicted thermal injury · Burns due to child maltreatment · NAI burns · Scald abuse
Fellowship guide to inflicted burns and scalds: pattern-based recognition of non-accidental thermal injury (immersion stocking-glove scalds, sharp demarcation, contact burns on hidden sites), the BuRN-Tool decision rule, co-existing injury assessment, the mandatory safeguarding pathway, and primary prevention with the SafeTea programme.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
Overview & Definition
Picture the eighteen-month-old brought in with a scald to both feet and lower legs that stops abruptly at a sharp line just above the ankles, like a sock pulled tight. The story is that he pulled a cup of tea over himself while standing at the coffee table. That pattern — symmetrical, sharply demarcated, no splash marks — does not fit the story, and it is an inflicted immersion scald until proven otherwise. [1]
Inflicted burns and scalds are thermal injuries caused deliberately or through wilful neglect by a carer, and they account for a meaningful and under-recognised fraction of all childhood burn presentations. They span the spectrum from a deliberate scald immersion to a contact burn from a hot implement held against the skin, to neglect allowing a child sustained access to a hazard. The unifying feature is that the injury pattern, its distribution on the body, or the history is not consistent with the stated mechanism and the developmental capability of the child. [11]
The conceptual anchor for the trainee is that the burn itself is rarely the whole story. Inflicted burns are a sentinel: a child who has been burned deliberately often has other unexplained injuries, a background of neglect, and is at high risk of further harm if returned to an unsafe environment. Your job at first contact is to recognise the pattern, document it forensically, and set the safeguarding pathway in motion — treating the burn well but never losing sight of the child behind it. [3] [6]
Classification
Inflicted burns are classified first by mechanism and then by whether the pattern is consistent with the history and the child's development. The mechanism shapes what the injury looks like and which inflicted features you search for. [1] [4]
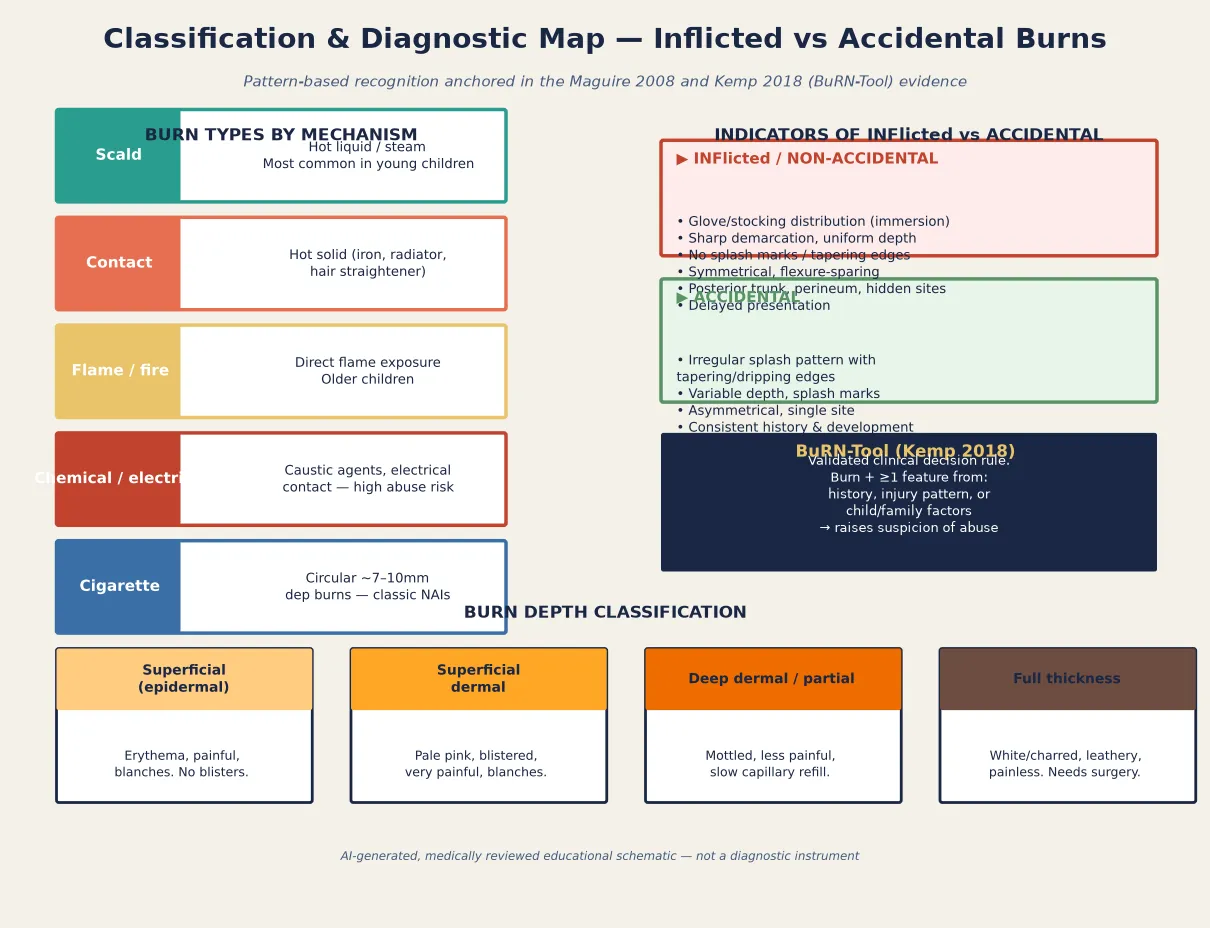
Scalds from hot liquids are the commonest burn in young children and the commonest inflicted burn. The two patterns are radically different: an accidental spill produces an irregular splash with tapering, dripping edges and superficial variable depth, while a forced immersion produces a symmetrical stocking-glove or glove distribution with a sharp upper margin and uniform depth because the child was held still in the hot liquid. [1] [12]
Contact burns from hot solids — irons, radiators, hair straighteners, and heaters — leave a sharply demarcated imprint whose shape often mirrors the offending object. A burn on the dorsum of the hand, on the perineum, or on other hidden sites is highly suspicious, as is a contact burn in a pre-mobile infant who cannot reach the object. Flame, chemical, and electrical burns are less common in abuse but carry a high index of suspicion when the pattern does not fit. [4]
A second, equally important classification is by burn depth, which drives both burn care and the interpretation of inflicted pattern. Superficial epidermal burns are erythematous and painful; superficial dermal burns are blistered, pale pink, and very painful; deep dermal and full-thickness burns are mottled or leathery and progressively less painful. The depth matters for inflicted injury because sustained forced contact produces a uniform deep burn — the depth itself is a clue when the history suggests a brief accidental exposure. [7]
Epidemiology & Risk Factors
