Paeds · clinical-assessment-and-reasoning
Weight loss in children and adolescents
Also known as Paediatric weight loss · Unintentional weight loss children · Adolescent weight loss · Restrictive eating weight loss · Atypical anorexia
Fellowship diagnostic approach to weight loss in children and adolescents: confirm true loss, quantify severity, threat-first assessment, mechanism-based differential spanning restriction and organic disease, refeeding-aware nutrition restart, and safe disposition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A fourteen-year-old’s jeans are loose. The BMI still sits in the “healthy” band. A nine-year-old has lost three kilograms with thirst and night-time wees. A toddler’s weight is falling because juice replaced meals. These are not the same disease. They share one clinical task: prove that weight really fell, judge danger, and find mechanism before you reassure. [1]
Infant and toddler faltering growth has its own fellowship page. Use that chapter when the problem is slow weight gain or centile crossing in early childhood. This page owns true weight loss and the older-child and adolescent presentations where restriction, diabetes, inflammatory bowel disease and systemic disease dominate the exam list. Technique for weighing and charting lives on the growth-measurement page — borrow the skill; do not re-teach it here. [1]
W.E.I.G.H.T.
Overview & Definition
Weight loss means the child is lighter than a previously established baseline. That sounds simple until you meet clothes-on weights, different scales, growth spurts, and a BMI chart that still looks “fine.” Fellowship answers start with data quality, then severity, then cause. [1]
Severity is more than today’s BMI percentile. Percentage loss from premorbid weight, speed of decline, and physiological cost (heart rate, blood pressure change on standing, temperature, electrolytes, cognition) tell you who is in danger. Adolescents with atypical anorexia nervosa can lose a large fraction of body weight and still land in a numerically normal BMI band. The band does not cancel the loss. [1]
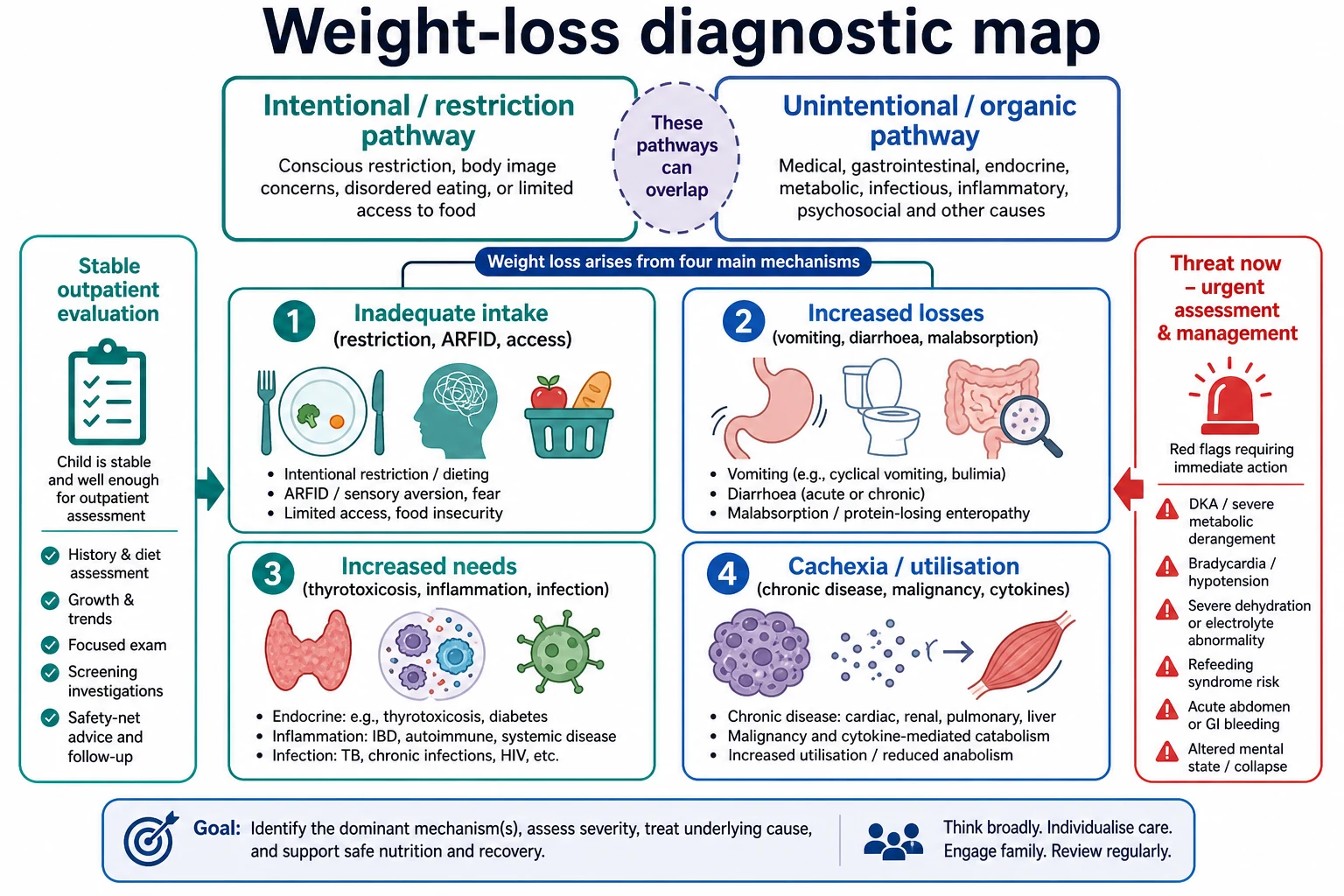
Intentional versus unintentional is a framing question, not a final label. Intentional pathways include restriction, purging, driven exercise and body-image fear. Unintentional pathways include new diabetes, malabsorption, inflammatory bowel disease, thyrotoxicosis, chronic infection, malignancy and food insecurity. Mixed pictures are common: a child with Crohn disease may also restrict because food triggers pain. Keep both doors open until the story closes them. [1]
Cachexia is not pure starvation. Evans and colleagues defined cachexia as a complex metabolic syndrome with loss of muscle, with or without fat loss, often driven by inflammation and illness. In a child with cancer or advanced chronic disease the plan is not “just eat more” alone. [1]
Classification
Think in three layers: data quality, threat, and mechanism. [1]
Data quality. Same scale when possible, minimal clothing, correct age and sex chart, and a premorbid anchor weight. A single lower clinic weight is a hypothesis until confirmed. [1]
Threat. Immediate danger includes diabetic ketoacidosis, severe dehydration, bradycardia or orthostatic instability from restriction, hypothermia, hypoglycaemia risk, suicidal crisis, and refeeding risk after prolonged undernutrition. Threat outranks elegant differential lists. [1]
