Paeds · gastroenterology-hepatology-and-nutrition
Paediatric feeding disorder: nutritional and gastrointestinal management
Also known as Paediatric feeding disorder · PFD · Feeding disorder of childhood · Oral intake dysfunction in children · Food refusal and faltering growth · Feeding difficulty nutritional management
Fellowship guide to paediatric feeding disorder and its nutritional and gastrointestinal management: the child whose oral intake is impaired across the four domains of medical, nutritional, feeding skill and psychosocial dysfunction; the Goday consensus definition built on the WHO ICF framework; prevalence of around one in thirty-seven children under five; the PFD-versus-ARFID distinction between an organ-based feeding disorder and a DSM-5 psychiatric eating disorder; the gastrointestinal drivers of reflux, constipation and eosinophilic oesophagitis; the stepped multidisciplinary plan from medical optimisation and behavioural intervention to oral nutritional support and enteral feeding; the intensive multidisciplinary program evidence; tube dependency and weaning; and the ESPGHAN gastrostomy guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the two-year-old who screams and turns away at the sight of lumps, the former premature infant who never learned to feed by mouth and is still tube-dependent at eighteen months, and the child with cerebral palsy whose reflux was poorly controlled and who now refuses every food he once enjoyed. These children do not have separate problems; they have a paediatric feeding disorder, a condition in which oral intake is impaired in a way that harms nutrition, growth, safety or the mealtime relationship, and the clinician's job is to work out which of the four domains is driving the failure and to treat all of them together. [1] [4]
For decades, feeding problems in children were described through the lens of whichever professional saw the child, so a speech-language therapist, a dietitian and a psychologist each labelled a different slice of the same child. The 2019 consensus paper by Goday and colleagues fixed this by proposing a single unifying term, paediatric feeding disorder, built on the World Health Organization International Classification of Functioning, Disability and Health framework. The definition is precise: paediatric feeding disorder is impaired oral intake that is not age-appropriate and is associated with medical, nutritional, feeding skill and/or psychosocial dysfunction. The word "and/or" is the key, because most real children have dysfunction in more than one domain, and a plan that treats only one is the commonest reason treatment fails. [1] [3]
This leaf owns the nutritional and gastrointestinal management of paediatric feeding disorder. It sits beside the dedicated leaf on feeding assessment and paediatric dysphagia, which owns the swallow study and the penetration-aspiration scale; here the focus is on the medical and nutritional drivers, the gastrointestinal conditions that trigger and sustain feeding difficulty, and the stepped multidisciplinary plan that runs from treating the gut through behavioural intervention to oral nutritional support and enteral feeding. The ARFID distinction runs through the whole topic, because every examiner wants to know whether the child in front of them has an organ-based feeding disorder or a psychiatric eating disorder. [1] [9]
