Paeds · fetal-neonatal-and-perinatal
Family-integrated developmental care in NICU
Also known as Family-integrated developmental care in NICU · Family Integrated Care (FiCare) · Developmental care in the NICU · NIDCAP · Family-centred neonatal care
Fellowship guide to family-integrated developmental care in the NICU, covering the FiCare model, the developmental care bundle, the evidence from the O'Brien 2018 cluster RCT and kangaroo-mother-care trials, and equitable implementation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A preterm infant admitted to a neonatal intensive care unit is separated from the parent at exactly the moment the brain is growing fastest and the autonomic nervous system is least able to regulate itself. The traditional NICU, built around monitoring, procedures, and staff-delivered care, adds bright light, loud noise, repeated pain, and parent separation on top of that vulnerability. Family-integrated developmental care is the combined response to that problem: it reshapes the environment to protect the developing brain and it reshapes the relationship so that parents become the infant's primary caregivers rather than visitors. [1]
The two halves of the name are easy to conflate but worth separating for an examiner. Developmental care (best known through Heidelise Als's Newborn Individualized Developmental Care and Assessment Program, NIDCAP) modifies what is done to and around the infant — light, sound, sleep, positioning, handling, and pain — so that the environment matches what the immature brain can tolerate. Family Integrated Care (FiCare), developed in Canada and tested in the 2018 multicentre cluster randomised trial, changes who does the caring: parents are educated, supported, and present at least eight hours a day to deliver hands-on care, while the nurse shifts from primary carer to teacher and mentor. [2]
Classification
The three terms an examiner will ask you to separate sit along a spectrum of how much the parent does. At one end the environment is changed but staff deliver all care; at the other the parent delivers most care and the staff coach. Naming the spectrum prevents the common error of treating these as synonyms. [5]
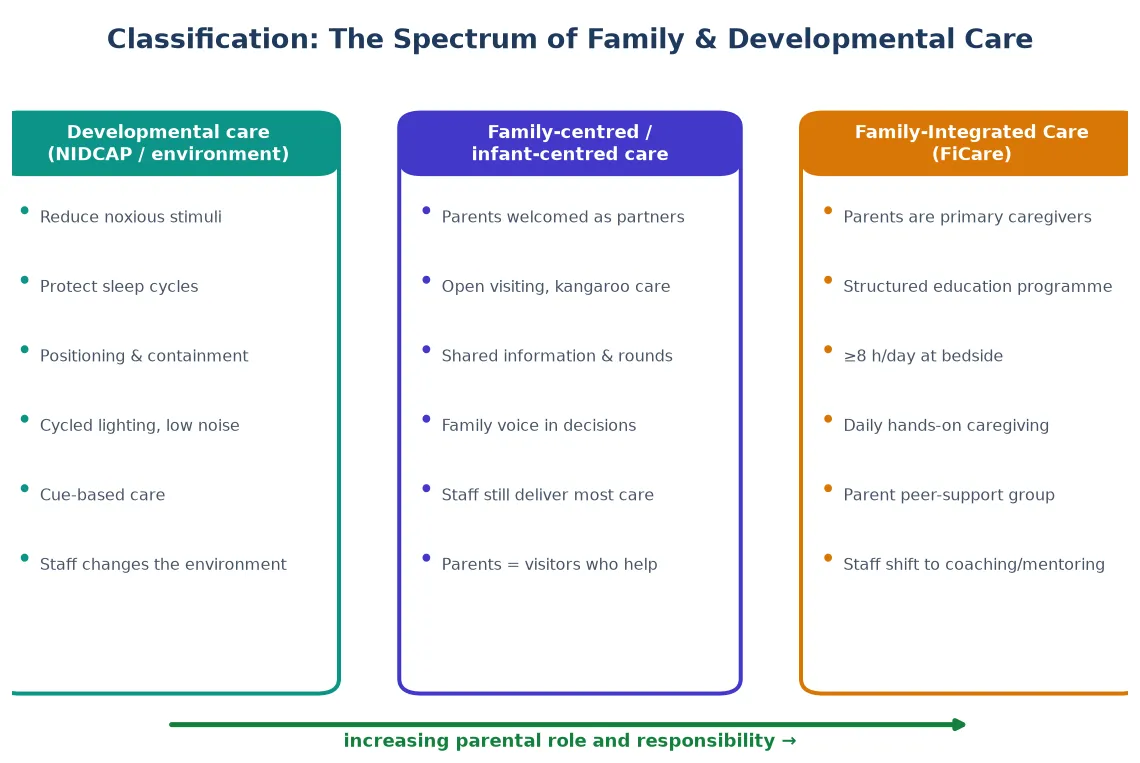
Developmental care (NIDCAP and the bundle) is environment- and handling-focused. The unit is darkened and quietened, sleep is protected, care is clustered, the infant is positioned in flexion and contained, and pain is minimised. Staff still deliver the care; parents are welcome but not central to the model. [5]
Family-centred (or infant-centred) care welcomes parents as partners: open visiting, kangaroo care, shared information, and a place on rounds. The parent's voice is honoured, but the staff still deliver most hands-on care — the parent remains, in effect, an involved visitor. [8]
Family Integrated Care (FiCare) goes the furthest. Parents are the primary caregivers for at least eight hours a day, they complete a structured education programme, they keep the clinical record, they join a parent peer-support group, and they are present on medical rounds. The nurse's job description changes from doing the care to teaching, mentoring, and supervising it. [1]
[2]Epidemiology & Risk Factors
