Paeds · clinical-assessment-and-reasoning
Structured physical examination from newborn to adolescent
Also known as Paediatric physical examination · Age-adapted physical examination · Newborn examination · Short case examination · NIPE style newborn screen
Fellowship guide to planning and performing an age-adapted structured physical examination from newborn through adolescence: preparation, opportunistic sequencing, growth and vital-sign technique, newborn screening manoeuvres, system exams, dignity and safeguarding, interpretation thresholds, and short-case performance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
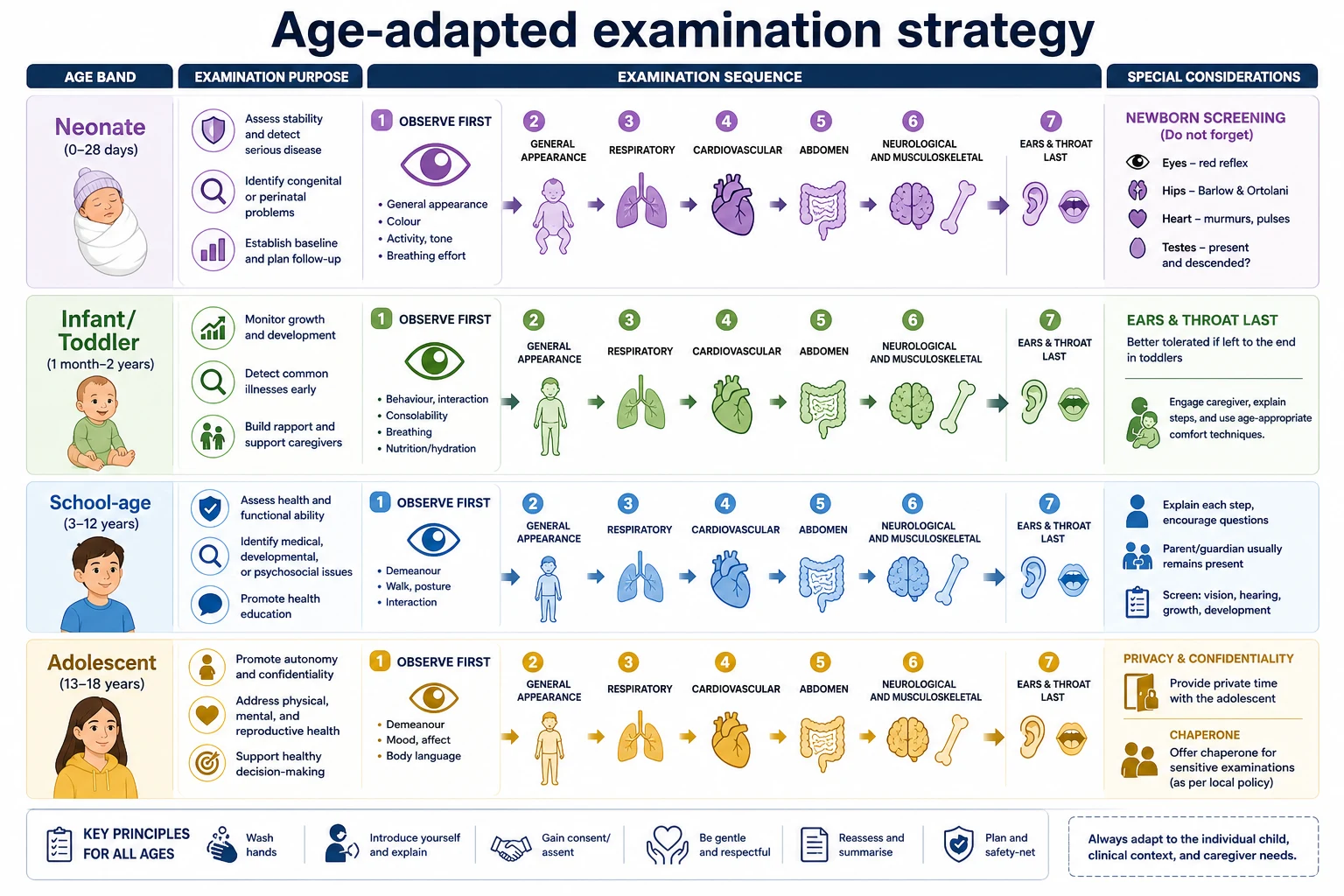
A structured paediatric physical examination is not a fixed head-to-toe script recited the same way for every child. It is a deliberate, age-adapted sequence that answers clinical questions while protecting dignity and trust. You start with what you can learn without touching. You choose an order that fits the child’s age, illness and tolerance. You leave the most upsetting steps until last when it is safe to do so. [15] [13]
