Paeds · fetal-neonatal-and-perinatal
Newborn examination and screening
Also known as Routine newborn check · Newborn infant physical examination · First newborn examination · NIPE · Newborn screening examination · 6-week baby check
Fellowship-level systematic newborn examination and universal newborn screening: head-to-toe assessment within 24-72 hours, the four targeted screens (pulse oximetry for critical congenital heart disease, red reflex for cataract and retinoblastoma, hearing screen, hip examination), New Ballard Score for gestational age, benign transitional findings versus pathology, escalation of abnormal findings, and ANZ/UK/US/Canada programme differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar is asked to "check the baby" before discharge. The parents are tired and anxious. This is one of the highest-yield examinations in paediatrics, because the serious findings — a duct-dependent heart, a cataract, a dislocatable hip — are easy to miss in a baby who looks completely well. [1]
The newborn examination (also called the routine infant check, the newborn infant physical examination, or NIPE in the UK) is a structured head-to-toe assessment carried out within the first 24 to 72 hours of life, before discharge home. It combines a full physical examination with the targeted universal screening tests. [19]
Two ideas sit behind it. First, a small number of conditions are treatable if found early and devastating if missed — the screening exists because they are silent at first. Second, most findings in a newborn are benign and transitional, so an important part of the job is recognising normal variants and reassuring parents well. [1]
Classification
Think of the examination as two overlapping layers — a full head-to-toe sweep, and the four universal screens woven through it. Keep them separate in your mind because each screen has its own pass-or-refer logic. [1] [19]
The two layers of the newborn examination
- Every region examined in sequence
- Catches dysmorphism, cleft palate, abdominal masses, spinal stigmata
- Documents what is normal, not just what is abnormal
- Repeated at the 6-week check
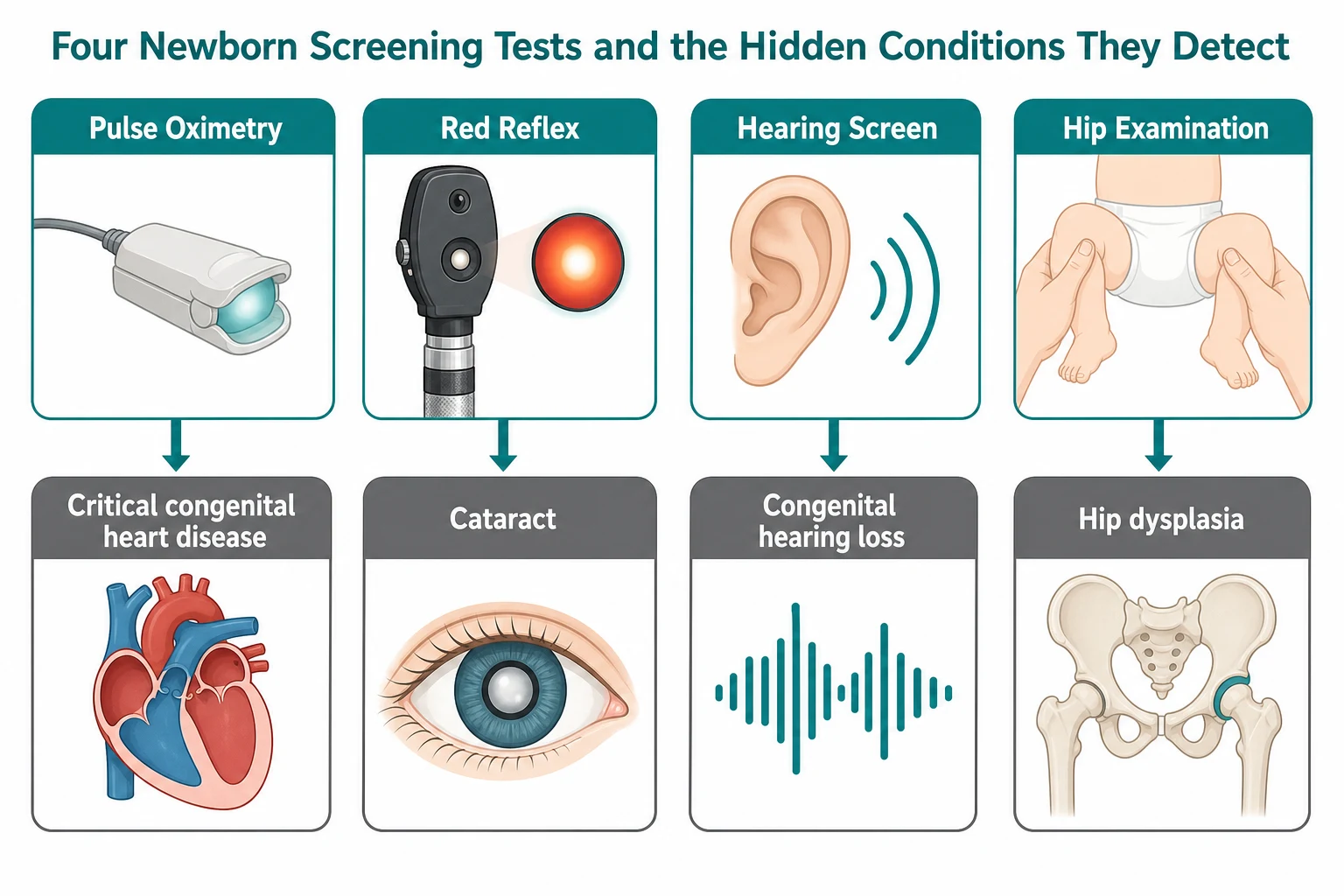
- Pulse oximetry → critical congenital heart disease
- Red reflex → cataract and retinoblastoma
- Hearing screen → congenital hearing loss
- Hip examination (Barlow/Ortolani) → DDH
The two layers catch different things. The sweep finds anatomical problems you can see or feel. The screens find physiological or functional problems that need an instrument or a manoeuvre to reveal. A normal sweep does not replace the screens, and a passed screen does not replace the sweep. [1] [19]
You will also separate universal screening (offered to every baby) from selective screening (offered to babies with risk factors). Universal pulse oximetry and hearing screening apply to all; selective hip ultrasound applies to breech babies and those with a family history regardless of a normal clinical exam. [5] [7]
