Paeds · ent-hearing-and-oral-health
Drooling, dysphagia and upper-aerodigestive disorders
Also known as Sialorrhoea · Paediatric dysphagia · Feeding and swallowing difficulty in children · Aspiration in neurodisability
Fellowship guide to drooling (sialorrhoea), dysphagia and the upper-aerodigestive disorders of childhood; the distinction between anterior drooling (visible, social and skin impact) and posterior drooling (silent, carrying aspiration and recurrent chest infection risk); drooling as a clearance problem of oromotor impairment rather than saliva overproduction; classification of dysphagia into oropharyngeal transfer and oesophageal transport forms; the four swallow phases and where each fails; overt and silent aspiration; the Drooling Severity and Frequency Scale and the clinical swallow evaluation; the roles of videofluoroscopic swallow study and fiberoptic endoscopic evaluation of swallowing; the stepwise drooling ladder from oromotor therapy and positioning through glycopyrrolate (glycopyrronium) and sublingual atropine, botulinum toxin injection of the salivary glands, and surgery; eosinophilic oesophagitis and structural aerodigestive anomalies; and the decisions around gastrostomy and oesophagogastric dissociation in the child with an unsafe swallow.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the six-year-old with severe cerebral palsy who comes to clinic with a permanently damp bib, raw skin around her chin, and a chest that has been treated twice this winter for infection. Her parents are exhausted by two-hour mealtimes and anxious about how she will manage at school. That single child holds the whole of this topic in her story: the saliva she cannot keep in her mouth (drooling), the food and drink she struggles to transfer safely to her stomach (dysphagia), and the airway that bears the consequences when either goes wrong (aspiration). The three problems travel together because they share one anatomy and one set of oromotor skills, and the clinician who treats one without noticing the others will miss harm. [5] [7]
Drooling (sialorrhoea) is the unintentional loss of saliva from the mouth. The common but crucial teaching point is that it is almost always a problem of handling saliva — poor lip seal, slow and discoordinated swallowing, reduced sensory awareness, poor head and trunk control — rather than of making too much saliva. Children with cerebral palsy produce similar or smaller volumes of saliva than their peers; they simply clear it less well. This reframes the whole management strategy toward improving clearance, not merely drying the child up. [5] [1]
Dysphagia is difficulty moving food, liquid or saliva from the mouth to the stomach. In childhood it splits cleanly into two forms that are investigated and managed quite differently: oropharyngeal (transfer) dysphagia, where the problem is in the mouth and throat and is usually neuromuscular. Oesophageal (transport) dysphagia is where the problem is in the food pipe and is usually structural or inflammatory. The bedside clue that separates them is the timing of the difficulty relative to the swallow: oropharyngeal dysphagia is a struggle during the swallow (coughing, choking, a wet voice). Oesophageal dysphagia is a struggle after the swallow has cleared the throat (food sticks, regurgitates, or does not pass). [7] [10]
Why this matters at fellowship level is that these are exactly the children who fall between specialties — paediatrics, neurodisability, ENT, speech-language therapy, dietetics, gastroenterology and respiratory — and the general paediatrician is expected to hold the whole picture. The high-yield skills are recognising posterior drooling and silent aspiration as dangerous, applying the stepwise ladder rather than jumping to surgery, and making defensible, family-centred decisions about the airway, feeding and quality of life in a child whose swallow will never be normal. [11] [8]
Classification
These disorders classify cleanly when you keep three questions separate: which direction does the saliva go, where in the swallow does the food stick, and is the airway involved. Mixing them up is how candidates treat the wet chin without noticing the wet lung. [5] [11]
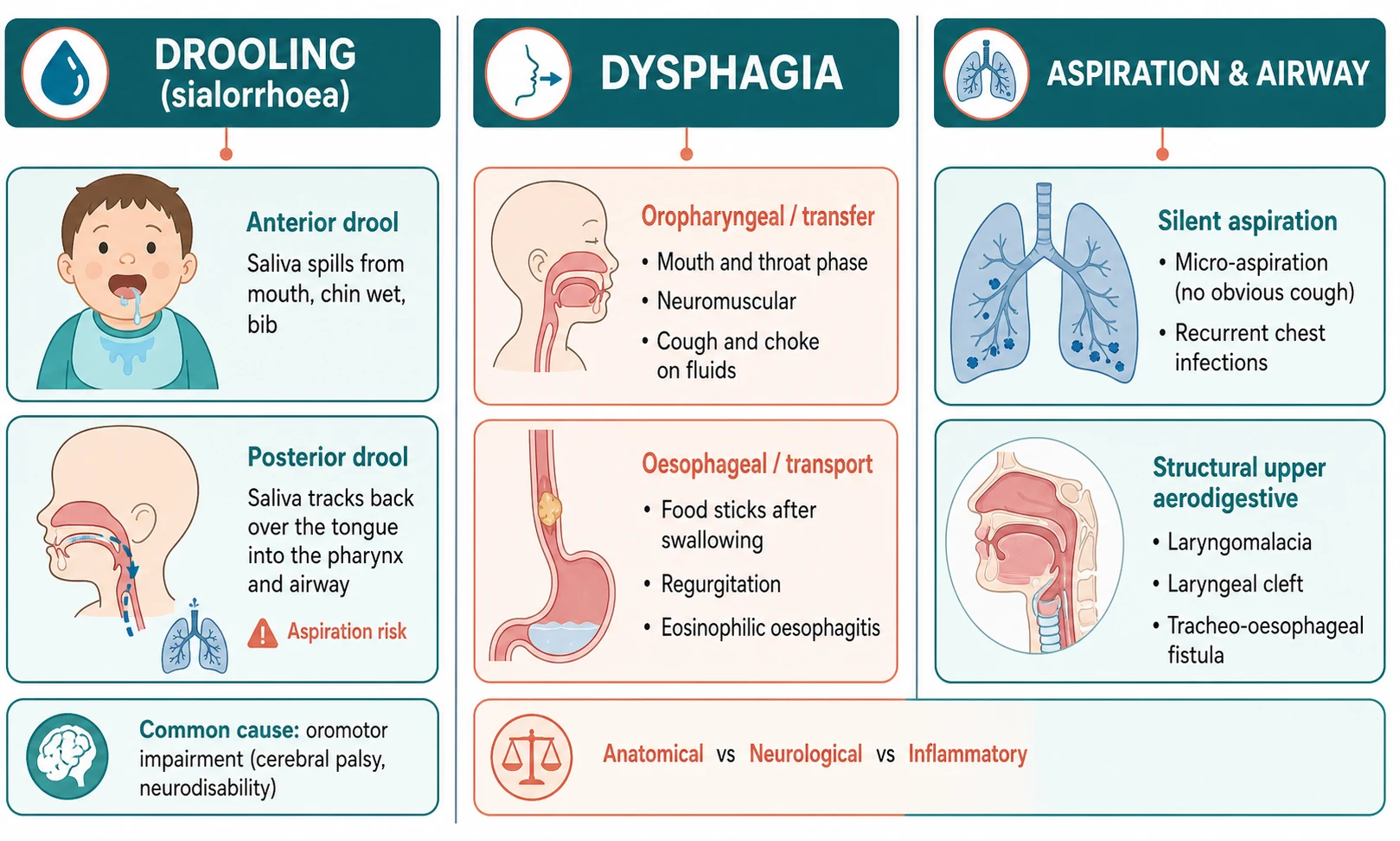
By direction of saliva flow, drooling divides into anterior and posterior. Anterior drooling is the visible form — saliva spills forward over the lip and down the chin, causing damp clothing, skin excoriation, dehydration, and social and educational difficulties. Posterior drooling is the silent, dangerous form — saliva tracks backward over the back of the tongue into the pharynx and down toward the larynx, where it is aspirated. A child can have one or both, and the clinical priority is not how wet the chin looks but whether the airway is being soiled. This single distinction drives how aggressively you intervene. [6] [5]