The population that most needs this model is the population the NICU is built for: very and extremely preterm infants, who may spend weeks to months in hospital during the most rapid phase of brain growth. These infants are exposed to hundreds of painful procedures, sustained bright light and noise, and prolonged separation from parents — all of which independently predict worse neurodevelopmental and behavioural outcomes. [10]
The family side carries its own epidemiology. Between a quarter and half of NICU parents score above threshold for anxiety, depression, or acute stress on validated tools such as the Parental Stressor Scale: NICU (PSS:NICU) and the Edinburgh Postnatal Depression Scale. Stress is driven by the infant's appearance and behaviour, the alteration of the parental role, and the sights and sounds of the unit — precisely the levers that family-integrated and developmental care are designed to change. [4]
Equity is the central risk-factor question. The eight-hour daily presence requirement assumes a parent who can be physically present, who has accommodation near the unit, who speaks the working language, and who has leave, childcare, and income to survive the stay. Single parents, families from remote and rural areas, migrant and refugee families, those in unstable housing, and those with their own illness or family violence are systematically less able to participate in a programme designed in its simplest form — and a poorly designed programme therefore widens inequity rather than closing it. [8]
Pathophysiology
To understand why changing the NICU environment and bringing parents to the cot-side is a clinical intervention rather than a kindness, picture the preterm brain between 23 and 34 weeks. This is the critical window of dendritic arborisation, synaptogenesis, and subplate development — the architecture on which all later cognition and behaviour is built. The cortex is exquisitely plastic, which means it is also exquisitely disruptable. [10]
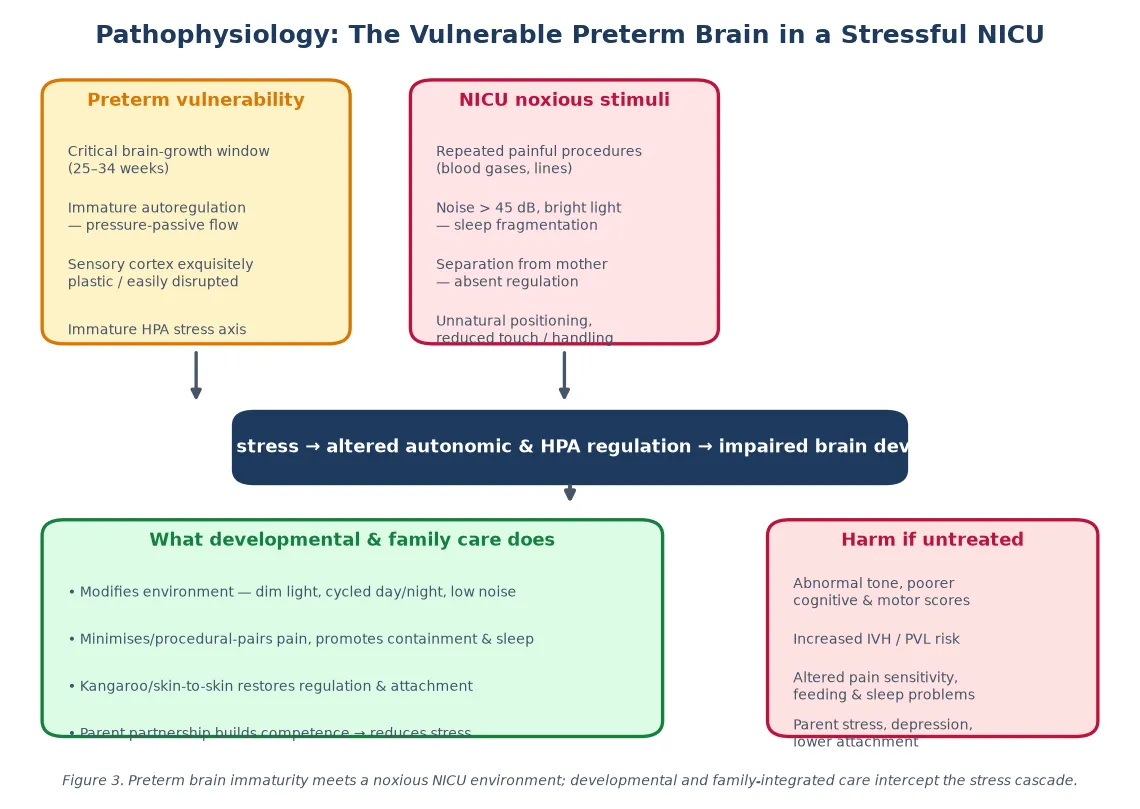
Three mechanisms turn the NICU experience into brain harm. First, cerebral autoregulation is immature, so the preterm circulation is pressure-passive — swings in blood pressure with handling, pain, or agitation are transmitted directly to the fragile cerebral vasculature, contributing to intraventricular haemorrhage and periventricular leukomalacia. Second, the hypothalamic-pituitary-adrenal stress axis is immature and easily upregulated; repeated painful procedures and fragmented sleep drive sustained cortisol elevations that alter brain architecture and later pain sensitivity. Third, sensory mismatch — bright light, loud noise, unnatural positioning, and absent maternal regulation — disrupts the patterned sensory input the brain expects during this window. [5]
The counter-intervention is mechanical. Skin-to-skin (kangaroo) contact restores maternal autonomic and neuroendocrine regulation: it stabilises heart rate, respiration, temperature, and oxygenation, organises behavioural state, and reduces cortisol. Dim and cycled lighting, noise below 45 decibels, protected sleep, containment, and procedural analgesia each remove a discrete stressor from a system that has no reserve to absorb it. [6]
Clinical Presentation