Epidemiology & Risk Factors
The hidden conditions the examination hunts for are individually rare but, taken together, common enough that every clinician will encounter them. [1]
Risk factors move a baby from universal to selective screening. For the hips, breech presentation (especially after 36 weeks), a positive family history, foot deformities, and oligohydramnios all raise the risk of DDH and trigger a hip ultrasound even when the clinical exam is normal. [5] [7]
For hearing, a family history of childhood hearing loss, NICU admission over five days, some congenital infections, and craniofacial anomalies raise the risk and change the screening pathway toward automated auditory brainstem response testing. [8] [9]
Antenatal and intrapartum history sharpen the focus. Maternal diabetes raises the chance of cardiac and caudal anomalies. A history of polyhydramnios raises concern for obstruction. Instrumental or difficult delivery raises the chance of birth trauma. Always read the antenatal notes before you examine. [1]
Pathophysiology
Each of the four universal screens exploits a different piece of physiology. Understand the mechanism and you will not need to memorise the threshold. [1]
Duct-dependent circulation. Some cardiac lesions are survivable only while the ductus arteriosus stays open, shunting blood either to the lungs (right-sided lesions) or to the body (left-sided lesions). As the duct closes over the first days, the baby decompensates. Pulse oximetry detects the abnormal mixing or right-to-left shunting that appears before clinical collapse. [1] [2]
Red reflex. Light from the ophthalmoscope passes through the pupil, reflects off the retina, and returns as an orange-red glow. Anything that blocks the light path — a cataract in the lens, blood or a mass in the vitreous, a retinal tumour such as retinoblastoma — extinguishes or whitens the reflex. [11] [12]
Hip instability. In developmental dysplasia, the femoral head is shallowly seated in an immature acetabulum. In the newborn this instability is reducible — the head can be pushed out (Barlow) and levered back in (Ortolani) — which is why the manoeuvre works at all. Left untreated, the joint remodels abnormally and the reducible clunk is lost. [5] [6]
Benign transitional findings cause most parental anxiety and most over-investigation. Mongolian (dermal melanocytosis) spots, erythema toxicum, milia, vernix, sebaceous gland hyperplasia, breast tissue enlargement, and the withdrawal vaginal bleed are all normal physiological phenomena of the transition from fetal to extrauterine life. [19]
Clinical Presentation
Most newborns present as well, feeding, and normocoloured — the challenge is that serious disease hides inside that normal picture. Walk through what each region can reveal. [1]
