Paeds · clinical-assessment-and-reasoning
Handover, referral and consultation in paediatrics
Also known as Paediatric handover · I-PASS handoff · ISBAR referral · Clinical consultation paediatrics · Interhospital transfer communication
A fellowship approach to paediatric handover, specialty consultation, written and verbal referral, closed-loop communication and transfer of clinical information using I-PASS and ISBAR from neonate to transition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
You are about to leave the ward. Another doctor must keep this child safe with only the story you pass across. That story is the handover (also called handoff). It is not a polite summary. It is a safety procedure. [1] [7]
A referral asks another service to take ongoing responsibility or to see the child for a defined problem. A consultation asks for advice or a specific action while you usually keep overall care. A closed-loop exchange means the receiver restates the critical content and the sender confirms it. Read-back is the short form of that loop for orders and numbers. [17] [20]
Picture a 14-month-old with bronchiolitis who looks quieter after high-flow oxygen. If you only say “stable on the ward,” the night team may miss that effort is falling. If you say the illness severity, the if-then plan and who owns the next blood gas, they can act before collapse. That is why structure matters. [1] [12]
What good communication does
Preserve severity
State how sick the child is now and the direction of travel.
Preserve actions
Name what must be done, by whom, and by when.
Preserve contingencies
Say what you fear next and what to do if it happens.
Confirm understanding
Require receiver synthesis, not a silent nod.
Match the record
Make verbal and written handoffs agree.
Classification
Not every information transfer is the same job. A night shift handoff moves many patients between similar teams. An ED-to-ward admission moves one child into a new system. A surgical consult asks a focused question. A retrieval call must package acuity, capability and logistics. Use the tool that fits the job. [7] [8]
I-PASS is built for team handoffs. I = illness severity. P = patient summary. A = action list. S = situation awareness and contingency planning. S = synthesis by receiver. The last S is the safety valve: the receiver restates the plan in their own words. [1] [2]
ISBAR (or SBAR with an explicit Identify step) is built for focused calls. I = who you are and where you are. S = the situation and urgency. B = background. A = your assessment. R = the recommendation or request. Australian services spread ISBAR for clear telephone communication. [20] [21]
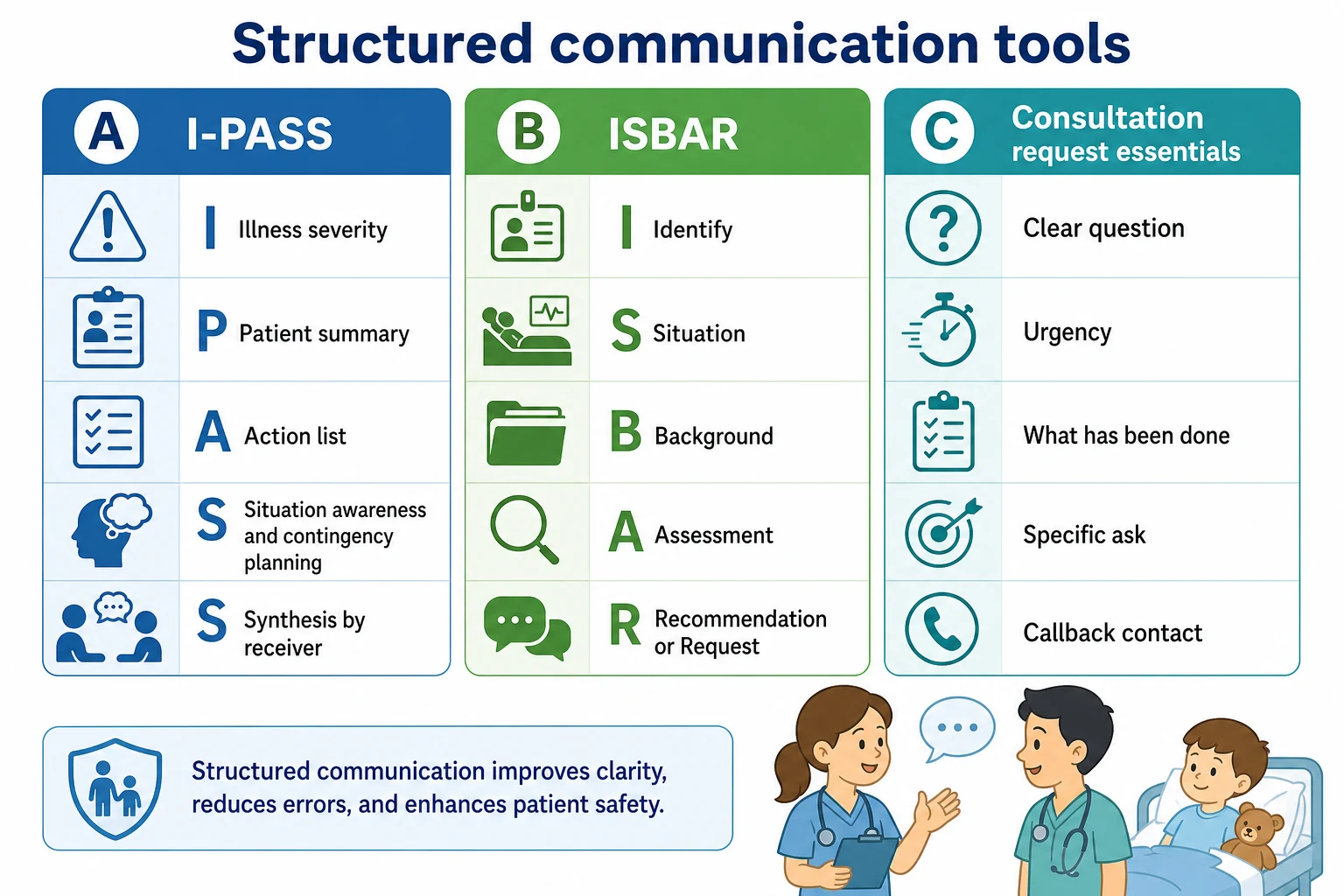
Read the figure like this: if your call has no question and no callback number, it is not a consult. If your handoff has no contingency and no synthesis, it is a monologue. [1] [20]
Handover / handoff
Transfer of responsibility
- Shift, unit or service change
- Needs severity and contingency
- Receiver must synthesise
- Verbal plus matched written record
Consultation
Advice or specific action