The preterm infant under environmental stress shows it behaviourally. Autonomic signs — desaturations, bradycardias, colour changes, sighing, hiccups, and gut motility changes — are the most visible. Motor signs include flaccidity or hypertonicity, finger splay, arching, and grimacing; state signs include inability to achieve or maintain quiet sleep and frequent startles; attentional signs include gaze aversion and inability to lock on a face. These are the avoidance cues of the Als synactive framework, and they signal that the current environment or handling exceeds the infant's threshold. [10]
Stability cues — approach cues — look the opposite: sustained physiologic calm, flexed and contained posture, smooth movements, sustained sleep states, and the ability to engage visually. Reading these cues is the bedside skill developmental care teaches, and cue-based care (feeding only when the infant is organised, clustering care around sleep) is its operational expression. [5]
Parental stress has its own presentation. The avoidant parent rarely visits and disengages at the cot-side; the hypervigilant parent watches every monitor and resists handing the infant back; the parent with depression is tearful, withdrawn, and anhedonic. Each pattern predicts poorer bonding, lower breastfeeding rates, and worse long-term family outcomes, and each is a target for the relational half of family-integrated care. [4]
Differential Diagnosis
When a preterm infant is autonomic and unstable, the environment is only one possibility, and the dangerous ones must not be missed. Sepsis presents with temperature instability, lethargy, feeding intolerance, and rising respiratory support. Anaemia of prematurity causes desaturation, tachycardia, and poor weight gain. A patent ductus arteriosus produces a widened pulse pressure, bounding pulses, and pulmonary overflow. Reflux, intraventricular haemorrhage, and apnoea of prematurity each have their own signature. Environmental and procedural stress is a diagnosis of pattern — instability during and after handling that resolves with containment and reduction of stimuli — and it coexists with these medical problems rather than excluding them. [5]
When a parent seems disengaged, the differential is similarly broad. Postnatal depression and anxiety are common and treatable. A language barrier may look like disengagement until an interpreter is used. Prior perinatal loss, family violence, substance use, and untreated parental illness all change a parent's behaviour at the cot-side, and none are addressed by simply inviting the parent to "be more involved". [4]
| Cause | Key Features | Action |
|---|---|---|
| Environmental/procedural stress | Instability during/after handling; resolves with containment | Pause, contain, cluster care, reduce stimuli, skin-to-skin |
| Sepsis | Temperature instability, lethargy, rising CRP/support | Sepsis screen, cultures, antibiotics |
| Anaemia of prematurity | Tachycardia, desaturation, low Hb | Transfuse if symptomatic and threshold met |
| PDA | Murmur, bounding pulses, widened pulse pressure | Echocardiogram, fluid restriction, consider closure |
| Gastro-oesophageal reflux | Vomiting, desaturation after feeds, arching | Positioning, feed thickening, rule out other causes |
| Intraventricular haemorrhage | Sudden deterioration, seizures, full fontanelle | Cranial ultrasound, neurosurgical review if progressive |
Clinical & Bedside Assessment