Classification
The most useful way to hold paediatric feeding disorder is through its four domains, because each domain points to a different assessor and a different treatment lever, and a child almost always has more than one affected. The medical domain covers impaired oral intake driven by an underlying condition, most often gastro-oesophageal reflux, constipation, eosinophilic oesophagitis or food allergy, but also cardiopulmonary disease, prematurity and anatomical airway problems. The nutritional domain covers an imbalance of intake, absorption or metabolism, presenting as faltering growth, a specific nutrient deficiency, or dependency on enteral feeds. The feeding-skill domain covers dysfunction of the oral, pharyngeal or oesophageal phases of swallowing, from immature suck-swallow-breathe to aspiration. The psychosocial domain covers disruption of the feeding relationship and mealtime behaviour, from conditioned food aversion to caregiver distress and family dysfunction. [1] [3]
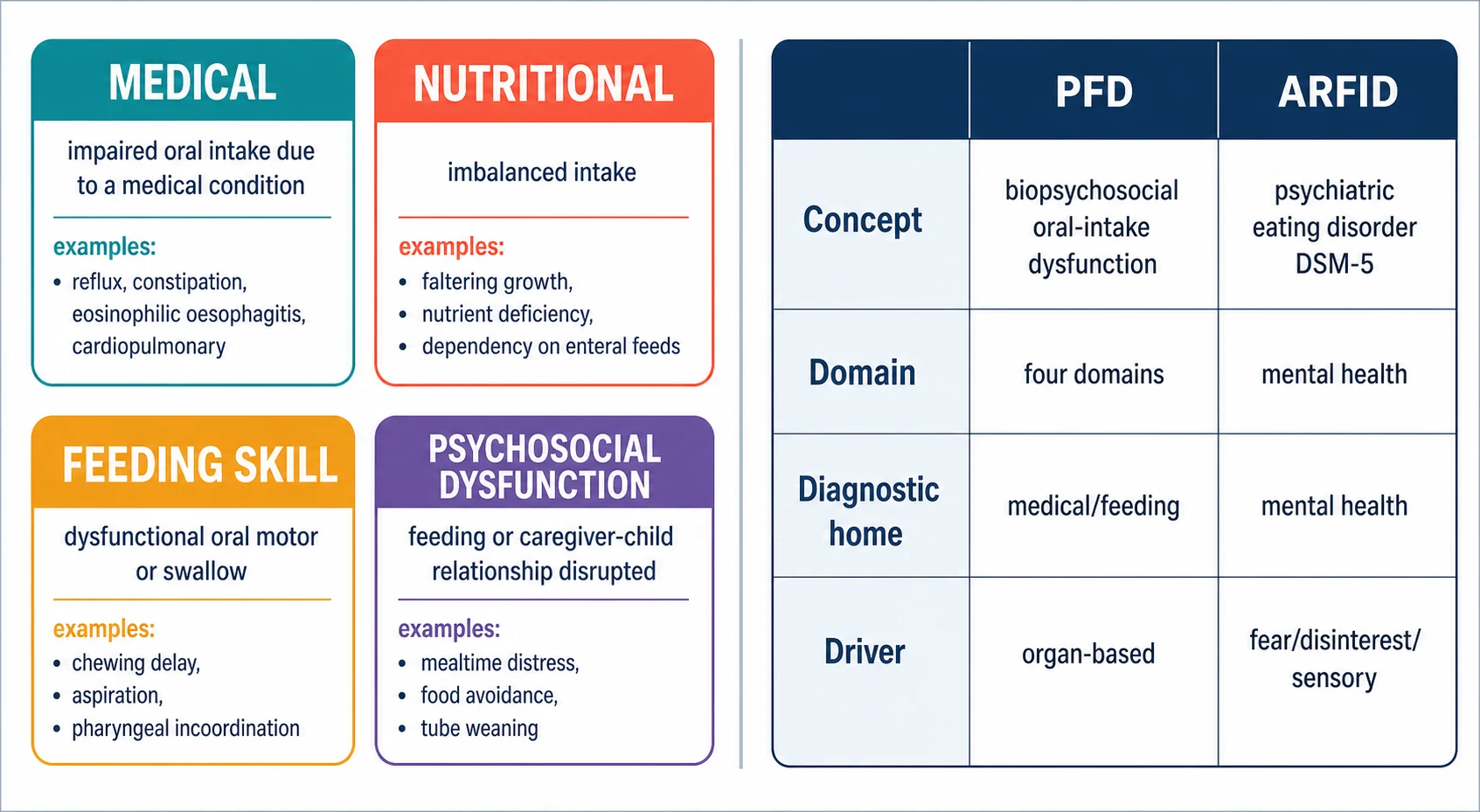
The second classification the examiner expects is the distinction between paediatric feeding disorder and avoidant/restrictive food intake disorder, because they overlap in presentation but differ in diagnostic home and management. Paediatric feeding disorder is an organ-based, biopsychosocial condition defined by the consensus framework, owned by paediatrics and feeding teams, and driven by medical, nutritional, feeding-skill and psychosocial factors. Avoidant/restrictive food intake disorder is a DSM-5 psychiatric eating disorder defined by a persistent failure to meet nutritional needs driven by lack of interest, sensory-based avoidance, or fear of aversive consequences, in the absence of a primary medical cause. The two can coexist, and a child with eosinophilic oesophagitis may develop a genuine ARFID-pattern sensory avoidance, so the assessment asks which came first and what is sustaining the restriction now. [1] [9]
[1] [9]Epidemiology & Risk Factors
Feeding problems are among the commonest concerns brought to a general paediatric clinic, but the consensus definition allows them to be quantified. In a United States nationwide prevalence study using public and private insurance databases, the annual prevalence of paediatric feeding disorder in 2014 was around one in thirty-seven children under five in the privately insured cohort and as high as one in twenty-three in the publicly insured cohort, and the prevalence rose significantly over the study period. That places feeding disorder on a par with conditions such as eating disorders and autism, which is why the study concluded it rivals commonly diagnosed conditions in children. [2]
The risk of paediatric feeding disorder is not spread evenly. It clusters in children with medical complexity, neurodisability and developmental difference. The child with cerebral palsy carries the heaviest burden, with oropharyngeal dysphagia, reflux, constipation and mealtime distress conspiring together, and feeding difficulty is a recognised contributor to faltering growth and reduced survival in the most severely affected. The premature and low-birthweight infant who is established on tube feeds in the neonatal unit is at high risk of tube dependency if oral feeding is not actively progressed. Children with autism spectrum disorder and sensory processing differences present with food selectivity and sensory-based restriction, and children with allergic or eosinophilic gastrointestinal disease develop conditioned food aversion after painful or uncomfortable feeding. [4] [11]
