Paeds · ent-hearing-and-oral-health
Acute otitis media
Also known as Acute middle-ear infection · Acute suppurative otitis media · Ear infection
Fellowship guide to acute otitis media (AOM): the acute suppurative inflammation of the middle-ear mucosa behind an intact tympanic membrane, diagnosed from a bulging eardrum or new otorrhea rather than redness alone; the AAP three-part criteria; the Streptococcus pneumoniae, Haemophilus influenzae and Moraxella pathogens and the Eustachian-tube-dysfunction mechanism; severity grading and the age-and-laterality matrix that separates watchful waiting with a safety-net from immediate antibiotics; analgesia for every child; first-line high-dose amoxicillin 90 mg/kg/day twice daily with the penicillin-allergy pathway; the red flags of mastoiditis; recurrent AOM and grommet decisions; and the ANZ, UK and North American guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the fourteen-month-old who has had a cold for two days and now wakes at night screaming, tugging at her ear, with a fever. She is miserable but not toxic, and when you look in her ear the eardrum bulges towards you, is a dull red-yellow, and does not move when you puff air into the speculum. That picture — an acute, painful, bulging eardrum after a viral prodrome in a young child — is acute otitis media, and recognising the bulge (not the redness) is what separates a confident diagnosis from an over-called one. [1] [2]
Acute otitis media is an acute, infective inflammation of the middle-ear cleft — the mucosa lining the tympanic cavity, mastoid antrum and Eustachian tube — accompanied by a middle-ear effusion. The term implies the eardrum is intact at the moment of diagnosis; if the drum perforates, the child develops ear discharge (otorrhoea), which is itself a diagnostic and therapeutic milestone. It is one of the commonest reasons a young child is brought to medical care and prescribed an antibiotic, which is exactly why getting the diagnosis and the antibiotic decision right matters for both the individual child and antibiotic stewardship. [1] [3]
Why this matters at fellowship level is that AOM sits at the intersection of three things examiners test: a strict diagnostic rule (the bulging eardrum), a nuanced treatment decision (the age-and-laterality matrix), and a red-flag mindset (mastoiditis and the toxic child). The evidence base is mature — antibiotics help a little, on average, and carry a real cost — so the modern skill is selective, evidence-based prescribing combined with genuine safety-netting, not reflex treatment of every red eardrum. [6] [3]
Classification
Acute otitis media is best classified two ways at once: by how the eardrum and middle ear look (which confirms the diagnosis), and by how severe the episode is (which drives the antibiotic decision). Keeping these separate prevents the common error of treating every red eardrum the same way. [1] [2]
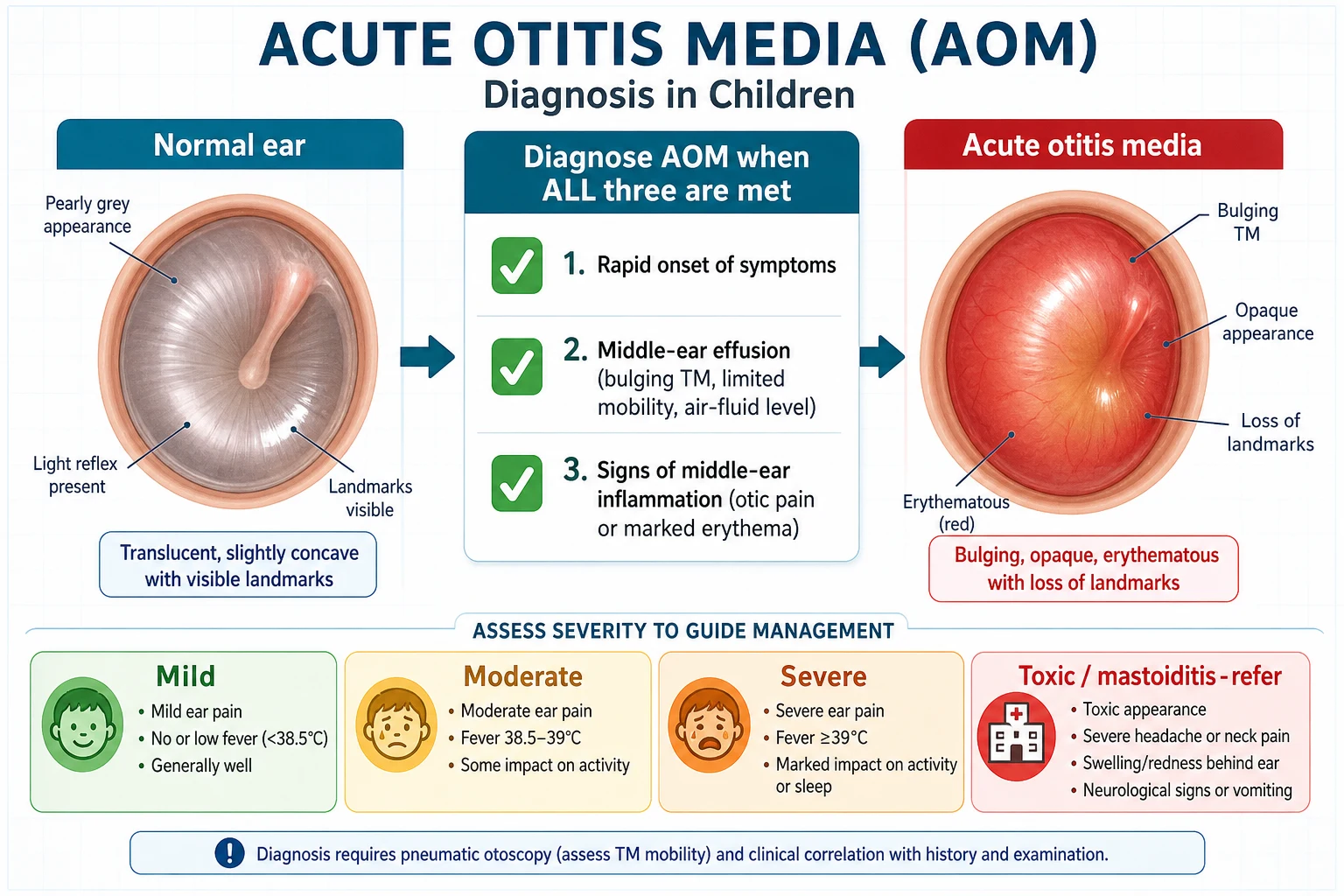
By appearance, the modern guideline diagnosis rests on the shape and mobility of the tympanic membrane. AOM is present when there is moderate-to-severe bulging of the drum, or new onset of ear discharge not caused by otitis externa. AOM may also be diagnosed when there is mild bulging together with recent ear pain or intense erythema. The common thread is a middle-ear effusion — a drum that is bulging or that does not move on pneumatic otoscopy — which is why AOM must not be diagnosed without one. A red drum in a crying, febrile child with no effusion is not AOM. [1] [2]
By severity, the AAP framework separates non-severe from severe AOM, and this single split, combined with age and laterality, decides whether to give antibiotics immediately or to watch and wait. Severe means ear pain that clearly interferes with the child's activity or sleep, or a fever of 39 °C or higher. Non-severe is everything else: mild ear discomfort and a lower fever in a child who is still playing and drinking. Laterality — one ear or both — is the second axis, because bilateral non-severe AOM in a young child is treated more readily than unilateral disease. [1] [3]