Assessment happens at three levels — the infant, the environment, and the family. At the cot-side you read the infant's behavioural organisation using the synactive framework, asking at each contact whether the infant can maintain autonomic, motor, and state stability under the current handling. The formal version is the NIDCAP naturalistic observation, in which a trained observer records the infant's behavioural cues before, during, and after a care event and tailors the care plan to the individual's thresholds. [10]
The environment is auditable. A simple decibel meter checks whether noise stays below 45 decibels; a lux meter checks whether lighting is dimmed and cycled with a day-night pattern; a walk-through checks that care is clustered, sleep is protected, and the infant is positioned in flexion with containment. These are quick, reproducible, and often revealing. [11]
The family assessment is relational and mental-health focused. The PSS:NICU quantifies stress across three domains — infant appearance and behaviour, parental role alteration, and sights and sounds of the unit — and the Edinburgh Postnatal Depression Screen flags depression that needs its own treatment. The parent-infant relationship is observed directly: who reaches for whom, how the parent holds and talks to the infant, and how the infant responds. Readiness to take on primary caregiving is assessed jointly by nurse and parent against the structured competencies of the programme. [4]
Investigations
There are no routine blood or imaging investigations for developmental or family care — the model is behavioural and relational. What exists is a set of monitoring and research tools that quantify the physiology the model tries to protect. Continuous or amplitude-integrated EEG documents sleep-state architecture and seizure activity. Near-infrared spectroscopy measures cerebral oxygenation during handling. Salivary or hair cortisol indexes the stress burden over time. Each can demonstrate harm or benefit but none is standard clinical practice in most units. [10]
What is standard is programme-level measurement. A FiCare or developmental-care service tracks length of stay, weight-gain velocity, exclusive breastmilk at discharge, nosocomial infection rate, readmission rate, and validated parental stress and anxiety scores before and after the programme. These metrics are the evidence the intervention is working in your unit, and they are the outcomes reported in the landmark trials. [2]
Management — Resuscitation
The immediate measures belong to every preterm admission regardless of model of care, because they cost nothing and prevent harm from the first hour. Protect sleep by clustering handling and procedures and leaving the infant undisturbed between. Dim the light and, as soon as feasible, cycle it to a day-night pattern. Keep noise below 45 decibels by lowering alarms, speaking softly, and closing portholes. Position the infant in flexed, contained midline posture with supportive boundaries. Minimise painful procedures, pair them where possible, and provide oral sucrose or breastmilk and non-nutritive sucking for procedural analgesia. [5]
When handling provokes autonomic instability, the response is to stop, contain, and reduce, not to push through. Pause the procedure. Bring the hands to the midline and contain the limbs. Lower the light and the noise. If instability persists, move to skin-to-skin contact, which reliably restores autonomic organisation. These are the resuscitative moves of developmental care, and they work within seconds to minutes. [6]