The well baby has a normal examination at every region. You expect equal tone and movement, a pink colour (allowing mild acrocyanosis), a soft non-bulging fontanelle, a normal red reflex in both eyes, clear breath sounds, a soft abdomen, patent anus, and a stable, symmetrical hip exam. Knowing this normal baseline is what makes the abnormal stand out. [19]
The duct-dependent cardiac baby may look well but show subtle tachypnoea, a difference in oxygen saturation between the right hand and a foot, or weak or absent femoral pulses. None of these is dramatic on its own; together they are the warning that the duct is about to close. [1] [2]
The hip examination reveals a clunk on Barlow (a dislocatable head) or Ortolani (a relocatable head) — the physical sign that the joint is unstable. An isolated click is ligamentous and benign; a clunk is the finding that matters. Asymmetric skin folds and leg-length discrepancy are late signs that appear after the joint has remodeled. [5] [6]
The eye examination reveals a white pupil (leucocoria) or an absent, dull, or asymmetric red reflex. This is the sign that converts a routine check into an emergency referral. [11]
Distracting and benign findings — a sacral dimple within the gluteal cleft, a tongue-tie, a heart murmur in the first day, erythema toxicum — generate parental anxiety but are usually normal. The skill is sorting these from their dangerous mimics, which the differential section addresses. [15] [16]
Differential Diagnosis
For each common finding, hold the benign explanation and the dangerous mimic side by side. The discriminator is usually a single feature you can elicit at the bedside. [1]
Benign finding versus dangerous mimic
- Mongolian spot (dermal melanocytosis) vs bruising or grey-blue naevus
- Erythema toxicum vs staphylococcal pustulosis or herpes
- Milia vs miliaria or early infection
- Congenital cataract — opacity in the lens
- Retinoblastoma — white retinal mass
- Persistent fetal vasculature or Coats disease
- Transient tachypnoea of the newborn — self-limiting
- Early sepsis — risk factors and inflammatory markers
- Congenital heart disease — pulse oximetry and murmurs
- Respiratory distress syndrome — prematurity and surfactant
- Simple dimple within the gluteal cleft — benign
- Occult spinal dysraphism — above the cleft, hair tuft, lipoma, deviated gluteal fold
The red-flag red reflex is the highest-stakes discriminator. An absent, dull, or white reflex demands same-day ophthalmology. Retinoblastoma is life- and sight-threatening, and congenital cataract causes irreversible amblyopia if surgery is delayed, so the reflex is never "watched and repeated" — it is referred. [11] [12]
Distinguish a hip click from a hip clunk. A click is a high-pitched, ligamentous snap that is benign. A clunk is the palpable jerk of the femoral head exiting or re-entering the acetabulum — the positive finding for DDH. Confusing the two is the classic pitfall. [5] [6]