Mechanism buckets. [1]
- Inadequate intake — restriction, ARFID sensory/fear avoidance, poverty, neglect, oral pain, depression. [1]
- Increased losses — vomiting, diarrhoea, malabsorption (including coeliac), protein-losing states.
- Increased needs / hypermetabolism — thyrotoxicosis, uncontrolled inflammation, infection, major burns or recovery states.
- Cachexia / disease utilisation — malignancy-related cytokines, advanced organ failure.
Eating-disorder phenotypes sit mainly in the intake bucket but create whole-body medical risk: anorexia nervosa, atypical anorexia, bulimia nervosa with weight effects, and ARFID without body-image distortion. [1]
Epidemiology & Risk Factors
Weight loss presentations cut across general paediatrics, adolescent medicine, gastroenterology and endocrinology. Restrictive eating disorders rise sharply in adolescence, with under-recognition in boys, gender-diverse youth and younger children. AAP guidance stresses active identification rather than waiting for extreme thinness. [1]
Risk climbs with dieting culture, competitive sport that rewards leanness, social media comparison, anxiety, perfectionism, prior overweight with rapid “success” on a diet, and family history of eating disorders. Neurodiversity and sensory feeding patterns raise ARFID risk. [1]
Organic weight-loss risk tracks the epidemiology of new-onset type 1 diabetes, coeliac disease, paediatric IBD and hyperthyroidism. New diabetes often declares itself with polyuria, polydipsia, weight loss and sometimes ketoacidosis. IBD may smoulder with abdominal pain, diarrhoea, poor energy and linear growth failure as well as weight loss. [1]
Social determinants matter. Food insecurity produces real loss without a rare diagnosis. Out-of-home care, family violence and caregiver mental illness change both risk and safety planning. Language discordance hides diet detail unless you use a professional interpreter. [1]
Pathophysiology
Energy balance is arithmetic until illness rewrites the rules. When intake falls below expenditure, fat and then muscle are used. Weight falls. In younger children linear growth may slow later; head growth is usually protected until late. That classic nutritional sequence still helps, but adolescents with pure restriction can look medically fragile long before height is affected. [1]
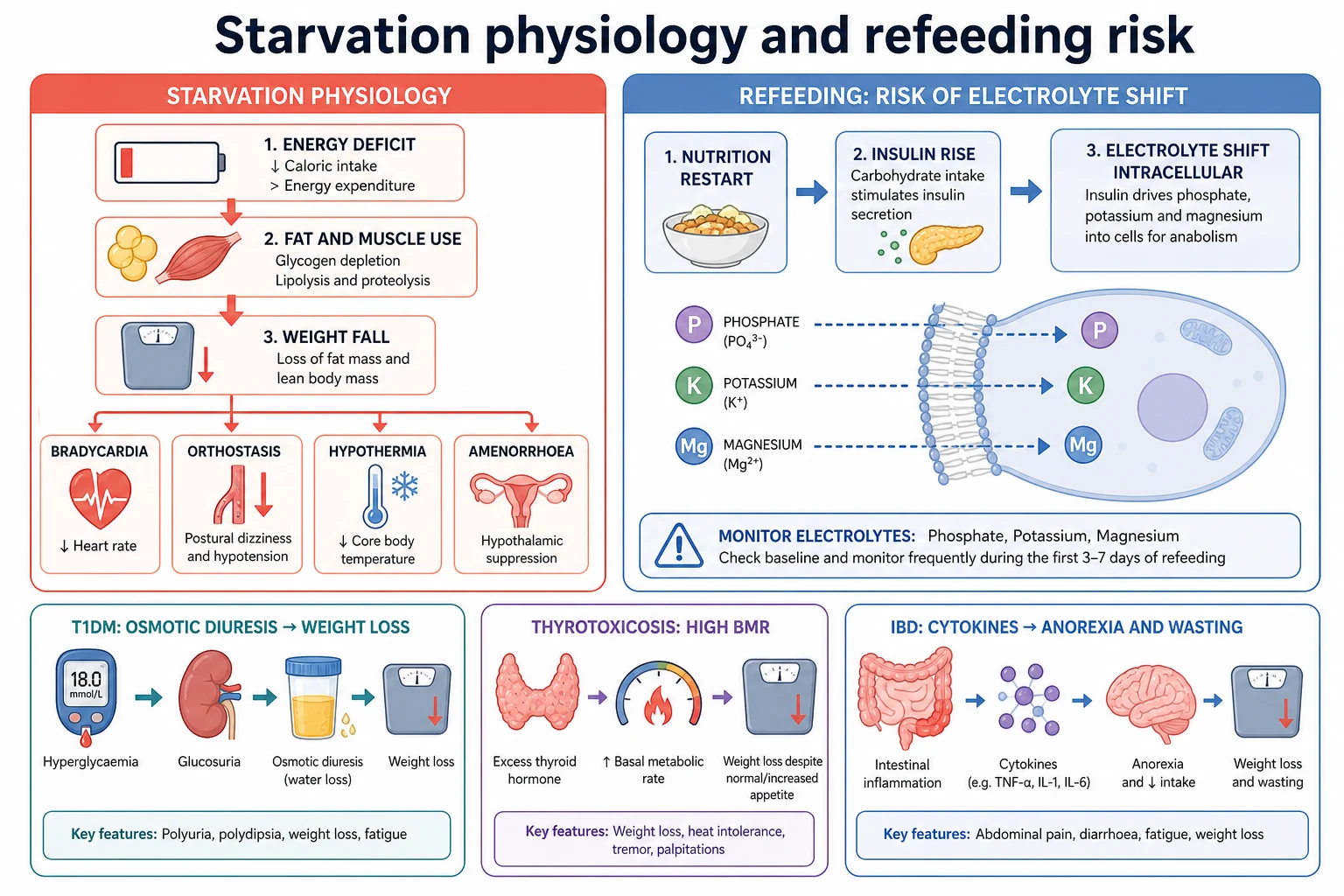
Starvation physiology explains many exam signs. Resting energy expenditure falls. Heart rate slows. Standing can drop blood pressure or raise heart rate excessively. Core temperature drifts down. Cognition narrows. Amenorrhoea and pubertal delay reflect energy shortage, not a separate primary gynaecological hobby diagnosis. Trapani’s review catalogues the multi-system medical complications of anorexia nervosa that general paediatricians must anticipate. [1]
Refeeding is the trap after the diagnosis is made. When nutrition restarts, insulin rises. Phosphate, potassium and magnesium shift into cells. Fluid balance can swing. Cardiac and respiratory complications can appear in the first days of refeeding. ASPEN consensus frames refeeding syndrome as a recognisable risk state; Garber’s review summarises approaches to refeeding in anorexia nervosa. Use supervised, protocolised restart — not an uncontrolled calorie binge. Exact electrolyte recipes are local; the principle is not. [1]