Pathophysiology
Paediatric feeding disorder is best understood as a causal loop rather than a single lesion, because medical, oral-motor, sensory and behavioural factors feed one another and a child can be drawn into the loop through any one of them. A medical driver such as reflux makes feeding painful, so the child learns to refuse; the refusal narrows the diet, which worsens nutrition and oromotor skill; the weakened oromotor skill makes solids harder, which deepens the sensory aversion; and the distressed mealtimes strain the caregiver-child relationship, which in turn reinforces refusal. Breaking the loop means intervening on more than one domain at once. [1] [4]
The gastrointestinal drivers are the focus of this leaf because they are common, treatable, and frequently unrecognised as the root cause. Uncontrolled gastro-oesophageal reflux inflames the oesophagus and conditions the child to associate feeding with pain, producing food refusal that persists even after the reflux is treated unless the behavioural layer is addressed. Constipation reduces appetite through early satiety and abdominal discomfort, and the child who is backed up will often eat poorly until the bowel is cleared. Eosinophilic oesophagitis produces dysphagia, food impaction and feeding aversion, and food allergy can drive enterocolitis or enteropathy that makes feeding uncomfortable or unsafe. Treating these drivers is the first lever in the nutritional and gastrointestinal management of paediatric feeding disorder. [4] [12]
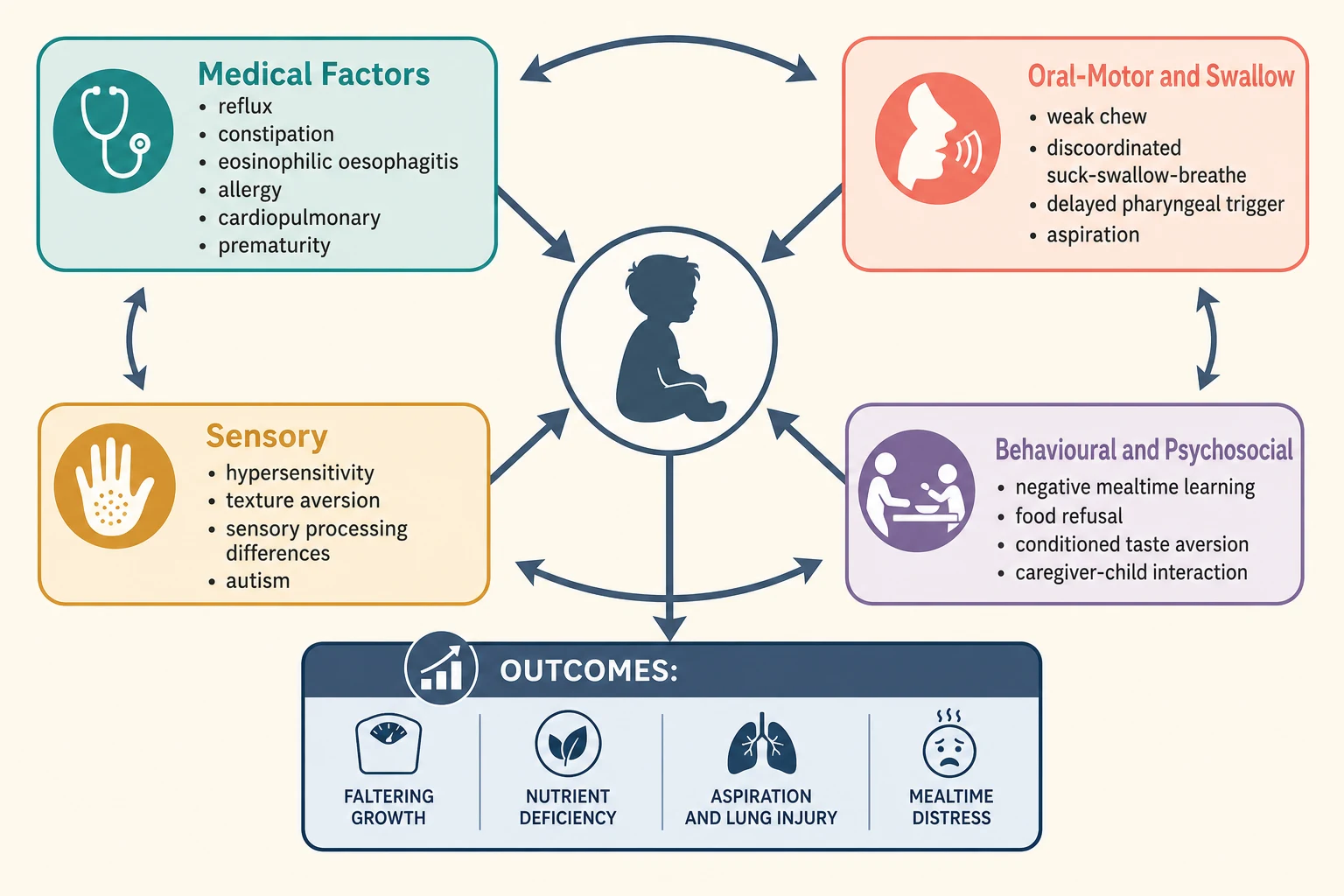
The behavioural and developmental layer explains why the problem persists after the medical driver is removed. A child who has been tube-fed learns that hunger is relieved without oral intake, so the motivation to eat by mouth falls away, and the longer the tube stays the harder the weaning becomes. A child who has experienced painful reflux or repeated choking develops a conditioned taste aversion to the foods that were associated with the discomfort, and this aversion does not extinguish on its own. The sensory-averse child, often with autism or sensory processing differences, restricts the diet to a narrow set of accepted textures and colours, and the resulting narrow intake both compromises nutrition and prevents the oromotor practice that would build skill. [4] [10]
Clinical Presentation
The child with paediatric feeding disorder presents through one of several doors, and recognising which door the family came through shapes the assessment. The first is the growth chart, with weight or length falling across centiles and the feeding difficulty identified only when someone plots and asks. The second is the mealtime itself, with food refusal, extreme selectivity, mealtimes lasting over thirty to forty minutes, distress, gagging, or a child who will eat only a tiny range of branded foods of a specific texture. The third is the gut, with reflux, constipation, vomiting or dysphagia pointing to a medical driver. The fourth is the developmental or behavioural presentation, with the autistic child who restricts to a narrow diet or the tube-dependent child who will not transition to oral feeding. [1] [4]
