Paeds · ent-hearing-and-oral-health
Pharyngitis, tonsillitis, peritonsillar abscess and deep neck infection
Also known as Sore throat · Group A streptococcal pharyngitis · Quinsy · Retropharyngeal abscess
Fellowship guide to paediatric sore throat progressing from viral pharyngitis through group A streptococcal tonsillitis to peritonsillar abscess and deep neck infection: the Centor and McIsaac clinical scoring systems and the principle that children need microbiological confirmation before antibiotics because clinical features alone cannot reliably separate bacterial from viral disease; first-line phenoxymethylpenicillin or amoxicillin for ten days; the drooling, trismus and toxic-child red flags that mark peritonsillar abscess, retropharyngeal abscess and parapharyngeal spread; contrast-enhanced CT of the neck; needle aspiration versus incision and drainage for quinsy; intravenous antibiotics and surgical drainage for deep neck space collections; acute rheumatic fever primary prevention; and the ANZ, UK and North American guideline approaches.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
Overview & Definition
Picture the six-year-old who comes in with a sore throat, a fever, and tonsils coated in white exudate. The parent expects an antibiotic. The fellowship task is to resist reflex treatment, because most sore throats in children are viral — and the one bacterial cause that matters, group A streptococcus, needs to be confirmed by a test, not guessed from the appearance of the throat. This single discipline — score, swab, then treat — is the hinge on which the entire topic turns. [1] [3]
Acute pharyngitis is inflammation of the pharynx, and acute tonsillitis is inflammation of the palatine tonsils; in practice the two overlap and are often described together as acute pharyngotonsillitis. The great majority of cases are viral, caused by rhinovirus, coronavirus, adenovirus, coxsackievirus, Epstein-Barr virus and many others. Group A beta-haemolytic streptococcus (Streptococcus pyogenes) is the single most important bacterial pathogen, accounting for roughly twenty to thirty per cent of sore throats in children over three years, and is the only common cause for which antibiotic treatment is recommended — both to shorten symptoms and to prevent acute rheumatic fever. [1] [6]
What makes this a fellowship topic rather than a routine prescription is that sore throat sits on a continuum with serious deep space infections. A simple tonsillitis can progress to a peritonsillar abscess (quinsy), infection can track into the retropharyngeal or parapharyngeal spaces to form a deep neck abscess, and the same organisms — GAS, mixed oral flora, Fusobacterium necrophorum — can produce Lemierre syndrome (septic jugular thrombophlebitis) or descend into the mediastinum. Recognising where on this spectrum a child sits — routine, urgent, or emergency — is the clinical skill that earns marks and saves lives. [9] [10]
Classification
Classify paediatric sore throat by depth of infection and severity, because this determines whether the child needs analgesia alone, an antibiotic, or an emergency pathway. Keeping the layers separate prevents the two great errors: treating every sore throat with antibiotics, and missing the child whose infection has already spread beyond the tonsil. [1] [10]
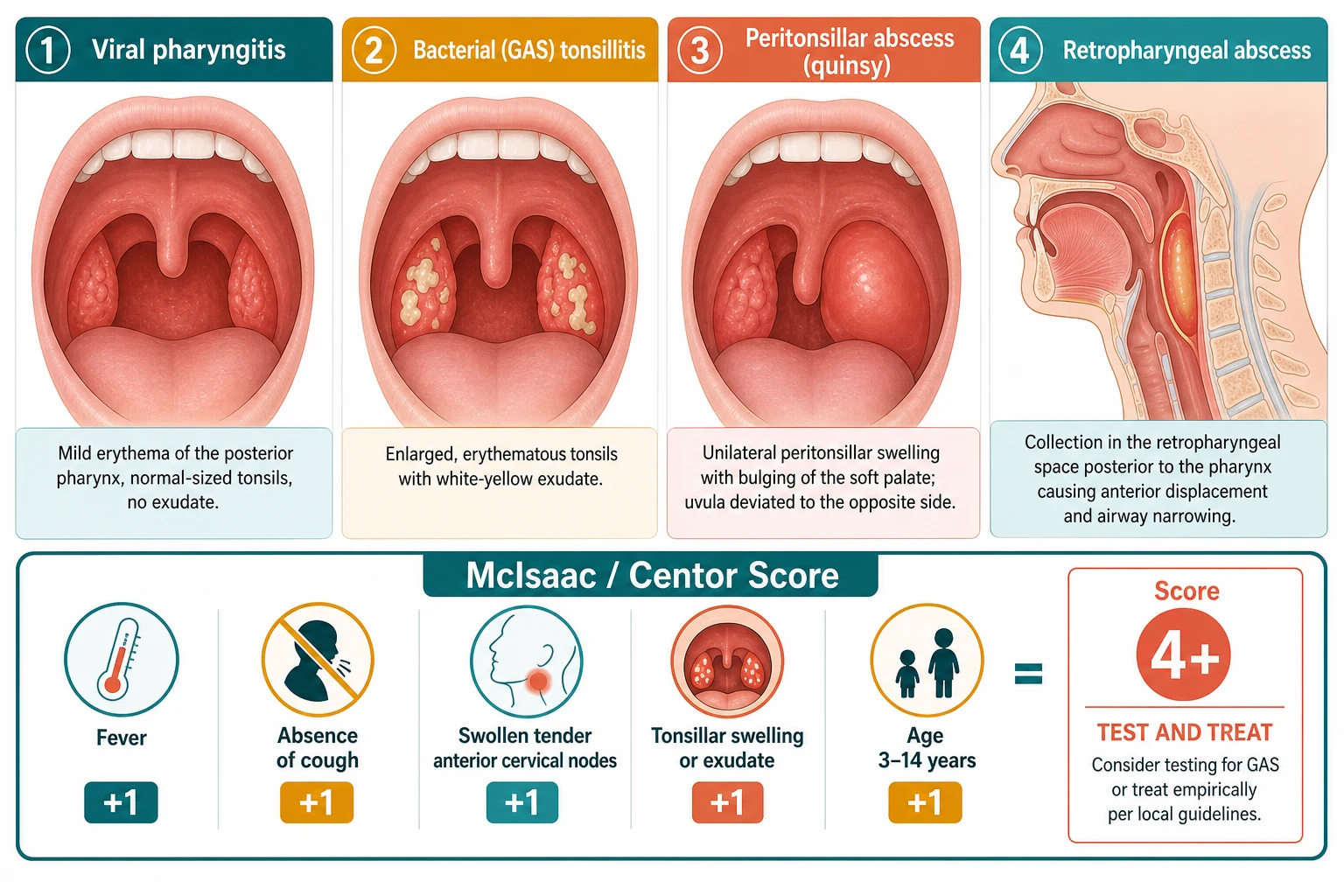
By depth, the spectrum has four layers. Acute viral pharyngitis is a superficial mucosal inflammation with cough, rhinorrhoea and no exudate — the most common form, needing no antibiotic. Acute bacterial (GAS) tonsillitis shows fever, tender cervical adenopathy, tonsillar exudate and absence of cough — the treatable form. Peritonsillar abscess (quinsy) is a collection of pus between the tonsil capsule and the superior constrictor muscle, producing asymmetrical tonsillar swelling, uvular deviation and trismus. Deep neck space infection — retropharyngeal, parapharyngeal or danger-space abscess — sits beyond the deep cervical fascia and threatens the airway and mediastinum. [10] [1]
By clinical scoring, the McIsaac score (a modification of the Centor score that adds an age component) stratifies the probability of GAS and drives the testing decision. The five components — fever above 38 degrees Celsius, absence of cough, tender anterior cervical lymphadenopathy, tonsillar swelling or exudate, and age three to fourteen years — each score one point. A score of zero or one means GAS is unlikely and neither testing nor treatment is recommended; a score of two or three warrants a throat swab or rapid antigen test, with treatment only if positive; and a score of four or five carries a high enough pre-test probability to test and, if positive, treat. [3] [4]
The numbers that anchor your viva
