Paeds · clinical-assessment-and-reasoning
Care of children with medical complexity and technology dependence
Also known as Children with medical complexity · CMC · Technology-dependent children · Complex chronic conditions · Pediatric medical complexity algorithm · PMCA · Complex care · Medical home for CMC
Fellowship approach to children with medical complexity and technology dependence: Cohen and Kuo definitions, PMCA and CCC identification tools, baseline-aware assessment, device versus disease deterioration, emergency care plans, care coordination, caregiver support, discharge, transition and exam-ready reasoning.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a school-age child who lives with a tracheostomy, overnight home ventilation, a gastrostomy and five specialty clinics. The family knows the usual colour, usual secretions and usual smile. Tonight the child is quieter, secretions are thicker, and the ventilator is alarming. That child is not “a bit complex for the ED.” That child is the centre of a whole care system, and your job is to recognise medical complexity, protect life-supporting technology, and coordinate what happens next. [1]
Children with medical complexity (CMC) are a subset of children with special health care needs. Cohen and colleagues framed CMC around four linked domains: chronic conditions that are often multi-system, functional limitations that are often severe and may need technology, high health-care use across settings, and substantial family-identified service needs. Kuo and the AAP Council on Children with Disabilities then gave clinicians a practical recognition-and-management report: identify complexity early, partner with families, build care coordination, and plan across the life course. [1]
Technology dependence means the child needs a medical device to compensate for loss of a vital body function, and interruption of that technology can cause serious harm or death. Common classes include airway and ventilation supports, enteral or parenteral nutrition access, vascular access, renal replacement, cerebrospinal fluid shunts and continuous monitoring. Not every CMC child is technology-dependent, and not every technology-dependent child has the same functional profile — but the acute risk profile changes the moment a device can fail. [1]
State a problem representation the way you would hand over on the phone: age and diagnoses that matter today; personal baseline; devices and settings; what changed; whether the threat looks like disease, device failure or both; what the emergency care plan says; and what help you need now. [1]
Classification
Start with clinical domains, then place identification algorithms beside them — not instead of them. [1]
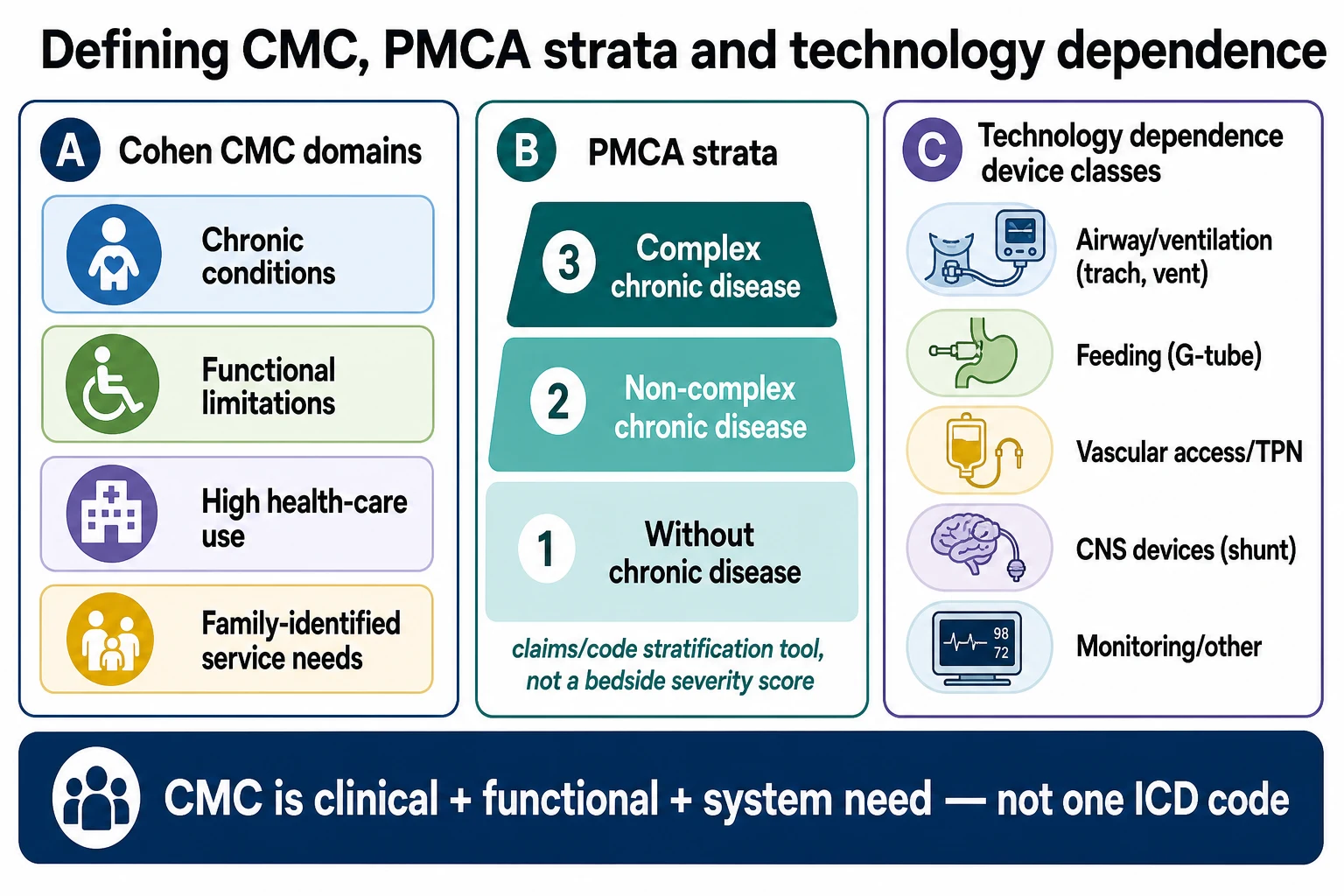
Cohen CMC domains (clinical framing). Chronic condition(s); functional limitation; health-care use; family-identified need. A child can sit high on one domain and lower on another. The examiner wants you to use the domains to organise history, not as a checkbox quiz. [1]