A parent in acute distress — panic, overwhelming tearfulness, dissociation — needs the same priority as an unstable infant: stay, calm, contain, and call for the mental-health and social-work support the unit should have on standby. Family-integrated care is built on parental presence, and parental presence is built on parental wellbeing. [4]
Management — Definitive & Stepwise
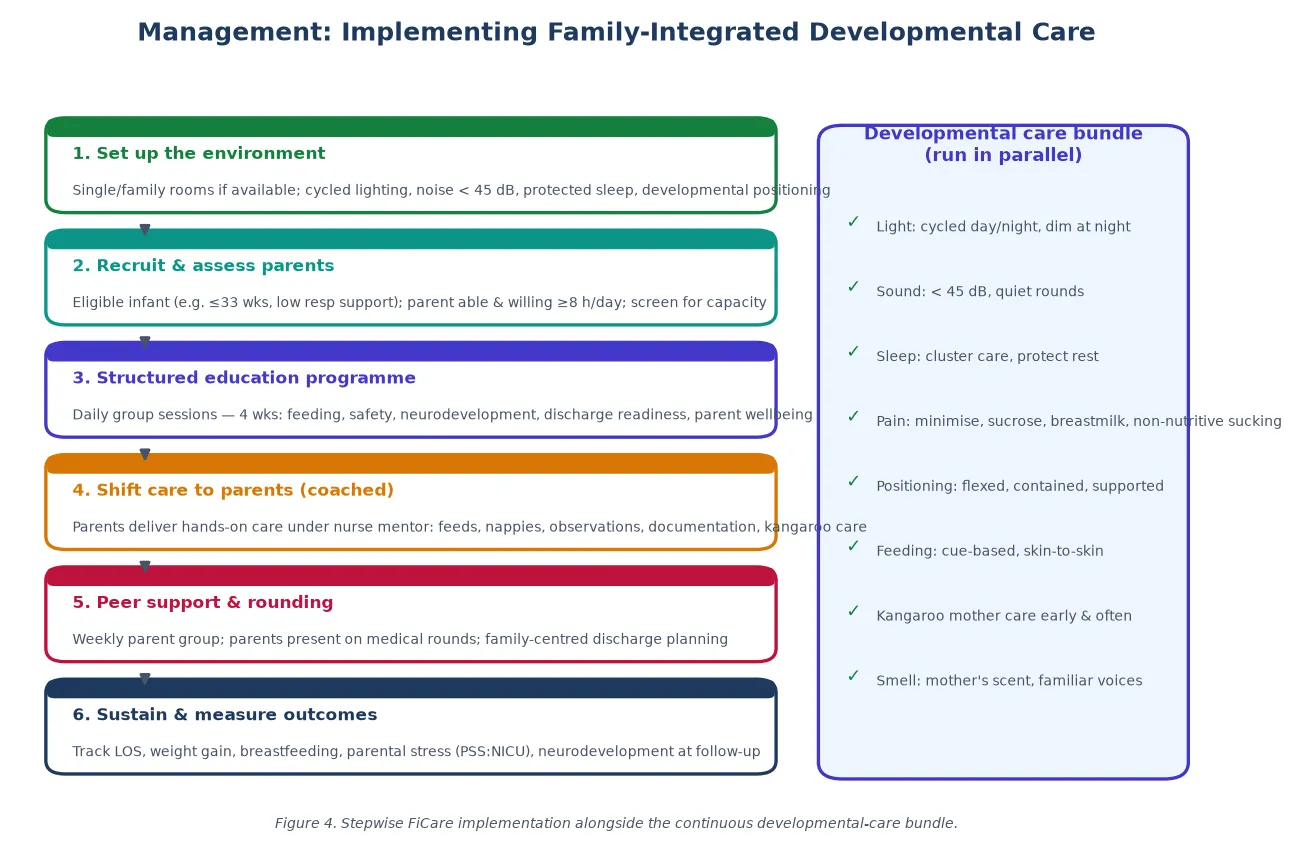
Definitive management is the full FiCare programme running in parallel with the continuous developmental care bundle. The bundle is the environmental and handling package described above; FiCare is the relational programme layered on top. Both run for the whole admission. [2]
The six steps of FiCare implementation
1. Set up the environment — single or family rooms, cycled lighting, noise < 45 dB, protected sleep, developmental positioning
2. Recruit and assess — confirm infant eligibility and parent willingness/capacity for ≥8 h/day presence
3. Structured education — daily group sessions over ~4 weeks covering feeding, safety, neurodevelopment, discharge, parent wellbeing
4. Shift care to parents (coached) — parents deliver feeds, nappies, observations, documentation, kangaroo care under nurse mentorship
5. Peer support and rounding — weekly parent group, parents present on medical rounds, family-centred discharge planning
6. Sustain and measure — track LOS, weight gain, exclusive breastmilk at discharge, parental stress, neurodevelopmental follow-up
The structured education programme is the engine. Parents attend daily sessions, usually over about four weeks, covering safe handling and feeding, recognising infant cues, neurodevelopment and brain protection, infection prevention, medication safety, resuscitation basics, discharge readiness, and parent mental health and wellbeing. Graduation is competency-based. The nurse's role pivots: instead of doing the care while the parent watches, the nurse supervises, teaches, and signs off as the parent takes over, then steps back. [1]
Parental presence is the non-negotiable core. In the O'Brien 2018 trial and the model programmes that followed, parents were present for at least eight hours a day, kept the infant's daily record, delivered oral and tube feeds, changed, settled, and monitored their infant, gave medications, and participated in rounds. The peer-support group — parents who have been through the programme supporting those starting — is one of the most consistently valued components and independently reduces parental isolation and stress. [2]
Kangaroo mother care (skin-to-skin)
Loading dose
Initiated as soon as mother and infant are stable; early, continuous contact preferred in low-birthweight infants
Maintenance dose
Sustained, prolonged or continuous skin-to-skin; aim for the longest daily duration achievable (many programmes target many hours per day)
Specific Subtypes & Scenarios
| Scenario | Adaptation | Evidence |
|---|---|---|
| FiCare in a level-II NICU | Shorter stays; condensed education; emphasis on family-centred care and early discharge readiness | Lehtonen 2020 international survey |
| FiCare with an extremely preterm or ventilated infant | Supported, modified parental involvement — presence and kangaroo care begin before full hands-on care | O'Brien 2018 included ≤33 weeks with low respiratory support |
| Surgical or cardiac NICU infant | Developmental care bundle and family partnership applied; care tailored to surgical constraints | Symington 2006 developmental care principles |