The numbers that anchor your viva
A separate and important category is recurrent AOM, defined as three or more well-documented episodes within six months, or four or more within twelve months (with at least one in the preceding six months). Recurrent disease raises the question of tympanostomy tubes (grommets), hearing assessment and an underlying contributor, and links this topic to otitis media with effusion and grommet decisions. [1] [10]
Epidemiology & Risk Factors
Acute otitis media is overwhelmingly a disease of early childhood. Incidence peaks between six and twenty-four months of age, and by three years roughly four in five children have had at least one episode; it then falls steadily through the school-age years. Boys are affected slightly more often than girls, and the seasonality tracks that of viral upper respiratory infections, clustering in autumn and winter. [2] [8]
The risk factors are the things that either bring a child into contact with more respiratory viruses or impair Eustachian tube function. Day-care attendance (especially large centres) and having older siblings increase viral exposure; parental smoking and household tobacco smoke irritate the nasopharyngeal mucosa; pacifier use beyond infancy and bottle-feeding while lying flat alter swallowing and tube mechanics; and not breastfeeding removes a modest protective effect. These modifiable factors are worth naming because they are the counselling opportunities that actually reduce recurrence. [2] [3]
The non-modifiable and structural risk factors matter because they change your threshold for investigation and referral. Cleft palate, Down syndrome and other craniofacial differences impair Eustachian tube drainage; primary immunodeficiency (including hypogammaglobulinaemia) and HIV predispose to severe or recurrent disease; and a family history of recurrent AOM raises a child's risk substantially. A child who recurs frequently or presents outside the usual age band deserves a deliberate search for one of these. [2] [8]
The microbiology has shifted with vaccination. Before pneumococcal conjugate vaccines, Streptococcus pneumoniae dominated; it remains the single commonest bacterial pathogen and the one most associated with severe disease, but non-typeable Haemophilus influenzae and Morazella catarrhalis now account for a larger share, and viral co-infection (respiratory syncytial virus, influenza, rhinovirus) is common and often drives the illness. Knowing the pathogens tells you both the first-line antibiotic and why beta-lactamase-producing organisms matter when amoxicillin fails. [8] [9]
Pathophysiology
The teaching model runs from the cold to the bulging drum, and it hinges on one piece of paediatric anatomy: the Eustachian tube. In a young child the tube is short, floppy and more horizontal than in an adult, so nasopharyngeal secretions and their microbes reach the middle ear more easily and drainage back to the nose is poorer — the structural reason AOM is a disease of toddlers. [2] [3]
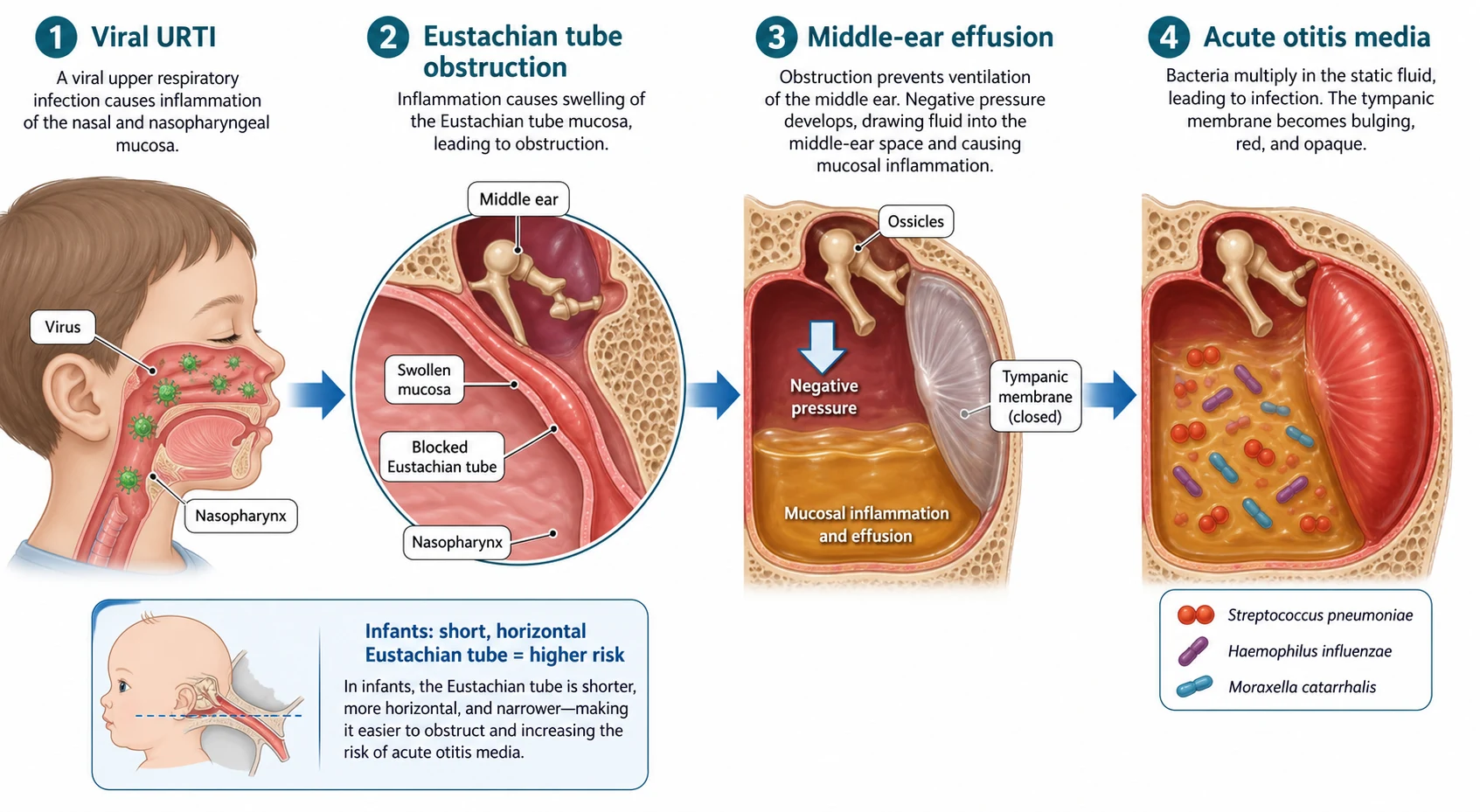
The chain begins with a viral upper respiratory infection, which inflames the nasopharyngeal mucosa and causes the Eustachian tube to swell and obstruct. With the tube blocked, the middle-ear mucosa absorbs the trapped air, generating negative middle-ear pressure, and a sterile transudate collects behind the drum. Static, nutrient-rich fluid in a warm space is then a perfect culture medium: the same bacteria that colonise the nasopharynx ascend the tube and multiply, converting the sterile effusion into a purulent, inflamed middle ear. [2] [8]