PMCA (Pediatric Medical Complexity Algorithm). Simon and colleagues developed PMCA to stratify children into three groups using administrative data: complex chronic disease, non-complex chronic disease, and without chronic disease. Later versions refined codes and validation (including version 3.0). Use PMCA for population identification and service design. Do not quote it as a bedside severity score or invent its full code tables from memory. [1]
Feudtner complex chronic conditions (CCC). CCC classification identifies children with chronic conditions expected to last at least 12 months (unless death intervenes) and to involve several different organ systems or one system severely enough to require specialty paediatric care and probably some period of hospitalisation. Version 2 updated ICD-10 mapping and explicitly strengthened categories for complex medical technology dependence and transplantation. Version 3 continues system refinement for contemporary data. CCC is a research and health-services tool; translate it into “this child has multi-system chronic disease with or without technology” at the bedside. [1]
Related but non-identical labels. [1]
CSHCN
Broad umbrella
- Chronic physical, developmental, behavioural or emotional condition
- Above-average health service need
- Includes milder chronic disease
- Not all are CMC
CMC
Highest complexity subset
- Multi-domain Cohen framing
- Often multi-specialty and multi-setting care
- High family care burden
- May or may not use life-supporting devices
Technology dependence
Device-critical subset
- Device replaces or supports a vital function
- Interruption can be immediately dangerous
- Needs emergency plan and supply chain
- Acute differential always includes device failure
An emergency care plan (sometimes part of a shared plan of care) is a living document that names diagnoses that matter in a crisis, baseline vitals and interaction, devices and settings, allergies, resuscitation and ceiling-of-care discussions if relevant, preferred hospital, and who to call. A discharge summary is a past event. An emergency plan is a future action script. [1]
Epidemiology & Risk Factors
CMC are a small fraction of children but a large and growing share of hospital resource use. In a longitudinal study of 28 US children’s hospitals, Berry and colleagues showed substantial inpatient growth and resource concentration among children with chronic and complex disease patterns — the clinical implication is that every general paediatrician will meet these children in ED, ward and clinic, not only tertiary complex-care teams. [1]
Risk of unplanned care rises with multi-system disease, technology dependence, recent hospital discharge, polypharmacy, fragmented specialty care, limited home nursing, rural distance, language barriers and caregiver strain. Kuo’s national caregiver profile among more medically complex children with special health care needs documented high care burden, employment and financial strain, and care coordination load carried by families. Bayer and colleagues later profiled elevated mental-health needs among parents of CMC. Home-health access is uneven; Medicaid analyses show variable utilisation rather than universal continuous skilled nursing. COVID-era service disruption amplified access gaps for many CMC families. [1]