For a sacral dimple, the location is the discriminator. A simple dimple within or below the gluteal cleft, less than 5 mm deep, with no other stigmata, is benign. A dimple above the cleft, or one paired with a hair tuft, lipoma, haemangioma, tail, or deviated gluteal fold, suggests occult spinal dysraphism and warrants imaging. [15] [16]
Clinical & Bedside Assessment
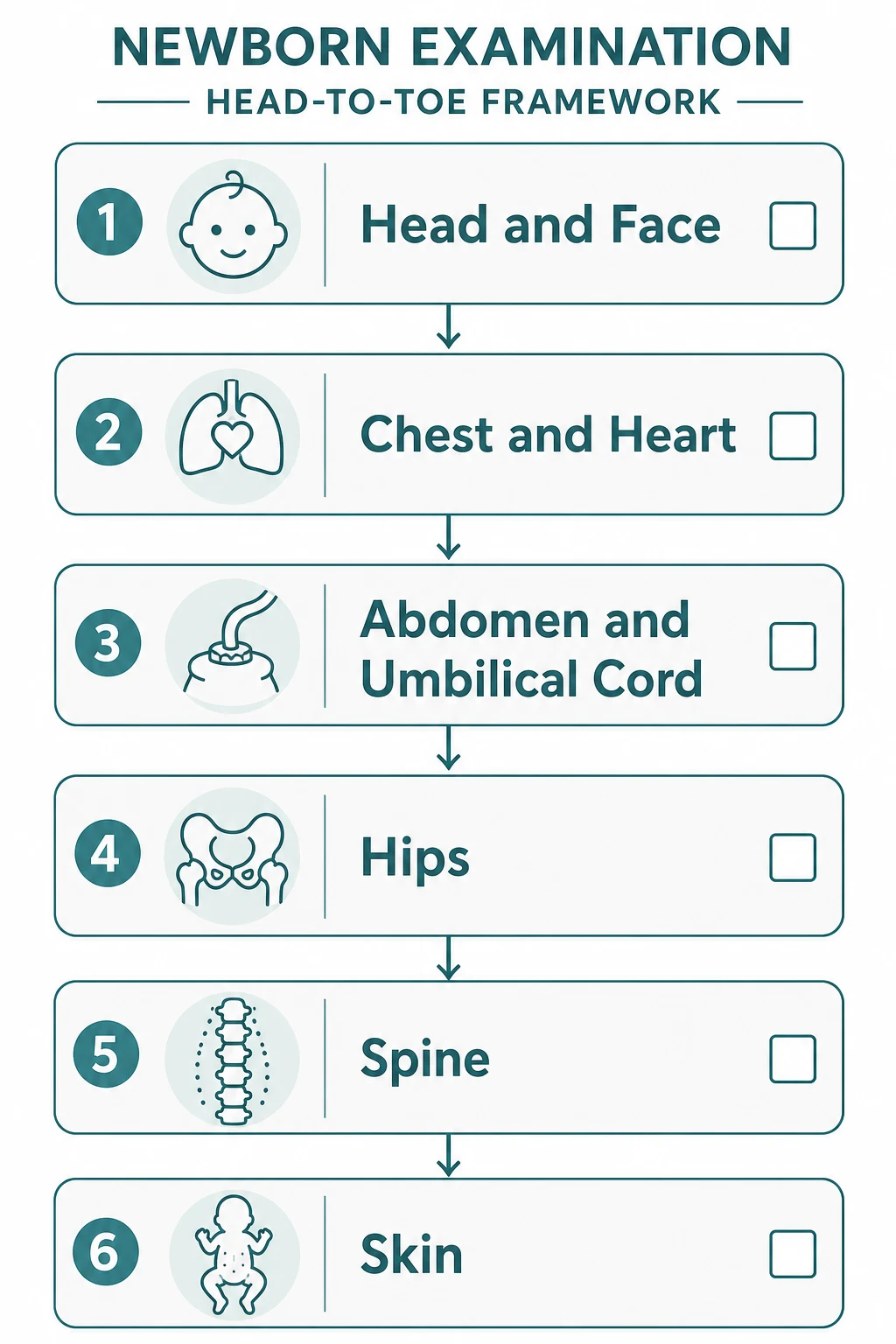
Examine warm, with the baby calm and the parent present. Observe first — colour, tone, posture, and any dysmorphism — then move head-to-toe, leaving the hips and the parts that upset the baby for last. A systematic order means you do not miss a region. [1]
Head and face. Feel the fontanelles (soft and flat), check the sutures, and assess moulding, caput succedaneum, and cephalohaematoma. Examine the face for dysmorphism. Look at the eyes and perform the red reflex. Inspect the ears and check the palate — visualise the entire palate including the posterior shelf, because a submucous cleft is easy to miss. [11] [19]
Chest and heart. Inspect for respiratory effort and inspect the precordium. Auscultate the heart for rate, rhythm, and murmurs, and feel the femoral pulses — absent or weak femorals suggest coarctation. Perform the pulse oximetry screen. [1] [3]
Abdomen and cord. Feel for masses, distension, and organomegaly. Inspect the umbilicus and cord (number of vessels — a single umbilical artery is a marker for other anomalies). Check the genitalia and confirm the anus is patent. [19]
Hips. With the baby supine and pelvis stabilised, perform Barlow (adduct and push posteriorly — a positive finding is the head dislocating out of the acetabulum) and Ortolani (abduct and lift — a positive finding is the head clunking back in). Record a clunk, not a click. [5] [6]
Spine and skin, then neurology. Inspect the spine for midline defects and sacral stigmata. Examine the skin for birthmarks, lesions, and signs of infection. Assess tone, posture, and primitive reflexes (Moro, grasp, suck) and check that limb movement is symmetrical — asymmetry suggests brachial plexus injury or a fracture. [15] [1]
Gestational age. Use the New Ballard Score to estimate gestational age from neuromuscular and physical maturity criteria. It is most reliable in the first 12 hours to 7 days and is essential when antenatal dating is uncertain or the baby is preterm. [4]
BALLARD
Investigations
The newborn examination is, mostly, an examination — but four universal and several selective investigations are woven through it. Know what each test detects and its pass-or-refer logic. [1]
Pulse oximetry screening. Measure oxygen saturation in the right hand (pre-ductal) and in a foot (post-ductal), after 24 hours of age. The screen is positive — and triggers echocardiography — if the saturation in either limb is under 90 per cent, if it is 90 to 94 per cent with a hand-to-foot difference over 3 per cent, or if a reading under 95 per cent persists on repeat. [1] [3]