The infant adds a specific set of presentations. The former premature infant who was tube-fed in the neonatal unit may fail to establish oral feeding because the suck-swallow-breathe pattern never matured, and the longer the tube remains the more entrenched the dependency. An infant with reflux may arch, cry and refuse feeds, and an infant with a cow's-milk-protein allergy may present with vomiting, irritability and food refusal that resolves only with dietary change. The recognition move is to ask, in any infant whose intake is poor or whose growth is faltering, whether a medical driver is making feeding uncomfortable or unsafe before labelling the refusal behavioural. [6] [4]
The older neurologically impaired child often presents through the lung or the growth chart rather than an explicit feeding complaint. Reflux, constipation and dysphagia coexist, the diet has narrowed to smooth textures, mealtimes are long and distressing for the family, and the child may be partly or wholly tube-dependent. A qualitative systematic review of caregivers' experiences found that feeding a child with cerebral palsy places a heavy and persistent burden on families, with mealtimes dominating family life and carer stress high, which is why the psychosocial domain is assessed alongside the medical and nutritional ones. [11] [4]
[1] [11]Differential Diagnosis
The differential for the child with feeding difficulty is broad, and the four-domain framework is what keeps it organised. For the child presenting through the gut, the medical differential includes gastro-oesophageal reflux disease, eosinophilic oesophagitis, food allergy such as cow's-milk-protein allergy and non-IgE-mediated enterocolitis or enteropathy, Helicobacter pylori, anatomical causes such as malrotation, and systemic conditions such as coeliac disease or inflammatory bowel disease. The discriminator is the temporal pattern: reflux and dysphagia are meal-related, eosinophilic oesophagitis produces solid-food dysphagia and impaction, and allergic enteropathy is accompanied by other allergic features and responds to dietary elimination. [4] [12]
For the child presenting through growth, the differential spans inadequate intake, malabsorption, increased requirement and increased losses, and paediatric feeding disorder sits firmly in the inadequate-intake arm. The discriminator that points to a feeding disorder rather than an organic cause of malabsorption is the mealtime history: the intake is limited by refusal, selectivity, distress or tube dependency rather than by appetite loss, vomiting or diarrhoea. The must-not-miss trap is attributing faltering growth to neglect or behavioural food refusal while a treatable medical driver such as eosinophilic oesophagitis, reflux or constipation goes unaddressed. [1] [4]
For the child presenting through behaviour, the central differential is avoidant/restrictive food intake disorder. The features that should pull the diagnosis toward ARFID rather than paediatric feeding disorder are the absence of an identifiable medical, nutritional or feeding-skill driver, restriction driven by lack of interest, sensory-based avoidance or fear of aversive consequences, and significant weight loss or nutritional compromise meeting DSM-5 criteria. The two are not mutually exclusive, and a child may have both an organ-based feeding disorder and a superimposed ARFID-pattern restriction, so the assessment asks what is primary and what is sustaining the restriction now. [9] [1]