- Clear clinical question
- Urgency stated
- You often keep ownership
- Callback path required
Referral
Request for ongoing care
- Defined problem and goal
- Relevant history and results
- Social and access context
- Safety-net until seen
Closed-loop talk
Confirm critical content
- Order or plan stated
- Receiver read-back
- Sender confirms
- Essential in resuscitation
Receiver-driven handoff invites questions and checks understanding. Sender-driven monologue dumps data and hopes it sticks. ED receiver-driven models reduce miscommunication when the receiving team leads clarification. [5]
Epidemiology & Risk Factors
Miscommunication is a leading source of serious medical error. In a nine-hospital paediatric resident handoff programme, medical errors fell from 24.5 to 18.8 per 100 admissions (about 23%). Preventable adverse events fell from 4.7 to 3.3 per 100 admissions (about 30%). Written and oral key elements improved without harming workflow. [1]
Later multicentre work spread I-PASS across diverse specialties and hospital types. Nursing I-PASS bundles improved communication quality. ED and transport adaptations show the same idea travels when local coaching supports it. [2] [4] [8] [9]
Communication-related safety events still cluster where complexity, night work and fragmented teams meet. Characterisation work in a paediatric quaternary hospital keeps this visible for quality teams. [18]
Child risk
- Medical complexity and devices
- Neonates on transport
- Rapidly changing physiology
- Multiple teams at once
Team risk
- Interruptions and fatigue
- Hierarchy silence
- Unstructured narrative
- No receiver synthesis
System risk
- Variable written templates
- Night staffing
- Rural distance and retrieval lag
- Electronic data dumps
Equity risk
- Language discordance
- No professional interpreter
- Discounted caregiver concern
- Fragmented out-of-home care historians
Family-centered communication programmes can cut harmful errors even when overall error counts move less. In seven North American paediatric units, harmful errors fell about 38% after a coproduced family-centered rounds communication package, and family engagement rose. [3]
Pathophysiology
Children compensate, then fall. The receiving team needs the trajectory, not only the last number. If illness severity and contingency plans are missing, the first abnormal page looks surprising when it was predictable. [1] [12]
Working memory is small. Interruptions, pagers and long unstructured stories overload it. Critical items drop: allergies, weight-based plans, pending cultures, “if work of breathing rises start X and call Y.” The failure is cognitive and system-level, not moral. [18] [19]
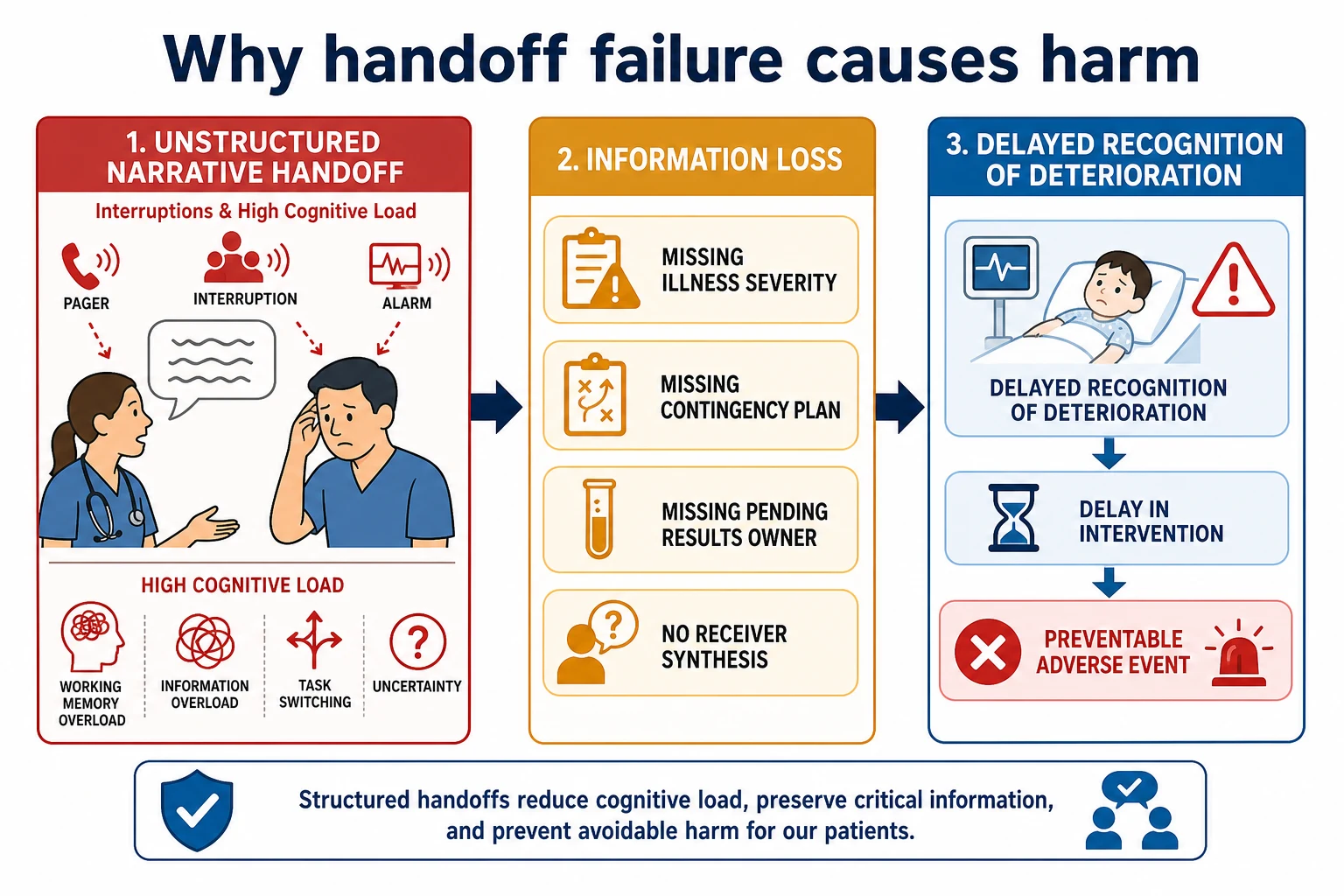
Read the figure like this: structure is not bureaucracy. It is a way to protect the few facts that keep a compensating child safe overnight. [1]
During resuscitation the same mechanism is faster. Ambiguous orders become wrong doses or delayed defibrillation. Standardised closed-loop communication creates a shared mental model under noise. [17]