Think of four related activities that people sometimes mix up. Doorway observation (including tools such as the Paediatric Assessment Triangle) tells you whether the child looks immediately threatened. Opportunistic examination means you use calm moments to listen to the chest or feel the abdomen before the child becomes distressed. Structured systems examination is the organised short-case style survey of a region or system. Screening manoeuvres (red reflex, hips, femoral pulses, spine, genitalia in newborns) deliberately seek silent conditions. Each has a job. None replaces the others. [15] [10] [7]
The examination pathway you can actually run
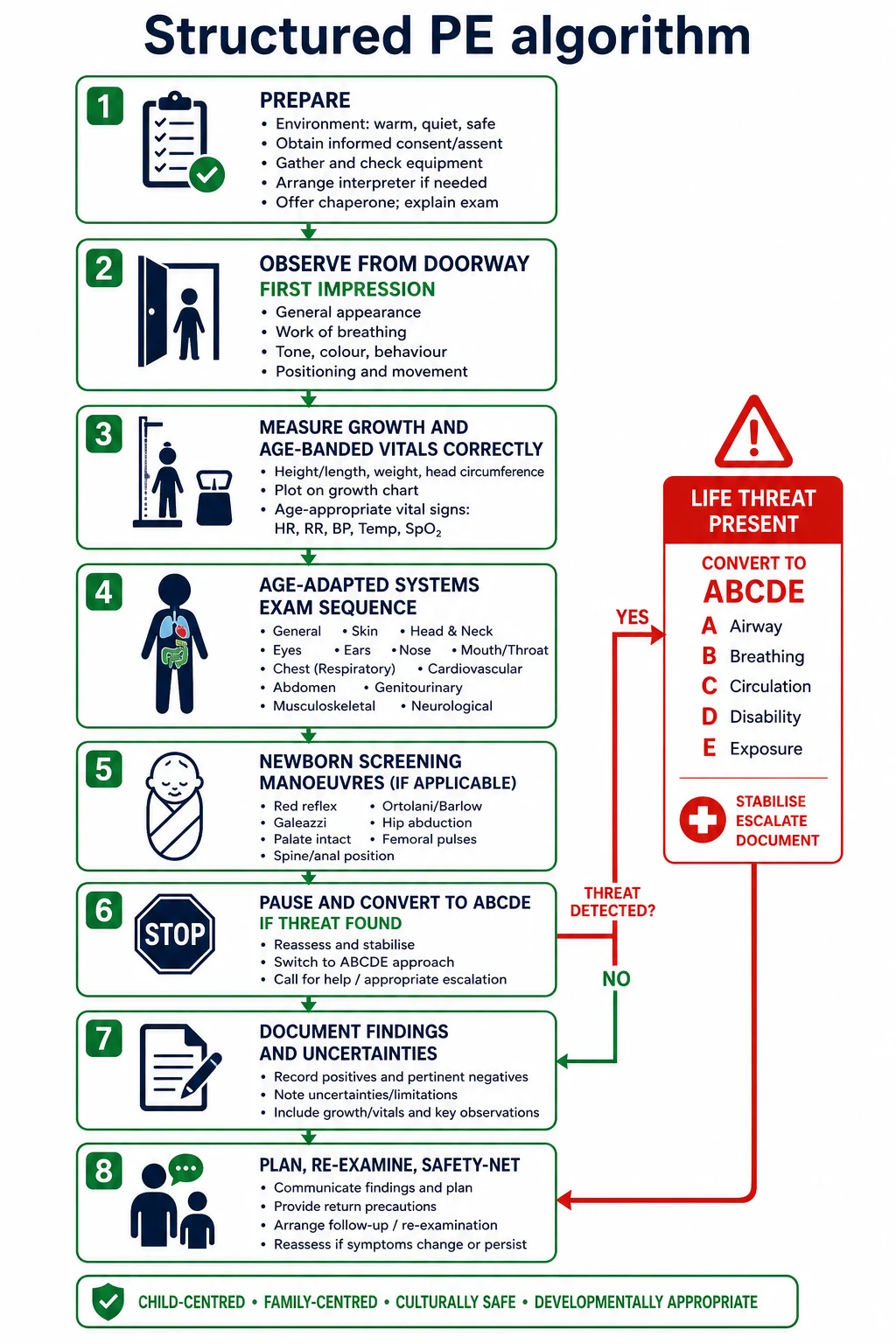
Prepare
Light, privacy, warm hands, equipment, growth chart, correct BP cuff, interpreter, chaperone when needed, infection control, and a plan for who stays in the room.
Observe first
Interaction, colour, work of breathing, posture, play, devices, and caregiver handling before you touch.
Measure with care
Growth, heart rate, respiratory rate, temperature, oxygen saturation and blood pressure using age-correct technique and local reference charts.
Examine by age strategy
Newborn screening manoeuvres; toddler opportunistic order; school-age systems order; adolescent confidentiality and consent.
Synthesise and act
Localise findings, state urgency, convert to ABCDE if needed, document gaps, and plan re-examination or referral.