The four domains of paediatric feeding disorder, FEED mnemonic
Clinical & Bedside Assessment
Assessment begins with the growth chart, the diet history and the mealtime history, because these three alone place the child in the right domain. Plot the weight, length and head circumference on age-appropriate charts and look for faltering growth or a fall across centiles. Take a detailed diet history: what the child eats and drinks, the range of accepted foods, the textures tolerated, the volume and duration of meals, and whether the child is reliant on oral nutritional supplements or enteral feeds. Ask about mealtime behaviour: refusal, distress, gagging, the time a meal takes, and the impact on the family. A validated tool such as the Behavioural Pediatric Feeding Assessment Scale helps structure this. [1] [3]
The medical assessment then asks whether a gastrointestinal driver is present, because that is the first treatment lever in this leaf. Ask about reflux symptoms such as vomiting, regurgitation, arching and discomfort with feeds; about constipation, which is often under-recognised and suppresses appetite; about dysphagia, food impaction or pain on swallowing, which point to eosinophilic oesophagitis; and about allergic features such as eczema, blood in the stool or irritability in the infant. Examine for the stigmata of the underlying condition, including tone and posture in cerebral palsy, abdominal distension and palpable faeces in constipation, and the oromotor and swallow status that belongs to the feeding-skill domain. [4] [12]
The feeding-skill assessment, led by the speech-language therapist, determines whether aspiration risk is present, because that changes the safety of any oral-feeding plan. This leaf links to the dedicated dysphagia assessment leaf for the videofluoroscopic swallow study and fibreoptic endoscopic evaluation of swallowing, but the principle stands: a child with coughing, choking, a wet voice or recurrent pneumonia needs instrumental swallow assessment before oral intake is pushed, and the bedside evaluation alone cannot exclude silent aspiration. The psychosocial assessment, often led by psychology, evaluates the mealtime interaction, the presence of conditioned aversion, and the carer burden that a qualitative review has shown to be substantial in families of children with cerebral palsy. [11] [3]
Investigations
Investigation in paediatric feeding disorder is directed by the domain that is compromised, and the goal is to find and stage the treatable drivers rather than to run a blanket panel. For the nutritional domain, the baseline workup includes a full blood count and ferritin to detect iron deficiency, a micronutrient screen where intake is narrow, and a review of growth trajectories over time. Where intake is severely limited or the diet is extremely selective, a broader screen for fat-soluble vitamins, zinc and bone health is warranted, calibrated to the individual child. [4] [1]