| Low-resource setting | Kangaroo mother care is the backbone — skin-to-skin, exclusive breastfeeding, early discharge with follow-up | Conde-Agudelo 2016 Cochrane |
| Single-family-room design | Reduces nosocomial infection and parental stress, but requires active family-care programming to avoid isolation | van Veenendaal 2020; Lehtonen 2020 |
| Parent unavailable (rural, out-of-home care, parental illness) | Accommodate absence; structured virtual involvement; named support person; avoid inequity-by-design | Programme-level adaptation |
Kangaroo mother care deserves its own emphasis because it is the most evidence-rich form of family-integrated care and the one most applicable globally. In low- and middle-income settings it is first-line for stable infants under 2500 g: continuous skin-to-skin contact, exclusive or nearly exclusive breastfeeding, and early discharge with close follow-up. The 2016 Cochrane review found it reduces mortality at discharge and at 6 to 12 months, and the meta-analysis of the same year confirmed reductions in sepsis, hypothermia, and length of stay. [6]
Single-family-room design is a frequent examiner trap. The architecture helps — it reduces noise, light, and nosocomial infection and lowers parental stress — but on its own it can isolate infants and has been associated in some studies with worse language and motor outcomes, because a baby alone in a quiet room receives less language exposure and handling. The lesson is that single rooms are an enabler of good developmental and family care, not a substitute for it. [8]
Complications & Pitfalls
Poorly implemented, the model can harm. Parents asked to be present eight hours a day without genuine support can burn out; the mother who is exhausted, isolated, and guilt-ridden is not a better caregiver. The programme that only resource-rich families can access widens the inequity it set out to close. Staff who treat parent involvement as free labour, or who keep clinical responsibility ambiguous, create conflict and documentation risk. And units that adopt the language of family-centred care without changing staffing ratios, culture, or the nurse's role are practising tokenism, not FiCare. [8]
The single-family-room pitfall, described above, is the best-studied example: architecture without activity can worsen outcomes. The countermeasure is to pair the room with active family-care programming so the infant is never alone and unstimulated for long. [9]
Prognosis & Disposition
The evidence base, though variable in quality, points consistently in the same direction. The O'Brien 2018 multicentre cluster randomised trial across 26 tertiary NICUs in Canada, Australia, and New Zealand found that FiCare improved weight gain — at day 21 the change in weight z-score was −0.07 in the FiCare group versus −0.16 in standard care (p<0.0002), with higher average daily weight gain — reduced parental stress and anxiety, and increased high-frequency exclusive breastmilk feeding at discharge. The Chinese cluster trial found that, after adjustment for clustering and confounders, FiCare was associated with shorter length of stay, lower medical expenditure, higher weight-gain velocity, and fewer nosocomial infections. The kangaroo-mother-care trials show mortality reduction in low-birthweight infants. [2]