The clinical signs follow directly from the mechanics. Pus under pressure pushes the tympanic membrane outwards, so it bulges towards the examiner and loses its normal concavity and landmarks; inflammation makes it erythematous and opaque; and the effusion behind it means the drum no longer moves when you puff air into the speculum — the loss of mobility on pneumatic otoscopy that is the single most reliable physical sign. The pressure and inflammation also stimulate the richly innervated drum, producing the ear pain (otalgia) that is the hallmark symptom, and the systemic response to infection produces the fever and malaise. [1] [2]
A common misconception is that AOM is primarily a disease of the external ear. It is a middle-ear process: the pain is deep and throbbing, the pathology sits behind an intact drum, and the danger — mastoiditis, labyrinthitis, intracranial spread — comes from extension of middle-ear infection, not from the canal. Keeping this orientation straight explains every part of the assessment and management. [2] [11]
Clinical Presentation
The classic story is a young child, often after two to three days of a cold, who develops acute ear pain, fever and irritability. In a verbal child the history is easy: she points to her ear, complains of pain, and may say her hearing is muffled. The pain is typically worse at night and may wake the child, and a preceding coryzal illness is the rule rather than the exception. [1] [2]
In a pre-verbal infant the presentation is less specific and is the part examiners probe. Tugging or rubbing at an ear, unexplained irritability, restless or broken sleep, feeding less, vomiting, and a fever without an obvious source are all ways an infant with AOM presents. None of these is diagnostic on its own — ear-tugging is common and non-specific — but the combination of an upper respiratory prodrome with new ear-focused behaviour and fever should prompt a careful otoscopic examination rather than a default diagnosis of a "viral illness". [3] [2]
| Picture | Bedside findings | Immediate response |
|---|---|---|
| Non-severe AOM | Mild ear pain, low fever, well and playing, bulging drum | Analgesia; watchful waiting or antibiotics by the age-and-laterality matrix; safety-net |
| Severe AOM | Moderate-severe otalgia disturbing activity, fever 39 °C or higher, unwell | Analgesia plus immediate antibiotics; review at 48–72 h |
| AOM with perforation | Sudden relief of pain with purulent, sometimes bloody ear discharge | Analgesia; antibiotics by age and severity; keep the ear dry; most heal spontaneously |
| Toxic or complicated | Toxic, postauricular swelling or redness, protruding ear, neurological signs | Treat as mastoiditis or complication: urgent assessment, imaging, IV antibiotics, ENT |
The trap is the well-looking child whose drum is bulging and immobile but who has little pain — this is still AOM and still needs the antibiotic decision applied, because the otoscopic findings carry the diagnosis regardless of symptom intensity. The opposite trap is the distressed, febrile child with a red but flat, mobile drum: that is not AOM, and treating it with antibiotics both fails the child and erodes stewardship. [1] [6]
Atypical features should always shift your thinking: a toxic or septic appearance, swelling or tenderness behind the ear, an ear pushed forwards and downwards, neurological signs, severe headache or neck stiffness, or disease in an immunocompromised or very young infant. These point away from simple AOM and toward a complication or a more serious differential, and they change the pathway from outpatient care to urgent assessment. [11] [1]
Differential Diagnosis
Sort the differential into three groups: the other middle-ear states that mimic AOM, the external-ear and referred causes of ear pain, and the complications that change everything. The aim is to confirm AOM on otoscopic findings while never anchoring on it when the drum or the child does not fit. [1] [2]