A critical caveat: the IDSA explicitly recommends against treating GAS pharyngitis empirically on clinical grounds alone in children and adolescents. Clinical features overlap too heavily with viral causes, and empirical antibiotics drive resistance and miss the diagnosis in some while over-treating many. Every child with suspected GAS should have a throat swab or rapid antigen test before an antibiotic is prescribed — the score selects who to test, not who to treat blind. [1] [2]
Epidemiology & Risk Factors
Sore throat is one of the commonest reasons children present to primary care, and GAS pharyngitis is the most frequent bacterial cause. The peak incidence of GAS pharyngitis is between five and fifteen years of age; it is uncommon under three years, where viral causes dominate and the presentation of GAS is atypical — more often rhinitis, fever and irritability than the classic exudative tonsillitis of the school-age child. The condition clusters in winter and early spring and spreads readily in schools and day-care through respiratory droplets. [1] [5]
The risk factors divide into those that increase exposure and those that increase the consequence of infection. School attendance and household crowding increase droplet transmission; immune naivety in young children means successive exposures to new serotypes; and close contact with a symptomatic person is the strongest behavioural risk. These exposure factors explain the seasonality and the age distribution, and they are why outbreaks occur in classrooms and dormitories. [1] [6]
The factors that increase the consequence of GAS infection are where the fellowship-level thinking lives. In many Aboriginal and Torres Strait Islander communities, and in other populations with high rates of rheumatic heart disease, a streptococcal sore throat carries a far higher risk of triggering acute rheumatic fever — the rationale for a lower threshold to test and treat in these communities. Household crowding, poverty, poor access to primary care and remote living all increase the risk that a streptococcal throat infection will progress to rheumatic heart disease, making sore throat management an equity issue, not just an antibiotic-stewardship one. [7] [8]
The microbiology of deep neck infections differs from simple pharyngitis. While GAS dominates uncomplicated tonsillitis, peritonsillar and deep neck abscesses are polymicrobial, involving a mix of oral aerobes (viridans streptococci, Streptococcus anginosus group, Staphylococcus aureus) and anaerobes (Fusobacterium, Prevotella, Peptostreptococcus). Fusobacterium necrophorum deserves special mention as the cause of Lemierre syndrome — a septic jugular thrombophlebitis with metastatic abscesses, classically in previously healthy adolescents after a sore throat — and as a cause of peritonsillar abscess in young adults and older children. [9] [10]
Pathophysiology
The teaching model runs from the throat surface to the deep fascia, and it hinges on understanding the fascial planes of the neck — the anatomy that determines how far infection can spread. [10] [1]
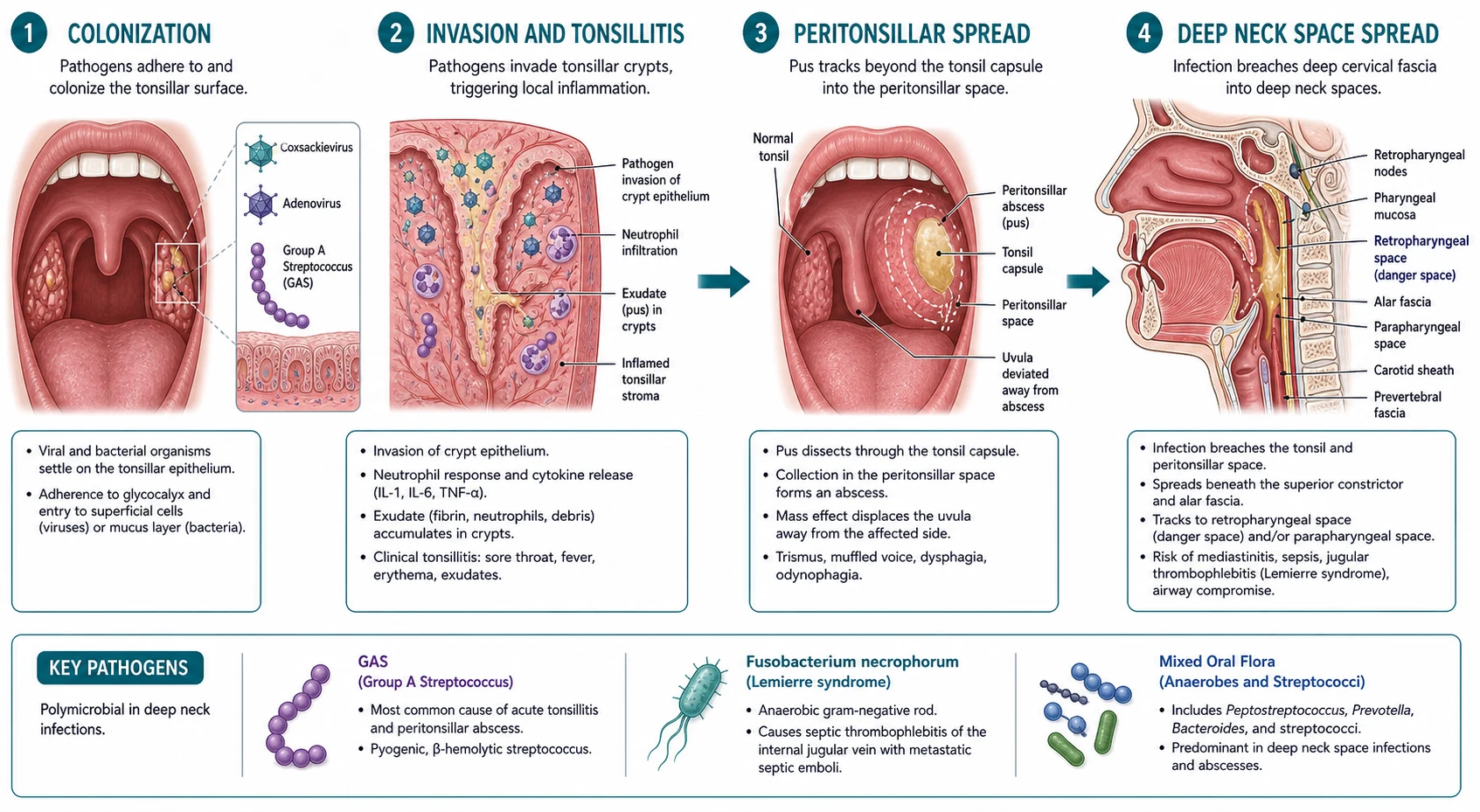
The chain begins with colonisation of the pharyngeal and tonsillar mucosa by respiratory viruses or GAS. Viral pharyngitis produces mucosal oedema, hyperaemia and lymphoid hyperplasia — the red, inflamed but exudate-free throat of a cold. GAS pharyngitis follows a different path: the organism adheres to the pharyngeal epithelium, invades the tonsillar crypts, and releases a cocktail of virulence factors including M protein (which inhibits complement activation and phagocytosis), streptolysins (which lyse red and white blood cells) and pyrogenic exotoxins (which produce the rash of scarlet fever). The host response — neutrophil infiltration, fibrin deposition and pus formation — produces the characteristic white-yellow tonsillar exudate and the tender enlarged anterior cervical nodes. [1] [9]
When infection is not contained by the local immune response, it can extend beyond the tonsil capsule into the peritonsillar space — the loose connective tissue between the palatine tonsil capsule and the superior pharyngeal constrictor muscle. Pus collecting here forms a peritonsillar abscess, which pushes the tonsil medially and forwards, displaces the uvula to the contralateral side, and produces the trismus (from irritation of the pterygoid muscles) and the muffled hot-potato voice that are its hallmarks. [10]