Classification
Examinations differ by purpose. A newborn screening examination looks for treatable silent problems in eyes, heart, hips and testes within a defined programme (in the UK, NIPE). A well-child surveillance examination tracks growth, development cues and focused systems over time. A focused acute examination answers a presenting complaint while still watching for red flags. A short-case performance examination tests technique, localisation and synthesis under time pressure. An adolescent confidential examination adds privacy, assent or consent, and chaperone decisions. [10] [13] [16]
Screening manoeuvre
- Seeks silent disease
- Standard technique matters
- Positive finding needs pathway, not reassurance alone
- Examples: red reflex, Ortolani/Barlow, femoral pulses
Diagnostic manoeuvre
- Tests a hypothesis from history
- Localises a known problem
- May be painful — leave until late if safe
- Examples: focused joint exam, abdominal guarding map
Reassessment finding
- Compared with earlier state
- After treatment or time
- Trend beats a single normal sign
- Examples: work of breathing after oxygen, perfusion after fluid
Life stage is a classification axis because anatomy and cooperation change. Neonates tolerate full undressing in a warm room and need full skin, hip and eye checks. Infants may be calmer on a caregiver’s lap. Toddlers often refuse strangers; examine through play and leave ears and throat last. School-age children can follow a classic systems order if you explain each step. Adolescents need private space, a clear offer of a chaperone, and explicit discussion of what will be examined and why. [16] [17] [13]
Epidemiology & Risk Factors
Missed findings cluster where examination is rushed, incomplete or technically wrong. High-risk settings include busy discharge nurseries, febrile toddlers who are never undressed, telehealth visits that pretend to replace hands-on care, and adolescents examined without privacy so genital or breast complaints are never disclosed. Children with medical complexity are at risk when teams examine only the device and not the whole child. [13] [10]
Risk rises when lighting is poor, skin tone is ignored during colour assessment, language barriers block consent and explanation, or forced restraint replaces a developmental approach. Pulse oximetry can under-read or mislead across skin tones; treat saturation as one sign among many, not a complete circulation exam. [14]
Conditions deliberately sought by early examinations include developmental dysplasia of the hip, congenital cataract and other media-opacifying eye disease, critical congenital heart disease cues (cyanosis, weak femorals, pathological murmur), undescended testes, neural tube stigmata, growth failure and concerning bruises. Programmes differ by country, but the clinical duty to examine carefully does not. [7] [10] [10]
Pathophysiology
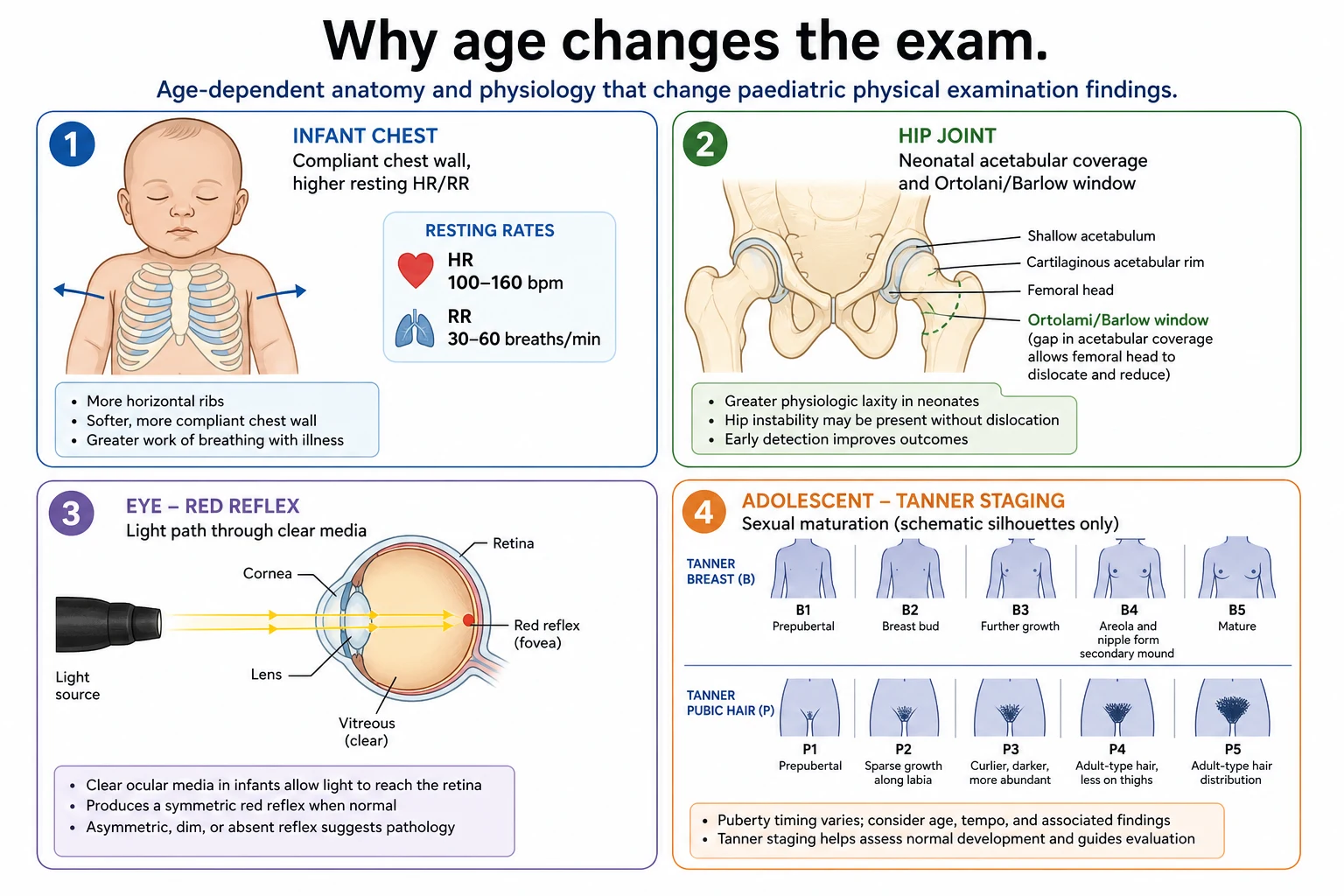
Age changes what “normal” looks and sounds like. Young infants have higher resting heart and respiratory rates; a rate that is fine for a newborn is alarming in a school-age child. Fleming’s systematic review and O’Leary’s Australian centiles both show why you must use age-banded ranges rather than adult memory. Local PEWS charts operationalise those ranges for the ward you work on. [1] [2] [18]
Compensation physiology matters during examination. A toddler may maintain blood pressure while tachycardia and cool peripheries show circulatory strain. Capillary refill time (CRT) can support that story, but measurement technique and reliability vary; prolonged CRT raises concern and must be integrated with other signs, not used alone as a discharge rule. [3] [4] [5]
Hip joint stability is greatest for detection early, when soft-tissue laxity and incomplete acetabular coverage allow Ortolani and Barlow to detect reducible dislocation or instability. A “click” without instability is not the same as a positive Ortolani. Limited abduction and asymmetric findings gain importance as the infant grows. [7] [8] [9]
Red-reflex screening works because light reflects from the fundus through clear media. Media opacity, high refractive error or retinal pathology can dull, whiten or asymmetric the reflex. The manoeuvre is a screen, not a full eye examination. [10]