Acute otitis media
the diagnosis to confirm
- Bulging, opaque, poorly mobile drum
- Acute otalgia, fever, viral prodrome
- Effusion behind the drum
- Analgesia plus selective antibiotics
Otitis media with effusion
- Non-acute; effusion without inflammation
- Painless hearing loss or incidental finding
- Flat, retracted or amber drum, no mobility
- Watchful; hearing test if persistent
Otitis externa
- Pain on tragal tug, canal oedema
- Discharge, normal drum if seen
- Often swimming or trauma
- Topical antibiotic/steroid drops
Red drum without AOM
- Crying, fever, struggling child
- Flat drum with normal mobility
- No effusion
- Do not diagnose or treat as AOM
Referred otalgia
- Teething, pharyngitis, TMJ, dental
- Normal otoscopy
- Normal middle ear
- Treat the source, not the ear
Otitis media with effusion (OME) is the most important mimic to separate, because it is common, painless and does not need antibiotics. An effusion without acute inflammation gives a flat, retracted or amber-coloured drum with no mobility and no acute pain or fever; the child may have reduced hearing or be entirely well, and the management is watchful waiting with hearing assessment if the effusion persists. Confusing OME with AOM is a leading cause of unnecessary antibiotics. [2] [1]
Otitis externa causes ear pain and discharge but the problem is in the canal: there is tenderness on movement of the tragus or pinna, an oedematous canal with debris, and a normal drum if you can see it. It often follows swimming or local trauma, and it is treated with topical antibiotic and corticosteroid drops, not oral antibiotics. Referred otalgia from teething, pharyngitis, tonsillitis, dental disease or temporomandibular joint problems gives ear pain with a completely normal otoscopy — the lesson is always to look at the drum before attributing ear pain to AOM. [1] [3]
Clinical & Bedside Assessment
Assessment is clinical and centred on a good otoscopic view of the drum, which is harder than it sounds in a wriggling, painful toddler. Take a focused history — the prodrome, the onset and severity of ear pain, any discharge, fever, feeding and activity, previous episodes, daycare and smoke exposure, immunisation status, and any craniofacial or immune problem — and then settle the child on a carer's lap and warm the speculum before you look. [1] [3]
The single highest-yield examination skill is pneumatic otoscopy: a tight-fitting speculum in a still ear, with a bulb attached, so you can puff air and watch whether the drum moves. A normal drum moves briskly; a drum with an effusion behind it is stiff and does not move. Bulging, opacification, loss of landmarks, an abnormal colour (white, yellow or haemorrhagic rather than pearly grey) and reduced or absent mobility together make the diagnosis, and mobility is the most discriminating of these. [1] [3]
Grading severity to drive the antibiotic decision
Toxic / complicated
Toxic, postauricular signs, neurological features — emergency pathway
Deliberately avoid the common errors: diagnosing AOM from a red drum alone (crying and fever redden a normal drum), failing to assess mobility (the key sign), cerumen that hides the drum being left in place when a view is essential, and trusting a single glimpse in a struggling child. If you cannot see the drum, remove the wax or ask for help rather than diagnose on probability. [1] [2]
Investigations
Acute otitis media is a clinical diagnosis and needs no routine tests in a typical case. Blood tests, inflammatory markers, viral swabs and imaging add nothing to the otoscopic diagnosis and are reserved for the toxic child, the treatment failure, or the suspected complication. The default in a well child with a clear otoscopic finding is analgesia and the antibiotic decision — no investigations. [1] [3]