O'Brien 2018 (Lancet Child Adolesc Health)
Multicentre, multinational, cluster-randomised controlled trial
Population: 26 tertiary NICUs in Canada, Australia, and New Zealand; infants ≤33 weeks' gestation on low respiratory support
Key finding
FiCare improved weight-gain z-score at day 21 (−0.07 vs −0.16, p<0.0002), reduced parental stress and anxiety, and increased exclusive breastmilk feeding at discharge
Practice change
The landmark trial establishing FiCare as an evidence-based model of neonatal care
Disposition is built into the model. Because the parent has been the primary caregiver for weeks, discharge is a continuation rather than a handover: the family leaves competent, confident, and already practised in feeding, settling, monitoring, and recognising problems. This is the mechanism by which FiCare is associated with reduced readmission and smoother community transition. Follow-up continues through standard preterm neurodevelopmental surveillance. [3]
Special Populations
In low- and middle-income settings, kangaroo mother care is the practical and evidence-based expression of family-integrated care, and it carries the strongest mortality evidence of any element of the model. The structured FiCare programme, built around prolonged in-hospital presence, is harder to deliver where distance, accommodation, and income are binding constraints, and adaptation rather than importation is the rule. [6]
For Indigenous families — Aboriginal and Torres Strait Islander, Māori, and First Nations — cultural safety is the precondition for family involvement. That means interpreter access, inclusion of extended family and elders, accommodation and travel support for remote families, and care that respects kinship and cultural practice. The same principles apply, with their own content, to migrant and refugee families, for whom language, health literacy, prior trauma, and housing instability are the barriers to participation. [8]
[8]Infants in out-of-home care, and those whose parents are themselves unwell, are the populations at greatest risk of missing out. A well-designed programme names a support person, builds virtual involvement where physical presence is impossible, and refuses to let the model become a privilege of the resourced. Adolescent parents benefit from the structure and peer support but need additional developmental and educational scaffolding. [4]
Evidence, Guidelines & Regional Differences
The Cochrane review of developmental care (Symington and Pinelli, 2006) found some benefits in growth and neurodevelopment at discharge but judged much of the evidence low quality, reflecting small trials and heterogeneity; its conclusion was that developmental care is widely practised with limited firm evidence rather than that it is ineffective. The kangaroo-mother-care Cochrane review (Conde-Agudelo and Díaz-Rossello, 2016) is stronger, showing reduced mortality and morbidity in low-birthweight infants, and it underpins WHO guidance. [5]
| Intervention | Best evidence | What it shows | Limits |
|---|---|---|---|
| FiCare (structured programme) | O'Brien 2018 cluster RCT; Hei 2021; Zhang 2024 | Improved weight gain, less parental stress, more exclusive breastmilk; adjusted shorter LOS | Cluster design; gestation/respiratory eligibility; LMIC adaptation |
| Developmental care bundle | Symington 2006 Cochrane | Some growth and neurodevelopment benefit | Low-quality, heterogeneous trials |