The deeper spaces are reached when infection penetrates the deep cervical fascia. The retropharyngeal space — between the buccopharyngeal fascia (covering the pharynx) and the alar fascia (in front of the vertebral column) — contains lymph nodes that drain the nasopharynx, oropharynx and sinuses; these nodes are prominent in young children and atrophy after about age four to six, which is why retropharyngeal abscess peaks in the two-to-four-year age group. Infection in these nodes suppurates and forms a collection that can push the pharynx forwards and narrow the airway. The parapharyngeal space lies lateral to the pharynx and connects to the retropharyngeal space, allowing infection to track between them and towards the mediastinum through the danger space — the potential space between the alar and prevertebral fascia that extends from the skull base to the diaphragm, providing a direct route for descending necrotising mediastinitis. [10] [11]
A specific pathophysiological pathway worth knowing is Lemierre syndrome. Fusobacterium necrophorum, an anaerobe of the oropharynx, invades the lateral pharyngeal wall, causes septic thrombophlebitis of the internal jugular vein, and releases septic emboli that seed the lungs, producing multifocal abscesses and septic arthritis. It presents in a previously healthy adolescent with a sore throat that does not resolve, followed by high fever, neck pain, and pulmonary symptoms days later — and it is the reason that a worsening sore throat in an older child or adolescent should never be dismissed. [9]
Clinical Presentation
The classic GAS pharyngitis story is a school-age child with the abrupt onset of sore throat, fever (typically 38 degrees Celsius or higher), headache and abdominal pain, without cough, rhinorrhoea or other viral features. On examination the tonsils are enlarged and coated with white-yellow exudate, there are tender enlarged anterior cervical lymph nodes, and the breath may be foul. The presence of viral features — cough, rhinorrhoea, hoarseness, oral ulcers, diarrhoea — strongly favours a viral cause and argues against GAS. [1] [5]
| Picture | Bedside findings | Immediate response |
|---|---|---|
| Viral pharyngitis | Cough, rhinorrhoea, mild fever, no exudate, viral features present | Analgesia, fluids, no antibiotic, no swab; safety-net |
| Suspected GAS tonsillitis | Fever, exudate, tender anterior nodes, no cough; McIsaac 2 or more | Throat swab or rapid antigen test; treat with penicillin if positive |
| Scarlet fever | Above plus fine sandpaper rash, strawberry tongue, pastia lines | Same as GAS; the rash confirms GAS toxin production |
| Peritonsillar abscess | Trismus, muffled voice, uvula deviated, asymmetric tonsillar bulge | Urgent ENT; needle aspiration or drainage; IV or oral antibiotics |
| Retropharyngeal or deep neck abscess | Toxic, neck stiffness or torticollis, drooling, refusal to move neck | Emergency: airway, IV antibiotics, contrast CT neck, ENT and surgery |
The suppurative complications announce themselves through a distinct set of signs that change the pathway. A peritonsillar abscess presents with worsening sore throat, often unilateral, with trismus (difficulty opening the mouth), a muffled or hot-potato voice, drooling from inability to swallow saliva, and referred ear pain. On examination one tonsil is pushed medially and forwards, the uvula is displaced to the opposite side, and the soft palate is swollen and red on the affected side. The child may hold the neck stiff and prefer a semi-recumbent position. [10]
A retropharyngeal abscess in a toddler presents with fever, neck pain or stiffness, refusal to move the neck, torticollis, dysphagia, and drooling. The child may hold the neck hyperextended and resist flexion — a sign easily mistaken for meningism. On inspection of the oropharynx there may be a bulge on the posterior pharyngeal wall, though this is often hard to see in a struggling child. Stridor, respiratory distress and a toxic appearance indicate airway compromise and demand immediate airway management before anything else. [11] [10]
A trap to avoid is the child whose sore throat is not improving after three to five days of appropriate treatment. GAS pharyngitis should improve within forty-eight hours of starting penicillin; a worsening course, new neck swelling or persistent high fever raises the question of a peritonsillar or deep neck collection, infectious mononucleosis (where amoxicillin produces a characteristic rash), or Lemierre syndrome. Persistence is a signal to reassess and image, not to repeat the same prescription. [9] [10]
Differential Diagnosis
Sort the differential into three groups: the other causes of sore throat, the suppurative complications, and the non-infectious mimics. The aim is to confirm or exclude GAS with a score and a swab while maintaining a low threshold to look deeper when the picture does not fit. [1] [10]
Viral pharyngitis
the majority
- Cough, rhinorrhoea, hoarseness, oral ulcers
- No exudate or mild erythema only
- Adenovirus, rhinovirus, coxsackie, RSV
- Analgesia, no antibiotic, no swab
GAS tonsillitis
- Sudden onset, fever, exudate, no cough
- Tender anterior cervical nodes