Burns are among the commonest injuries in young children, and a proportion of these are inflicted. Estimating that proportion is difficult because inflicted burns are under-recognised and under-reported, but systematic reviews converge on the message that a substantial minority of paediatric burns presenting to health services have features of inflicted injury or neglect. [5] [11]
Headline numbers for viva
The child-level risk factors are developmental. Infants and toddlers under five are at highest risk because their skin is thinner (producing deeper burns at lower thermal energy), they are dependent on carers for all safety, and they are developmentally unable to escape or report harm. Pre-mobile infants warrant particular concern: a non-rolling, non-crawling baby cannot spill hot water on themselves, pull a kettle over, or reach a radiator, so any significant burn in this group is a red flag. [7] [11]
The family and social risk amplifiers are the same as for other forms of maltreatment: domestic violence, parental substance misuse, parental mental ill-health, social isolation, housing overcrowding, and prior child-protection involvement. These factors do not diagnose inflicted injury on their own, but they raise the index of suspicion and they shape the safeguarding plan once concern is raised. Crucially, inflicted burns co-exist with other injuries: the Pawlik study of children referred for child-abuse evaluation found that a high proportion had bruises, fractures, or other injuries in addition to the burn, which is why a full top-to-toe examination is mandatory whenever inflicted injury is suspected. [3] [5]
Pathophysiology
The severity of a thermal injury depends on the temperature of the agent, the duration of contact, and the thickness of the skin — and all three conspire against the young child in an inflicted injury. [7]
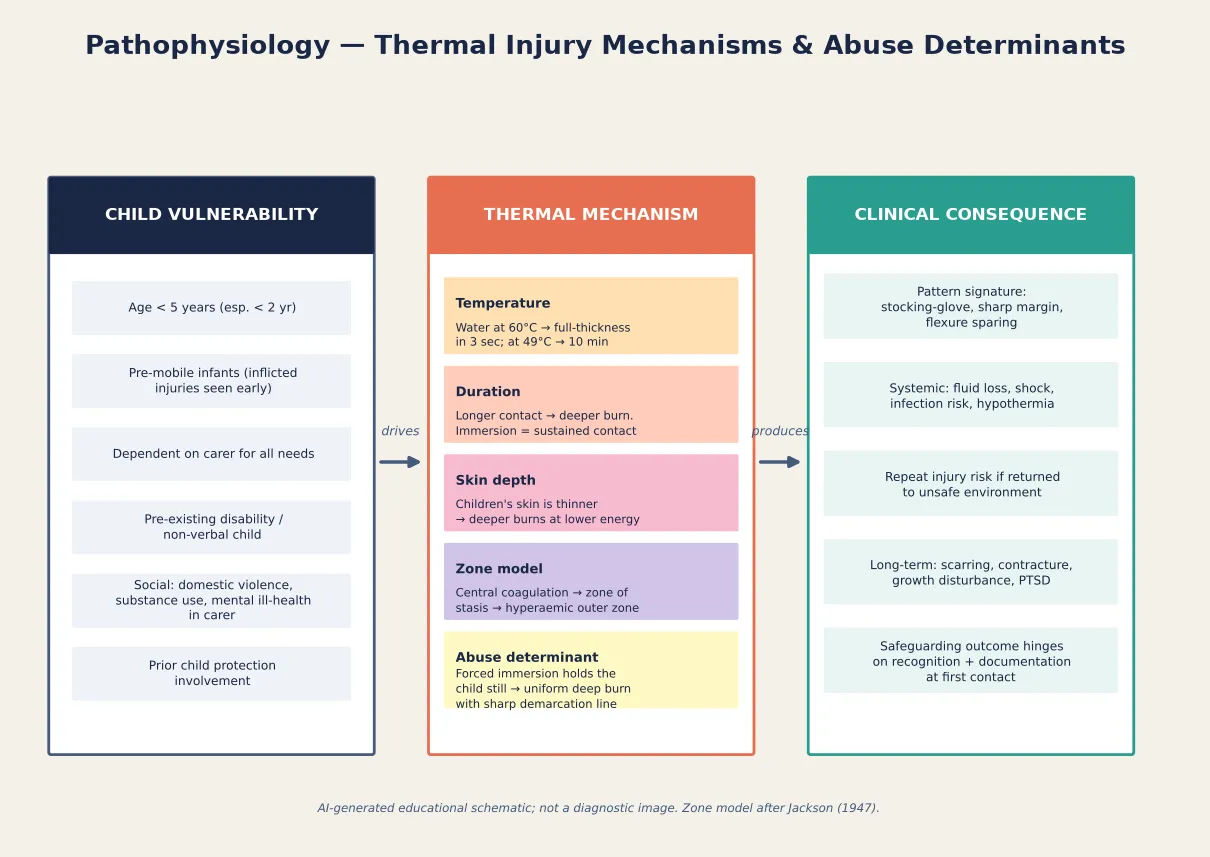
Water at 60 degrees Celsius produces a full-thickness burn in about three seconds, while at 49 degrees it takes around ten minutes. This temperature–time relationship is the scientific basis for mandatory hot-water thermostat regulations and for the interpretation of inflicted scalds: a deep, uniform scald implies sustained immersion, not a brief splash. A child's skin is considerably thinner than an adult's, so the same thermal exposure produces a deeper burn in a child — the pre-mobile infant is doubly vulnerable. [7]
Temperature \u00d7 duration \u2192 burn depth
critical
The classical Jackson's zone model describes the burn wound in three concentric zones: a central zone of coagulation (irreversibly destroyed tissue), a surrounding zone of stasis (threatened but potentially salvageable tissue where good resuscitation and cooling can limit progression), and an outer zone of hyperaemia (inflamed but recoverable tissue). Good first aid — cool running water for twenty minutes within three hours of injury — works by protecting the zone of stasis and limiting deepening, which is why it is both a first-aid measure and an evidence-based intervention. [7] [9]
For inflicted injury, the mechanism translates directly into the recognisable pattern. A forced immersion holds the child motionless in hot water, so the entire exposed area receives a uniform sustained exposure, producing a deep burn with a sharp fluid-level margin and no splash marks — the stocking-glove signature. By contrast, a cup of tea spilling produces droplet and splash marks with tapering edges because the contact is brief and the liquid runs off. The pathophysiology is the diagnostic vocabulary: when you can read the mechanism off the pattern, you can test the history against it. [1] [12]
Clinical Presentation