Innocent murmurs arise from normal flow in a structurally normal heart. They are typically soft, early-to-mid systolic, change with position or fever, and lack diastolic components, thrills or signs of heart failure. Pathological features force a different pathway. [12]
Clinical Presentation
What normal looks like by age band [1] [2]
A healthy neonate may sleep through much of the exam, show symmetric Moro and grasp, pink colour (assess carefully across skin tones), equal red reflexes, stable hips, palpable femorals, and a soft abdomen with a healing cord. An infant at six months should fix and follow, sit with or without support according to development, and tolerate lap-based auscultation better than a cold table. A toddler may cling, cry and then settle with bubbles or a song; respiratory rate counted while crying is not a resting rate. A school-age child can point to pain and cooperate with auscultation if you narrate. An adolescent may look well while hiding distress; privacy changes what you hear. [13] [1]
Subtle high-yield abnormalities include: quiet tachypnoea at rest; preferential head posture; unequal chest movement; a soft but pansystolic murmur with weak femorals; hepatomegaly with poor weight gain; a single petechial patch that expands; a white red reflex; and a non-mobile infant with any unexplained bruise. [11] [10] [4]
Fear, fever and crying raise heart rate and respiratory rate and can create flow murmurs. State the conditions of measurement: “HR 148 while crying; calmer rate not yet obtained.” Do not label a child “tachycardic” from a single distressed reading without context. [1] [2]
Neurodisability baselines change tone, posture, eye contact and consolability. Compare with the caregiver’s description of usual. A child who is “always a bit stiff” still needs a full exam for new asymmetry, new seizures signs, device sites and skin pressure injury. [13]
Differential Diagnosis
Murmur at the bedside. Favour innocent when the child is well grown, the murmur is soft and early systolic, there is no thrill, no diastolic component, no radiation of concern, and pulses are equal. Favour pathology when there is cyanosis, poor growth, hepatomegaly, abnormal pulses, a loud or harsh murmur, diastolic timing, or symptoms. When uncertain, document carefully and arrange timely cardiology review rather than guessing. [12]
Hips. Asymmetric thigh creases alone are weak. Limited abduction, leg-length discrepancy, a positive Ortolani (clunk of reduction) or Barlow (dislocatable hip) change management. The Rational Clinical Examination review and AAP clinical report guide how much weight to place on each finding and when imaging or orthopaedic referral is needed. Do not invent universal ultrasound ages here—follow local and guideline pathways. [7] [8] [9]
Colour. Pallor, mottling, jaundice and cyanosis are harder to judge on darker skin. Use mucous membranes, palms/soles where appropriate, perfusion, behaviour and saturation together. Never rely on a single visual label under poor light. [14]
Bruises and safeguarding. In young children, bruise location and pattern matter. Pierce and colleagues validated a clinical decision rule based on bruising characteristics to help identify children who need a full abuse evaluation. A rule supports concern; it does not by itself diagnose abuse. Any non-mobile infant with unexplained bruising needs a safeguarding pathway. [11]
Clinical & Bedside Assessment
Preparation
Warm the room. Wash hands. Introduce yourself to the child first when age allows. Explain to the caregiver what you will do. Offer an interpreter before you start, not after consent fails. For adolescents and for intimate examinations, discuss a chaperone; preferences vary, so ask rather than assume. Have a growth chart, tape, infant scales or standing stadiometer, ophthalmoscope, otoscope, and a set of blood-pressure cuffs ready. [16] [17] [6]
Sequence that reduces distress
- Observe from the door and while taking history. [1] [2]
- Count respiratory rate before undressing if the child is calm. [1] [2]
- Examine hands, face and skin while talking. [1] [2]
- Auscultate heart and lungs early in infants and toddlers—before ears and throat.