Type 1 diabetes produces weight loss through insulin deficiency: glucose spills in urine, water follows, calories are lost, and fat and muscle break down. Ketoacidosis adds volume depletion, acidosis and a child who looks acutely unwell — abdominal pain and Kussmaul breathing are classic pitfalls if you only think “gastro.” [1]
IBD and other inflammatory states combine reduced intake (pain, nausea) with cytokine-driven anorexia and increased needs. Growth failure can be as prominent as weight loss in paediatric-onset disease. [1]
Thyrotoxicosis raises basal metabolic rate. Children may eat well and still lose weight, with heat intolerance, tremor, tachycardia and sometimes goitre or eye signs. [1]
Cachexia adds inflammatory signalling that breaks down muscle even when someone is trying to feed the child. Treat the disease, not only the plate. [1]
Clinical Presentation
Families rarely open with “please run a fellowship differential.” They say the school uniform is baggy, training times improved then collapsed, “they are picky,” or “they are healthier now.” Listen for percentage change hidden inside lifestyle language. [1]
Restriction pathway clues: skipping meals, cutting food into tiny pieces, fear of specific macronutrients, excessive exercise that continues when injured, body checking, menstrual change, social withdrawal, and bathroom visits after meals. Atypical anorexia looks the same behaviourally with a less extreme BMI. [1]
ARFID clues: sensory refusal, fear of choking or vomiting after a past event, very narrow accepted food list, and no drive for thinness. Medical risk can still be high. [1]
Organic red-flag bundles: [1]
- Polyuria, polydipsia, nocturia, candida, blurred vision → diabetes until proven otherwise. [1]
- Chronic diarrhoea, blood or mucus in stool, nocturnal stool, mouth ulcers, perianal disease, delayed growth → IBD pathway. [1]
- Post-gluten gastrointestinal or extraintestinal clues with progressive loss → coeliac testing before gluten is removed. [1]
- Heat intolerance, tremor, palpitations, goitre → hyperthyroidism. [1]
- Fever, night sweats, bone pain, progressive nodes, bruising → infection or malignancy work-up. [1]
Younger children may present through the faltering-growth door. Cross-link that page when velocity failure, not acute kilogram loss, is the main pattern. [1]
Differential Diagnosis
Rank common and dangerous together. [1]
| Pattern | Think first | Do not miss |
|---|---|---|
| Adolescent, large % loss, body-image fear | Restrictive eating disorder | Medical instability; atypical anorexia |
| Narrow diet, no body-image fear | ARFID | Micronutrient deficiency, refeeding risk |
| Polyuria + polydipsia | Type 1 diabetes | DKA |
| Diarrhoea, pain, poor energy | IBD, coeliac, infection | Growth failure, delayed diagnosis |
| Good appetite, heat intolerance | Hyperthyroidism | Arrhythmia, thyroid storm rare but serious |
| Fever, sweats, nodes | Infection, malignancy | Context-specific TB/HIV risk |
| Chaotic home, multi-domain neglect signs | Inadequate provision | Parallel safeguarding |
| Chronic disease already known | Disease flare or feed-plan failure | Cachexia vs simple underfeeding |
| Use this table as a ranking aid, not a closed list. [1] |