Tympanometry is a reasonable adjunct when the otoscopic view is uncertain or you need to document an effusion objectively, but it does not separate acute inflammation from a chronic effusion — that distinction remains clinical, based on pain, fever and the appearance of the drum. A hearing test is not part of the acute workup; it belongs later, when an effusion and hearing concern have persisted, linking forward to the OME and grommet-decisions topic. [2] [1]
When genuine treatment failure, immunocompromise or a severe course raises the question of the causative organism, tympanocentesis — needle aspiration of middle-ear fluid through the drum — can identify the pathogen and its sensitivities, but it is an ENT or skilled-operator procedure used selectively, not a routine diagnostic step. Imaging is reserved for suspected complications: a CT temporal bone for mastoiditis, and MRI when intracranial extension is suspected. [11] [1]
Management — Resuscitation
For the small number of children who are toxic or have a complication, the priority shifts from the routine AOM pathway to the recognition and stabilisation of a serious infection. Assess airway, breathing and circulation, manage pain and fever, obtain intravenous access, take cultures, and start broad intravenous antibiotics — while arranging urgent imaging and ENT or paediatric infectious-diseases input for the suspected complication. [11] [1]
Acute mastoiditis is the complication to recognise at the bedside: a toxic, febrile child with postauricular pain, swelling, erythema and tenderness, and an ear pushed forwards and downwards by a subperiosteal abscess. It is a surgical as well as a medical emergency — arrange urgent CT of the temporal bone, start intravenous antibiotics covering the AOM pathogens, and involve ENT early, because a proportion need cortical mastoidectomy or drainage. The red flags for any intracranial spread (severe headache, neck stiffness, neurological signs, persistent vomiting) demand imaging and a lower threshold for lumbar puncture once it is safe. [11] [1]
For the much larger group of well children with uncomplicated AOM, "resuscitation" simply means analgesia, and this is the step most often under-done. Ear pain from a bulging drum is severe, and relief of that pain is the first treatment for every child regardless of the antibiotic decision. [1] [7]
Management — Definitive & Stepwise
The definitive management of AOM is built in three layers: analgesia for every child, an antibiotic decision driven by age, laterality and severity, and a clear reassessment and safety-net. Treating these as distinct steps prevents both under-treatment of the sick child and over-treatment of the well one. [1] [6]
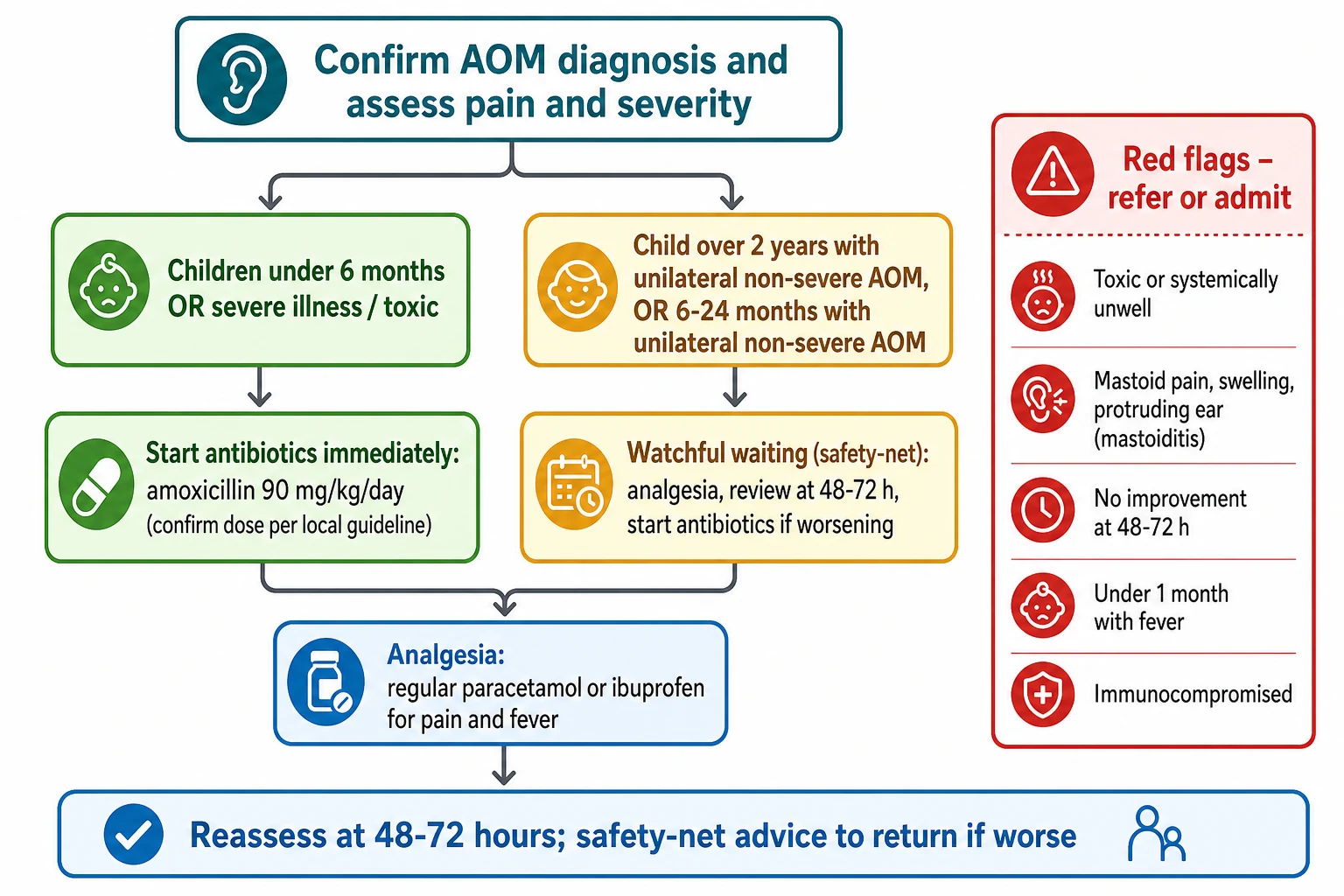
Step one — analgesia for everyone. Regular weight-based analgesia is the universal first treatment. Give paracetamol 15 mg/kg orally every four to six hours (maximum 60 mg/kg/day, not exceeding 4 g/day), or ibuprofen 5–10 mg/kg orally every six to eight hours (maximum 30 mg/kg/day); ibuprofen is generally avoided in the dehydrated child and in infants under three months. Topical anaesthetic ear drops (for example lignocaine or a tetracaine-based preparation where licensed) can give short-term additional relief in a child with an intact drum, though evidence for benefit is modest. [7] [2]
Step two — the antibiotic decision. Apply the AAP age-and-laterality matrix. Prescribe antibiotics immediately for: any child under six months with AOM; children six to twenty-three months with bilateral AOM (whether severe or not); children six to twenty-three months with unilateral severe AOM; and any child two years or older with severe AOM (bilateral or unilateral). Offer watchful waiting (a safety-net prescription or a planned review) for: children six to twenty-three months with unilateral non-severe AOM, and children two years or older with unilateral or bilateral non-severe AOM — provided the diagnosis is certain and the family is reliable and safety-netted. Severe, recall, means otalgia interfering with activity or fever of 39 °C or higher. [1] [3]