For the medical domain, the gastrointestinal workup is the focus. Reflux is usually assessed clinically, but where it is severe or atypical a pH or impedance study or an upper endoscopy may be indicated. Eosinophilic oesophagitis is diagnosed by upper endoscopy with biopsy showing fifteen or more intraepithelial eosinophils per high-power field, and it should be suspected in any child with solid-food dysphagia, food impaction or persistent feeding aversion. Food allergy is assessed with a careful history and, where indicated, elimination and rechallenge, guided by an allergy specialist rather than blanket testing, because indiscriminate food panels can deepen dietary restriction. Constipation is a clinical diagnosis, and an abdominal X-ray is not required to confirm it. [4] [12]
For the feeding-skill domain, the instrumental swallow assessment is the key investigation and is detailed in the dedicated dysphagia leaf. For the psychosocial domain, structured questionnaires and a clinical psychology assessment characterise the behavioural pattern and the mealtime interaction. The case report form proposed by the consensus framework is the tool that pulls these together, prompting characterisation across all four domains so that no driver is missed and the treatment plan is genuinely multidisciplinary. [3] [1]
When to refer for upper endoscopy in feeding disorder
Refer a child with feeding disorder for upper endoscopy with biopsy when there is solid-food dysphagia, food impaction, persistent feeding aversion despite medical treatment of reflux, evidence of mucosal disease such as vomiting or blood in the stool, or faltering growth that is not explained by intake alone. The goal is to detect eosinophilic oesophagitis, which requires fifteen or more intraepithelial eosinophils per high-power field on biopsy, and other mucosal pathology that may be driving the feeding difficulty. Endoscopy is not a first-line test for every child with feeding difficulty, but it is the arbiter for the medical driver when reflux treatment has failed. [4] [12]
Management — Resuscitation
Most paediatric feeding disorder is managed electively, but a small number of children present acutely unwell from the consequences of the disorder and need immediate stabilisation. The severely malnourished child with faltering growth or dehydration needs safe nutrition and hydration established without delay, and where the swallow is unsafe or intake impossible this means nasogastric feeding while the assessment proceeds. The key safety principle is refeeding awareness: a severely malnourished child started on nutrition is at risk of refeeding syndrome with hypophosphataemia, hypokalaemia and hypomagnesaemia, so electrolytes are checked and corrected, thiamine is given, and feeding is started at a conservative rate and advanced under monitoring. [1] [10]
The child who aspirates and develops pneumonia needs the pneumonia treated as well as the feed made safe. Assess the work of breathing, give oxygen and respiratory support as needed, and treat the infection with antibiotics guided by severity and local policy. The pivotal step is to stop the ongoing aspiration, which means pausing or modifying oral feeding until an instrumental swallow study defines what is safe, because treating the pneumonia without fixing the swallow and the underlying feeding disorder guarantees recurrence. [11] [3]
The child who presents with an acute medical driver such as severe eosinophilic oesophagitis, an allergic enteropathy, or severe constipation may need that condition treated before feeding can improve. Acute constipation is cleared, reflux is optimised, and allergic disease is managed with dietary elimination under supervision. The resuscitation phase is a bridge to the definitive multidisciplinary feeding plan, and its goal is to stabilise the airway, the hydration and the medical driver while the four-domain assessment is completed. [4] [12]