- McIsaac score 2-plus; confirm with swab or RADT
- Penicillin V or amoxicillin for 10 days
Infectious mononucleosis (EBV)
- Adolescent, prolonged fever, fatigue
- Marked tonsillar exudate, posterior cervical nodes
- Hepatosplenomegaly; amoxicillin causes rash
- Symptomatic; avoid contact sports if splenomegaly
Peritonsillar abscess
- Trismus, uvular deviation, unilateral bulge
- Hot-potato voice, drooling
- Needle aspiration or incision and drainage
- Antibiotics covering oral anaerobes
Retropharyngeal abscess
- Toddler, neck stiffness, torticollis, drooling
- Toxic, refuses to move neck
- Contrast CT neck; IV antibiotics
- Surgical drainage if large or not responding
Infectious mononucleosis (Epstein-Barr virus) is the most important mimic of GAS in the adolescent. It produces fever, marked tonsillar exudate (often more impressive than GAS), generalised lymphadenopathy with prominent posterior cervical nodes, fatigue and hepatosplenomegaly. The clue is the duration (symptoms last one to two weeks rather than three to five days), the profound fatigue, and the development of a maculopapular rash if amoxicillin is given — a well-known and frequently tested reaction. A Monospot or EBV serology confirms it, and management is supportive, with avoidance of contact sports while splenomegaly is present because of the risk of splenic rupture. [1] [5]
Coxsackievirus causes herpangina (small vesicles and ulcers on the soft palate and tonsillar pillars) and hand-foot-and-mouth disease (oral ulcers with palmar and plantar vesicles). Adenovirus causes pharyngoconjunctival fever (sore throat with conjunctivitis). These viral causes are distinguished by their specific features and need no antibiotic. Among non-infectious causes, aphthous stomatitis causes painful oral ulcers without systemic features, and in rare cases, leukaemia or agranulocytosis presents with necrotic tonsillar ulcers and systemic symptoms — a differential to keep in mind when the sore throat is unusually severe or accompanied by cytopenias. [1] [6]
Clinical & Bedside Assessment
Assessment of a sore throat starts with a focused history that applies the McIsaac score mentally before you even look in the mouth. Ask about the onset (abrupt favours GAS, gradual favours viral), the associated symptoms (cough and rhinorrhoea favour viral; headache, abdominal pain and vomiting favour GAS), the fever pattern, and any contact with a known GAS case. In high-risk communities, ask specifically about a personal or family history of acute rheumatic fever or rheumatic heart disease, because this lowers the threshold to test and treat. [3] [7]
Examination of the oropharynx should be done carefully and gently, especially in any child with signs that might suggest a deep space infection — forcing a throat examination in a child with a retropharyngeal abscess can precipitate abscess rupture and airway obstruction. In the cooperative child, inspect the tonsils for size, symmetry and exudate, look for uvular deviation (peritonsillar abscess), check for a posterior pharyngeal wall bulge (retropharyngeal abscess), and palpate the neck for lymphadenopathy, swelling, warmth or tenderness. [10] [1]
The key examination skill that distinguishes a peritonsillar from a retropharyngeal collection is the neck examination. In peritonsillar abscess, trismus and unilateral tonsillar findings dominate. In retropharyngeal abscess, the child holds the neck stiff or extended, resists flexion, may have torticollis, and there may be visible swelling or fullness in the neck. A child who will not move their neck, or who holds it hyperextended, should be treated as having a deep neck infection until imaging proves otherwise. [11] [10]
Deliberately avoid the common errors: diagnosing GAS from the throat appearance alone without a score or swab; missing a peritonsillar abscess by not looking for uvular deviation and trismus; attributing neck stiffness to meningitis when the pharynx is the source; and failing to examine the neck in a child with a sore throat and fever. The neck is part of the throat examination, every time. [1] [10]
Investigations
The primary investigation for suspected GAS pharyngitis is the throat swab for culture or a rapid antigen detection test (RADT). Both have high specificity (a positive test reliably indicates GAS), but sensitivity varies — culture is the gold standard at over ninety per cent, while RADT sensitivity is typically seventy to ninety per cent. In children, the IDSA recommends a back-up throat culture if the RADT is negative, because a false negative risks missing a treatable GAS infection and its rheumatic-fever-prevention role. [1] [2]