Safeguarding-related neglect can present as weight loss or faltering. Harper’s review places growth failure within neglect frameworks without claiming every low weight is abuse. Hold both truths. [1]
Age shifts the list. Preschool: ARFID-like selectivity, chronic disease, coeliac, social risk. School-age: coeliac, IBD onset, early body image, new diabetes. Adolescent: eating disorders rise, still never drop organic gates. [1]
Clinical & Bedside Assessment
1. Stability first. Look at the child before the chart. Work of breathing, colour, interaction, hydration, glucose risk and temperature outrank percentile debate. A drowsy acidotic child with Kussmaul breathing is DKA until proven otherwise. [1]
2. Confirm and quantify loss. Re-weigh. Compare with the best premorbid weight. Calculate approximate percentage loss. Plot on the correct chart. Measure height so you can interpret BMI context without worshipping it. Check resting heart rate and orthostatic vital signs when restriction is possible. [1]
3. Take two histories: food and fear. What is offered, what is taken, who controls food, exercise minutes, purge behaviours, and body-image beliefs. In adolescents, part of this is confidential. Explain limits of confidentiality (safety) and then ask directly. [1]
4. Screen for organic drivers every time. Polyuria/polydipsia, stool pattern, blood in stool, abdominal pain, fever, night sweats, heat/cold intolerance, cough, travel, sexual history when relevant, medications and supplements (including diet pills). [1]
5. Examine with a hypothesis. Nutrition stores, lanugo, parotid enlargement, dental enamel, Russell sign, delayed puberty, goitre, tremor, abdominal masses, perianal disease, lymphadenopathy, chest findings, neurological state. Document factually. [1]
6. Mental-health and safety screen. Mood, self-harm, suicidal ideation, compulsive exercise as self-punishment, and family conflict around meals. Medical and psychiatric risk travel together. [1]
7. Social context without shame. Food security, housing, sport culture, social media, bullying, out-of-home care. Trauma-informed posture keeps the alliance usable. [1]
Investigations
Tests answer hypotheses. They do not replace a meal plan or a mental-health referral. [1]
Immediate point-of-care when unwell or polyuria/polydipsia present: glucose, blood gas/ketones as per DKA pathways, and urgent electrolytes. Do not wait for a “next-day clinic panel” if DKA is possible. [1]
Often first-line for progressive unexplained loss: full blood count, electrolytes and renal function, glucose, liver enzymes, inflammatory markers when IBD/infection is plausible, coeliac serology if gluten-exposed, thyroid function when clinically suggested, and urinalysis. Add phosphate, magnesium and ECG when restriction and refeeding risk are on the table. [1]
Directed second-line tests: faecal calprotectin or gastroenterology pathway for IBD suspicion, imaging or oncology work-up for constitutional symptoms, infectious serologies by exposure, and specialist endocrine tests after basic exclusion — not as a first shotgun. [1]
Low-yield patterns. Endless panels in clear restrictive eating with classic history can delay care, but “classic” is not a licence to skip glucose, electrolytes or ECG when physiology is abnormal. Normal labs never exclude an eating disorder. [1]