- Abdomen next while the child is still relatively calm.
- Hips, spine, genitalia and ears/throat last in younger children when safe.
- Save painful joints or wound checks until you have the cooperative parts done—unless the pain source is the emergency. [15]
If the child deteriorates, stop the script and treat threats. [15]
Growth and vital signs
Measure weight, length or height, and head circumference with the correct device and plot on the correct chart (WHO standards for many young children; preterm charts such as Fenton for preterm infants—use local policy). For blood pressure, choose a cuff with bladder width covering about 40% of mid-upper arm circumference and length 80–100% of the circumference; the AAP 2017 guideline is the key reference for technique and elevated BP definitions by age and height. [6]
Count heart rate and respiratory rate for enough time to be accurate, ideally when the child is quiet. Use age-banded normal ranges from syntheses such as Fleming 2011 and local charts such as O’Leary 2015 or your hospital PEWS. [1] [2] [1]
For CRT, apply light pressure for a few seconds on a standard site (often sternum or finger), release, and time return of colour. Interpret with other perfusion signs; evidence shows variable reliability and diagnostic value depending on setting and method. [3] [4] [5]
Newborn examination core
Undress fully in warmth. Inspect skin for jaundice, birthmarks and sacral stigmata. Check red reflexes bilaterally. Auscultate the heart; feel femoral pulses. Examine hips with Ortolani and Barlow using gentle, correct technique. Assess tone, posture and primitive reflexes in context. Examine genitalia for descended testes and ambiguous features. Check the palate, clavicles and red flags for sepsis or respiratory distress. Document which parts were incomplete. [10] [7] [10]
System examinations (short-case style)
Cardiovascular: inspection (cyanosis, scars, respiratory effort), pulses (rate, rhythm, volume, femorals), precordium, auscultation in all areas, liver edge, oedema. [1] [2] Respiratory: effort, recession, tracheal position, expansion, percussion if cooperative, auscultation all zones. [1] [2] Abdomen: inspection, gentle palpation from non-tender area, organomegaly, hernial orifices, genitalia when indicated with consent. [1] [2] Neurology: observe posture and gait first; cranial nerves through play; tone, power, reflexes; cerebellar signs if age allows. [1] [2] ENT: leave otoscopy and throat last in toddlers. [1] [2] MSK: look, feel, move; compare sides; gait. [1] [2] Skin: full undress when indicated; document bruises with location, size and explanation. [1] [2] Puberty: Tanner staging only when clinically needed, with consent/chaperone and clear purpose. [16] [12] [11]
Special examination contexts
Distressed toddler: caregiver lap, toys, demonstrate on doll or caregiver first, minimal restraint, multiple short looks rather than one forced session. [1] [2]
Medical complexity: ask usual baseline, check device sites, secretions, tone, pressure areas; avoid attributing everything to “the syndrome.” [13]
Adolescent: private history first when appropriate; negotiate examination; document chaperone offered/accepted; never surprise with genital examination. [17]
Investigations
Examination findings should trigger tests, not the other way around. Examples of urgent triggers: white red reflex → same-day ophthalmology pathway; suspected critical heart disease signs → urgent senior/cardiology and local critical congenital heart disease protocol; unstable hip with positive Ortolani → follow AAP/local DDH pathway including imaging timing; unexplained bruise in non-mobile infant → safeguarding evaluation. [10] [7] [11]
Optional tests follow after a reasoned differential: echocardiogram for pathological murmur features; hip ultrasound or radiograph per age and guideline; hearing assessment if newborn screen missed or concerns arise. [15]
Harmful patterns include blanket blood panels after a normal exam, repeated imaging without a question, and “just in case” restraint for incomplete otoscopy when observation and follow-up would be safer. [15]
Interpret vital signs and growth with age-specific ranges and measurement error in mind. A single high BP reading needs correct cuff, calm repeat and guideline-based next steps, not an instant chronic hypertension label. [6] [1]
Management — Resuscitation
If structured examination uncovers airway compromise, severe respiratory distress, shock signs, seizure or reduced consciousness, stop the routine sequence. Call for help. Switch to age-adapted ABCDE. Treat as you find. Keep the findings you already noted (for example, petechiae or a white reflex) in the handover, but do not finish a full hip exam while the airway is at risk. Check immediately reversible threats: airway position, oxygen, glucose when relevant, tension pneumothorax signs, haemorrhage, seizure activity. [15] [4]
Management — Definitive & Stepwise
Prioritise when time is short: life threats first; then findings that change same-day disposition (red reflex, femorals, bruising in infants, severe dehydration signs); then complete systems later. Escalation after abnormal screening follows local pathways and specialty guidance (ophthalmology, orthopaedics, cardiology, safeguarding). [7] [10] [10]
Specific Subtypes & Scenarios
Newborn / NIPE-style. Eyes, heart, hips, testes (and full general exam) within programme timeframes; clear referral routes for positives. [10] [7]
Infant well-child or sick visit. Growth trajectory, development observation, focused systems, opportunistic full undress when fever or parental concern. [15]
Preschool / school-age short case. Introduce, wash hands, expose adequately, examine systematically, talk findings, present a synthesis. [15] [15]
Adolescent confidential exam. Separate time if safe; explain limits of confidentiality; chaperone; indicated breast/genital/MSK exams only with clear reason. [16] [17]
Technology-dependent / neurodiverse. Sensory-aware approach; device check; baseline comparison; avoid overstimulation. [13]