The thresholds above are the widely adopted values derived from the AHA/AAP scientific statement and used across ANZ, the UK, the US, and Canada. Some programmes use a single post-ductal reading; many now measure both limbs. Always apply your local programme's exact rule, because the pass logic around the 90-94 per cent band differs slightly between countries. [1] [2]
Hearing screening. Two technologies are used: otoacoustic emissions (OAE), which test the cochlear outer hair cells, and automated auditory brainstem response (AABR), which tests the whole auditory pathway up to the brainstem. A "refer" result prompts a repeat, then a diagnostic audiological assessment. Well babies are usually screened with OAE; NICU and at-risk babies are screened with AABR. [8] [9]
Red reflex. Darken the room, hold the ophthalmoscope about 30 cm (an arm's length) from the baby, and shine at both eyes together. A normal reflex is a symmetric orange-red glow. An absent, white, dull, or asymmetric reflex is abnormal and warrants same-day ophthalmology. [11]
Selective hip imaging. A positive clinical exam (a clunk on Barlow or Ortolani) or a relevant risk factor (breech, family history) prompts a hip ultrasound using the Graf method, typically at around six weeks, though an obviously unstable hip at birth is referred earlier for orthopaedic assessment. [5] [7]
Newborn bloodspot screening. The heel-prick bloodspot card, taken around 48 to 72 hours, screens for a panel of conditions (such as hypothyroidism, sickle cell disease, cystic fibrosis, inborn errors of metabolism) depending on the country. It complements the physical examination and has its own recall pathway. [19]
Management — Resuscitation
A small number of findings are emergencies. Recognise them, stabilise, and escalate immediately. [1]
If the baby collapses or is shocked, follow the airway, breathing, circulation approach and call senior neonatal or paediatric help. Most newborn resuscitation is in supporting transition, but a baby who is blue, grunting, apnoeic, or floppy after birth needs active resuscitation and urgent review. [1]
A baby who looks septic — temperature instability, poor feeding, lethargy, respiratory distress — needs blood cultures and empirical antibiotics without delay. Neonatal sepsis is a clinical diagnosis made on risk factors and appearance, not on waiting for a fever. [1]
Bilious (green) vomiting is a surgical emergency. It implies malrotation with possible volvulus until proven otherwise. Make the baby nil-by-mouth, obtain urgent imaging, and refer to paediatric surgery. [19]
Management — Definitive & Stepwise
For most babies the examination is normal. The skill is the clean handover of a normal result, and the rapid, correct pathway for the few abnormal ones. [19]
Acting on the four universal screens
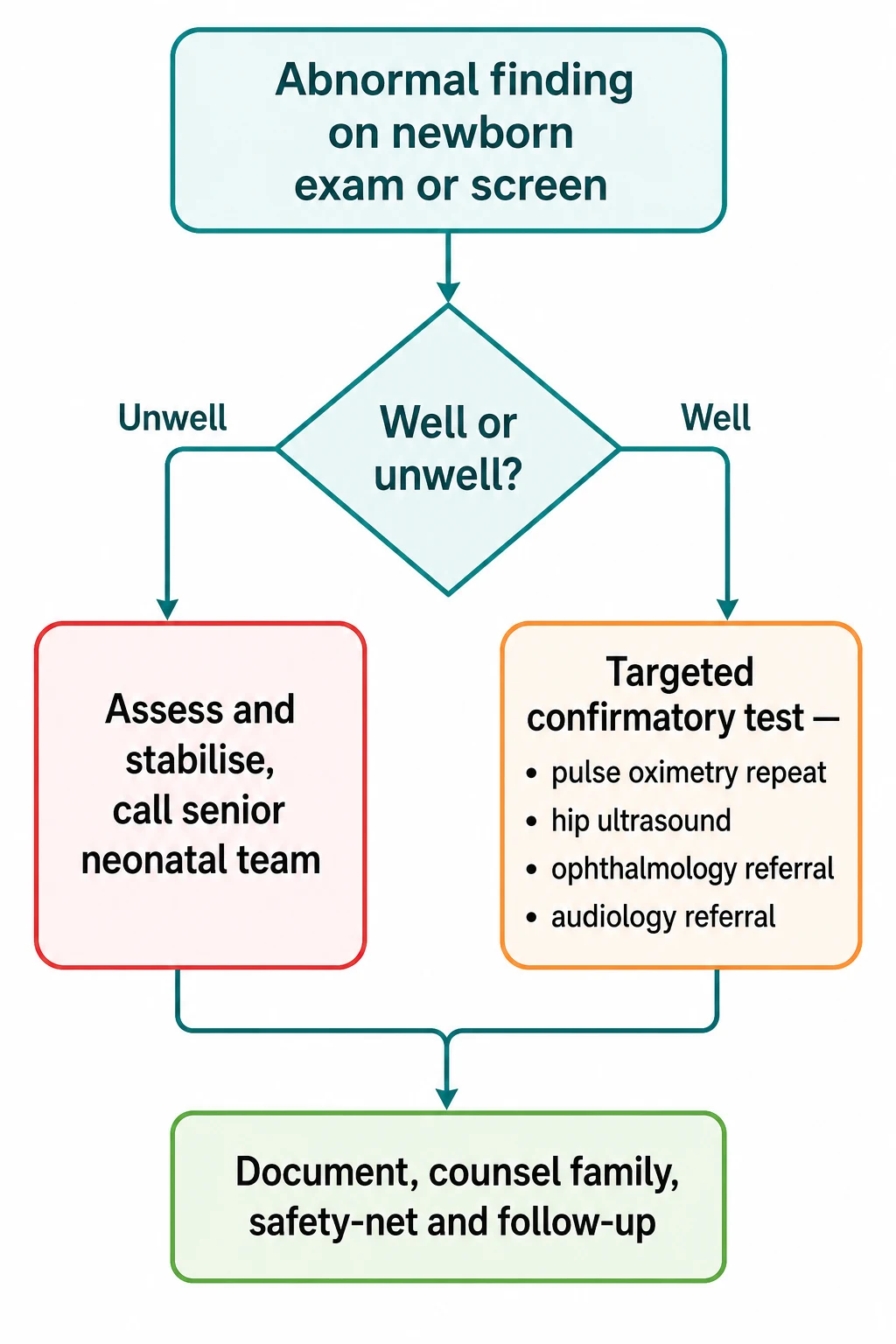
Normal examination and passed screens — document findings, reassure the parents, safety-net, and schedule the 6-week check.