Management — Resuscitation
If the child is critically unwell, follow ABCDE and local emergency pathways. For suspected DKA, fluid and insulin management follow paediatric DKA protocols — this is not the place to invent doses. Recognise the syndrome, involve senior help, and use your hospital guideline. [1]
For restrictive eating with medical instability, think like a physician first. Bradycardia, significant orthostasis, hypothermia, dehydration, electrolyte abnormalities, arrhythmia risk, acute food refusal with medical danger, or suicidality push toward medical admission for stabilisation. SAHM statements and AAP guidance frame medical management priorities and the need for structured care rather than brief reassurance. Local numerical cut-offs vary — learn yours and state principles in exams if exact institutional numbers are not provided. [1]
Refeeding risk starts when nutrition restarts after prolonged restriction or undernutrition. Monitor clinical state and electrolytes (phosphate, potassium, magnesium) under a supervised plan informed by ASPEN and eating-disorder refeeding evidence. Do not celebrate a huge first day of intake without a monitoring plan. [1]
If safeguarding risk is high, protect the child in parallel with medical care. Document facts. Escalate per local statute. [1]
Management — Definitive & Stepwise
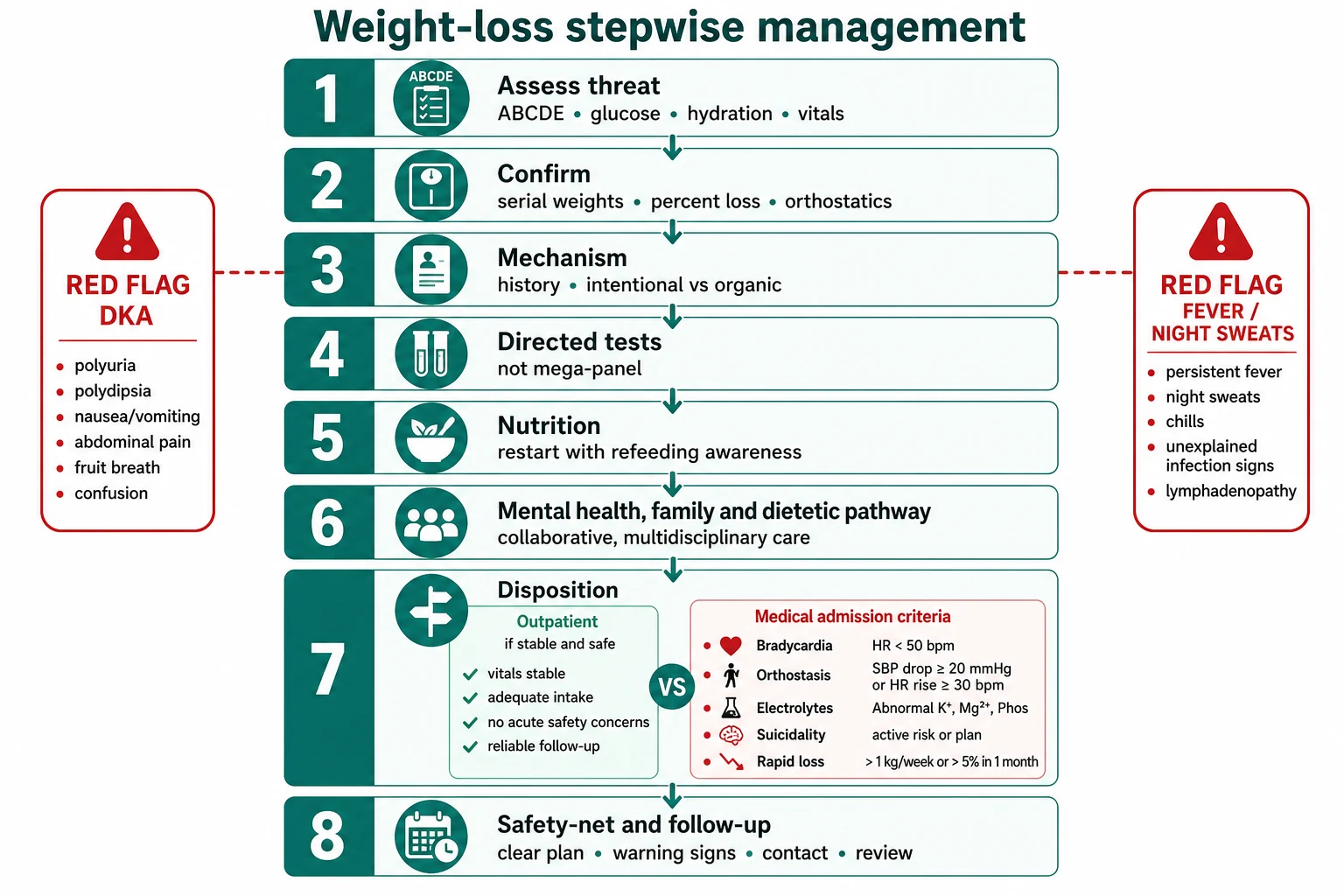
Step 1 — Name the problem representation. [1] Example: “Fifteen-year-old with 12% weight loss over four months, resting bradycardia, fear of fatness, normal BMI percentile — medically unstable restrictive eating until stabilised.” Or: “Nine-year-old with 3 kg loss, polyuria and polydipsia — new diabetes until glucose known.” [1]
Step 2 — Treat the immediate medical problem. [1] DKA pathway, fluids for dehydration, warming, electrolyte correction under protocol, and senior review for cardiovascular instability. [1]
Step 3 — Restart nutrition with eyes open. [1] Dietetic-led plans, family-based approaches for many restrictive presentations, and supervised refeeding when risk is high. Garber’s review and SAHM papers support structured medical nutrition rehabilitation rather than ad-hoc “eat what you like” advice in high-risk restriction. Exact meal plans are individual. [1]
Step 4 — Parallel mental-health care when restriction or ARFID is active. [1] Medical stabilisation is not therapy, and therapy is not a substitute for phosphate checks. Coordinate early. [1]
Step 5 — Treat organic disease specifically. [1] Insulin and education for new diabetes; gastroenterology pathways for IBD/coeliac; antithyroid pathways for Graves disease after confirmation — each on the correct specialty rails, with the general paediatrician owning the first diagnosis and handover. [1]
Step 6 — Disposition and follow-up. [1] Outpatient care needs a named review date, weight-monitoring plan, clear return precautions, and a team that actually exists in the patient’s system. Admission is a tool, not a punishment. [1]
Step 7 — Communicate without shame. [1] Explain that weight loss is a medical problem with many causes. With adolescents, balance caregiver involvement and confidential space. Use teach-back. Avoid power struggles in the first five minutes that destroy the alliance. [1]
Specific Subtypes & Scenarios