By site of the swallow problem, dysphagia divides into oropharyngeal and oesophageal. Oropharyngeal dysphagia is a problem of the oral preparatory, oral and pharyngeal phases, usually due to neuromuscular impairment — cerebral palsy, neuromuscular disease, brain injury — and it presents with coughing, choking, a wet or gurgly voice, nasal regurgitation and prolonged, effortful meals. Oesophageal dysphagia is a problem of transport through the food pipe, usually structural or inflammatory — stricture, eosinophilic oesophagitis, vascular ring, achalasia — and it presents with food sticking after the swallow, regurgitation, food impaction and, in young children, refusal or distress on feeding. They share the word dysphagia and little else. [7] [10]
The numbers that anchor your viva
A third axis is whether the airway is compromised, captured by aspiration and by the structural upper-aerodigestive disorders. Aspiration may be overt (coughing, choking, desaturation during feeds) or, more often in neurodisability, silent — no protective cough, but recurrent lower-respiratory infections, chronic lung change, wheeze and faltering growth. The structural disorders — laryngomalacia, posterior laryngeal cleft, tracheo-oesophageal fistula and vascular ring — cause feeding and breathing symptoms together because they sit at the shared crossroads of the airway and the food passage, and they are evaluated by the aerodigestive team. [9] [10]
Epidemiology & Risk Factors
Drooling and dysphagia are, overwhelmingly, the problems of children with neurodisability and structural upper-aerodigestive anomaly, and the risk profile follows that population. Drooling is uncommon and self-limiting in typically developing toddlers (it usually resolves by two to three years as oromotor control matures), so persistent or severe drooling beyond early childhood should always prompt a search for an underlying cause. [5] [7]
The strongest single risk factor for problematic drooling is cerebral palsy, particularly the dyskinetic and severe spastic forms and Gross Motor Function Classification System level IV to V, where poor head and trunk control, poor lip seal, dyskinetic oromovements and reduced swallow frequency combine. Around one in five children with cerebral palsy drool to a degree that interferes with daily life, rising to a third or more in the most severely affected. Other neurodisabilities — intellectual disability, acquired brain injury, neuromuscular disease and certain syndromes — carry a similar burden. [5] [1]
The risk factors for dysphagia are the conditions that impair the oropharyngeal or oesophageal phases of swallowing. On the neuromuscular side these are cerebral palsy, neuromuscular disorders, brainstem lesions and severe intellectual disability; on the structural side, repaired oesophageal atresia and tracheo-oesophageal fistula, laryngeal cleft, and the airway anomalies of the infant (laryngomalacia, tracheomalacia). On the inflammatory side sit eosinophilic oesophagitis and peptic stricture from uncontrolled gastro-oesophageal reflux. The child with severe cerebral palsy often has several of these at once, which is why a single intervention rarely solves the whole problem. [7] [9]
The factors that tip drooling from a minor nuisance to a clinical problem are worth naming because they are also the targets of management: poor posture and head control, mouth breathing (often from adenoidal hypertrophy or nasal obstruction), dental disease and malocclusion, reduced sensory awareness of the saliva. Medications that increase saliva production, such as some antipsychotics and cholinergic agents, also contribute. Removing an aggravating factor is sometimes the most effective single move. [5] [11]
Pathophysiology
To understand how drooling and dysphagia happen you need two mechanical pictures: the four phases of swallowing, and the normal handling of saliva between swallows. Most drooling is a failure of the second, and most oropharyngeal dysphagia is a failure of the first. [7] [1]
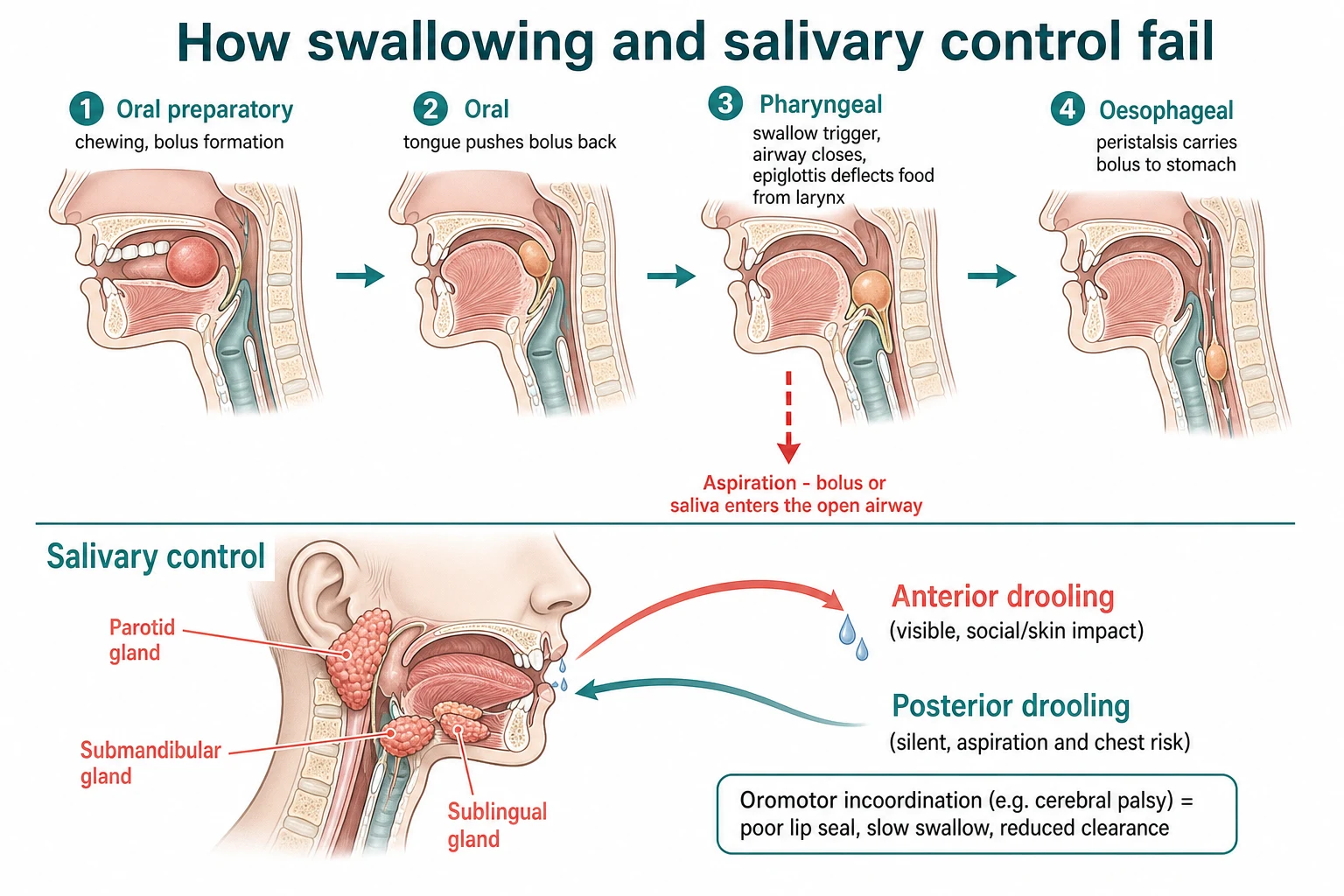
Swallowing runs through four phases. In the oral preparatory phase the child takes in food, chews (or forms the bolus with the tongue) and mixes it with saliva; in the oral phase the tongue pushes the bolus backward to the pharynx. In the pharyngeal phase the swallow is triggered, the airway is protected by closure of the larynx and tilt of the epiglottis, and the bolus is swept through the pharynx into the oesophagus. In the oesophageal phase peristalsis carries the bolus to the stomach. Oropharyngeal dysphagia is a failure of the first three phases, and aspiration occurs when, at the pharyngeal phase, residue or a mistimed bolus enters the unprotected airway. [7] [9]