| Kangaroo mother care | Conde-Agudelo 2016 Cochrane; Boundy 2016 meta-analysis | Reduced mortality, sepsis, hypothermia in LBW infants | Strongest in stable LBW; LMIC settings |
| Single-family-room design | van Veenendaal 2020; Lehtonen 2020 | Less nosocomial infection, less parental stress; some motor/language concerns if isolated | Architecture enables, does not replace, care |
| Noise management | Sibrecht 2024 Cochrane | Sound-reduction strategies feasible; outcome evidence emerging | Few high-quality trials |
Current guidance converges across regions. In Australia and New Zealand, neonatal consensus statements and unit-level protocols endorse family partnership and the developmental care bundle, with explicit attention to equity. In the United Kingdom, BAPM and BLISS resources support family-integrated care, and NICE guidance covers the preterm infant. In the United States, the AAP endorses family-centred and developmental care, and single-family-room design is widespread. In Canada, FiCare originated and is embedded in many units. The strongest disagreement is not about whether to do this, but about how far the structured FiCare programme generalises beyond the trial population and how to fund the parental presence it requires. [2]
Exam Pearls
FiCare PARENTS
DEVELOPMENTAL BUNDLE
References
- [1]O'Brien K, Bracht M, Macdonell K, et al A pilot cohort analytic study of Family Integrated Care in a Canadian neonatal intensive care unit BMC Pregnancy Childbirth, 2013.PMID 23445639
- [2]O'Brien K, Robson K, Bracht M, et al Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: a multicentre, multinational, cluster-randomised controlled trial Lancet Child Adolesc Health, 2018.PMID 30169298
- [3]Hei M, Gao X, Li T, et al Family Integrated Care for Preterm Infants in China: A Cluster Randomized Controlled Trial J Pediatr, 2021.PMID 32898578
- [4]Zhang Y, Jiang M, Li T, et al Effect of family integrated care on stress in mothers of preterm infants: A multicenter cluster randomized controlled trial J Affect Disord, 2024.PMID 38232775
- [5]Symington A, Pinelli J Developmental care for promoting development and preventing morbidity in preterm infants Cochrane Database Syst Rev, 2006.PMID 16625548
- [6]Conde-Agudelo A, Díaz-Rossello JL Kangaroo mother care to reduce morbidity and mortality in low birthweight infants Cochrane Database Syst Rev, 2016.PMID 27552521
- [7]Boundy EO, Dastjerdi R, Spiegelman D, et al Kangaroo Mother Care and Neonatal Outcomes: A Meta-analysis Pediatrics, 2016.PMID 26702029
- [8]van Veenendaal NR, van Kempen AAMW, Dijkshoorn B, et al Hospitalising preterm infants in single family rooms versus open bay units: A systematic review and meta-analysis of impact on parents EClinicalMedicine, 2020.PMID 32548575
- [9]Lehtonen L, Hallman M, Andersson S, et al Family Rooms in Neonatal Intensive Care Units and Neonatal Outcomes: An International Survey and Linked Cohort Study J Pediatr, 2020.PMID 32525041
- [10]McAnulty G, Duffy FH, Butler S, et al Individualized developmental care for a large sample of very preterm infants: health, neurobehaviour and neurophysiology Acta Paediatr, 2009.PMID 19735497
- [11]Sibrecht G, Wróblewska-Seniuk K, van der Spek K, et al Noise or sound management in the neonatal intensive care unit for preterm or very low birth weight infants Cochrane Database Syst Rev, 2024.PMID 38813836