In a typical case of suspected GAS pharyngitis, no other investigations are needed — the score plus the swab or RADT is sufficient. Blood tests (full blood count, CRP) do not reliably distinguish GAS from viral pharyngitis and add no useful information in the routine case. The same applies to viral panels: identifying the specific virus does not change management in an uncomplicated sore throat. [1] [6]
| Test | When to use it | What it tells you |
|---|---|---|
| Throat swab (culture) | Suspected GAS; score 2 or more; negative RADT back-up | Gold standard; specificity high; results in 24 to 48 hours |
| Rapid antigen test (RADT) | Suspected GAS; score 2 or more in clinic | Specificity high; sensitivity 70 to 90 per cent; negative needs culture back-up in children |
| Contrast CT of the neck | Suspected deep neck or peritonsillar abscess | Defines the collection, its size and the space involved; guides drainage |
| Ultrasound of the neck | Selected cases; some centres for superficial collections | Can identify a peritonsillar collection; operator and child dependent |
| Blood cultures | Toxic child; suspected Lemierre or mediastinitis | Identifies bacteraemia and the organism; take before antibiotics if possible |
When a deep neck infection is suspected, the investigation of choice is contrast-enhanced computed tomography (CT) of the neck. CT defines the abscess, its size, the deep space involved (retropharyngeal, parapharyngeal, danger space), and the extent of any airway compromise or mediastinal extension. A collection measuring more than two centimetres in diameter, or one that fails to respond to intravenous antibiotics, generally warrants surgical drainage. Blood cultures should be taken in the toxic or septic child, particularly when Lemierre syndrome is suspected — blood cultures growing Fusobacterium necrophorum confirm the diagnosis. [10] [11]
Management — Resuscitation
For the child with a deep neck infection, the priority shifts from the routine pharyngitis pathway to airway protection, sepsis management and surgical planning. The first step is to assess and secure the airway: a child with stridor, drooling or respiratory distress needs to be managed in a position of comfort (usually sitting upright and leaning forward), kept calm, and assessed by an anaesthetist and ENT surgeon. Do not force the child to lie flat and do not instrument the oropharynx without airway expertise at the bedside, because either can precipitate catastrophic abscess rupture or airway obstruction. [10] [11]
Obtain intravenous access, take blood cultures and inflammatory markers, and start broad-spectrum intravenous antibiotics covering GAS, oral anaerobes and Staphylococcus aureus — for example, a combination of ceftriaxone and metronidazole, or clindamycin, or ampicillin-sulbactam, adjusted to local resistance patterns and guidelines. Arrange urgent contrast CT of the neck once the child is stabilised, and involve ENT and, if mediastinal extension is suspected, cardiothoracic or general surgery. [10] [11]
For Lemierre syndrome, the combination of high fever, neck pain, pulmonary infiltrates and a history of recent sore throat in an older child or adolescent demands blood cultures, a neck ultrasound or CT looking for internal jugular vein thrombosis, and a chest imaging to identify septic emboli. Treatment is prolonged intravenous antibiotics active against Fusobacterium necrophorum — typically a beta-lactam with beta-lactamase inhibitor cover (such as piperacillin-tazobactam or amoxicillin-clavulanate) or clindamycin plus metronidazole — for four to six weeks, with anticoagulation considered on a case-by-case basis. [9]
For the much larger group of well children with uncomplicated pharyngitis, "resuscitation" simply means analgesia — paracetamol and ibuprofen, weight-based and regular, and encouragement of oral fluids. This is the step most under-appreciated by families who expect an antibiotic, and good pain relief often resolves the concern entirely. [6]
Management — Definitive & Stepwise
The definitive management of pharyngitis is built in three layers: score-based testing, targeted antibiotic therapy for confirmed GAS, and a clear reassessment and safety-net. For the suppurative complications, the layers are drainage, intravenous antibiotics and airway protection. [1] [6]
Grading the severity to drive the pathway
Emergency
Deep neck abscess or Lemierre; airway risk; IV antibiotics, CT, surgical drainage
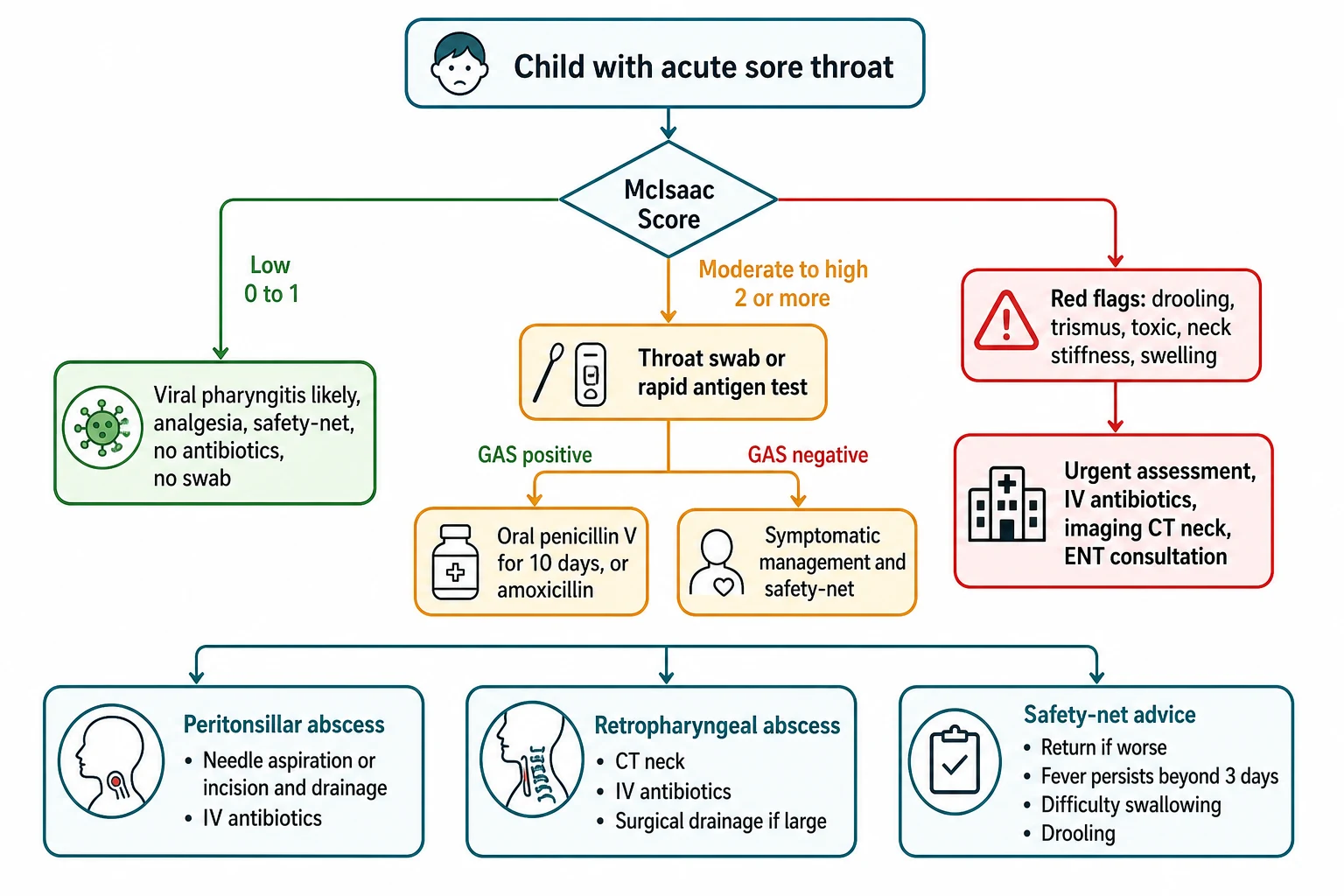
Step one — score and test. Apply the McIsaac score. A score of zero or one needs no testing and no antibiotics. A score of two or more warrants a throat swab or rapid antigen test; treat only if GAS is confirmed. In high-risk communities (Aboriginal and Torres Strait Islander children in remote settings, or those with a history of rheumatic fever), the threshold to test and treat is lower because the goal includes rheumatic fever prevention. [1] [7]