Abnormal pulse oximetry — repeat the reading; if still positive, assess clinically and arrange echocardiography and cardiology referral for suspected duct-dependent disease.
Abnormal red reflex — same-day ophthalmology referral; never watch and wait, because cataract and retinoblastoma are time-critical.
Positive hip exam (clunk on Barlow or Ortolani) or risk factors — hip ultrasound at ~6 weeks and, for an unstable hip at birth, earlier orthopaedic referral; confirmed DDH is managed in a Pavlik harness.
Refer result on hearing screen — repeat, then diagnostic audiology assessment and, if confirmed, early intervention for hearing loss.
Suspicious midline or spinal finding — ultrasound and, if indicated, MRI, with neurosurgical referral.
The communication is part of the management. Explain the finding in plain language, name the next step and its timing, and give the parents written safety-net advice about when to return — poor feeding, colour change, breathing difficulty, or fever. A parent who understands the plan is the most reliable follow-up system there is. [19]
In Australia and Aotearoa New Zealand, newborn hearing screening is delivered through universal programmes (such as the Victorian Infant Hearing Screening Programme and the New Zealand Universal Newborn Hearing Screening and Early Intervention Programme). Pulse oximetry for critical congenital heart disease is recommended as an adjunct to the routine exam. Confirm current local protocols, because programme detail is set at the state or district level. [9]
Specific Subtypes & Scenarios
Each abnormal finding has its own pathway. Walk through the common ones a fellowship candidate must defend. [1]
The well term low-risk newborn has a normal examination. Document every region, complete the four screens, offer vitamin K and the first immunisations as appropriate, reassure the parents, and arrange routine follow-up. The danger here is complacency — perform every screen every time. [19]
The baby with a murmur or differential saturations is approached as possible duct-dependent disease until proven otherwise. A murmur alone is common and often innocent, but a murmur with low or differential saturations, weak femorals, or respiratory distress triggers echocardiography and, if duct-dependent, prostaglandins. [1] [2]
The baby with hip instability or risk factors gets a hip ultrasound at around six weeks; a clearly unstable hip at birth is referred immediately. Breech presentation and a positive family history are the risk factors that trigger imaging even with a normal exam. Confirmed DDH is managed in a Pavlik harness in the first months. [5] [7]
The white pupil (leucocoria) is retinoblastoma until proven otherwise. This is the finding where delay costs a life or an eye. Same-day ophthalmology, every time. [11]
The sacral dimple is sorted by location and associated stigmata. A simple dimple within or below the gluteal cleft is benign. A dimple above the cleft, or with a hair tuft, lipoma, or deviated fold, prompts spinal ultrasound and, if abnormal, MRI and neurosurgical referral. [15] [16]
The tongue-tie (ankyloglossia) affecting breastfeeding is assessed for both the frenulum appearance and the functional impact on latch. When a tongue-tie is causing genuine feeding difficulty and conservative support has not helped, frenotomy may help, but routine frenotomy for an isolated asymptomatic tie is not warranted. [13] [14]
The dysmorphic newborn or a congenital anomaly triggers a syndromic assessment — look for associated anomalies, review growth and the antenatal history, and refer for genetics evaluation. Multiple minor anomalies raise the probability of an underlying syndrome. [1]
The late-preterm or small-for-gestational-age newborn needs modified thresholds and closer surveillance — they are more likely to fail screening, become hypoglycaemic or hypothermic, and have feeding difficulty. Confirm gestational age with the New Ballard Score when dating is uncertain. [4]
Complications & Pitfalls
The errors are predictable. Knowing them is most of the defence. [1]
The classic miss is duct-dependent cardiac disease in a baby who looked well at discharge. A normal clinical examination does not exclude it — that is why pulse oximetry screening was introduced. Always complete the screen. [1] [2]
The classic hip error is confusing a click with a clunk, or accepting a single normal hip exam in a high-risk infant. A click is benign; a clunk is the finding. And risk factors (breech, family history) trigger imaging regardless of the exam. [5] [6]