Immediate management of the acutely unwell child with feeding disorder
Stabilise the airway and treat aspiration pneumonia with oxygen, respiratory support and antibiotics guided by local policy
Pause or modify oral feeding until an instrumental swallow study confirms what is safe
Establish safe hydration and nutrition by nasogastric tube where intake is unsafe or impossible
Check and correct phosphate, potassium and magnesium before and during nutrition in the severely malnourished child, give thiamine, and start feeding at a conservative rate to avoid refeeding syndrome
Treat the acute medical driver: clear constipation, optimise reflux, manage allergic or eosinophilic disease
Complete the four-domain assessment and build the definitive multidisciplinary feeding plan
Management — Definitive & Stepwise
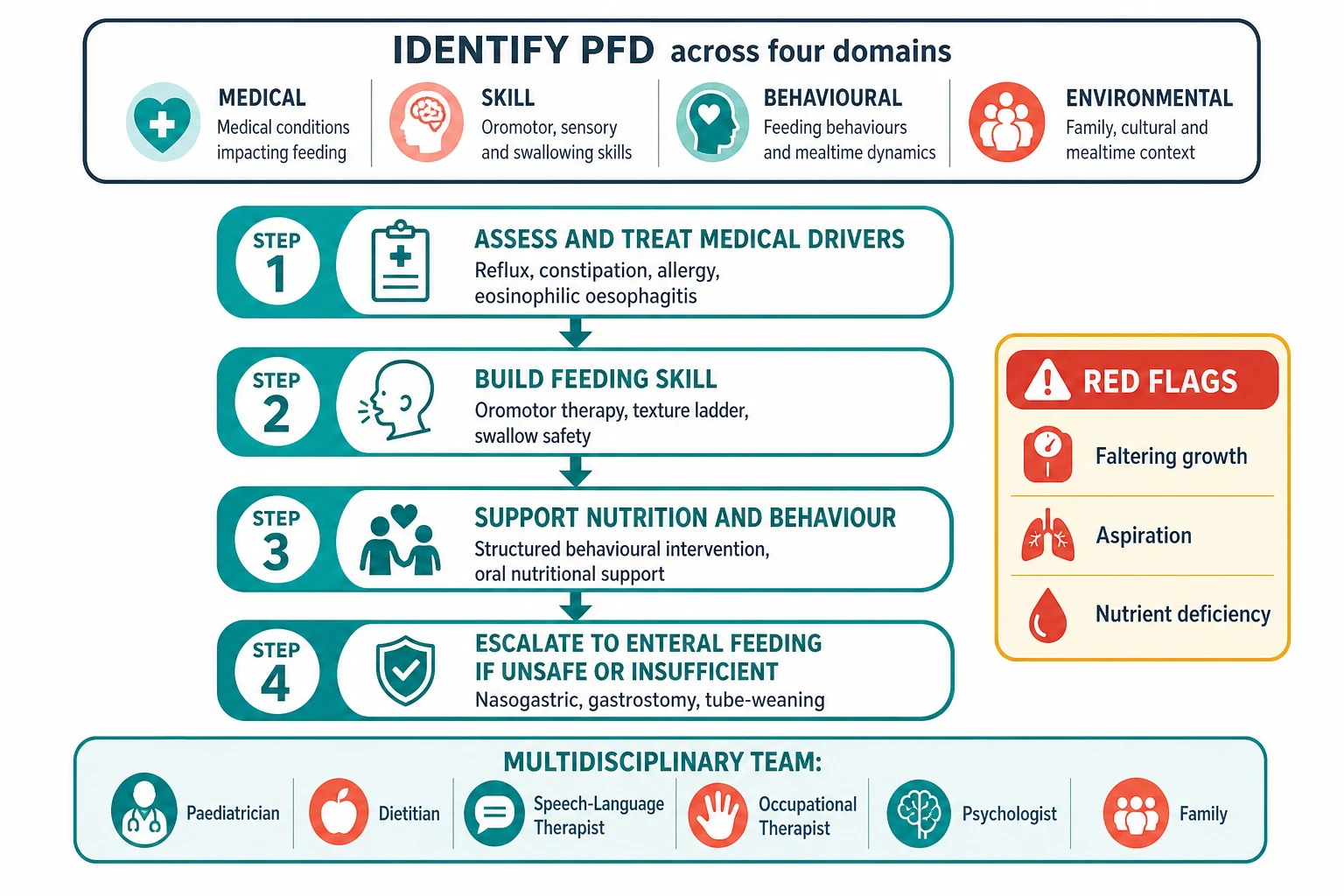
The definitive plan is built by a multidisciplinary team around the child and family, and it treats all four domains in parallel rather than in sequence. The paediatrician or gastroenterologist coordinates the medical care and treats the gastrointestinal drivers; the dietitian secures the nutrition and growth; the speech-language therapist builds the feeding skill and the swallow safety; the occupational therapist addresses posture, seating and sensory tolerance; the psychologist leads the behavioural intervention and supports the family; and the family carries the plan at every meal. No single discipline owns the problem, because the medical, nutritional, skill and psychosocial drivers all interact. [1] [5]
The first lever is to treat the medical driver, because feeding will not improve while the gut is uncomfortable. Optimise reflux management with feed thickeners, positioning and, where indicated, acid suppression; treat constipation aggressively with disimpaction and a maintenance regimen; manage eosinophilic oesophagitis and food allergy with dietary elimination or medical therapy guided by a specialist; and address any anatomical or airway cause. The principle the examiner rewards is that medical optimisation is the foundation on which every other intervention stands, and skipping it dooms the behavioural and nutritional work to fail. [4] [12]
The second lever is behavioural intervention, which is the evidence-based treatment for food selectivity and refusal. A systematic review and meta-analysis of intensive multidisciplinary intervention for paediatric feeding disorders found that structured, often Applied Behaviour Analysis-based programs produce substantial and clinically meaningful gains in oral intake, and that this intensive model is the effective standard of care for moderate to severe feeding disorders. A randomised comparison of a modified sequential oral sensory approach with an applied behaviour-analytic approach in children with autism and food selectivity found that the behaviour-analytic approach produced greater acceptance of novel foods, though the sequential oral sensory approach also helped. Behavioural intervention is delivered in outpatient, day-program or intensive inpatient settings depending on severity. [5] [7]