Step two — treat confirmed GAS. For confirmed GAS pharyngitis, first-line therapy is phenoxymethylpenicillin (penicillin V) orally for ten days. The standard ANZ dosing is: child under 10 kg, 250 mg orally twice daily for ten days; child 10 kg or more, 500 mg orally twice daily for ten days. An equivalent alternative is amoxicillin 50 mg/kg (maximum 1 g) orally once daily for ten days, which is preferred by many for its once-daily convenience and palatable suspension. For a child with genuine penicillin allergy (non-anaphylactic), cephalexin is a reasonable option; for anaphylactic penicillin allergy, clindamycin or a macrolide such as azithromycin or roxithromycin is used. No GAS strain has ever demonstrated penicillin resistance, which is why penicillin remains first-line after decades. [1] [7]
Drugs in paediatric pharyngitis and tonsillitis
Step three — manage the suppurative complications. For a peritonsillar abscess, the definitive treatment is drainage — either needle aspiration or incision and drainage — performed by a clinician experienced in the technique, combined with antibiotics covering GAS and oral anaerobes (amoxicillin-clavulanate, or penicillin plus metronidazole). Many children can be managed as outpatients after successful drainage, but admission is warranted for airway concern, dehydration, immunocompromise, or failure of initial management. [10]
For retropharyngeal and deep neck abscesses, management combines intravenous antibiotics (ceftriaxone plus metronidazole, or clindamycin, or ampicillin-sulbactam) with surgical drainage when the collection is large (typically more than two centimetres on CT), when there is airway compromise, or when the child fails to improve on antibiotics alone. Small retropharyngeal abscesses in a stable child may be managed with IV antibiotics alone and close observation, with surgery reserved for non-response or enlargement. [10] [11]
The stepwise pathway
Apply the McIsaac score to every child with acute sore throat; look for viral features and red flags.
Score 0 to 1 — no testing, no antibiotic, analgesia and safety-net. Score 2 or more — throat swab or RADT.
Treat confirmed GAS with phenoxymethylpenicillin (or amoxicillin) for ten days; give analgesia to all.
Recognise the red flags of suppurative complications: drooling, trismus, muffled voice, neck stiffness, toxic appearance.
For peritonsillar abscess — drainage (needle or incision) plus antibiotics covering anaerobes.
For deep neck abscess — airway first, IV antibiotics, contrast CT neck, and surgical drainage if large or failing medical therapy.
Step four — safety-net and reassessment. Every family goes home with a concrete plan: return early if the sore throat or fever is not improving after forty-eight hours, if new symptoms develop (neck swelling, difficulty swallowing, drooling), or if they are simply worried. For confirmed GAS, a planned review at forty-eight to seventy-two hours confirms response; failure to improve after this period warrants reassessment for a complication, an alternative diagnosis (EBV, abscess), or antibiotic non-adherence. [1] [6]
SCORE
Specific Subtypes & Scenarios
Recurrent GAS pharyngitis is defined as seven or more documented episodes in one year, five or more per year for two consecutive years, or three or more per year for three consecutive years. The approach is to confirm each episode with a swab, address carriage versus true infection (a chronic GAS carrier with repeated viral sore throats is often mislabelled as recurrent GAS), consider tonsillectomy in selected cases meeting Paradise criteria, and ensure the family understands the safety-net. Tonsillectomy reduces the frequency of sore throats but carries its own morbidity, and the decision is shared with the family after balanced counselling. [1] [6]
Scarlet fever is GAS pharyngitis complicated by a toxin-mediated rash, caused by streptococcal pyrogenic exotoxins (usually SpeA or SpeC). The rash is a fine, sandpaper-textured erythema that starts on the trunk and spreads, accentuates in flexural creases (Pastia's lines), and is accompanied by a strawberry tongue (white coating that desquamates to reveal a red, papillae-covered surface). It is treated identically to GAS pharyngitis, and the rash confirms rather than changes the management. The rash desquamates after one to two weeks. [1] [8]
Spinks, Glasziou, Del Mar 2013 — Cochrane (PMID 24190439)
Systematic review of randomised trials of antibiotics versus placebo for sore throat
Key finding
Antibiotics reduced symptom duration by about 16 hours overall and reduced the incidence of complications (otitis media, sinusitis, quinsy). The greatest benefit was in GAS-positive sore throat and in populations at high risk of complications. Antibiotics increased rash, diarrhoea and abdominal symptoms.