Drugs in acute otitis media
Step three — first-line antibiotic when indicated. High-dose amoxicillin 90 mg/kg/day orally in two divided doses (maximum 4 g/day) is first-line, chosen to overcome intermediate penicillin resistance in pneumococci; the lower traditional dose is no longer adequate. Duration is ten days for children under two years, seven days for those two to five years, and five to seven days for those six years and older, reflecting the faster resolution in older children. Use amoxicillin-clavulanate (90 mg/kg/day of the amoxicillin component, twice daily) when the child has AOM with purulent conjunctivitis (a beta-lactamase-producing Haemophilus pattern), when amoxicillin fails at 48–72 hours, or for recurrent disease, and switch to a cephalosporin or macrolide in penicillin allergy according to the severity of the allergy. [1] [8]
The stepwise pathway
Confirm AOM on a bulging, poorly mobile drum or new otorrhea; assess pain and grade severity.
Give regular weight-based analgesia (paracetamol and/or ibuprofen) to every child.
Apply the age-and-laterality matrix: immediate antibiotics for the young, bilateral, severe or under-6-months child; watchful waiting with a safety-net for older unilateral non-severe disease.
When antibiotics are given, use high-dose amoxicillin 90 mg/kg/day twice daily; switch to amoxicillin-clavulanate for failure or conjunctivitis-AOM.
Reassess at 48–72 hours; if not improving, confirm the diagnosis, start or change antibiotics, and reconsider a complication.
Safety-net every family: return early if worse, and arrange follow-up and a hearing check if symptoms or effusion persist.
Step four — managing failure and recurrence. A child who has not improved at 48–72 hours needs reassessment rather than a reflex repeat prescription: confirm the diagnosis (was it really AOM, or OME?), check for a complication (mastoiditis, perforation), and either start amoxicillin if they were observed or switch to amoxicillin-clavulanate if they failed amoxicillin. Recurrent AOM (three episodes in six months, or four in a year with one recent) should prompt a search for a contributor, hearing assessment, and referral for consideration of tympanostomy tubes, which reduce the frequency of further episodes. [1] [10]
EAR-DX
Specific Subtypes & Scenarios
AOM with spontaneous perforation presents as sudden relief of pain with a purulent, sometimes blood-tinged ear discharge, because the build-up of pressure has ruptured the drum. The diagnosis is still AOM (new otorrhea not due to otitis externa is a diagnostic criterion), the perforation usually heals on its own within a couple of weeks, and antibiotics are given by the same age-and-severity rules; keep the ear dry and review to confirm the drum has healed and the hearing is normal. [1] [2]
AOM with purulent conjunctivitis is a distinct syndrome caused by non-typeable, beta-lactamase-producing Haemophilus influenzae. It does not respond well to amoxicillin alone, so treat it from the outset with amoxicillin-clavulanate rather than plain amoxicillin — a high-yield exam point because it is the main exception to amoxicillin as first-line. [8] [1]
Venekamp 2015 — Cochrane (PMID 26099233)
Systematic review of randomised trials of antibiotics versus placebo or no treatment
Key finding
Antibiotics modestly increased the proportion of children with pain or fever resolved at two to three days, but most children recovered regardless; the benefit was concentrated in children under two years with bilateral AOM and in those with otorrhoea. Antibiotics increased vomiting, rash and diarrhoea.