Atypical anorexia pattern. Large percentage loss, intense fear of weight gain, BMI still not “low.” Assess vital signs and electrolytes as carefully as you would for classic anorexia. [1]
New diabetes / DKA. Do not attribute weight loss and abdominal pain to a virus without glucose. Pitfalls include partial treatment with fluids only and missed cerebral oedema risk in DKA care — use paediatric protocols. [1]
IBD. Weight loss with chronic gut symptoms or isolated growth failure. Early referral beats endless symptomatic labels. [1]
Coeliac disease. Variable presentation; test before removing gluten. [1]
Hyperthyroidism. Good appetite, still losing; check TFTs when the phenotype fits. [1]
ARFID. No fat-phobia; still measure medical risk and involve feeding-skilled teams. [1]
Athlete underfuelling. Performance culture can mask restriction. Ask training load and intake explicitly. [1]
Preschool faltering boundary. If the issue is poor weight gain rather than kilogram loss, pivot to the faltering-growth approach. [1]
Neglect / food insecurity. Feed and protect; investigate enough to exclude organic disease; do not humiliate. [1]
Post-illness slide. Expected short loss should recover; failure to regain needs a new look. [1]
Complications & Pitfalls
- Reassured by normal BMI despite large percentage loss. [1]
- Missing DKA while labelling abdominal pain as gastroenteritis. [1]
- Unsafe aggressive refeeding after prolonged restriction. [1]
- Endless tests while delaying nutrition and mental-health care. [1]
- Confrontational counselling that ends the alliance. [1]
- Assuming “it is anorexia” and missing IBD or diabetes. [1]
- Assuming “labs normal” excludes restriction. [1]
- Ignoring suicidality or compulsive exercise risk. [1]
- No interpreter for a detailed diet history. [1]
Prognosis & Disposition
Many children and adolescents recover weight and health when medical risk is managed and the right team stays involved. Restrictive eating disorders can become chronic without structured care; early medical identification improves the chance of a usable pathway. [1]
Organic causes track the prognosis of the underlying disease — new diabetes needs lifelong systems, IBD needs disease control for growth recovery, thyrotoxicosis usually responds once treated. [1]
Safe discharge after medical stabilisation means stable vitals and electrolytes for the local protocol, a written nutrition plan, mental-health follow-up if indicated, caregiver understanding, and clear return precautions (dizziness, fainting, chest pain, ongoing loss, mood crisis, polyuria). [1]
Special Populations
Younger children more often need ARFID, coeliac, chronic disease and neglect lenses; body-image anorexia is less common but not impossible. [1]
Adolescents need confidential enquiry, sport and social-media context, and explicit medical criteria for admission. [1]
Gender-diverse and neurodiverse youth carry higher rates of disordered eating and need respectful, adapted communication. [1]
Athletes may present with “performance nutrition” that is actually energy deficit. [1]
Indigenous families need culturally safe, non-racialised conversations about food and body size. [1]
Migrant and refugee children may have dual infection–nutrition risk and interrupted records; use interpreters. [1]
Medical complexity can lose weight when feeds, devices or carer systems fail — treat the system. [1]