Practice change
The symptom benefit is modest, but the prevention of suppurative complications (including peritonsillar abscess) and rheumatic fever justifies targeted antibiotic use in confirmed GAS pharyngitis — the foundation of selective, test-then-treat prescribing.
Infectious mononucleosis presents a specific pitfall: if amoxicillin is given empirically to a child or adolescent who turns out to have EBV, a widespread maculopapular rash develops in over ninety per cent of cases. This is not a true penicillin allergy, but it is dramatic and distressing, and it is one of the reasons the IDSA mandates microbiological confirmation before antibiotics — prescribing amoxicillin for an untested sore throat risks this reaction and the mislabelling of the child as penicillin-allergic for life. [1] [5]
Lemierre syndrome deserves specific recognition because it is easily missed. A previously well adolescent presents with a sore throat that does not resolve, followed days later by high spiking fevers, neck pain (from internal jugular thrombophlebitis) and pulmonary symptoms (septic emboli — pleuritic chest pain, productive cough, haemoptysis). Blood cultures grow Fusobacterium necrophorum, and neck imaging shows the jugular thrombus. Treatment is prolonged intravenous antibiotics for four to six weeks, and anticoagulation is individualised. [9]
Complications & Pitfalls
The complications of GAS pharyngitis divide into suppurative and non-suppurative. The non-suppurative complications are the reason antibiotics are given at all: acute rheumatic fever (occurring two to three weeks after untreated GAS pharyngitis, prevented by ten days of penicillin) and post-streptococcal glomerulonephritis (occurring one to two weeks after GAS pharyngitis or skin infection, not prevented by antibiotics but generally self-limiting). [7] [8]
| Complication | Recognise it by | Key action |
|---|---|---|
| Acute rheumatic fever | Migratory polyarthritis, carditis, chorea, 2 to 3 weeks after GAS | Prevented by 10 days of penicillin; treat ARF with anti-inflammatories and secondary prophylaxis |
| Post-streptococcal glomerulonephritis | Haematuria, oedema, hypertension 1 to 2 weeks after GAS | Not prevented by antibiotics; supportive; monitor renal function and blood pressure |
| Peritonsillar abscess | Trismus, uvular deviation, unilateral tonsillar bulge | Drainage plus antibiotics covering anaerobes |
| Retropharyngeal or deep neck abscess | Neck stiffness, drooling, toxic, airway compromise | IV antibiotics, contrast CT, surgical drainage |
| Lemierre syndrome | Worsening sore throat, high fever, neck pain, septic pulmonary emboli | Prolonged IV antibiotics; anticoagulation individualised |
| Descending necrotising mediastinitis | Chest pain, septic shock, mediastinal air or fluid | Emergency surgical drainage of neck and mediastinum; ICU |
The suppurative complications — peritonsillar abscess, retropharyngeal abscess, parapharyngeal abscess, Lemierre syndrome and descending necrotising mediastinitis — represent the progressive spread of infection through fascial planes. Each is managed by drainage where feasible, broad-spectrum intravenous antibiotics, and airway protection. The rarer the complication, the higher the stakes: descending necrotising mediastinitis has a mortality of twenty-five to forty per cent even with aggressive surgical and medical management. [10] [11]
The diagnostic and stewardship pitfalls are where fellowship marks are lost. The first is treating every sore throat with antibiotics without testing — the single biggest driver of unnecessary antibiotics and the one the IDSA explicitly prohibits. The second is giving amoxicillin to a child with EBV — producing the characteristic rash and a lifelong (usually false) penicillin-allergy label. The third is missing a deep neck infection by attributing neck stiffness to meningitis or by not examining the neck. The fourth is undertreating or delaying drainage of a peritonsillar abscess, allowing it to extend. Each is prevented by the same discipline: score, swab, treat only confirmed GAS, examine the neck, and escalate the red flags. [1] [10]
Prognosis & Disposition
The prognosis of uncomplicated GAS pharyngitis treated with penicillin is excellent: symptoms improve within forty-eight hours of starting antibiotics, the child is no longer infectious after twenty-four hours of therapy, and complete recovery is the rule. Untreated GAS resolves in three to five days, but the risk of acute rheumatic fever persists — which is why completing the full ten-day course matters even after symptoms resolve. Post-streptococcal glomerulonephritis is not prevented by antibiotics, but most children recover fully with supportive care. [1] [7]
Disposition is decided by the position on the severity spectrum. A well child with viral pharyngitis or confirmed GAS managed with oral antibiotics stays home with analgesia, a safety-net, and a planned review if not improving. A child with a peritonsillar abscess needs same-day drainage and may be managed as an outpatient or with a short admission. A child with a deep neck abscess is admitted for intravenous antibiotics, imaging, and possible surgical drainage. A child with airway compromise, sepsis or mediastinal extension goes to ICU with anaesthetics, ENT and surgery involved from the outset. [10] [11]
The child at high risk of rheumatic fever — Aboriginal and Torres Strait Islander children in endemic settings, or those with a personal history of ARF — needs a lower threshold to test and treat, reliable follow-up to confirm the ten-day course is completed, and, for secondary prevention after ARF, long-term benzathine penicillin prophylaxis. For these children, a sore throat is never just a sore throat; it is the gateway to a lifelong and preventable cardiac disease. [7] [8]
Special Populations
Aboriginal and Torres Strait Islander children living in remote and rural settings carry among the highest burdens of acute rheumatic fever and rheumatic heart disease in the world. In these communities, the threshold to test and treat sore throats is lower than in the general population, because the consequence of an untreated GAS infection is far more severe. Many regional guidelines recommend throat swabs for all sore throats in high-risk children and treatment of confirmed GAS, alongside broader public health measures addressing crowding, skin health and access to primary care. [7] [8]