Inequity matters. Families facing socioeconomic disadvantage, racism, or discrimination when staff treat complexity as “always like this” can experience delayed escalation. Cook’s commentary on discriminating against children with medical complexity is a warning for viva culture: complexity is never a reason to listen less. [1]
Pathophysiology
CMC physiology is the story of reduced reserve plus interacting systems. A neuromuscular or genetic condition may limit cough, swallow and chest wall movement. Chronic lung disease or aspiration loads the work of breathing. Cardiac or autonomic disease changes perfusion responses. Seizure disorders and sedating polypharmacy blunt protective responses. Infection, constipation with autonomic crisis, dehydration through a failed feed, or adrenal stress can tip a compensated child quickly. [1]
Devices change the failure modes. A blocked or dislodged tracheostomy produces sudden airway obstruction. A disconnected ventilator circuit produces hypoventilation. A failed feed pump or displaced gastrostomy produces missed hydration, missed medicines and metabolic instability. A central-line infection can progress with muted early signs. Barton and colleagues described real-world home device workarounds — adaptations families invent when equipment, training or supply systems fail. Workarounds can keep a child alive at home, and they can also hide unsafe practice that needs redesign, not blame. [1]
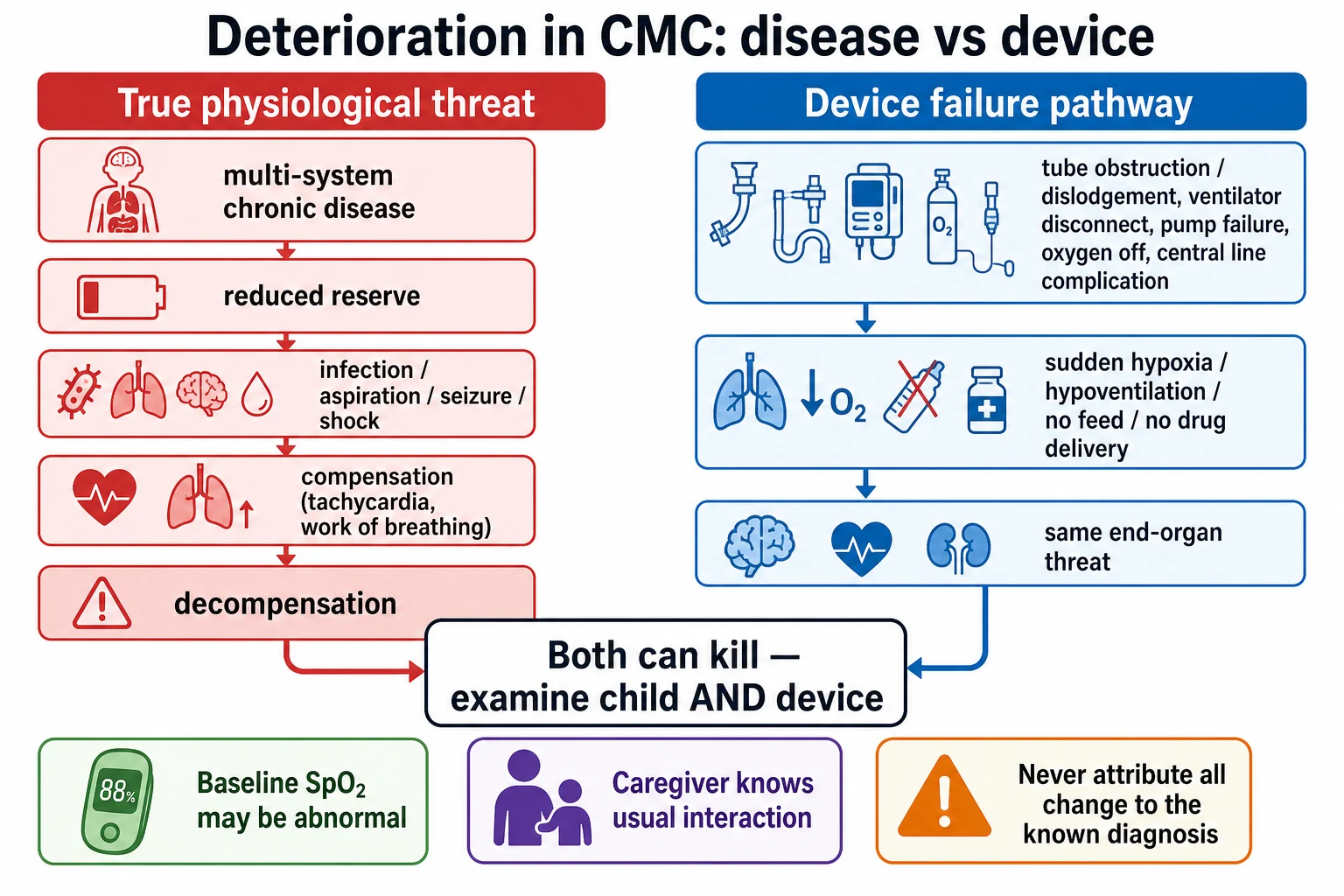
Diagnostic overshadowing is the cognitive error of attributing every new symptom to the known diagnosis. The nonverbal child with a ventriculoperitoneal shunt and vomiting may have constipation — or rising intracranial pressure. The child with “always noisy breathing” may now have a blocked tube. Pathophysiology and reasoning fail together when you stop looking for a second process. [1]
Clinical Presentation
CMC present across the whole system: planned clinic reviews, school health crises, home-care escalation, ED visits, ward admissions and PICU step-downs. The most useful early signal is often change from baseline, not a dramatic new number. Caregivers may say the child is less interactive, secretions smell different, seizures cluster, urine is darker through the nappy, or the ventilator is “working harder.” Families of hospitalised CMC describe safety risks when staff do not listen to that baseline knowledge. [1]
Age shapes the picture. Neonates and ex-preterm graduates may enter technology dependence after NICU survival with feeding tubes, oxygen or monitoring. Infants show colour change, poor feed tolerance and apnoea risk. Toddlers add mobility hazards around tubes. School-age children may have emergency plans at school that staff have never read. Adolescents may hide distress, negotiate autonomy over device care, or face mental-health crises while still technology-dependent. [1]
Device alarms and workarounds are presentations too. Repeated “nuisance” alarms, taped connectors, unofficial adapters, or a parent who never leaves the bedside because no one else can troubleshoot the ventilator are clinical findings about system fragility. [1]
Differential Diagnosis