Telehealth. You can observe work of breathing, interaction and some skin lesions. You cannot reliably perform red reflex, hips, full auscultation quality, or intimate exams. State limits and arrange in-person review when those manoeuvres are required. [15]
Complications & Pitfalls
Classic technique errors: cold hands causing “voluntary guarding”; wrong BP cuff size; counting respiratory rate for three seconds and multiplying; otoscopy without bracing your hand; red-reflex check with lights on and too close; hip manoeuvres that are rough or mislabelled as positive because of a soft click; abdominal exam only above the navel; declaring “no bruises” without undressing. [6] [3] [8]
False reassurance from one normal sign is dangerous: a normal CRT does not exclude serious illness; a soft murmur does not exclude structural disease if other features worry you; a smiling toddler can still be hypoxic. [4] [14]
Forced restraint destroys trust and can injure. Incomplete undressing misses abuse marks and rashes. Missing spine or genital examination in newborns misses time-critical findings. Over-investigation after a sloppy exam wastes resources and harms families. Lighting and oximetry bias worsen inequity if you do not compensate with careful mucous-membrane and perfusion assessment. [14] [11]
Prognosis & Disposition
Disposition after examination is a clinical decision: home with safety-net, timed re-examination, outpatient referral, same-day senior review, imaging pathway, admission, or resuscitation bay. Borderline findings (soft asymmetric creases, single high BP, incomplete toddler exam) need an explicit plan, not vague hope. Growth trajectory abnormalities increase follow-up intensity even when today’s systems exam is normal. [6] [13]
Safety-net language should name what to watch for, when to return, and how incomplete parts will be finished (“ears not examined today because of distress; GP review tomorrow if fever persists; return tonight if breathing worsens”). [15]
Special Populations
Preterm and NICU graduates need corrected-age thinking for growth and development cues, careful hip and eye follow-up per neonatal pathways, and scar/device awareness. [15]
Complex chronic disease needs whole-child examination beyond the technology. [13]
Indigenous, migrant and refugee families need interpreters, cultural safety, and careful explanation of intimate or undressing steps. [15]
Out-of-home care and safeguarding populations need meticulous skin and injury documentation and low threshold for multi-agency pathways. [11]
Gender-diverse adolescents need affirmed names/pronouns, privacy, and trauma-informed examination only for clear clinical indications. [17]
Evidence, Guidelines & Regional Differences
Vital-sign ranges: Fleming 2011 provides broad evidence-based centiles; O’Leary 2015 adds Australian tertiary-hospital centiles; local PEWS and RCH-style observation charts turn ranges into escalation rules. PEWS systems improve recognition processes but are not magic—EPOCH did not show all-cause mortality reduction from one implementation package, so clinical judgement remains central. [1] [2] [18]
Hips: AAP 2016 clinical report guides evaluation and referral; JAMA Rational Clinical Examination 2024 summarises manoeuvre accuracy; Ortolani positivity carries high positive predictive value in some screening cohorts but is not the whole pathway. [7] [8] [9]
Eyes: AAP visual system assessment guidance supports red-reflex screening by paediatricians. [10]
BP: AAP 2017 CPG defines technique and thresholds. [6]
Bruising: Pierce 2021 validates a decision rule for abuse concern based on bruise characteristics. [11]
ANZ: local PEWS/observation ranges; maternity newborn exams; RCH clinical guidelines. [1]
UK: NIPE programme for eyes, heart, hips, testes. [10]
US: AAP red reflex, DDH report, BP CPG, Bright Futures periodicity. [10] [7] [6]
Canada: RCPSC EPA emphasis on performing and presenting a basic physical examination; adolescent confidentiality practice aligned with national paediatric guidance. [15]
Chaperone evidence is preference- and survey-based rather than trial-based; still, offering a chaperone and documenting the discussion is expected professional practice. [16] [17]
Worked short-case scripts
Cardiovascular short case (school-age)
Introduce yourself and wash hands. Ask the child’s preferred name. Expose the chest while keeping a blanket for dignity. Look for scars, chest shape, respiratory effort and colour. Feel both radial pulses, then femoral pulses, comparing timing and volume. Count the rate when the child is quiet. Palpate the apex and right ventricular lift. Auscultate with the diaphragm and bell at apex, lower left sternal edge, pulmonary and aortic areas, and the back. Listen specifically in systole and diastole. Check for radiation to the neck or axilla. Feel the liver edge and look for oedema. Present: “I examined the cardiovascular system of this well-looking [age] child. Pulse was [rate], regular, normal volume, with [equal/unequal] femorals. Apex was [site]. There was [no] thrill. I heard [murmur description or no murmur]. There were no signs of heart failure. My synthesis is [innocent features vs concern], and next I would [observe/refer/investigate].” [12]
Newborn focused exam (eyes, hips, tone)
Warm hands. Dim the room for red reflex; hold the light at arm’s length and compare both eyes. State clearly if a reflex is absent, white or asymmetric. For hips, examine one side at a time with the pelvis stabilised; perform Barlow and Ortolani gently; describe a clunk, not a soft tendon click. Assess resting posture, pull-to-sit head lag appropriate for age, and ventral suspension if trained and indicated. Say what is normal and what triggers the local orthopaedic or ophthalmology pathway. [10] [7] [8]
Abdomen short case (preschool)
Observe first for distension, scars and movement with respiration. Ask where it hurts and start away from that point. Warm hands; use the child’s hand under yours if ticklish. Palpate lightly then more deeply. Examine for hepatosplenomegaly with appropriate technique. Check hernial orifices. Only examine genitalia if the case requires it and consent is clear. Present positives and important negatives (guarding, masses, organomegaly). [15]
Communication during examination