Missing a submucous cleft palate happens when the posterior palate is not visualised. Run a finger along the full palate or look directly at the posterior shelf, because a submucous cleft is invisible on casual inspection and causes feeding and speech problems. [19]
Over-investigation of benign findings (a simple sacral dimple, a Mongolian spot, erythma toxicum) generates cost and parental anxiety without benefit. The counter-error — under-investigating a high-risk stigmata — is worse. Sort each finding by its discriminator. [15] [16]
Treating jaundice in the first 24 hours as physiological is a serious error. Jaundice within the first day is always pathological and demands a bilirubin level and a haemolysis work-up. [20]
Poor communication turns a normal variant into weeks of parental anxiety. Name the finding, explain that it is benign, and document the conversation. The red reflex, the hips, and the palate should all be repeated at the 6-week check, because new findings can emerge. [11] [19]
Prognosis & Disposition
Most newborns have a normal examination and pass every screen. They go home with their parents, primary-care follow-up, and a 6-week check booked. [19]
The conditions the screens hunt for have excellent outcomes when caught early. DDH treated in a Pavlik harness in the first months usually resolves without surgery. Congenital cataract removed early preserves vision. Congenital hearing loss identified and managed early allows near-normal language development. These are the reasons the screening exists. [5] [8]
Late presentation is where the harm sits. Duct-dependent cardiac disease that collapses before diagnosis carries significant mortality. Retinoblastoma diagnosed late threatens life and sight. Untreated DDH leads to early osteoarthritis. The screen buys the time that treatment needs. [1] [11]
The safety-net is the discharge contract. Parents must know to return for poor feeding, colour change, breathing difficulty, fever, or anything that worries them. A clear, written safety-net is part of the examination, not an afterthought. [19]
Special Populations
Several groups need a modified examination, different thresholds, or closer follow-up. [1]
Late-preterm and early-term infants (37 to 38 weeks) fail screening more often, become hypoglycaemic and hypothermic more readily, and feed less well. They need closer surveillance and sometimes a longer stay. [4]
Small-for-gestational-age and growth-restricted infants need extra attention to polycythaemia, hypoglycaemia, and the possibility of an underlying syndrome or congenital infection. Confirm gestational age, because size alone can mislead. [4]
Infants of diabetic mothers carry higher risks of cardiac anomalies, caudal regression, sacral agenesis, hypoglycaemia, and macrosomia with birth injury. Examine the heart, spine, and glucose with extra care. [1]
Newborns with antenatally diagnosed anomalies need targeted confirmation of the finding and counselling that starts before birth where possible. The examination confirms or refines what was seen on ultrasound. [19]
Migrant, refugee, asylum-seeker, and Indigenous families need culturally safe communication, interpreter access, and attention to screening access and follow-up continuity. Screening only works if the family can return. [8]
Out-of-hospital and home births need explicit attention to completing and documenting every screen, because these babies can slip through the screening net. [19]
Evidence, Guidelines & Regional Differences
The newborn examination rests on screening evidence and on national programmes that differ in detail. The principles are shared; the operational rules are local. [1]
The AHA and AAP scientific statement established pulse oximetry as a complement to the routine exam for detecting critical congenital heart disease, and a Cochrane review confirmed its sensitivity and specificity. This is the evidence base that moved pulse oximetry from selective to universal screening. [1] [2]
Plana et al. 2018 — Cochrane review
Population: Newborns undergoing pulse oximetry screening for critical congenital heart defects
Key finding
Pulse oximetry has high specificity and good sensitivity for critical congenital heart disease, with a low false-positive rate when performed after 24 hours of age.
Practice change
Pulse oximetry is now recommended as a universal adjunct to routine newborn examination across ANZ, the UK, the US, and Canada.