Practice change
Antibiotics have a real but small average benefit, so the skill is selecting who benefits most (the young, bilateral and severe) and safety-netting the rest — the foundation of selective prescribing.
The infant under six months is treated with antibiotics rather than observation, because the diagnostic certainty is lower, the consequences of missing a serious infection are higher, and the evidence for safety of observation is weakest in this age group. A febrile, ill infant under one month with any ear finding is not managed as simple AOM at all — it enters the urgent septic-workup and admission pathway for the young febrile infant. [1] [3]
Recurrent AOM is managed by confirming and documenting each episode, addressing modifiable risk factors (smoke exposure, feeding position, daycare where possible), assessing hearing, and referring for consideration of tympanostomy tubes (grommets) when the recurrence meets the threshold, since the Cochrane evidence shows they reduce the number of further episodes over the following six to twelve months, at the cost of a small rate of tympanic membrane changes. The decision belongs with the family after balanced counselling, and it links directly to the OME and grommet-decisions topic. [10] [1]
Complications & Pitfalls
Serious complications of AOM are uncommon in the antibiotic era but remain the reason AOM cannot be trivialised. The most common is tympanic membrane perforation, which usually heals spontaneously. Persistent otitis media with effusion follows many episodes and is the usual reason for transient hearing reduction; it generally resolves over weeks but, when it persists, leads into the hearing and grommet pathway. [2] [1]
The suppurative complications are the dangerous ones. Acute mastoiditis — extension of infection into the mastoid air cells with subperiosteal abscess — is the commonest and the one to recognise at the bedside through postauricular pain, swelling and a protruding ear; it needs urgent imaging, intravenous antibiotics and often surgery. Beyond it lie the rarer labyrinthitis (vertigo, nystagmus, hearing loss), facial nerve palsy as the nerve traverses the middle ear, venous sinus thrombosis, meningitis, and epidural, subdural or brain abscess, each presenting with escalating systemic or neurological features and each demanding imaging, intravenous antibiotics and neurosurgical or ENT input. [11] [1]
| Complication | Recognise it by | Key action |
|---|---|---|
| TM perforation / otorrhoea | Sudden pain relief with discharge | Antibiotics by rules; keep dry; review healing |
| Acute mastoiditis | Postauricular pain, swelling, erythema, protruding ear | CT, IV antibiotics, ENT — often surgery |
| Labyrinthitis | Vertigo, nystagmus, hearing loss | Urgent ENT; imaging; IV antibiotics |
| Facial nerve palsy | Acute lower motor neuron facial weakness | IV antibiotics; ENT; often myringotomy |
| Meningitis / abscess / sinus thrombosis | Headache, neck stiffness, neurological signs, seizures | Emergency imaging, IV antibiotics, neurosurgery |
The diagnostic and stewardship pitfalls are where most marks are lost. The first is over-diagnosing AOM from a red drum alone — the single biggest driver of unnecessary antibiotics, corrected by insisting on a bulging or immobile drum. The second is confusing OME with AOM and treating a chronic, painless effusion with repeated courses of antibiotics that cannot help. The third is poor safety-netting, sending a family home without a concrete return plan and then re-presenting late with a complication. Each is avoided by the same discipline: confirm the bulge, separate acute from chronic, and give a written, specific safety-net. [1] [6]
Prognosis & Disposition
The prognosis of uncomplicated AOM is excellent. Most children improve within two to three days whether or not they receive antibiotics, pain typically settles as the effusion drains or the drum perforates, and the great majority recover completely without sequelae. Antibiotics shorten symptoms by roughly one day on average and modestly reduce early treatment failure, with the largest benefit in the youngest, the bilateral and those with otorrhoea — which is exactly why selective prescribing is both safe and evidence-based. [6] [5]
Disposition is decided by severity, age and response rather than by a fixed rule. A well child with non-severe AOM managed with analgesia and a safety-net can stay home with a clear plan; a child given immediate antibiotics stays home too, with a planned review at 48–72 hours. Admission is reserved for the toxic or young febrile infant, the child with a complication such as mastoiditis, the child who cannot tolerate oral fluids or analgesia, the genuine treatment failure, or the family whose social or geographical circumstances make safe review impossible. [1] [11]
Safety-net advice is part of the treatment and must be concrete and written. Tell the family to return early — at any time, not at 48 hours — if the pain gets worse or does not improve, if the child becomes toxic, drowsy, pale or develops swelling behind the ear, if there is persistent vomiting, a rash that does not blanch, or simply if they are worried. Pair this with a planned review at 48–72 hours for a child under observation, and a hearing check if effusion or hearing concern persists beyond three months. [1] [2]
Special Populations
Infants under six months are treated with antibiotics rather than observation, and a febrile infant under one month is not managed as AOM at all but enters the urgent young-febrile-infant septic pathway. The youngest children have the least reserve, the hardest examination, and the greatest risk of a serious bacterial illness masquerading as a simple ear infection, so the default is caution. [1] [3]