When a CMC child looks worse, sort by immediate threat and reversibility, not by which specialty owns the clinic letter. [1]
- Airway/device: tracheostomy obstruction, accidental decannulation, circuit disconnect, oxygen failure, severe secretions. [1]
- Breathing: aspiration, pneumonia, atelectasis, fatigue on chronic support, pneumothorax. [1]
- Circulation: sepsis (including line sepsis), dehydration, cardiomyopathy, autonomic instability, bleeding. [1]
- Neurology: seizure cluster, shunt failure, encephalopathy, medication toxicity. [1]
- Abdomen/feeds: tube displacement, obstruction, volvulus risk in some surgical anatomies, constipation crisis, feed intolerance. [1]
- Medicines: missed doses through failed enteral access, polypharmacy interaction, withdrawal. [1]
- Safeguarding and environment: injury, neglect of device care, caregiver collapse — complexity does not exclude maltreatment. [1]
“Known complex child with a viral illness” is a temporary working label, not a final diagnosis, until you have excluded device failure and other can’t-miss threats. [1]
Clinical & Bedside Assessment
Begin with safety and baseline. Ask: what does usual look like for colour, SpO2, ventilator settings, seizure frequency, interaction and feeds? Ask what is different today. Ask what the caregiver is most worried about. Read the emergency care plan if one exists — and if it does not, that absence is itself a problem to fix before discharge. [1]
Run ABCDE with technology: [1]
- Airway: native airway or tracheostomy? Tube size, ties, spare tube, suction. Look for obstruction or dislodgement. [1]
- Breathing: effort, chest movement, ventilator alarms, oxygen source, secretions. Compare SpO2 to this child’s baseline, not only to a pink-child chart. [1]
- Circulation: perfusion, heart rate, blood pressure if available, line sites, fluid status through feeds and urine. [1]
- Disability: interaction versus baseline, seizures, pupils if shunt concerns, glucose if indicated. [1]
- Exposure: skin under devices, pressure injuries, abdomen around gastrostomy, temperature. [1]
Complete a technology inventory at the bedside: each device, indication, settings, last change date if known, power supply, spare parts, and who is competent to troubleshoot. Examine with dignity — positioning aids, time, and communication supports. Use professional interpreters when language is a barrier; do not default to siblings. [1]
Investigations
First reverse threats. Do not delay airway rescue or oxygen for a blood test. Then choose tests that change management. [1]
Often useful early: glucose; blood gas when respiratory or perfusion threat is real; electrolytes if feed failure or polypharmacy; cultures and inflammatory markers when infection is plausible, especially with central lines; targeted imaging only if the child is stable enough for transfer or imaging comes to the child. Device interrogation and equipment checks are investigations too. [1]
Interpret against baseline. A “normal” SpO2 of 98% may be impossible or undesirable for some cyanotic or chronic lung phenotypes; a “normal” sodium may hide dehydration if the child usually runs lower. “Normal for age” is not always “normal for this child.” [1]