Saliva, by contrast, is managed not in discrete swallows but by frequent, unconscious clearance — a swallow roughly every minute, day and night, coordinated by intact oromotor and sensory function. Drooling emerges when this clearance slows or breaks down. Poor lip seal lets saliva escape forward; slow, discoordinated and infrequent swallows leave saliva pooling in the mouth; reduced head and trunk control prevents gravity from helping; and reduced oral sensation means the child does not register the pool and trigger a swallow. The net result is the same volume of saliva handled badly, which is why the strategy is to improve clearance and, when that is insufficient, to reduce saliva production. [5] [1]
Aspiration and reflux reinforce one another, which is why a child's chest often deteriorates and a single cause is hard to pin down. Saliva, food and gastric contents can all be aspirated; chronic micro-aspiration inflames and scars the airway; and reflux that reaches the pharynx may trigger reflex laryngospasm or be aspirated itself. Morton and colleagues showed in children with severe neurodisability that respiratory tract infections were driven by both direct aspiration of oropharyngeal contents and by reflux aspiration, The two were often entangled, so the practical lesson is that protecting the airway usually means addressing both the swallow and the reflux. [9] [8]
Clinical Presentation
The presentation of these disorders is shaped by whether the problem is drooling, dysphagia or aspiration, but in the child with neurodisability all three are often present and the family history is the richest source of information. Take a careful feeding and saliva history: the time taken for meals, fatigue, coughing or choking, wet-sounding voice or breathing during or after feeds, recurrent chest infections, weight and growth, skin problems from saliva, and the social and educational impact. [5] [7]
Drooling presents as visible, persistent saliva loss from the mouth — wet chin, damp clothing and bibs, perioral skin excoriation and secondary infection, and dehydration if the child cannot manage fluids well. The family will describe the social burden: difficulty at school, damaged books and equipment, rejection by peers, and the time and cost of constant laundry and clothing changes. Always ask specifically about posterior features — a wet or rattly chest, recurrent infections, a gurgly breathing pattern — because the wet chin may be the lesser problem. [5] [6]
| Picture | Bedside findings | Immediate response |
|---|---|---|
| Anterior drooling | Persistent saliva loss over chin; raw perioral skin; damp bibs; socially limiting | Oromotor therapy and posture; anticholinergic if persistent and impacting quality of life |
| Posterior drooling | Wet or rattly chest, recurrent infections, gurgly breathing, faltering growth | Treat as airway risk: assess swallow, lower threshold to pharmacological and surgical saliva reduction |
| Oropharyngeal dysphagia | Coughing, choking, wet voice, nasal regurgitation, long meals, chest infections | Clinical swallow evaluation; instrumental assessment; texture modification; consider enteral feeding |
| Oesophageal dysphagia | Food sticking after swallow, regurgitation, impaction, feeding refusal | Endoscopy with biopsy for eosinophilic oesophagitis; contrast study for structural causes |
| Acute aspiration event | Sudden cough, distress, desaturation or cyanosis during a meal | Clear airway, stop oral intake, urgent assessment; consider foreign body or impaction |
Oropharyngeal dysphagia presents during the swallow. The infant may cough, choke, gag or go blue on feeds, take a long time, tire, sweat with effort, or refuse feeds; there may be nasal regurgitation, a wet or gurgly voice after swallowing, or pooling of residue in the cheek or pharynx. In the older child, meals are long and effortful, the child tires or refuses, and chest infections recur. The trap is the child whose swallow is unsafe but who does not cough — silent aspiration — where the only clues are the chest and the growth chart. [7] [9]
Oesophageal dysphagia presents after the swallow has cleared the throat. The child describes food sticking, chest discomfort, regurgitation of undigested food, or food impaction; young children may simply refuse solids or favour liquids and soft foods. Food impaction in an older child or adolescent, particularly with atopy, should raise eosinophilic oesophagitis specifically, and progressive or persistent dysphagia warrants endoscopy with biopsy rather than reassurance. [10]
Atypical presentations should always shift your thinking: sudden onset of drooling or feeding difficulty in a previously well child suggests an acute cause (infection, foreign body, oesophageal impaction, medication effect) rather than chronic neurodisability; new or worsening dysphagia may indicate a stricture or eosinophilic oesophagitis. A child whose chest has deteriorated while on anticholinergic medication may have developed thickened secretions that are harder still to clear. [11] [10]
Differential Diagnosis