The child with an inflicted burn usually presents because the burn itself needs attention, not because anyone has declared abuse. Your task is to recognise, in the pattern and the story, that this burn does not fit — and to do so before the child is dressed and discharged. [11]
The immersion scald is the archetype. Look for a symmetrical stocking-glove distribution on the feet and lower legs or the hands and forearms, with a sharp, clear upper margin at a consistent height — the fluid level. There are no splash marks, no tapering edges, and the depth is uniform because the limb was held still. Flexure creases may be spared where the skin was folded or protected against itself, producing clear-cut sparing lines that are themselves a clue to sustained positioning. [1]
Accidental spill
Hot drink pulled over
- Irregular splash pattern with tapering, dripping edges
- Variable depth — shallow where liquid ran off quickly
- Splash marks on nearby skin or clothing
- Asymmetric, single area, face or upper trunk common
Inflicted immersion
Held in hot water
- Symmetrical stocking-glove or glove distribution
- Sharp fluid-level margin, uniform depth
- No splash marks, flexure-sparing lines
- Feet/hands dominant; posterior or perineal involvement
Inflicted contact
Hot object pressed
- Sharply demarcated imprint mirroring the object
- Uniform deep depth from sustained pressure
- Dorsum of hand, perineum, hidden sites
- Pre-mobile infant who cannot reach the object
The inflicted contact burn leaves a sharply demarcated imprint that often mirrors the hot object — the triangular base of an iron, the bar of a hair straightener, the grid of a heater. The depth is uniform because sustained pressure was applied, and the site is often somewhere the child would not naturally press themselves against: the dorsum of the hand, the buttocks, the perineum, or the posterior trunk. A circular burn roughly seven to ten millimetres across is consistent with a cigarette and is a classic inflicted-injury sign. [4] [6]
The presentation must be read against the child's developmental stage, which is the single most powerful discriminator. A six-month-old infant cannot pull a kettle from a worktop, turn on a hot tap, or climb to a radiator, so any burn in a pre-mobile child that implies voluntary reaching or climbing is developmentally implausible. Document the child's developmental milestones explicitly alongside the burn description — the gap between what the history requires and what the child can do is the core diagnostic finding. [2] [11]
Differential Diagnosis
The differential for a suspected inflicted burn has three layers: genuine accidental burns whose pattern actually fits the history, skin conditions that mimic burns, and inflicted injury that you must not miss. Build the differential explicitly so that you neither over-call a plausible accidental burn nor dismiss a sentinel. [1] [6]
| What you see | Do not stop here | Must still do |
|---|---|---|
| 'Spilled a cup of tea' | Check the pattern — is it a splash with tapering edges, or a sharp-margin immersion? | Map the burn; test the history against the developmental stage and pattern |
| 'Turned on the hot tap' | Tap-water scalds can be accidental or inflicted — check for stocking-glove pattern | Ask about water temperature; examine for co-existing injuries |
| Blistering rash on a mobile toddler | Could be impetigo, bullous impetigo, or a phytophotodermatitis mimicking a burn | Dermatology review if pattern is atypical; do not assume abuse or accident without full assessment |
| 'Leant against a heater' | A single contact burn may fit — but check site, depth, and developmental plausibility | Full top-to-toe exam for co-existing injuries; document the imprint shape |
| Multiple burns of different ages | This is not a single accident — repeated injury is a sentinel | Safeguarding referral, skeletal survey, strategy discussion today |