Low-value or harmful patterns: indiscriminate full panels on every presentation; sending an unstable technology-dependent child to remote radiology without airway-capable escort; repeating radiation without a decision question; treating PMCA/CCC assignment as if it were a diagnostic test. [1]
Management — Resuscitation
If the child is peri-arrest or a critical device has failed, call for help and treat what you see. Follow local paediatric advanced life support while protecting or replacing the artificial airway. For suspected tracheostomy obstruction, the practical sequence is oxygen, suction, remove inner cannula if present, attempt to pass a suction catheter, and if the tube is blocked or dislodged, replace with the same size or one size smaller using the emergency kit — exact institutional algorithms and training standards sit in airway topics and local policy; your job in general paediatrics is to start, not freeze. [1]
Use the caregiver as a skilled partner: “Show me the usual settings. Show me how you bag if the ventilator fails.” That is not abdication; it is using expertise in the room while you lead the medical response. Follow the emergency care plan for preferred interventions and goals. Escalate MET, PICU or retrieval when needs exceed local capability. Document device settings before and after changes. Check immediately reversible threats: disconnection, obstruction, empty oxygen, hypoglycaemia, seizure, tension physiology. [1]
Management — Definitive & Stepwise
After the first threat is controlled, build the longitudinal system the AAP report and medical-home literature describe. [1]
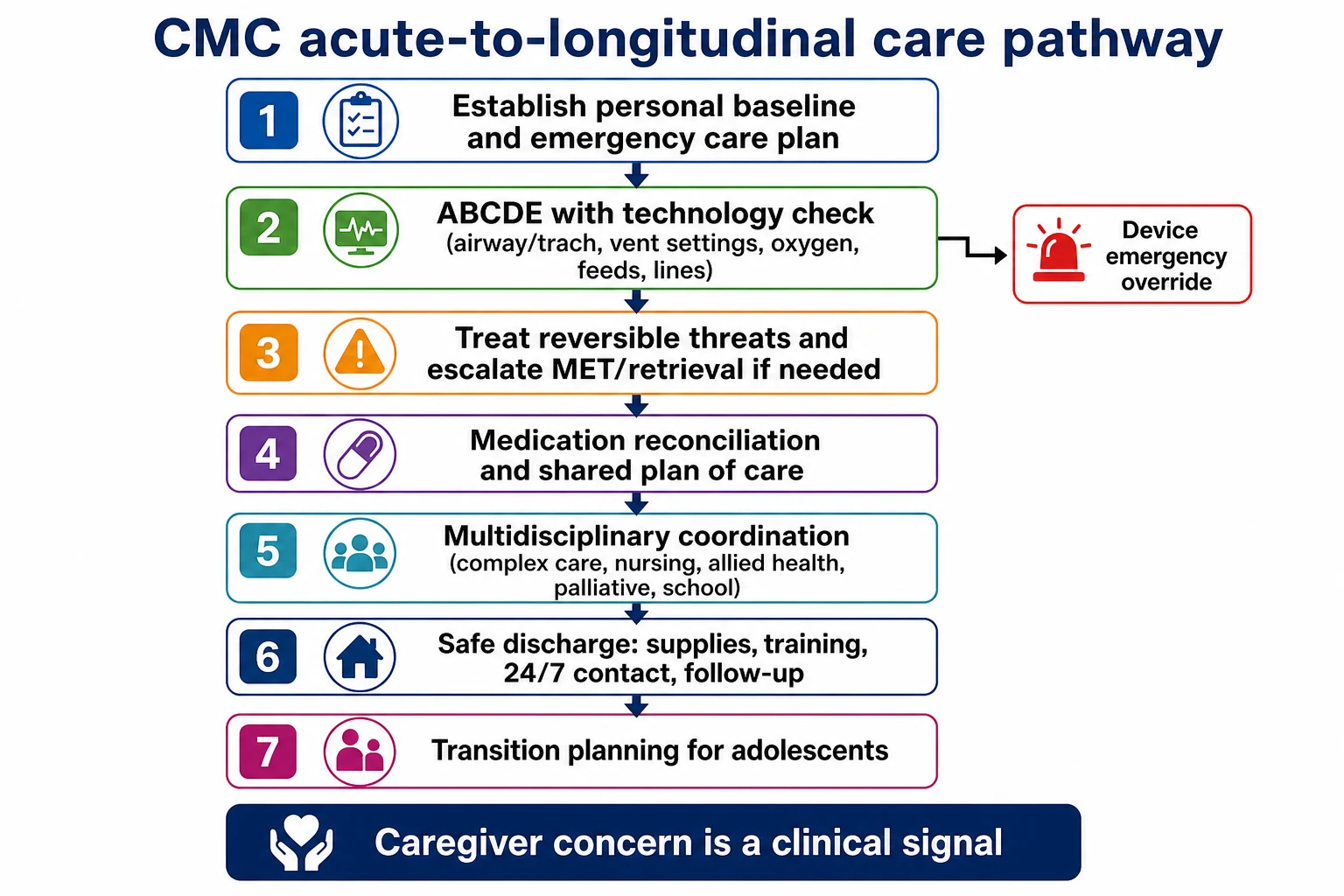
1. Shared plan of care and emergency plan. One living document that families and clinicians can actually use. Update after every major admission. [1]
2. Medication reconciliation. Polypharmacy is common and risky. Feinstein’s work on safer polypharmacy for CMC emphasises structured review, indication checking, and harm reduction rather than endless additions. Reconcile hospital, home and clinic lists every transition. [1]
3. Care coordination. de Banate and colleagues summarise coordination as the deliberate organisation of patient care activities between participants — including the family — to facilitate appropriate delivery of health care services. In practice that means a named coordinator or clinic, proactive scheduling, after-visit summaries families can use, and closed-loop referrals. Complex care programmes are one model; the medical home remains the conceptual core. [1]
4. Multidisciplinary team. General paediatrics, nursing, respiratory, dietetics, speech, physiotherapy, occupational therapy, pharmacy, social work, palliative care when appropriate, education supports and primary care. Who leads? Usually a clearly identified paediatric medical home clinician with authority to prioritise. [1]
5. Handoffs. Starmer’s multicentre handoff programme reduced medical errors and preventable adverse events after structured I-PASS implementation. CMC care is multi-team care; unstructured “they’re complex, see the notes” is an error mode. [1]