Universal newborn hearing screening rests on the Joint Committee on Infant Hearing principles and accumulated evidence that early identification and intervention improve language outcomes. The technology (OAE and AABR) and the risk-factor-based escalation to AABR are broadly shared. [8] [10]
Hip screening shows the clearest regional difference. The UK (NIPE) relies on clinical examination plus selective ultrasound for risk factors. Many European centres use universal ultrasound (the Graf method). The US relies on clinical exam with selective imaging. ANZ practice follows the selective-risk-factor model. [5] [7]
The controversies cluster around routine vitamin K and parental refusal, frenotomy for tongue-tie, and the imaging yield for simple sacral dimples. Each has evidence behind the conservative position: vitamin K prevents haemorrhagic disease; frenotomy helps symptomatic ties but not asymptomatic ones; and simple dimples within the gluteal cleft rarely need imaging. [13] [16] [17]
Exam Pearls
A fellowship candidate should carry a small set of one-liners that examiners reward. [1]
Examine the hips last — it is the most upsetting part and lets the baby settle for the cardiac and abdominal examination. [5]
A clunk, not a click, is the positive finding for DDH. Barlow dislocates a dislocatable hip; Ortolani relocates a dislocated hip. [5] [6]
A white pupil (leucocoria) is retinoblastoma until proven otherwise — same-day ophthalmology, no exceptions. [11]
Jaundice in the first 24 hours is always pathological. Measure the bilirubin and investigate haemolysis. [20]
Pulse oximetry screen: right hand plus a foot, after 24 hours. Positive if either is under 90 per cent, if 90 to 94 per cent with a hand-to-foot difference over 3 per cent, or if under 95 per cent persists on repeat. [1]
Visualise the entire palate, including the posterior shelf, to exclude a submucous cleft. [19]
Breech presentation and family history are the key DDH risk factors that trigger hip ultrasound regardless of a normal exam. [5] [7]
The New Ballard Score combines neuromuscular and physical maturity criteria and is reliable from the first 12 hours to 7 days. [4]
References
- [1]Mahle WT Role of pulse oximetry in examining newborns for congenital heart disease: a scientific statement from the AHA and AAP. Pediatrics, 2009.PMID 19581259
- [2]Plana MN Pulse oximetry screening for critical congenital heart defects. The Cochrane database of systematic reviews, 2018.PMID 29494750
- [3]Kemper AR Strategies for implementing screening for critical congenital heart disease. Pediatrics, 2011.PMID 21987707
- [4]Ballard JL New Ballard Score, expanded to include extremely premature infants. The Journal of pediatrics, 1991.PMID 1880657
- [5]Zhang S Developmental dysplasia of the hip. British journal of hospital medicine (London, England : 2005), 2020.PMID 32730146
- [6]Maikku M The Ortolani test has a high positive predictive value in clinical hip screening for developmental dysplasia of the hip. Acta paediatrica (Oslo, Norway : 1992), 2023.PMID 36928888
- [7]Kolovos S Ultrasonographic screening for developmental dysplasia of the hip: the Graf method revisited. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie, 2024.PMID 37884843
- [8]Wrightson AS Universal newborn hearing screening. American family physician, 2007.PMID 17508530
- [9]Wroblewska-Seniuk KE Universal newborn hearing screening: methods and results, obstacles, and benefits. Pediatric research, 2017.PMID 27861465
- [10]Thompson DC Universal newborn hearing screening: summary of evidence. JAMA, 2001.PMID 11667937
- [11]Cagini C Red reflex examination in neonates: evaluation of 3 years of screening. International ophthalmology, 2017.PMID 27822637
- [12]Duret A The infrared reflex: a potential new method for congenital cataract screening. Eye (London, England), 2019.PMID 31267092
- [13]Bruney TL Systematic review of the evidence for resolution of common breastfeeding problems-Ankyloglossia (Tongue Tie). Acta paediatrica (Oslo, Norway : 1992), 2022.PMID 35150472
- [14]O'Shea JE Frenotomy for tongue-tie in newborn infants. The Cochrane database of systematic reviews, 2017.PMID 28284020
- [15]Kucera JN The simple sacral dimple: diagnostic yield of ultrasound in neonates. Pediatric radiology, 2015.PMID 24996813
- [16]Albert GW Spine ultrasounds should not be routinely performed for patients with simple sacral dimples. Acta paediatrica (Oslo, Norway : 1992), 2016.PMID 27059606
- [17]Jullien S Vitamin K prophylaxis in newborns. BMC pediatrics, 2021.PMID 34496783
- [18]Sankar MJ Vitamin K prophylaxis for prevention of vitamin K deficiency bleeding: a systematic review. Journal of perinatology : official journal of the California Perinatal Association, 2016.PMID 27109090
- [19]Townsend J Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers. Health technology assessment (Winchester, England), 2004.PMID 15038906
- [20]Par EJ Neonatal Hyperbilirubinemia: Evaluation and Treatment. American family physician, 2023.PMID 37192079