Genuine accidental scalds from hot drinks are the commonest burn in under-fives and usually produce a characteristic irregular pattern with splash marks and tapering edges over the face, upper trunk, or arm — consistent with a cup pulled or knocked over. Tap-water scalds can be accidental (a child turning on a hot tap) or inflicted (forced immersion), and the pattern distinguishes them: the Titus study of accidental sink scalds showed a splash-and-drip pattern unlike the sharp immersion line. [12]
Skin mimics include bullous impetigo, staphylococcal scalded skin syndrome, phytophotodermatitis (linoleic-acid plant sap plus sunlight producing streaky blistering), and cultural practices such as cupping or moxibustion, which can produce circular marks that worry clinicians. These mimics do not explain stocking-glove immersion scalds or contact imprints, and where there is genuine diagnostic uncertainty a dermatology or burns-team opinion is appropriate — but uncertainty is never a reason to skip the safeguarding referral when the index of suspicion is high. [1] [11]
Clinical & Bedside Assessment
The bedside assessment has two parallel goals: assess and treat the burn, and assess and document the safeguarding concern. Both must happen at the same encounter, because the first presentation is often the only chance to capture the pattern and the history before they change. [2] [6]
Begin with the burn itself: estimate the total body surface area using an age-appropriate Lund-Browder chart (children's head proportions differ from adults), assess the depth at each site, and identify any features suggesting inhalational injury if the mechanism involved fire or smoke in an enclosed space. Provide adequate analgesia before any examination or dressing, because a child in pain cannot cooperate with a careful assessment and an under-examined burn is an under-documented one. [7] [13]
The physical examination is a full top-to-toe and head-to-skin assessment, not just the burn. Look for co-existing injuries — bruises of different ages, fractures, older scars or burns, and signs of neglect such as severe dental caries or failure to thrive — because inflicted burns frequently travel with other injuries. The Pawlik study found a high rate of co-existent injury in children referred for child-abuse burn evaluation, which is why a single-system examination is a safeguarding error. Examine the genitalia, perineum, posterior trunk, and hidden sites explicitly and document the findings. [3]
Photograph the injury at presentation, with consent and with a measuring ruler in frame, because the burn will evolve and the pattern is most interpretable early. Record the body sites, the distribution, the depth, the presence or absence of splash marks, and any demarcation lines in the medical record in objective, non-leading language — this documentation may become evidence in legal proceedings, so write it as a clinician describing what you see, not as an advocate. [6] [11]
Investigations
Investigations serve two purposes: to support the medical and surgical management of the burn, and to look for occult injury that confirms or refutes safeguarding concern. The strategy is driven by the level of concern, not applied reflexively to every burn. [6]
The investigation pathway when inflicted injury is suspected
Confirm the burn assessment — %TBSA via Lund-Browder, depth at each site, photograph with consent and ruler.
Bloods for burn management and occult injury: full blood count, coagulation, and consider a bleeding screen if bruising is present.
Skeletal survey for any child under two years, or any non-mobile infant, when inflicted injury is suspected — look for occult fractures of different ages.