For complex and technology-dependent children, missing baseline and device data is a special path to harm. The new team may treat chronic findings as acute, or miss a failing ventilator circuit because the personal plan never transferred. [14] [15]
Clinical Presentation
A strong handoff sounds organised and short enough to hold. Severity comes first. The summary uses age, baseline, tempo and key features. Actions are concrete. Contingencies use if-then language. The receiver talks back. [1]
A weak handoff sounds like a list of overnight tasks with the word “stable” repeated. Allergies appear late or never. Pending results have no owner. Nobody asks a question. The written sheet contradicts the spoken story. [19]
Caregiver concern is a clinical finding. If a parent says the child is not themselves, put that sentence into the handoff even when the score looks mild. Prospective hospital data link caregiver concern with critical illness. [12]
A weak consult call sounds like: “Can you see this kid?” A strong call sounds like: “I am the paediatric registrar in ED. I have a 6-year-old with focal peritonism after 24 hours of pain. I think they need urgent surgical review for possible appendicitis. Ultrasound is pending. Can you review within 30 minutes? My number is…” [20] [21]
Differential Diagnosis
Not every messy transition is a “communication problem” alone. Sometimes the real issue is unnamed diagnostic uncertainty. Say “working diagnosis viral illness, but I have not excluded evolving sepsis” rather than forcing false certainty. [7]
Sometimes the issue is hierarchy: juniors fear sounding stupid, so they do not ask. Sometimes it is production pressure: the team rushes because beds are tight. Sometimes safeguarding information is buried because no one knows who may hear it. Name the true barrier so the fix matches. [18] [3]
Distinguish a necessary specialty consult from a work-avoidance dump. A consult needs a question only that specialty can answer. A dump transfers anxiety without a decision request. [20] [21]
Clinical & Bedside Assessment
Before you hand over, reassess the child yourself when acuity is more than trivial. Confirm current vitals and trajectory. Check devices, lines, oxygen, feeds and emergency plans. Confirm allergies and an accurate weight source. List pending results with expected times. [1] [7]
Assess the environment. Can the receiver hear you? Are you both looking at the same list? Pause non-urgent interruptions. For family-inclusive handoff, assess language need and book a professional interpreter rather than using a sibling. [11] [16]
Technique errors to avoid: reading without eye contact; skipping illness severity; ending with “any questions?” so quickly that silence is forced; handing over from memory for a complex child; forgetting the contingency. [1] [5]
Investigations
Investigations enter communication as pending work with owners, not as laboratory poetry. Every critical pending culture, imaging study or blood gas needs a name and a time window in the handoff. [19]