Speak to the child in short concrete sentences. “I am going to listen to your chest with my warm stethoscope. It will not hurt.” For procedures that may hurt, warn once honestly. For adolescents, ask who they want in the room. Explain findings in plain language without false certainty: “I can hear a soft murmur that often is flow in a normal heart, but I want a senior to listen because of [feature].” [17]
When an interpreter is present, speak to the family, not to the interpreter. Pause after each step so meaning is checked. Cultural modesty may require same-gender examiner or extra draping—ask rather than assume. [15]
Documentation standards
Write what you examined, what you found, the conditions (crying, febrile), and what remains incomplete. Prefer: “Tympanic membranes not visualised due to distress; plan re-exam with GP within 24 h if fever continues.” Avoid: “ENT normal” when you never looked. For bruises, record location, size, colour description carefully, and the explanation offered. Photograph only within local safeguarding and consent policy. [11]
Growth numbers need units, date, and chart used. Blood pressure needs cuff size, limb, position and repeat if elevated. [6]
Linking examination to history without duplicating history topics
History tells you where to look harder. A limp directs a full hip and knee exam and spine check. Nocturnal cough directs chest and growth. Headache with vomiting directs neurology and blood pressure. Adolescent abdominal pain may need a confidential sexual history before a sensitive examination. The examination page owns technique and interpretation thresholds; the history page owns question structure. Use both. [15]
Age-banded vital sign practice (without inventing fixed cut-offs)
Do not memorise a single “normal HR” for “children.” Use the Fleming synthesis and your local chart. In practice: count for a full window when possible; note sleep versus cry; recheck outliers; escalate using local PEWS response algorithms rather than personal gut alone. O’Leary’s Australian centiles are a useful hospital-based reference alongside international data. [1] [2] [18] [1]
CRT teaching point for general practice and hospital: standardise site and pressure, interpret with the whole picture, and remember diagnostic performance is imperfect. [5] [4]
Hip screening depth for fellowship
AAP clinical report emphasises serial clinical examinations and risk-factor awareness (for example breech and family history—quote risk factors from the source when counselling, and follow imaging recommendations current in your jurisdiction). Singh’s Rational Clinical Examination review helps you weight limited abduction and Ortolani findings more heavily than isolated soft clicks. Maikku’s data support high positive predictive value of a true positive Ortolani in screening contexts, which is why you must not dilute the word “positive.” [7] [8] [9]
If you are unsure of your technique, ask a senior to supervise—false positives drive unnecessary imaging; false negatives delay treatment of dysplasia. [15]
Red reflex depth
Donahue and AAP visual assessment guidance place red-reflex testing firmly in the paediatrician’s role for early detection of cataract and other media problems. Perform in a dim room, use a direct ophthalmoscope light, view both eyes, and compare. Leukocoria or absent reflex is an urgent referral, not a “review next visit” item. [10]
Blood pressure depth
Wrong cuff size is the commonest technical error. Too small a cuff falsely elevates readings. Confirm elevated readings with correct technique, repeated measurements, and the AAP 2017 tables by sex, age and height percentile for definitions of elevated BP and hypertension stages. Initial evaluation steps and when to investigate secondary causes belong with the hypertension topic; this leaf owns getting the measurement right during the physical examination. [6]
Safeguarding examination without tunnel vision
A structured PE can be the first time concerning injuries are seen. Pierce’s validation study supports using bruise pattern decision tools to identify young children who need full evaluation for abuse. Still examine the whole child: growth, development interaction, oral injury, frenulum, pinnae, genitals when indicated under safeguarding protocols, and the caregiver–child interaction. Document objectively. Escalate through local child-protection procedures. [11]
Medical complexity checklist during PE
Ask: What is different from this child’s usual? Check airways devices, oxygen baseline, feed route, tone baseline, contractures, pressure areas, VP shunt sites, and emergency plans. Kuo’s report on medical complexity reminds clinicians that standard “well child” scripts underserve these children if used blindly. [13]
Equity of colour and perfusion assessment
Sharma’s review of pulse-oximetry disparities is a warning: device readings can misclassify hypoxaemia across skin tones. Combine saturation with work of breathing, mental status, pulse quality and careful visual assessment of mucous membranes. Advocate for better lighting and calibrated equipment. [14]
Converting incomplete exams into safe plans
Incomplete does not mean abandoned. Examples: [1] [2]
- Febrile toddler too distressed for throat exam → treat on available findings, safety-net for stridor/drooling/dehydration, re-examine when calmer or in better setting. [1] [2]
- Adolescent declines genital exam → explore reasons, offer chaperone/same-gender clinician, document refusal, ensure alternative pathway if STI or torsion remains possible (urgent senior review). [1] [2]
- Telehealth well-baby without red reflex → book timely in-person screen. [15]
OSCE and long-case performance cues
Long case: integrate exam findings with functional history, growth charts brought by family, and school/developmental context; do not examine endlessly without synthesising. Short case: technique and localisation dominate. OSCE: narration and consent language are scored. Structured oral: defend why you left the throat until last or why you stopped for ABCDE. [15] [15] [15]
Common examiner traps
- Calling every click DDH. [1] [2]
- Declaring ENT normal without otoscopy. [1] [2]
- Using adult BP norms.