6. Discharge and home readiness. Training completed and assessed; supplies for a defined period; power and oxygen plans; 24/7 contact pathway; follow-up appointments that fit family logistics; school or respite plan if relevant. Home health is not automatically present — Sobotka’s Medicaid analysis reminds examiners that utilisation is limited and uneven. Do not discharge into an empty skill set. [1]
7. Transition. From mid-adolescence, plan adult providers, device suppliers, legal decision-making, insurance or funding interfaces, and goals of care. Transition failure is a predictable safety event for technology-dependent young people. [1]
Specific Subtypes & Scenarios
Tracheostomy ± home ventilation. Always carry the emergency kit. Separate tube problems from lung problems. Practice bagging via stoma. [1]
Enteral tube displacement. Stop feeds if dislodged; do not use a newly replaced tube for medicines or feeds until position is confirmed per local protocol. Plan hydration and drug route alternatives. [1]
Central line fever / TPN dependence. Treat as possible line infection until proven otherwise; involve senior and infectious diseases early; protect the line while assessing other sources. [1]
Shunt concerns in neurodisability. Vomiting, irritability, sunsetting, or new seizures need shunt-aware assessment — not automatic attribution to “baseline reflux.” [1]
ED, near-baseline vitals, high caregiver concern. Escalate evaluation. Families detect change earlier than strangers. [1]
Polypharmacy adverse effect. New sedation, arrhythmia risk, serotonin signs, or constipation crisis after a medication change — review the list before adding another drug. [1]
Rural family with thin home nursing. Disposition must match real capability, retrieval geography and supply chains, not an urban ideal. [1]
Caregiver mental-health crisis. Treat caregiver collapse as a child-safety issue requiring urgent social supports and a safe care plan. [1]
“Always complex” discrimination. If staff delay because the child “lives like this,” reframe: what is different from this child’s baseline today? [1]
Transition clinic. Map adult respiratory, gastroenterology, primary care, equipment vendors and emergency department orientation before the paediatric exit. [1]
Complications & Pitfalls
Other traps: ignoring caregiver expertise; missing device workarounds that signal system failure; incomplete medication reconciliation; losing the emergency plan at handover; assuming continuous home nursing exists; using family as sole interpreter; overlooking safeguarding; discharging without supplies or training; and treating complexity as a reason for lower, not higher, listening. [1]
Prognosis & Disposition
Outcomes that matter include survival, function, comfort, school participation, unplanned hospital days, and family wellbeing — not only procedure counts. Disposition follows capability: ward observation when stable and needs are met; HDU/ICU or retrieval when airway, ventilation, perfusion or nursing intensity exceeds the ward; home only when training, equipment, power, medicines and escalation routes are real. Goals-of-care and palliative partnership can sit alongside active treatment; they are not opposites. Safety-net advice should name specific return features for this child and this device set. [1]