Sort the differential into three groups: the mimics of drooling that are not oromotor, the causes of oesophageal dysphagia that must not be missed, and the structural aerodigestive anomalies. The aim is to confirm the mechanism while always checking that a treatable contributor has not been overlooked. [5] [10]
Oromotor drooling
the diagnosis to confirm
- Neurodisability (cerebral palsy), poor oromotor control
- Persistent beyond early childhood
- Anterior and/or posterior pattern
- Treat clearance, posture and swallow
Hypersalivation mimics
- Teething in infancy (self-limiting)
- Oral inflammation, dental disease, gingivitis
- Gastro-oesophageal reflux
- Drugs (antipsychotics, cholinergics)
Oesophageal dysphagia
- Food sticks after the swallow
- Eosinophilic oesophagitis (atopy, impaction)
- Peptic stricture from reflux
- Achalasia, vascular ring
Structural aerodigestive
- Laryngomalacia (infant stridor)
- Posterior laryngeal cleft (aspiration)
- Tracheo-oesophageal fistula
- Vascular ring (dysphagia plus airway)
Silent aspiration
- No cough; recurrent chest infections
- Wet voice, chronic lung change
- Faltering growth
- Confirm by instrumental swallow study
The important mimics of drooling to exclude are the causes of true hypersalivation, because treating those is different from drying the child. Teething produces mild, self-limiting drooling in infants and resolves as dentition matures; oral inflammation from dental disease, gingivitis or mucosal infection increases saliva and is relieved by treating the mouth; gastro-oesophageal reflux can increase salivation. Certain medications, particularly antipsychotics and cholinergic agents, also increase saliva production. A child with new drooling should have the mouth and the medication list checked before saliva-reducing therapy is started. [5] [11]
Within oesophageal dysphagia, the diagnosis that examiners most want you to name is eosinophilic oesophagitis, a chronic immune-mediated inflammation of the oesophagus that presents in children with feeding difficulty, food refusal, vomiting, abdominal or chest pain, and — classically in adolescents — food impaction. It is diagnosed on upper gastrointestinal endoscopy with biopsy showing oesophageal eosinophilia, and it is managed with dietary exclusion, proton pump inhibition and, where needed, topical swallowed corticosteroid or endoscopic dilation. Peptic stricture from chronic reflux, achalasia (regurgitation of undigested food, weight loss) and vascular ring (dysphagia with respiratory symptoms in infancy) complete the structural differential. [10]
Clinical & Bedside Assessment
Assessment is clinical and multidisciplinary, and it rests on observing the child feed and on systematic measurement of the saliva problem — because you cannot treat what you have not quantified. Take a structured feeding history, examine the oromotor and respiratory systems, watch a meal, and use a validated severity scale so that change can be measured over time and across interventions. [5] [7]
The drooling assessment uses validated scales that capture both severity and frequency, because a child who drools constantly at a low rate is a different problem from one who drools intermittently but in large volumes. The Drooling Severity and Frequency Scale (Thomas-Stonell and Greenberg) grades severity from dry (1) to profuse, with saliva pooling and requiring continuous wiping (5), and frequency from never (1) to constantly (4). The Drooling Impact Scale measures the effect on the child and family over time and is well suited to tracking response to an intervention. Because anterior scales miss the dangerous form, the Paediatric Posterior Drooling Scale specifically captures the silent, aspiration-prone posterior pattern — the single most important distinction in the assessment. [6] [5]
The clinical swallow evaluation by a speech-language therapist observes the child's oral structures, tone and sensation, how the bolus is formed and controlled, the timing and coordination of the swallow, and the voice quality and breathing after the swallow. Signs of concern are poor bolus control, residue in the mouth or pharynx, a delayed or absent swallow, a wet or gurgly voice, cough or throat-clearing during or after the swallow, and desaturation. The clinical evaluation raises and ranks suspicion, but it cannot reliably detect silent aspiration — which is why instrumental assessment is needed when the swallow is in doubt. [7] [9]
Grading the risk to drive the intervention
Acute aspiration or refractory disease
Acute event, chronic lung damage or failure of maximal therapy; consider airway-protection surgery and oesophagogastric dissociation