Consider a CT head if there is any neurological concern, and urinalysis if abdominal or renal injury is possible.
Swab the burn for microbiology if infection is suspected; consider toxicology if substance exposure is possible.
Convene a strategy discussion with social care, police, and the safeguarding team to agree further investigations and the safe disposition.
The skeletal survey is a core investigation in suspected inflicted burns in children under two. Its purpose is to detect occult fractures — particularly rib fractures, metaphyseal corner fractures, and fractures of different ages — that indicate additional inflicted injury and reshape the safeguarding risk. The survey should be performed to a standard protocol and, where concern persists, repeated at around two weeks to capture fractures that were not visible acutely. [6]
Blood tests support both the burn (baseline haemoglobin and coagulation before any surgical intervention) and the safeguarding assessment (a coagulation and platelet screen where bruising co-exists, to characterise any bleeding tendency). Neuroimaging is indicated when there is any concern about inflicted head injury — a drowsy, irritable, or neurologically abnormal child with a burn must not be assumed to be simply in pain. [3] [13]
Management — Resuscitation
The immediate priority is the same as for any serious burn: secure the airway, support breathing and circulation, and give adequate analgesia — but with the safeguarding pathway running in parallel from the moment suspicion is raised. [7] [13]
Assess the airway first: facial burns, soot, or stridor after an enclosed-space fire mandate early anaesthetic review and a low threshold for intubation before oedema obliterates the airway. Estimate the percentage TBSA of partial- and full-thickness burns using the Lund-Browder chart, and commence fluid resuscitation according to your local burns protocol for burns meeting the threshold — children have proportionally larger heads and different fluid requirements than adults, so use a paediatric formula and titrate to urine output. Keep the child warm; hypothermia deepens the zone of stasis and worsens the burn, and small children lose heat rapidly through a large wound. [7] [13]
Give adequate opioid analgesia early, titrated to a validated pain score, because undertreated pain compounds the child's distress and undermines cooperation with examination. Apply cool running water for twenty minutes if the injury occurred within three hours — this is evidence-based first aid that limits burn progression — but do not use ice, and do not immerse a large-area burn in cold water, which precipitates hypothermia. [9] [7]
Management — Definitive & Stepwise
Once the child is physiologically stable and the burn has been assessed and documented, definitive management is stepped and safeguarding-centred: local wound care and surgical decision-making proceed alongside the mandatory child-protection process, and the two tracks do not wait for each other. [6] [2]