Out-of-home care treats weight trajectory as a welfare vital sign. [1]
Evidence, Guidelines & Regional Differences
AAP’s clinical report (Hornberger and colleagues) is a core US-facing synthesis for identification and management of eating disorders in children and adolescents. [1]
SAHM position statements (2015 and 2022 updates) set expectations for medical management of restrictive eating disorders in adolescents and young adults, including the medical nature of complications and need for structured care. [1]
Trapani’s 2025 Pediatrics review consolidates medical complications of anorexia nervosa for clinicians who must anticipate multi-system risk. [1]
Robatto and colleagues and Kambanis and colleagues summarise diagnosis/treatment landscapes for eating disorders and ARFID. Bohon and colleagues synthesise US practice guidelines. Harrington remains a practical primary-care evaluation frame. [1]
Diabetes and DKA sources (Ziegler; Veauthier; Kostopoulou) anchor the polyuria–polydipsia–weight-loss emergency gate. [1]
Paediatric IBD (Rosen; Ishige; Veauthier), coeliac (Riznik; Al-Toma/ESsCD) and hyperthyroidism (Vaidyanathan) cover major organic pathways. [1]
ASPEN refeeding consensus and Garber’s refeeding review guide safe nutrition restart principles. [1]
For younger children with velocity problems rather than acute loss, Homan, Gonzalez-Viana (NICE faltering growth) and Shields remain the bridge literature. [1]
Local children’s hospital pathways (for example RCH-style clinical guidelines) and regional eating-disorder services operationalise admission and outpatient criteria. Pair medical care with culturally safe practice for Aboriginal and Torres Strait Islander families and Te Tiriti-informed care in Aotearoa New Zealand. [1]
NICE NG69 shapes recognition and treatment of eating disorders; NICE NG75 faltering-growth language covers younger velocity problems. Use UK-WHO chart plotting conventions in child health records. [1]
AAP and SAHM documents dominate teaching language; AFP practical reviews support outpatient evaluation. Chart policy often uses WHO under 24 months and CDC thereafter for growth context (cross-link measurement topic). [1]
Adolescent medicine and provincial eating-disorder programmes vary by region; growth monitoring aligns with WHO early-years standards. Follow local admission and mental-health access pathways. [1]
Exam Pearls
- Percentage loss and physiology beat a single BMI number. [1]
- Polyuria + polydipsia + weight loss → glucose now. [1]
- Bradycardia and orthostasis are medical findings. [1]
- Refeeding watch: phosphate, potassium, magnesium. [1]
- ARFID lacks fat-phobia; still assess medical risk. [1]
- Normal labs ≠ no eating disorder. [1]
- Do not miss IBD or thyrotoxicosis because the stem “sounds psychiatric.” [1]
- Cross-link FTT for infants; own adolescent loss here. [1]
- Confidential adolescent history is a core skill. [1]
- Safety-net every disposition. [1]
High-yield anchors
References
- [1]Hornberger LL Identification and Management of Eating Disorders in Children and Adolescents. Pediatrics, 2021.PMID 33386343
- [2]Society for Adolescent Health and Medicine Medical Management of Restrictive Eating Disorders in Adolescents and Young Adults. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2022.PMID 36058805