Deliberately avoid the common errors: treating a wet chin without asking about the chest (missing posterior drooling and silent aspiration); relying on a single swallow study when aspiration is intermittent; starting anticholinergic medication without a baseline swallow and chest assessment; and forgetting to check the mouth, the posture and the medication list for a treatable contributor. Assessment is a team activity, and the general paediatrician's job is to assemble and interpret it, not to perform every test. [11] [7]
Investigations
These disorders are largely diagnosed clinically, with instrumental tests reserved for confirming an unsafe swallow, characterising an oesophageal problem, or defining a structural anomaly. The choice of swallow study is a high-yield fellowship point because the two main tests answer different questions. [7] [10]
The videofluoroscopic swallow study (VFSS) is the reference test for oropharyngeal dysphagia. The child is given radio-opaque liquids and foods of different textures while fluoroscopy captures the swallow in real time, allowing direct visualisation of bolus control, swallow timing, residue, penetration (material entering the laryngeal vestibule) and aspiration (material passing below the vocal cords), and silent aspiration in particular. Its strengths are that it assesses all four phases and allows compensatory strategies to be tested on the spot; its limitations are radiation exposure (kept low with pulsed screening), the need for cooperation, and that it samples only a short period and may miss intermittent aspiration. [7] [9]
Fiberoptic endoscopic evaluation of swallowing (FEES) is a bedside alternative in which a flexible endoscope is passed through the nose to view the pharynx and larynx before and after swallows of dyed liquids and foods. It is particularly good at assessing pharyngeal residue and secretion pooling, at detecting laryngeal penetration and aspiration, and at being repeated at the bedside without radiation, but it does not assess the oral phases and the view is briefly obscured during the swallow itself. The two tests are complementary rather than interchangeable: VFSS for the whole swallow and to test compensations, FEES for secretion management and bedside monitoring. [7]
For oesophageal dysphagia, upper gastrointestinal endoscopy with biopsy is the key investigation, because it both visualises and samples the mucosa — diagnosing eosinophilic oesophagitis (oesophageal eosinophilia on biopsy, typically 15 or more eosinophils per high-power field), peptic stricture and other mucosal disease, and allowing dilation where a stricture is present. Contrast swallow and airway endoscopy define structural aerodigestive anomalies such as laryngeal cleft, recurrent or H-type tracheo-oesophageal fistula, and vascular ring, while pH or impedance monitoring characterises reflux that may be driving aspiration or peptic disease. [10] [9]
Management — Resuscitation
For the small number of children with an acutely unsafe swallow or an aspiration event, the priority shifts to airway protection and stabilisation. Stop oral intake, clear the airway, assess breathing and circulation, give oxygen and respiratory support as needed, and arrange urgent assessment — recognising that an acute event may be an aspiration of food, saliva or gastric contents, or may signal an oesophageal foreign body or food impaction that needs urgent endoscopic removal. [9] [8]
A child with an acutely unsafe swallow who cannot safely take anything by mouth needs enteral access — initially a nasogastric tube for short-term nutrition and medication, with definitive feeding access (a gastrostomy, or a jejunostomy when reflux and aspiration are severe) once the need is established. Aspiration pneumonia is managed with respiratory support, chest physiotherapy and antibiotics directed at the likely pathogens, while the underlying cause — the unsafe swallow and any reflux — is addressed in parallel, because recurrent aspiration will defeat any amount of antibiotic treatment if the swallow is not protected. [9] [8]
For the much larger group of children with chronic but not acutely dangerous drooling and dysphagia, "resuscitation" means establishing safety: confirming whether the swallow is safe, optimising posture and chest health, treating reflux if present, ensuring nutrition and hydration, and putting in place the oromotor and positioning strategies that are the foundation of everything that follows. [5] [7]
Management — Definitive & Stepwise
Definitive management is built on two stepwise ladders — one for drooling and one for dysphagia — climbed in order and only as far as the child needs. The discipline is to start at the bottom, measure the response with a validated scale, and step up for impact or airway risk rather than jumping straight to the most aggressive option. [11] [5]
The drooling ladder — step up as needed
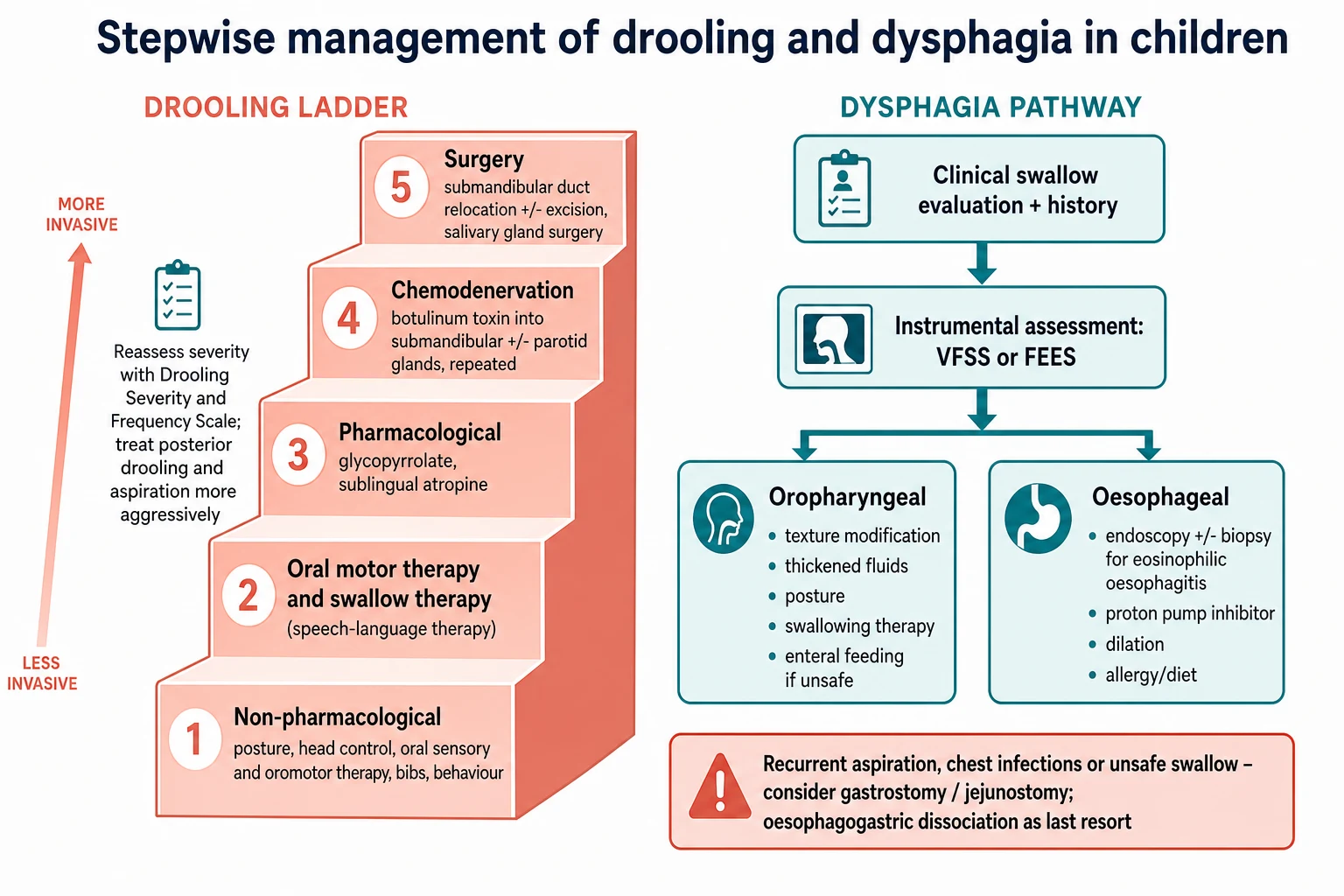
Non-pharmacological: posture and head control, oral hygiene and dental care, treat nasal obstruction and mouth breathing, bibs and skin care, and behavioural strategies.