- Missing femorals.
- Examining genitalia in adolescents without explanation.
- Reassuring on a single normal CRT.
- Ignoring caregiver baseline in disability.
- Inventing findings under time pressure. [15]
Putting it together: three rapid mental models
Model A — The calm well child: full age-appropriate exam, growth, screening items, anticipatory guidance. [1] [2] Model B — The unhappy toddler: observe, opportunistic cardiorespiratory and abdomen, defer painful ENT, recheck vitals when calmer. [1] [2] Model C — The silent emergency: doorway concern → help → ABCDE; park the checklist. [1] [2]
These models keep you flexible without lowering standards. [1] [2]
Exam Pearls
- Short case: wash hands, introduce, expose properly, talk findings as you go, localise, then synthesise in one breath. [15]
- Toddlers: heart and lungs before ears and throat. [15] [1] [2]
- Innocent murmur phrase examiners like: soft, early systolic, no diastolic, no thrill, normal pulses and growth. [12]
- Ortolani is a clunk of reduction, not every click. [8]
- Red reflex: dim room, both eyes, compare. [10]
- TEN-4-FACESp-style thinking flags concerning bruise regions in young children—use it to trigger evaluation, not as a courtroom verdict. [11]
- If you did not examine it, write that you did not examine it. [15] [1] [2]
PREPARE for paediatric PE
Summary for the night before the exam
You are not scored for undressing every child in the same order. You are scored for choosing a safe, kind, complete-enough examination that finds silent disease, respects dignity, measures correctly, and changes into resuscitation when the child declares an emergency. Practice the words of synthesis until they are automatic. [15]
References
- [1]Fleming, Susannah Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet (London, England), 2011.PMID 21411136
- [2]O'Leary, F Defining normal ranges and centiles for heart and respiratory rates in infants and children: a cross-sectional study of patients attending an Australian tertiary paediatric hospital. Archives of disease in childhood, 2015.PMID 25784747
- [3]Fleming, Susannah Validity and reliability of measurement of capillary refill time in children: a systematic review. Archives of disease in childhood, 2015.PMID 25260515
- [4]Fleming, Susannah The Diagnostic Value of Capillary Refill Time for Detecting Serious Illness in Children: A Systematic Review and Meta-Analysis. PloS one, 2015.PMID 26375953
- [5]Fleming, Susannah Capillary refill time in sick children: a clinical guide for general practice. The British journal of general practice : the journal of the Royal College of General Practitioners, 2016.PMID 27789509
- [6]Flynn, Joseph T Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics, 2017.PMID 28827377
- [7]Shaw, Brian A Evaluation and Referral for Developmental Dysplasia of the Hip in Infants. Pediatrics, 2016.PMID 27940740
- [8]Singh, Abhinav Does This Infant Have a Dislocated Hip?: The Rational Clinical Examination Systematic Review. JAMA, 2024.PMID 38619828
- [9]Maikku, M The Ortolani test has a high positive predictive value in clinical hip screening for developmental dysplasia of the hip. Acta paediatrica (Oslo, Norway : 1992), 2023.PMID 36928888
- [10]Donahue, Sean P Visual System Assessment in Infants, Children, and Young Adults by Pediatricians. Pediatrics, 2016.PMID 29756730
- [11]Pierce, Mary Clyde Validation of a Clinical Decision Rule to Predict Abuse in Young Children Based on Bruising Characteristics. JAMA network open, 2021.PMID 33852003
- [12]Advani, N The diagnosis of innocent murmurs in childhood. Cardiology in the young, 2000.PMID 10950330
- [13]Kuo, Dennis Z Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [14]Sharma, Megha Racial and skin color mediated disparities in pulse oximetry in infants and young children. Paediatric respiratory reviews, 2024.PMID 38233229
- [15]Dieckmann, Ronald A The pediatric assessment triangle: a novel approach for the rapid evaluation of children. Pediatric emergency care, 2010.PMID 20386420
- [16]Moon, Rebecca J Confidence, consent and chaperones for pubertal staging examinations: a national survey. Archives of disease in childhood, 2023.PMID 36328439
- [17]Wilson, M The Use of Medical Chaperones During Physical Examinations: The Perceptions of Adolescents and Their Caregivers. Pediatric emergency care, 2024.PMID 38032984
- [18]Trubey, Rob Validity and effectiveness of paediatric early warning systems and track and trigger tools for identifying and reducing clinical deterioration in hospitalised children: a systematic review. BMJ open, 2019.PMID 31061010