- [3]Society for Adolescent Health and Medicine Position Paper of the Society for Adolescent Health and Medicine: medical management of restrictive eating disorders in adolescents and young adults. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2015.PMID 25530605
- [4]Trapani S Medical Complications of Anorexia Nervosa. Pediatrics, 2025.PMID 40659363
- [5]Robatto AP Diagnosis and treatment of eating disorders in children and adolescents. Jornal de pediatria, 2024.PMID 38158193
- [6]Kambanis PE Assessment and Treatment of Avoidant/Restrictive Food Intake Disorder. Current psychiatry reports, 2023.PMID 36640211
- [7]Veauthier B Diabetic Ketoacidosis: Evaluation and Treatment. American family physician, 2024.PMID 39556629
- [8]Kostopoulou E Diabetic Ketoacidosis in Children and Adolescents; Diagnostic and Therapeutic Pitfalls. Diagnostics (Basel, Switzerland), 2023.PMID 37568965
- [9]Ziegler R Diabetes in Childhood and Adolescence. Deutsches Arzteblatt international, 2018.PMID 29563012
- [10]Rosen MJ Inflammatory Bowel Disease in Children and Adolescents. JAMA pediatrics, 2015.PMID 26414706
- [11]Ishige T Growth failure in pediatric onset inflammatory bowel disease: mechanisms, epidemiology, and management. Translational pediatrics, 2019.PMID 30881894
- [12]Veauthier B Crohn's Disease: Diagnosis and Management. American family physician, 2018.PMID 30485038
- [13]Riznik P Clinical Presentation in Children With Coeliac Disease in Central Europe. Journal of pediatric gastroenterology and nutrition, 2021.PMID 33306584
- [14]Al-Toma A European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United European gastroenterology journal, 2019.PMID 31210940
- [15]Vaidyanathan P Update on Pediatric Hyperthyroidism. Advances in pediatrics, 2022.PMID 35985711
- [16]da Silva JSV ASPEN Consensus Recommendations for Refeeding Syndrome. Nutrition in clinical practice : official publication of the American Society for Parenteral and Enteral Nutrition, 2020.PMID 32115791
- [17]Garber AK A systematic review of approaches to refeeding in patients with anorexia nervosa. The International journal of eating disorders, 2016.PMID 26661289
- [18]Harrington BC Initial evaluation, diagnosis, and treatment of anorexia nervosa and bulimia nervosa. American family physician, 2015.PMID 25591200
- [19]Homan GJ Failure to Thrive: A Practical Guide. American family physician, 2016.PMID 27548594
- [20]Gonzalez-Viana E Faltering growth in children: summary of NICE guidance. BMJ (Clinical research ed.), 2017.PMID 28963099
- [21]Evans WJ Cachexia: a new definition. Clinical nutrition (Edinburgh, Scotland), 2008.PMID 18718696
- [22]Białek-Dratwa A ARFID-Strategies for Dietary Management in Children. Nutrients, 2022.PMID 35565707
- [23]Bohon C United States-based practice guidelines for children and adolescents with eating disorders : Synthesis of clinical practice guidelines. Journal of eating disorders, 2025.PMID 40217324
- [24]Kerem NC Respiratory acidosis in adolescents with anorexia nervosa hospitalized for medical stabilization: a retrospective study. The International journal of eating disorders, 2012.PMID 21321988
- [25]Shields B Weight faltering and failure to thrive in infancy and early childhood. BMJ (Clinical research ed.), 2012.PMID 23014901
- [26]Harper NS Neglect: failure to thrive and obesity. Pediatric clinics of North America, 2014.PMID 25242707