Oromotor and swallow therapy: speech-language therapy to improve lip seal, tongue control, oral sensory awareness and swallow frequency.
Pharmacological: an anticholinergic to reduce saliva production — glycopyrrolate (glycopyrronium) oral, weight-based and titrated; sublingual atropine as an alternative or adjunct.
Chemodenervation: botulinum toxin injected into the submandibular and, where needed, parotid salivary glands, repeated every few months.
Surgery: submandibular duct relocation with or without submandibular gland excision, and parotid duct ligation or relocation, for refractory or posterior disease.
Step one and two — therapy, posture and oral care. These are the foundation and are never optional, because no drug or operation replaces them. Optimise head and trunk posture so gravity can help clearance; treat nasal obstruction and mouth breathing (often adenoidal hypertrophy) so the child can close the mouth and seal the lips; maintain oral hygiene and dental health, which reduce salivary stimulation and skin complications; and provide skin protection and bibs. Speech-language therapy works on lip closure, tongue control, oral sensory awareness and swallow frequency, and should be delivered before and alongside any medication. [5] [7]
Step three — pharmacological saliva reduction. The first-line agent is an anticholinergic, which reduces saliva production by blocking muscarinic receptors. Glycopyrrolate (glycopyrronium) given orally is the best-studied and most used; in the seminal double-blind dose-ranging study by Mier and colleagues it reduced drooling in a weight-based, titrated regimen (per-dose ranges in trials of around 0.04 to 0.1 mg/kg), and a recent randomised trial of an oral glycopyrronium solution confirmed significant benefit in children and adolescents with severe sialorrhoea and neurodisability. Sublingual atropine (a 1% solution in small, weight-based volume under the tongue) is an alternative or adjunct when glycopyrrolate is unavailable or poorly tolerated; a network meta-analysis of pharmacological treatments for sialorrhoea supports the anticholinergics as effective relative to placebo. The shared adverse effects — dry mouth, thickened secretions that can paradoxically worsen swallow and airway clearance, constipation, urinary retention, blurred vision, flushing, irritability and reduced sweating with hyperthermia — are the reason every child started on these drugs needs a baseline and repeat swallow and chest assessment, and prompt review if the chest deteriorates. [1] [3] [12]
Drugs for problematic drooling
Step four — chemodenervation with botulinum toxin. When oral therapy is insufficient or not tolerated, botulinum toxin A injected into the submandibular salivary glands (and, where needed, the parotid glands) reduces saliva production for around three to four months. Reid and colleagues showed in a randomised trial that botulinum toxin into the salivary glands reduced drooling in children with neurological disorders, and it has become a mainstay for moderate to severe disease. Its risks are local pain and infection, thickened and tenacious secretions that may worsen swallow and airway clearance, and — rarely — generalised weakness from toxin spread, which is why it is delivered by a specialist with attention to dose and distribution. It is repeatable, which makes it useful for the child who needs relief while a longer-term plan is made. [2] [11]
Step five — surgery. For refractory, severe or predominantly posterior drooling, surgery offers a durable solution. The principal operation is submandibular duct relocation (rerouting the ducts so the submandibular saliva drains backward into the pharynx rather than into the mouth), performed with or without submandibular gland excision; parotid duct ligation or relocation may be added when parotid saliva contributes. A randomised trial comparing surgery with botulinum toxin found surgery more durable for reducing drooling and improving daily life, at the cost of the usual surgical risks — infection, ranula formation, and thickened secretions — so surgery is reserved for children who have failed or outgrown less invasive options, and posterior disease is weighted toward earlier and more definitive intervention. [4] [11]
For dysphagia, the ladder runs in parallel. Texture modification and thickening (altering food and fluid consistency to match what the swallow can safely handle), postural and feeding-strategy management, and swallowing therapy are the first tier, guided by the swallow study. When oral feeding is unsafe or nutrition cannot be maintained, enteral feeding is provided via a nasogastric tube in the short term and a gastrostomy for long-term need, with a jejunostomy considered when reflux and aspiration are severe despite gastric feeding. When aspiration is refractory to maximal medical and surgical management and the airway cannot otherwise be protected, total oesophagogastric dissociation — disconnecting the oesophagus from the stomach to eliminate reflux and oral intake into the stomach — is a last-resort airway-protection procedure reported in series of severely neurologically impaired children; it is a major undertaking offered only when all else has failed and the family has been fully counselled. [8] [7]
SALIVA
Specific Subtypes & Scenarios
Drooling in cerebral palsy and neurodisability is the archetype and demands the full multidisciplinary approach. Establish the pattern (anterior, posterior, or both) using severity, frequency and posterior scales; optimise posture, oral hygiene and nasal airway; begin speech-language therapy; and step up the ladder according to impact and airway risk. In severe (Gross Motor Function Classification System level IV to V) disease, posterior drooling and an unsafe swallow often coexist with reflux and chronic lung change, so saliva management, swallow assessment, reflux treatment and chest care are delivered together — the wet chin is treated, but the airway is the priority. [5] [7]
Mier 2000 — Arch Pediatr Adolesc Med (PMID 11115305)
Randomised, double-blind, dose-ranging study of oral glycopyrrolate versus placebo in children with developmental disabilities and chronic sialorrhoea
Key finding
Glycopyrrolate produced a clinically and statistically significant reduction in drooling weight compared with placebo, with benefit across the weight-based dose range; adverse effects were anticholinergic and dose-related, including behavioural changes and thickened secretions.
Practice change
Oral glycopyrrolate is an effective first-line pharmacological therapy for problematic drooling, weight-based and titrated, with monitoring for anticholinergic adverse effects.