Normal recent labs do not clear residual risk if the child is tiring or the caregiver is alarmed. Say that explicitly so the next team does not treat “normal CRP” as a discharge argument. [12]
For transfer, do not delay life-saving movement to complete a perfect image set. State what is done, what is pending and what must not delay the ambulance. Interhospital transport quality depends on complete yet practical pre-transfer communication. [13] [9]
Written handoff documents vary widely across hospitals. Multicentre needs assessment work showed inconsistency and recommended standard elements rather than free-text sprawl. Prefer concise critical fields over an unreadable dump. [19]
Management — Resuscitation
When the child is crashing, communication is treatment. Assign roles out loud. Use closed-loop for every critical order: drug, dose, route; read-back; confirm. Share the mental model in one sentence: “This is likely septic shock; we are giving fluids and antibiotics and preparing for intubation.” [17]
If MET, code or retrieval is activated, the handover must still carry baseline, current physiology, first actions, response and the next escalation task. Do not let paperwork delay the call. Stabilise and speak in parallel. [13] [9]
Management — Definitive & Stepwise
Prepare
Reassess. Update the list. Mark sickest first. Gather weight, allergies, code status or emergency care plans, devices, pending results and family presence needs. [1] [14]
Choose the tool
Use I-PASS for team shift or unit handoffs. Use ISBAR for phone referral, specialty consult and many retrieval openings. Adapt labels to local policy without dropping severity, contingency or synthesis. [1] [20]
Deliver I-PASS
State illness severity in plain words: stable watcher, unstable, or critical. Give a one-sentence patient summary with age, baseline and key problem. List actions with owners. Give situation awareness and if-then contingencies. Demand synthesis. [1] [2]
Deliver ISBAR
Identify yourself and the patient identifiers. State the situation and time frame needed. Give only the background that changes decisions. Offer your assessment. Make a specific request and leave a callback number. Marshall’s telephone referral education work supports structured teaching of this skill. [20] [21]
Match documents
Printed or electronic handoff sheets must include the same severity, actions and contingencies you spoke. Variation without standard elements is a known failure mode. [19]
Include families and interpreters
Family-centered structured communication can reduce harmful errors and improve experience. Use professional interpreters for limited English proficiency; disparities persist when language access is weak. [3] [11] [16]
Close the loop after consult or transfer
Confirm acceptance, destination, transport plan and who updates the family. After hospital-to-home transition for complex children, structured communication reduces post-discharge incidents. [15] [13]
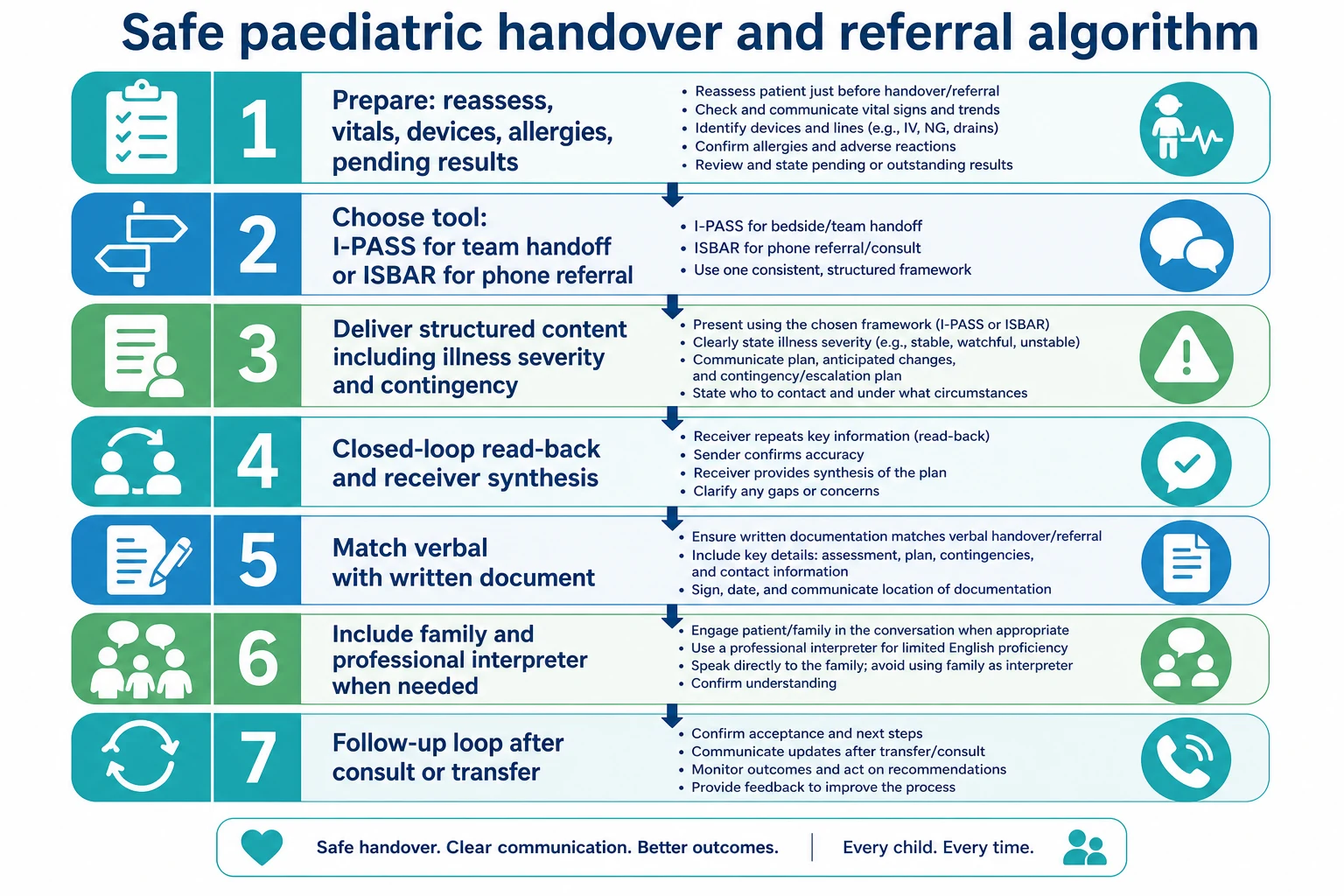
Read the figure like this: skip any step and the risk returns. Most exam failures sit in missing contingency, missing synthesis or missing interpreter. [1] [11]
Specific Subtypes & Scenarios