Children under three years rarely develop GAS pharyngitis and usually have viral causes; routine testing is not recommended unless there are specific risk factors or close contact with a confirmed case. Sore throat in an infant is non-specific and should prompt a broader assessment — the diagnosis of GAS pharyngitis in an infant should be questioned and alternative diagnoses sought. [1]
Immunocompromised children — those on chemotherapy, with primary immunodeficiency, or post-transplant — are at higher risk of severe and atypical infections, including fungal and resistant bacterial pharyngitis and deep neck infections. The threshold for investigation, intravenous antibiotics and specialist input is lower, and the microbial differential is broader. [10]
Adolescents deserve specific attention because they are the group in whom EBV and Lemierre syndrome are most likely, and because the consequence of giving amoxicillin empirically (the EBV rash) is most damaging here. An adolescent with a sore throat needs a score, a swab, and a Monospot or EBV serology if the clinical picture fits — and a low threshold to investigate further if the sore throat does not resolve as expected. [9] [1]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | Testing stance | First-line |
|---|---|---|---|
| ANZ | RCH Melbourne, Therapeutic Guidelines | Score plus throat swab; lower threshold in high-risk communities | Phenoxymethylpenicillin or amoxicillin for 10 days |
| UK | NICE NG84 | No testing for most; delayed or no antibiotic; immediate if features of severity | Phenoxymethylpenicillin; clarithromycin if penicillin-allergic |
| North America | IDSA (Shulman 2012; Linder 2025 update) | Score plus RADT with culture back-up if negative in children | Penicillin V or amoxicillin for 10 days |
| High-risk / Indigenous | National ARF/RHD guidance | Lower threshold to test and treat; public health focus | Penicillin V; benzathine penicillin for ARF prophylaxis |
The evidence backbone begins with the IDSA guideline (Shulman 2012), which established the test-then-treat principle for GAS pharyngitis and formalised the recommendation against empirical antibiotics in children. The 2025 update (Linder et al) refines the risk-assessment approach using clinical scoring systems. The Cochrane review of antibiotics for sore throat (Spinks, Del Mar 2013) quantified the modest symptom benefit (about sixteen hours) and confirmed that antibiotics reduce suppurative complications, including peritonsillar abscess — but also confirmed that most sore throats resolve without antibiotics, underpinning selective prescribing. [1] [2] [6]
The clinical-score evidence rests on the McIsaac validation studies (McIsaac 1998 CMAJ, McIsaac 2004 JAMA), which showed that a structured clinical score reduces unnecessary antibiotic use without increasing missed GAS diagnoses, and the Aalbers 2011 systematic review, which validated the Centor score in adults. For rheumatic fever prevention, the AHA scientific statement (Gerber 2009) and the Nature Reviews Disease Primers on ARF and RHD (Zuhlke 2026) provide the evidence that ten days of penicillin prevents acute rheumatic fever and that the burden remains devastating in endemic populations. [3] [4] [5] [7] [8]
The live areas of nuance are the role of clinical scoring without testing (acceptable in adults in some settings but not recommended for children), the choice of RADT versus culture (culture back-up is recommended for negative RADT in children), the duration of therapy (ten days is evidence-based for penicillin V; shorter courses are under investigation), and the role of tonsillectomy for recurrent disease. A fellowship candidate shows depth by naming the guideline and the trade-off rather than reciting a single number. [1] [2]
Exam Pearls
The single discipline that keeps children safe is the same one that earns fellowship marks: score the sore throat, confirm GAS before treating, give ten days of penicillin when confirmed, and escalate the child with drooling, trismus or neck stiffness as a deep neck emergency while safety-netting the rest with a plan the family can act on. [1] [10]
And when you teach this topic, teach it as a model of selective antibiotic stewardship combined with vigilance — a common complaint where the modern default is test-then-treat, but where the rare child whose tonsillitis has become a mediastinal abscess depends on you having looked at the neck and recognised the shift from routine to emergency. [6] [11]
References
- [1]Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis, 2012.PMID 22965026
- [2]Linder JA, Patel SS, Lott L, et al. 2025 Clinical Practice Guideline Update by the Infectious Diseases Society of America on Group A Streptococcal (GAS) Pharyngitis: Risk assessment using clinical scoring systems in children and adults. Clin Infect Dis, 2025.PMID 41343363
- [3]McIsaac WJ, Kellner JD, Aufricht P, Vanjaka A, Low DE. Empirical validation of guidelines for the management of pharyngitis in children and adults. JAMA, 2004.PMID 15069046
- [4]McIsaac WJ, White D, Tannenbaum D, Low DE. The validity of a sore throat score in family practice. CMAJ, 2000.PMID 11033707
- [5]Aalbers J, O'Brien KK, Chan WS, et al. Predicting streptococcal pharyngitis in adults in primary care: a systematic review of the diagnostic accuracy of symptoms and signs and validation of the Centor score. BMC Med, 2011.PMID 21631919
- [6]Spinks A, Glasziou PP, Del Mar CB. Antibiotics for sore throat. Cochrane Database Syst Rev, 2013.PMID 24190439
- [7]Gerber MA, Baltimore RS, Eaton CB, et al. Prevention of rheumatic fever and diagnosis and treatment of acute Streptococcal pharyngitis: a scientific statement from the American Heart Association. Circulation, 2009.PMID 19246689
- [8]Zuhlke L, Trott K, Tsuboi M, et al. Acute rheumatic fever and rheumatic heart disease. Nat Rev Dis Primers, 2026.PMID 41748639
- [9]Centor RM, Atkinson NF, Ratliff AE, et al. Fusobacterium necrophorum oral infections - A need for guidance. Anaerobe, 2022.PMID 35122953
- [10]Darawish SM, Patel P, Scolaro C, et al. Deep neck space infections in children: Peritonsillar, retropharyngeal, parapharyngeal, and Ludwig's angina emergencies in the pediatric emergency department. Am J Otolaryngol, 2026.PMID 42275833
- [11]Suchecki M, Marzec J, Krawczyk P, et al. Retropharyngeal and parapharyngeal abscesses in children - a 9.5-year retrospective single-center analysis followed by literature review. Otolaryngol Pol, 2026.PMID 42417448
- [12]DiBlasi M, Shulman J, Sheyn A, et al. Increased pediatric head and neck abscesses following the COVID-19 pandemic. Laryngoscope, 2026.PMID 42425765