Oropharyngeal dysphagia in the neurologically impaired child is managed by matching the diet to the swallow. A validated screening tool can flag feeding and swallowing difficulty (and undernutrition) in children with cerebral palsy, prompting formal assessment; the swallow study then defines the safe consistencies and the compensations (posture, bolus size, pace), and swallowing therapy is delivered. When safe oral intake cannot be maintained, enteral feeding is established — gastrostomy for long-term need, with jejunal feeding and anti-reflux measures when aspiration persists. The decision is shared with the family, balancing nutrition, chest health, the burden of feeding and the child's quality of life. [7] [8]
Eosinophilic oesophagitis is the diagnosis examiners most want named in an older child with progressive dysphagia or food impaction, particularly with a personal or family history of atopy. It is diagnosed on upper gastrointestinal endoscopy with biopsy showing oesophageal eosinophilia, and managed, per the ESPGHAN update, with proton pump inhibition, dietary exclusion (elemental or six-food elimination diets), and topical swallowed corticosteroid, with endoscopic dilation for strictures that cause persistent impaction. Recognising it matters because it is treatable, it is increasing in frequency, and it is a leading cause of food impaction in children and adolescents. [10]
Structural upper-aerodigestive anomalies sit at the crossroads of the airway and the food passage and present with feeding and breathing symptoms together. Laryngomalacia is the commonest cause of stridor in infants and is usually self-limiting, but severe disease with feeding difficulty and faltering growth needs airway evaluation and occasionally supraglottoplasty. Posterior laryngeal cleft causes aspiration, recurrent chest infections and choking and is diagnosed on airway endoscopy, with surgical repair guided by the depth of the cleft. Tracheo-oesophageal fistula, repaired in infancy, leaves a legacy of tracheomalacia, recurrent respiratory symptoms and feeding difficulty that may require long-term aerodigestive care; and vascular ring causes dysphagia with respiratory symptoms in the infant and is defined by imaging. These children are managed by the aerodigestive team — the general paediatrician coordinates rather than treats alone. [9] [10]
Complications & Pitfalls
The complications of drooling and dysphagia are the consequences of saliva and food going to the wrong place, or of the treatments that stop it. Aspiration is the central danger: overt aspiration causes choking, distress and acute respiratory events, while silent aspiration causes recurrent lower-respiratory infections, chronic lung damage (bronchiectasis), wheeze, oxygen dependence and faltering growth, and is the commonest reason a child with neurodisability deteriorates respiratorily. Malnutrition, dehydration and electrolyte disturbance follow when oral intake is insufficient, and skin excoriation and secondary infection follow chronic anterior drooling. [9] [8]
| Complication | Recognise it by | Key action |
|---|---|---|
| Silent aspiration | Recurrent chest infections, chronic lung change, wet voice, faltering growth | Instrumental swallow study; protect the airway; treat reflux |
| Anticholinergic adverse effects | Thickened secretions, constipation, urinary retention, irritability, hyperthermia | Reduce dose or switch; review swallow and chest; do not overlook worsening aspiration |
| Botulinum toxin complications | Thick tenacious secretions, worsening swallow, local infection, rare weakness | Specialist injection; review swallow; hydrate and clear secretions |
| Surgical complications | Infection, ranula, thick secretions, persistent drooling | Reserve for refractory disease; combined-approach surgery for posterior disease |
| Eosinophilic oesophagitis missed | Progressive dysphagia, food impaction, atopy | Endoscopy with biopsy; treat with diet, PPI or swallowed steroid |
The treatment-related complications are where the fellowship marks are. The anticholinergics (glycopyrrolate, atropine) reduce saliva but thicken the remaining secretions, which may paradoxically make the swallow and the airway clearance worse and precipitate chest deterioration in a child already prone to aspiration — the reason every child started on these drugs needs a baseline and repeat swallow and chest assessment. Botulinum toxin can similarly leave thick, tenacious secretions that are hard to clear, and surgery carries infection, ranula formation and the risk of an over-dry, uncomfortable mouth. The pitfall is to chase the visible drool into overtreatment of an asymptomatic child, or to undertreat the silent posterior drooling because the chin looks better. [1] [2]
The diagnostic pitfalls are equally important: missing silent aspiration because the child does not cough; treating drooling without addressing the swallow, reflux and chest; relying on a single swallow study when aspiration is intermittent; and forgetting to check the mouth, posture and medication list for a treatable contributor before reaching for a drug. Each is avoided by the same discipline: quantify with scales, assess the swallow and the chest, and step up the ladder with measurement rather than habit. [11] [5]
Prognosis & Disposition
The long-term outlook for drooling and dysphagia is the outlook of the underlying condition, and for children with static neurodisability it is a chronic disease managed over years rather than cured in an episode. Most children improve with the stepwise ladder, and many achieve a saliva pattern and a swallow that is safe, dignified and socially manageable, but the child with the most severe oromotor impairment, recurrent aspiration and chronic lung change has a guarded prognosis that is driven more by airway and chest health than by the visible drool. [5] [8]
Disposition is decided by airway safety, nutrition and the family's capacity, rather than by a fixed rule. A child with manageable anterior drooling and a safe swallow is managed in the community with the multidisciplinary team and serial review. A child with an unsafe swallow, recurrent aspiration or failure of maximal oral management is referred for instrumental assessment and, where needed, enteral feeding and airway-protection surgery, coordinated through an aerodigestive or neurodisability service. Admission is reserved for the acute aspiration event, the deteriorating chest, the need for feeding access, or the surgical intervention itself. [8] [7]
The decision to feed enterally — and, in rare cases, to proceed to oesophagogastric dissociation — is among the hardest in paediatrics and is explicitly shared with the family, balancing nutrition, chest health, the burden of prolonged oral feeding and the child's quality of life. Reported series of total oesophagogastric dissociation in severely neurologically impaired children describe it as a last-resort airway-protection procedure for refractory aspiration unresponsive to maximal medical therapy and feeding gastrostomy, and it is undertaken only after full counselling and multidisciplinary agreement. The general paediatrician's role is to hold the whole picture, coordinate the team, and make sure the airway, the nutrition and the family are all heard. [8] [9]
Special Populations
Infants and young children with drooling and dysphagia are approached with particular caution because the swallow matures with development, and what is abnormal at six months may be age-appropriate. Persistent drooling beyond two to three years, or any feeding difficulty with respiratory compromise, prompts assessment rather than watchful waiting; structural causes (laryngomalacia, laryngeal cleft, tracheo-oesophageal fistula, vascular ring) present in infancy and are sought actively when an infant chokes, aspirates or fails to thrive on feeds. [9] [10]