Night ward handoff. Lead with the sickest child. Time-box stable patients. Protect contingency plans for the three who could turn. [1]
ED to ward. Use receiver-driven clarification. State what treatment already happened and what response you saw. [5] [8]
PICU step-down. Residual risk is the point. Name the personal baseline, devices and first signs of return to ICU physiology. Stepped-wedge PICU handoff programmes have reduced adverse events in implementation trials. [6]
Rural retrieval. Open with ISBAR, capability gap and stabilisation already done. Do not delay the call for perfect imaging. [13] [9]
Neonatal transport. Modified SBAR tools have been used to standardise physician report on transport. Keep airway, glucose, temperature and maternal/perinatal context explicit. [10]
Specialty consult. One question, one urgency, one ask. Attach the decision-changing findings only. [20] [21]
Primary-care written referral. Problem, tempo, what you need from the clinic, red flags already discussed, and how the family will access care if they worsen while waiting. Safety-net content belongs until the appointment. [22]
Language-discordant family. Book the interpreter for handoff and rounds. Do not use children as interpreters. [11] [16]
Technology-dependent child. Hand over the emergency plan, baseline vitals, device settings and who the family trusts as the expert historian. [14] [15]
Safeguarding. Share need-to-know facts with the right team. Do not broadcast sensitive detail in a corridor handoff. [18] [7]
Adolescent confidentiality. Separate what may be shared with caregivers from what stays in the clinical team, within local law. [7] [3]
Complications & Pitfalls
Classic traps: false certainty; disagreeing verbal and written records; hierarchy that punishes questions; consulting without a question; polishing notes while the child needs transfer; omitting caregiver concern; equity failures when language access is skipped. [18] [3] [16]
Prognosis & Disposition
Better structured handoffs associate with fewer medical errors and fewer preventable adverse events in landmark paediatric work. Family-centered structured communication can reduce harmful errors and improve experience. Transport and ED adaptations aim at the same outcome: fewer miscommunications at high-risk edges. [1] [3] [5] [9]
Recurrent failures are a system signal. Fix templates, staffing for protected handoff time, interpreter access and observation coaching—not only the last junior who forgot a detail. [2] [4]
After consultation, disposition is incomplete until recommendations are acknowledged, owners are named and the family hears a consistent plan. After discharge of complex children, transition communication is part of prognosis for safe home care. [15]
Special Populations
Neonates. Include perinatal context, glucose, temperature and transport physiology. [10]
Medical complexity. Baseline, devices, emergency plans and hospital-to-home loops. [14] [15]
Language discordance and migrant/refugee families. Professional interpreters improve hospital communication quality and are a safety intervention, not a courtesy. [11] [16]