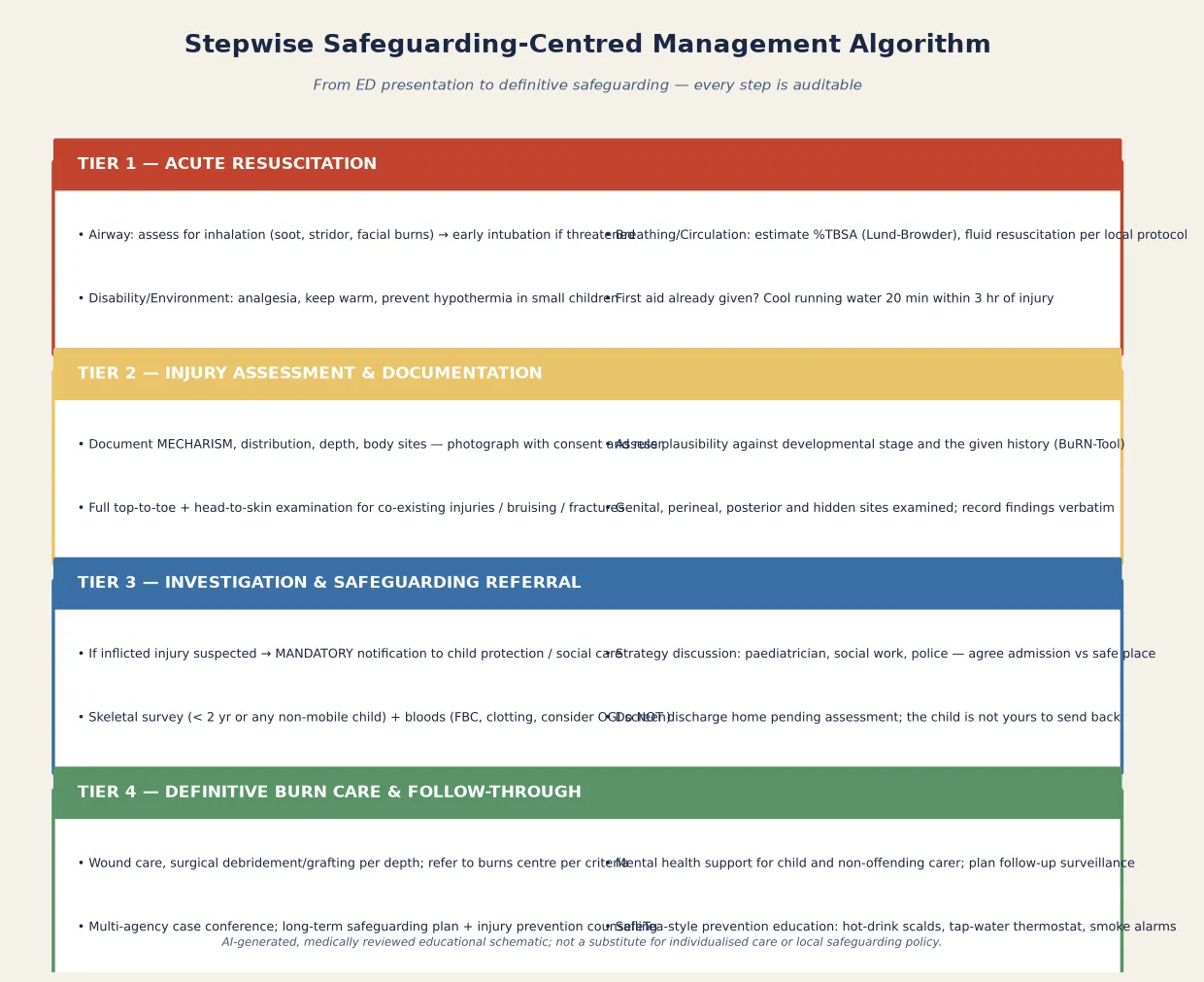
The four-step safeguarding-centred pathway
Resuscitate: airway, breathing, circulation, analgesia, cooling, warming — the burn track.
Assess and document: %TBSA, depth, sites, pattern, photograph, history verbatim, full top-to-toe exam — the evidence track.
Raise concern and refer: apply the BuRN-Tool, notify child protection or social care, convene a strategy discussion — the safeguarding track.
Definitive care and follow-through: wound care or surgery, mental-health support, multi-agency case conference, prevention counselling — the recovery track.
Raising and objectifying suspicion is structured with the BuRN-Tool, the validated clinical decision rule derived and tested by Kemp and colleagues. It combines features of the history, the injury pattern, and child or family factors to flag burns that warrant a child-protection response, and the Johnson acceptability study confirmed that frontline clinicians find it usable in practice. The tool does not replace clinical judgement, but it gives you a defensible, evidence-based basis for escalating concern — which matters when the family is pressing to go home. [2] [8]
Local wound care follows standard burns principles: clean the wound, debride loose non-viable skin, apply an appropriate dressing, and review depth at forty-eight to seventy-two hours because burns can deepen. Deep dermal and full-thickness burns, and burns meeting local criteria for area or site, require referral to a specialist burns centre. Surgical debridement and skin grafting are planned according to depth and site, and splinting and physiotherapy are started early to prevent contracture across joints. [7] [13]
The safeguarding track is mandatory and time-critical. When inflicted injury is suspected, you must notify your designated child-protection lead or social care — the duty is statutory in ANZ, the UK, and North America and it overrides ordinary confidentiality. A strategy discussion brings together paediatrics, social work, and police to agree whether the child is admitted to a place of safety, discharged to a safe carer, or removed from the home, and to coordinate further investigation. The child is not yours to send home while safeguarding assessment is incomplete. [6] [11]
Kemp 2018 — BuRN-Tool derivation and validation (PMID 28918905)
Multicentre UK prospective derivation and validation study of features associated with child maltreatment in burns.
Key finding
The BuRN-Tool combines history, injury-pattern, and child/family features to identify burns with a high probability of maltreatment, providing a structured, evidence-based trigger for child-protection referral.
Practice change
Use the tool to objectify and defend your decision to escalate safeguarding concern in a busy emergency setting.