Special Populations
Neonates leaving NICU need meticulous caregiver training and early community linkage. Children with severe neurological impairment need baseline interaction descriptions in the notes. Immunocompromised CMC may declare infection late. Indigenous and migrant families need culturally safe care and professional interpreters. Out-of-home care complicates consent and history. Socioeconomic disadvantage multiplies missed appointments and supply gaps. Adolescents need privacy, mental-health screening and transition work even when parents still run the ventilator. [1]
Evidence, Guidelines & Regional Differences
Kuo 2016 (PMID 27940731). AAP clinical report on recognition and management of medical complexity — identify CMC, partner with families, coordinate care, address needs across settings and the life course. This is the core guideline-level reference for the leaf. [1]
Cohen 2011. Operational clinical/research definition of CMC domains that still organises teaching and service design. [1]
PMCA (Simon 2014; v3 2018). Validated administrative stratification into complex chronic, non-complex chronic, and without chronic disease. [1]
CCC (Feudtner v2; Feinstein v3). Classification systems for multi-system chronic disease, with v2 strengthening technology dependence and transplantation categories. [1]
Berry 2013. Inpatient growth and resource concentration in children’s hospitals — why CMC care is core general paediatrics. [1]
Caregiver evidence. Kuo 2011 caregiver challenges; Bayer 2021 parental mental health; Mauskar 2023 family safety voice in hospital. Quote direction of findings; do not invent precise percentages you have not verified in the paper in front of you. [1]
Handoffs. Starmer I-PASS programme reduced medical errors — directly relevant to multi-team CMC. [1]
Regional practice. ANZ candidates work within state complex-care clinics, retrieval networks and disability funding interfaces (for example NDIS in Australia) — name them as system context and verify local eligibility rules rather than inventing them. UK practice interfaces with NHS complex/continuing care and NICE guidance on integrated services for severe complex needs. US practice uses medical-home and CSHCN frameworks with highly variable Medicaid home health. Canadian practice is described in national CMC commentaries with provincial home-care differences. Bedside device emergencies are universal; funding packages are local. [1]
ANZ: Lead with baseline-aware ABCDE, emergency care plan, and capability-matched disposition via local retrieval. Document NDIS or disability-support interfaces as care coordination facts after verifying the child’s actual package — never invent entitlements in an exam answer. [1] UK: Integrate community children’s nursing and named consultant care; use NICE complex-needs service organisation principles for multi-agency planning. [1] US/Canada: Anchor on medical-home language, PMCA/CCC population tools for systems answers, and explicit home-health variability. [1]
Exam Pearls