Disability and neurodiversity. Hand over the child’s usual communication method and personal signs of pain or distress. [14]
Indigenous families. Use culturally safe communication, correct names and local support pathways without stereotyping. [11] [3]
Out-of-home care. Identify the legal decision-maker and the best historian; records are often fragmented. [14] [18]
Youth justice and adolescent mental health. Privacy, risk and escort plans must be explicit in multi-agency handoffs. [7] [18]
Safeguarding and family violence. Controlled information sharing; document who was told what and why. [18] [7]
Evidence, Guidelines & Regional Differences
Evidence anchor. Starmer 2014 remains the core multicentre paediatric resident I-PASS result: errors 24.5→18.8 and preventable adverse events 4.7→3.3 per 100 admissions. Starmer 2023 extends implementation across diverse environments. Nursing bundles and ED/transport adaptations support spread with local coaching. [1] [2] [4] [8]
Family communication. Khan 2018 showed harmful errors falling after structured family-centered rounds communication even when overall errors were unchanged. [3]
ISBAR. Australian hospital spread of ISBAR and education research on telephone referral structure support phone consult craft. [20] [21]
ANZ. ACSQHS Communicating for Safety Standard expects systems for effective clinical communication at transitions. Local health services operationalise ISBAR/I-PASS variants; quote local forms when you work there. [20] [1]
US. ABP EPA 8 centres on executing handovers within or across settings. Joint Commission handoff safety expectations shape hospital policy; I-PASS is a common operational response. [1]
UK/Canada. Structured handover culture is expected in paediatric training and service standards; RCPSC Foundations EPA 10 explicitly assesses transfer of clinical information. Use local mnemonics without dropping severity, contingency and confirmation. [1] [2]
Controversies. Structured handoff takes minutes; the data argue those minutes buy safety. Family presence is not always appropriate for every corridor detail, but exclusion by default loses a safety partner. Electronic health records help only if they are curated; dumps recreate cognitive overload. [19] [3]
Exam Pearls
- I-PASS ends with Synthesis by receiver—make them talk. [1]
- ISBAR for phone: Identity, Situation, Background, Assessment, Request. [20]
- Quote Starmer rates only as 24.5→18.8 errors and 4.7→3.3 preventable AEs per 100 admissions. [1]
- Every pending result needs a named owner. [19] [1]
- Caregiver concern belongs in the handoff. [12]
- Professional interpreter, not family, for language discordance. [11]
- Consults need a question, urgency and callback. [20] [21]
- Closed-loop in codes: order → read-back → confirm. [17]
- Boards test this as EPA work (ABP 8, RCPSC Foundations 10), not soft skills. [1] [2]
I-PASS at the bedside
References
- [1]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [2]Starmer AJ Implementation of the I-PASS handoff program in diverse clinical environments: A multicenter prospective effectiveness implementation study. Journal of hospital medicine, 2023.PMID 36326255