Specific Subtypes & Scenarios
The immersion scald in a pre-mobile infant is the highest-stakes scenario. An infant who cannot yet stand, walk, or reach cannot immerse their own feet in hot water, so a stocking-glove scald in this age group is inflicted until proven otherwise. Admit the infant, photograph the pattern, perform a skeletal survey, and convene a strategy discussion the same day. [1] [6]
Contact burns from hair straighteners and irons are a common presentation and can be accidental in a mobile toddler who touches a hot device. The discriminator is the site and the developmental plausibility: a burn on the dorsum of the hand or the palm of a pre-mobile infant, or a deep uniform imprint suggesting sustained pressure rather than a brief reflexive pull-away, raises concern. Johnson's prospective study of non-scald burns mapped the agents and mechanisms and identified the inflicted features that distinguish them. [4]
Neglect as a mechanism is under-recognised relative to deliberate infliction. A burn that arises because a carer left a young child unattended near a known hazard, failed to supervise bath water temperature, or delayed seeking medical care for a significant burn is a safeguarding concern even when no one 'held' the child in the hot water. Chester and colleagues argued that the field's focus on deliberate infliction risks neglecting the equally harmful pattern of neglect, and neglect is the commonest confirmed category of child maltreatment in burn series. [5]
Children with disabilities and non-verbal children are at higher risk of inflicted injury and may be unable to report what happened. Reliance on carer history is greater and the scope for an unrecognised pattern is wider, so a low threshold for full assessment and safeguarding referral is essential. The developmental baseline and the carer's account of the child's capabilities must be documented explicitly. [11] [3]
Complications & Pitfalls
The complications of inflicted burns are both physical and situational. Physically, a deep burn risks scarring, contracture across joints, growth disturbance, infection, and the systemic consequences of a large-area injury. Situationaly, the greatest harm comes from missed recognition: a child whose inflicted burn is dressed and discharged returns to the unsafe environment and is at risk of further, sometimes fatal, injury. [3] [11]
The largest pitfall is explaining away the pattern — accepting a plausible-sounding history without testing it against the burn and the child's development. A cup-of-tea story is easy to tell and easy to accept, but a stocking-glove scald with a sharp margin is not a cup-of-tea burn. The BuRN-Tool exists precisely to make this testing structured and defensible. [2] [1]
Explaining away
- Accepting a history without testing it against the pattern
- Missing the stocking-glove immersion signature
- Assuming a mobile-toddler story fits a pre-mobile infant
- Dressing and discharging without a strategy discussion
Incomplete exam
- Examining only the burn, not the whole child
- Missing co-existing bruises or fractures
- Not examining hidden or genital sites
- Forgetting the skeletal survey in the under-twos
Documentation failure
- No photograph with consent and ruler
- Paraphrasing rather than recording the history verbatim
- Using leading or accusatory language
- Not noting discrepancies between informants
Safeguarding delay
- Waiting for the burn to heal before referring
- Forgetting the mandatory-notification duty
- Sending the child home pending assessment
- Not convening a strategy discussion the same day
The opposite pitfall is over-calling a plausible accidental burn as inflicted, which causes serious harm to a family and erodes trust. Most childhood burns are genuinely accidental, and the task is to discriminate accurately using the pattern, the developmental plausibility, the co-existing-injury assessment, and the BuRN-Tool — not to assume abuse by default. Where the index of suspicion is genuinely uncertain, a senior clinician and the safeguarding team should be involved early rather than the decision resting on a single junior assessment. [1] [8]
A further pitfall is poor documentation. If the case proceeds to legal proceedings, the medical record is central evidence; vague, delayed, or leading notes undermine both the child's protection and a fair process. Photograph with consent, write objectively and contemporaneously, record the history in the informant's own words, and note discrepancies explicitly — these habits protect the child and the integrity of the process. [6] [11]
Prognosis & Disposition
The physical prognosis of an inflicted burn depends on its depth, site, and area, and follows standard burn-care principles: superficial burns heal without scarring, deeper burns scar and may contract, and burns across joints require splinting, physiotherapy, and sometimes surgery. The safeguarding prognosis depends on whether the inflicted nature was recognised and acted upon at first contact. [7] [3]
Disposition is driven by safeguarding, not by the burn alone. A child with suspected inflicted injury is admitted to a place of safety — usually the paediatric ward under consultant supervision — while the strategy discussion, investigations, and social-care assessment proceed. The child is not discharged home until the multidisciplinary team is satisfied that the home environment is safe or that an alternative safe carer is identified. [6] [11]
Long-term follow-up addresses both the burn and the child's wider welfare. Burn follow-up manages scarring, contracture, and growth; safeguarding follow-up, coordinated through a multi-agency case conference, maintains a child-protection plan, supports the non-offending carer, and monitors for repeat injury. Mental-health support for the child and family is part of the plan, because the psychological consequences of inflicted injury are substantial and persistent. [3] [11]
Special Populations
Pre-mobile infants warrant the highest index of suspicion. Any significant burn in an infant who cannot yet reach, pull, climb, or turn on a tap is inflicted or neglectful until proven otherwise, because the developmental capability implied by most accidental histories is simply absent. Admit, investigate, and refer. [6] [11]