- Long-case spine: baseline → current threat → ABCDE with technology → investigations that change care → coordination → family impact → disposition/transition. [1]
- Short-case: show the devices, state tube sizes/settings if known, and compare findings to baseline. [1]
- Never claim a mortality reduction for complex-care programmes you cannot cite. Claim what the papers show: recognition frameworks, utilisation patterns, caregiver burden, handoff safety, polypharmacy risk. [1]
- Polypharmacy review is a safety intervention, not optional paperwork. [1]
- Discrimination and overshadowing are examiner favourites because they are common and fixable. [1]
COMPLEX care for CMC
References
- [1]Kuo, Dennis Z Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [2]Cohen, Eyal Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics, 2011.PMID 21339266
- [3]Simon, Tamara D Pediatric medical complexity algorithm: a new method to stratify children by medical complexity. Pediatrics, 2014.PMID 24819580
- [4]Simon, Tamara D Development and Validation of the Pediatric Medical Complexity Algorithm (PMCA) Version 3.0. Academic pediatrics, 2018.PMID 29496546
- [5]Feudtner, Chris Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC pediatrics, 2014.PMID 25102958
- [6]Feinstein, James A Pediatric Complex Chronic Condition System Version 3. JAMA network open, 2024.PMID 39008301
- [7]Berry, Jay G Inpatient growth and resource use in 28 children's hospitals: a longitudinal, multi-institutional study. JAMA pediatrics, 2013.PMID 23266509
- [8]Kuo, Dennis Z A national profile of caregiver challenges among more medically complex children with special health care needs. Archives of pediatrics & adolescent medicine, 2011.PMID 22065182
- [9]Cohen, Eyal Status Complexicus? The Emergence of Pediatric Complex Care. Pediatrics, 2018.PMID 29496971
- [10]Kuo, Dennis Z The Medical Home for Children with Medical Complexity: Back to Basics. The Journal of pediatrics, 2019.PMID 30553538
- [11]Dewan, Tammie Children with medical complexity in Canada. Paediatrics & child health, 2013.PMID 24497777
- [12]de Banate, Maria A Care coordination for children with medical complexity. Current opinion in pediatrics, 2019.PMID 31290774
- [13]Natesan, Sujit Technology-Dependent Children. Emergency medicine clinics of North America, 2021.PMID 34215407
- [14]Barton, Hannah J Medical Device Workarounds in Providing Care for Children With Medical Complexity in the Home. Pediatrics, 2021.PMID 33926988
- [15]Bayer, Nathaniel D A National Mental Health Profile of Parents of Children With Medical Complexity. Pediatrics, 2021.PMID 34155129
- [16]Starmer, Amy J Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [17]Feinstein, James A Making Polypharmacy Safer for Children with Medical Complexity. The Journal of pediatrics, 2023.PMID 36252865
- [18]Cook, Stefanie Discriminating Against Children With Medical Complexity. Pediatrics, 2023.PMID 37357723
- [19]Sobotka, Sarah A Home Health Care Utilization in Children With Medicaid. Pediatrics, 2022.PMID 35028664
- [20]Mauskar, Sangeeta In their own words: Safety and quality perspectives from families of hospitalized children with medical complexity. Journal of hospital medicine, 2023.PMID 37559415