Children with severe cerebral palsy (Gross Motor Function Classification System level IV to V) carry the greatest burden and need the most coordinated care. Oromotor impairment, poor head and trunk control, reflux, constipation, recurrent chest infections and undernutrition cluster together, and a single intervention rarely suffices; the management combines saliva control, swallow assessment and texture modification, reflux treatment, chest physiotherapy and immunisation, nutritional support (often enteral), and attention to posture, skin, bowel and comfort. The goal is a safe swallow, a clear chest, adequate nutrition and a good quality of life, delivered by a team around the family. [5] [7]
Children with repaired oesophageal atresia and tracheo-oesophageal fistula have a lifelong aerodigestive legacy — tracheomalacia, recurrent respiratory symptoms, anastomotic stricture, gastro-oesophageal reflux and feeding difficulty — that needs long-term aerodigestive surveillance. Dysphagia in this group may reflect stricture, reflux oesophagitis or eosinophilic oesophagitis (more common in these children), and is evaluated with endoscopy and contrast study as indicated. [10]
Children with life-limiting neurodisability and their families face decisions in which feeding is bound up with love, hope and dignity, and the role of the paediatrician is to support a family-centred, culturally sensitive plan that balances nutrition, comfort and the burden of intervention. The aim is not to impose a single pathway but to share the evidence, respect the family's goals, and protect the airway and comfort of the child — recognising that in advanced disease the priorities may shift toward symptom control and quality of life. [8] [5]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | Stance | First-line pharmacological |
|---|---|---|---|
| ANZ | RCH Melbourne, state neurodisability services | Stepwise multidisciplinary ladder; airway and chest health first | Glycopyrrolate (glycopyrronium) oral |
| UK | NICE NG62 (cerebral palsy) | Assess drooling and feeding; intervene for impact and airway risk | Glycopyrronium or hyoscine; specialist referral for refractory |
| North America | AACPDM care pathway | Stepwise algorithm with measurement; botulinum toxin and surgery for refractory | Glycopyrrolate oral solution (where licensed) |
| Europe | Italian Delphi consensus | Consensus stepwise pathway emphasising posterior drooling and aspiration | Glycopyrrolate first-line; atropine and BTX as alternatives |
The evidence backbone you should be able to name begins with the double-blind dose-ranging study of glycopyrrolate by Mier and colleagues (2000), which established the anticholinergic as effective and weight-based, and a recent randomised trial of an oral glycopyrronium solution (Fayoux and colleagues, 2024) that confirmed significant benefit in children and adolescents with severe sialorrhoea and neurodisability. The network meta-analysis of pharmacological treatments for sialorrhoea (Sridharan and Sivaramakrishnan, 2018) compares the anticholinergics and other agents relative to placebo and informs the choice of drug. [1] [3] [12]
For chemodenervation and surgery, the randomised trial of botulinum toxin into the salivary glands (Reid and colleagues, 2008) showed short-term reduction in drooling in children with neurological disorders, and a randomised trial comparing surgery with botulinum toxin (Bekkers and colleagues, 2021) found surgery more durable for reducing drooling and improving daily life. A systematic review with a stepwise evidence-based clinical algorithm (Almohanna and colleagues, 2026) integrates these into a practical management pathway, and the Italian Delphi consensus (Riva and colleagues, 2022) emphasises the priority of posterior drooling and aspiration. The ESPGHAN update on eosinophilic oesophagitis in children (2024) anchors the oesophageal-dysphagia pathway, and the long-term series of total oesophagogastric dissociation (Battaglia and colleagues, 2020) defines the last-resort airway-protection option. [2] [4] [11] [10] [8]
The live areas of nuance are the exact first-line anticholinergic and its formulation, the threshold and timing for botulinum toxin versus surgery, how aggressively to investigate the swallow in a child who does not clinically aspirate, and the role of oesophagogastric dissociation — all areas where reasonable guidelines differ and where a fellowship candidate shows depth by naming the guideline and the trade-off rather than reciting a single regimen. [11] [5]
Exam Pearls
The single move that keeps these children safe is the disciplined one: separate anterior from posterior drooling, assess the swallow (clinically and, when in doubt, instrumentally), and step up the ladder with measurement — therapy and posture, then anticholinergic, then botulinum toxin, then surgery — while treating the chest, the nutrition and the family together, and reserving the most irreversible interventions for the airway that cannot otherwise be protected. [11] [8]
And when you teach drooling and dysphagia, teach them as one system — mouth, throat, airway, food pipe — united by the question of whether a child can move saliva and food safely to the stomach without soiling the lung — so that the next generation of paediatricians treats the wet lung as readily as the wet chin, and never lets the visible problem hide the dangerous one. [9] [5]
References
- [1]Mier RJ, et al. Treatment of sialorrhea with glycopyrrolate: A double-blind, dose-ranging study. Arch Pediatr Adolesc Med, 2000.PMID 11115305
- [2]Reid SM, et al. Randomized trial of botulinum toxin injections into the salivary glands to reduce drooling in children with neurological disorders. Dev Med Child Neurol, 2008.PMID 18201301
- [3]Fayoux P, et al. Glycopyrronium 320 micrograms/mL in children and adolescents with severe sialorrhoea and neurodisabilities: A randomized, double-blind, placebo-controlled trial. Dev Med Child Neurol, 2024.PMID 38214675
- [4]Bekkers S, et al. Surgery versus botulinum neurotoxin A to reduce drooling and improve daily life for children with neurodevelopmental disabilities: a randomized controlled trial. Dev Med Child Neurol, 2021.PMID 33997959
- [5]Riva A, et al. Impact and management of drooling in children with neurological disorders: an Italian Delphi consensus. Ital J Pediatr, 2022.PMID 35854335
- [6]Koeken DCRM, et al. Validity, Reliability and Application of the Paediatric Posterior Drooling Scale. Child Care Health Dev, 2025.PMID 41236173
- [7]Bell KL, et al. Development and validation of a screening tool for feeding/swallowing difficulties and undernutrition in children with cerebral palsy. Dev Med Child Neurol, 2019.PMID 30937885
- [8]Battaglia S, et al. Total Oesophagogastric Dissociation in Neurologically Impaired Children: 18 Years' Experience and Long-term Follow-up. J Pediatr Gastroenterol Nutr, 2020.PMID 31913925
- [9]Morton RE, Wheatley R, Minford J Respiratory tract infections due to direct and reflux aspiration in children with severe neurodisability. Dev Med Child Neurol, 1999.PMID 10378759
- [10]Amil-Dias J, et al. Diagnosis and management of eosinophilic esophagitis in children: An update from the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr, 2024.PMID 38923067
- [11]Almohanna S, et al. Management of pediatric sialorrhea: A systematic review with a stepwise evidence-based clinical algorithm. Int J Pediatr Otorhinolaryngol, 2026.PMID 42242174
- [12]Sridharan K, Sivaramakrishnan G Pharmacological interventions for treating sialorrhea associated with neurological disorders: A mixed treatment network meta-analysis of randomized controlled trials. J Clin Neurosci, 2018.PMID 29475576