Children with disabilities and non-verbal children are at elevated risk of all forms of maltreatment, including inflicted burns, and are less able to disclose. The assessment relies more heavily on the pattern, the physical examination, and the carer's account of the child's capabilities, and the threshold for full safeguarding assessment should be correspondingly low. Document the child's developmental baseline explicitly. [11] [3]
Children in out-of-home care and those known to child protection have a documented background of risk, and a burn in this group warrants particular scrutiny of the supervision environment and the mechanism — not because carers are presumed guilty, but because the baseline risk is higher and the safeguarding net must hold. [5]
Indigenous, migrant, refugee, and socioeconomically disadvantaged families experience higher rates of both accidental and inflicted burns, driven by housing conditions (overcrowding, shared bathing facilities, absent thermostatic mixing valves), reduced access to safety equipment, and cumulative social stress. Engaging Indigenous health workers and interpreters, understanding the family's living conditions, and framing prevention within the family's reality improves both recognition and care. Rural and remote children may present later and face transfer for definitive care, which compounds the safeguarding timeline. [9] [11]
Evidence, Guidelines & Regional Differences
The inflicted-burn pattern is universal, but the safeguarding framework, the mandatory-reporting law, and the prevention infrastructure differ by region. Name the framework you are operating in and carry the differences explicitly into the exam. [6] [2]
| Region | Safeguarding framework | Mandatory reporting | Prevention infrastructure |
|---|---|---|---|
| ANZ | State child-protection services; RACPCH-style guidance via RACP | Mandatory for all professionals in all states | Hot-water thermostat regulations; smoke-alarm programmes |
| UK (RCPCH / NHS) | Working Together to Safeguard Children; local safeguarding partnerships | Statutory duty for all professionals | SafeTea national scald-prevention campaign; LFDs |
| US (AAP / ACGME) | State CPS; CAPTA framework | Mandatory in all states for all professionals | Hot-water heater thermostat limits; burns-centre network |
| Canada / RCPSC | Provincial child welfare; duty-to-report legislation | Mandatory in all provinces | Thermostatic mixing valves; public-health campaigns |
The evidence backbone is a set of studies you should be able to name. The Maguire 2008 systematic review is the definitive synthesis of features distinguishing intentional from accidental scalds. The Kemp 2018 BuRN-Tool provides the validated clinical decision rule for raising maltreatment suspicion from a burn, with the Johnson 2016 acceptability study confirming its usability. The Pawlik 2016 study characterised co-existent injuries in referred children, and the Johnson 2017 study mapped non-scald burn mechanisms. The Gasteratos 2023 systematic review is the contemporary overview of paediatric nonaccidental burns. [1] [2] [3] [4] [11]
The prevention evidence is anchored by the SafeTea programme — a multimedia campaign to prevent hot-drink scalds in young children and promote correct burn first aid — evaluated in the Bennett feasibility and Cowley process-evaluation studies. SafeTea demonstrates that targeted, parent-facing prevention works at the population level, which is why prevention counselling is part of the management of every burn presentation, inflicted or accidental. [9] [10]
Exam Pearls
When the examiner asks what you will do for a toddler with a scald whose pattern does not fit the story, the answer is not "apply a dressing" — it is "recognise the inflicted pattern, assess and document the burn and the whole child, apply the BuRN-Tool, notify child protection and convene a strategy discussion, admit to a place of safety, investigate with a skeletal survey, and run the burn-care and safeguarding tracks in parallel." That is the fellowship answer. [2] [6]
References
- [1]Maguire S, Moynihan S, Mann M, et al. A systematic review of the features that indicate intentional scalds in children. Burns, 2008.PMID 18538478
- [2]Kemp AM, Hollén L, Emond AM, et al. Raising suspicion of maltreatment from burns: Derivation and validation of the BuRN-Tool. Burns, 2018.PMID 28918905
- [3]Pawlik MC, Kemp A, Maguire S, et al. Children with burns referred for child abuse evaluation: Burn characteristics and co-existent injuries. Child Abuse Negl, 2016.PMID 27088728
- [4]Johnson EL, Maguire S, Hollén LI, et al. Agents, mechanisms and clinical features of non-scald burns in children: A prospective UK study. Burns, 2017.PMID 28645715
- [5]Chester DL, Jose RM, Aldlyami E, et al. Non-accidental burns in children--are we neglecting neglect? Burns, 2006.PMID 16448766
- [6]Peck MD, Priolo-Kapel D Child abuse by burning: a review of the literature and an algorithm for medical investigations. J Trauma, 2002.PMID 12435962
- [7]Hettiaratchy S, Dziewulski P ABC of burns: pathophysiology and types of burns. BMJ, 2004.PMID 15191982
- [8]Johnson EL, Hollén LI, Kemp AM, et al. Exploring the acceptability of a clinical decision rule to identify paediatric burns due to child abuse or neglect. Emerg Med J, 2016.PMID 27068866
- [9]Cowley LE, Bennett CV, Brown I, et al. Mixed-methods process evaluation of SafeTea: a multimedia campaign to prevent hot drink scalds in young children and promote burn first aid. Inj Prev, 2021.PMID 33093127
- [10]Bennett CV, Hollén L, Quinn-Scoggins HD, et al. Feasibility of Safe-Tea: a parent-targeted intervention to prevent hot drink scalds in preschool children. Inj Prev, 2020.PMID 30765457
- [11]Gasteratos K, McCarthy M, Chatziathanasiou D, et al. A Systematic Review of Pediatric Nonaccidental Burns: Protecting the Children Through Knowledge, Vigilance, and Prevention. Ann Plast Surg, 2023.PMID 37157138
- [12]Titus MO, Baxter AL, Starling SP Accidental scald burns in sinks. Pediatrics, 2003.PMID 12563095
- [13]Popowicz P, Regan A, Hotwagner DT Burn Fluid Resuscitation. StatPearls, 2026.PMID 30480960