Children with craniofacial anomalies or immunodeficiency — cleft palate, Down syndrome, primary immunodeficiency, HIV, or those on immunosuppression — have a higher burden and severity of otitis media and often recurrent or chronic disease. They need a lower threshold for antibiotics and for specialist input, active surveillance of hearing, and coordination with an ENT and audiology service, because the long-term risk is of persistent effusion and conductive hearing loss affecting development and learning. [2] [8]
Indigenous, rural and remote children in many settings carry a far higher burden of recurrent and chronic suppurative ear disease than the general population, with early onset, frequent episodes, persistent effusion and a substantial risk of hearing loss that affects language, learning and social development. The equity-critical interventions are early detection, reliable treatment of acute episodes, systematic hearing surveillance, and culturally safe, coordinated long-term care — recognising that for these children a single acute episode is often part of a chronic disease, not an isolated event. [9] [2]
Children with cochlear implants, existing grommets or craniofacial syndromes need particular care: a middle-ear infection in an implanted child is a potential threat to the device and a route to meningitis, so the threshold for antibiotics, ENT involvement and aggressive treatment of any AOM is lower than for the general child. [1] [11]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | Antibiotic stance | First-line |
|---|---|---|---|
| ANZ | RCH Melbourne, Therapeutic Guidelines, NPS | Analgesia first; safety-net or delayed prescribing for many older children | Amoxicillin 90 mg/kg/day BID when indicated |
| UK | NICE NG91 | No antibiotic or delayed prescribing for most; immediate if systemically unwell or high-risk | Amoxicillin; clarithromycin if penicillin-allergic |
| North America | AAP (Lieberthal 2013) | Age-and-laterality matrix; observation for selected non-severe cases | Amoxicillin 90 mg/kg/day BID |
| Indigenous / remote | National guidance (e.g. Deadily Ears) | Lower threshold; treat acute episodes and manage chronic disease | Coordinated surveillance plus hearing care |
The evidence backbone you should be able to name starts with the Cochrane review of antibiotics for AOM (Venekamp 2015), which established that antibiotics produce a modest reduction in pain at two to three days at the cost of more vomiting, rash and diarrhoea, with the greatest benefit in children under two years with bilateral disease and in those with otorrhoea. Two contemporary placebo-controlled trials sharpened this: Hoberman 2011 (NEJM) showed a modest benefit of amoxicillin-clavulanate in children under two years, and Tähtinen 2011 (NEJM) showed a similar small benefit, both confirming that most children recover without antibiotics while a minority benefit clearly. [6] [4] [5]
For prevention, the Cochrane review of pneumococcal conjugate vaccines (Fortanier 2014) confirmed that vaccination prevents a meaningful fraction of otitis episodes, especially pneumococcal disease, which underlies the fall in AOM burden in vaccinated populations. For recurrent disease, the Cochrane review of grommets for recurrent AOM (Venekamp 2018) found that ventilation tubes reduce the number of further episodes over the following six to twelve months, balanced against tympanic-membrane sequelae — informing the shared decision around tubes. [9] [10]
The live areas of nuance are the exact cut-offs of the age-and-laterality matrix, the choice of plain amoxicillin versus amoxicillin-clavulanate as routine first-line, the duration of therapy by age, and the threshold for tympanostomy in recurrent disease — all areas where reasonable guidelines differ and where a fellowship candidate shows depth by naming the guideline and the trade-off rather than reciting a single number. [1] [6]
Exam Pearls
The single move that keeps children safe is the disciplined one: confirm the bulge, give analgesia to everyone, split the antibiotic decision by age and severity, and treat the toxic child or any postauricular sign as an emergency while safety-netting the rest with a plan the family can act on. [1] [11]
And when you teach AOM, teach it as a model of antibiotic stewardship — a common illness where the default used to be an antibiotic and the modern default is thoughtful selection — while never letting the routine of a familiar complaint dull your alertness to the rare child whose ear infection has spread to the mastoid or the brain. [6] [2]
References
- [1]Lieberthal AS, et al. The diagnosis and management of acute otitis media. Pediatrics, 2013.PMID 23439909
- [2]Schilder AG, et al. Otitis media. Nat Rev Dis Primers, 2016.PMID 27604644
- [3]Coker TR, et al. Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: a systematic review. JAMA, 2010.PMID 21081729
- [4]Hoberman A, et al. Treatment of acute otitis media in children under 2 years of age. N Engl J Med, 2011.PMID 21226576
- [5]Tähtinen PA, et al. A placebo-controlled trial of antimicrobial treatment for acute otitis media. N Engl J Med, 2011.PMID 21226577
- [6]Venekamp RP, et al. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev, 2015.PMID 26099233
- [7]Foxlee R, et al. Topical analgesia for acute otitis media. Cochrane Database Syst Rev, 2006.PMID 16856108
- [8]Casey JR, Pichichero ME Changes in frequency and pathogens causing acute otitis media in 1995-2003. Pediatr Infect Dis J, 2004.PMID 15361720
- [9]Fortanier AC, et al. Pneumococcal conjugate vaccines for preventing otitis media. Cochrane Database Syst Rev, 2014.PMID 24696098
- [10]Venekamp RP, et al. Grommets (ventilation tubes) for recurrent acute otitis media in children. Cochrane Database Syst Rev, 2018.PMID 29741289
- [11]Anne S, et al. Medical Versus Surgical Treatment of Pediatric Acute Mastoiditis: A Systematic Review. Laryngoscope, 2019.PMID 30284265