- [3]Khan A Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study. BMJ (Clinical research ed.), 2018.PMID 30518517
- [4]Starmer AJ Effects of the I-PASS Nursing Handoff Bundle on communication quality and workflow. BMJ quality & safety, 2017.PMID 28679836
- [5]Huth K Implementing receiver-driven handoffs to the emergency department to reduce miscommunication. BMJ quality & safety, 2021.PMID 32299957
- [6]Jorro-Barón F Handoff improvement and adverse event reduction programme implementation in paediatric intensive care units in Argentina: a stepped-wedge trial. BMJ quality & safety, 2021.PMID 33893213
- [7]Alcalá Minagorre PJ Safe handoff practices and improvement of communication in different paediatric settings. Anales de pediatria, 2023.PMID 37640658
- [8]Yanni E Implementation of ED I-PASS as a Standardized Handoff Tool in the Pediatric Emergency Department. Journal for healthcare quality : official publication of the National Association for Healthcare Quality, 2023.PMID 37141571
- [9]Norman KM Implementing IPASS Handoff to Improve Patient Safety in Pediatric Critical Care Transport. Air medical journal, 2023.PMID 36958881
- [10]Shahid S Evaluation of a Modified SBAR Report to Physician Tool to Standardize Communication on Neonatal Transport. American journal of perinatology, 2022.PMID 32819017
- [11]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [12]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [13]Chaichotjinda K Assessment of interhospital transport care for pediatric patients. Clinical and experimental pediatrics, 2020.PMID 31477679
- [14]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [15]Huth K Reduced Postdischarge Incidents After Implementation of a Hospital-to-Home Transition Intervention for Children With Medical Complexity. Journal of patient safety, 2023.PMID 37729645
- [16]Pelpola JS Disparities During Family-Centered Rounds for Families Using Languages Other Than English. Pediatrics, 2025.PMID 40716767
- [17]Lauridsen KG Standardising communication to improve in-hospital cardiopulmonary resuscitation. Resuscitation, 2020.PMID 31891790
- [18]Simmons P Characterization of Communication-Related Safety Events in a Pediatric Quaternary Care Hospital. Journal of patient safety, 2026.PMID 42008794
- [19]Rosenbluth G Variation in printed handoff documents: Results and recommendations from a multicenter needs assessment. Journal of hospital medicine, 2015.PMID 26014471
- [20]Finnigan MA ISBAR for clear communication: one hospital's experience spreading the message. Australian health review : a publication of the Australian Hospital Association, 2010.PMID 21108899
- [21]Marshall SD Telephone referral education, and evidence of retention and transfer after six-months. BMC medical education, 2012.PMID 22676409
- [22]Burvenich R Towards an international consensus on safety netting advice for acutely ill children presenting to ambulatory care: a modified e-Delphi procedure. Archives of disease in childhood, 2024.PMID 38123917