The third lever is nutritional support, which closes the gap between what the child will eat and what the child needs. The dietitian fortifies the accepted foods to increase energy density, uses age-appropriate oral nutritional supplements to top up intake, and addresses specific deficiencies such as iron. Where oral intake cannot be made safe or sufficient despite medical optimisation and behavioural intervention, enteral feeding is used. A nasogastric tube is the short-term option, and a gastrostomy is the long-term option for the child who will need non-oral feeding for months or years; the ESPGHAN position paper on percutaneous endoscopic gastrostomy in children guides the decision, the timing and the procedure, and emphasises the importance of an active tube-weaning plan from the outset to prevent feeding tube dependency. [12] [10]
[4] [12]Specific Subtypes & Scenarios
The child with cerebral palsy is the central scenario, because all four domains are often compromised at once. Reflux, constipation, oropharyngeal dysphagia and mealtime distress coexist, and the plan must address them together. The Eating and Drinking Ability Classification System grades how safely and efficiently the child eats and drinks and tracks aspiration risk, the swallow study defines the safe consistencies, and early gastrostomy is considered when oral intake cannot be made safe or sufficient. The qualitative evidence on caregivers' experiences confirms that feeding a child with cerebral palsy is a heavy and persistent burden, so carer support and respite are part of the plan, not an afterthought. [11] [12]
The tube-dependent child is the second scenario, and preventing tube dependency is far easier than treating it. The former premature infant who was tube-fed in the neonatal unit is at the highest risk, and an active oral-feeding pathway that advances feeding as the infant matures is the preventive strategy. When tube dependency is established, the treatment is a structured multidisciplinary tube-weaning program that combines hunger induction, behavioural intervention and oromotor therapy, and the evidence supports intensive programs for entrenched dependency. The principle is that the tube is a bridge, and a weaning plan should be in place from the day it is placed, because the longer a child is tube-dependent the harder the transition to oral feeding becomes. [10] [6]
The child with autism and food selectivity is the third scenario. The restriction is typically sensory-based, centred on texture, colour or brand, and the diet may be extremely narrow. The evidence-based treatment is structured behavioural intervention, and the randomised comparison of approaches found the applied behaviour-analytic method effective for expanding food acceptance in this group. The dietitian screens for the nutritional consequences of a narrow diet, particularly iron deficiency, and the team works with the family to generalise new foods into the everyday mealtime rather than the clinic room alone. [7] [4]
The child with eosinophilic oesophagitis or food allergy is the fourth scenario, because these conditions are common medical drivers of feeding aversion. The child develops dysphagia, food impaction or discomfort and learns to restrict the foods that cause symptoms, producing a conditioned aversion that persists after the inflammation is treated. The management is to treat the mucosal disease with dietary elimination or medical therapy, to confirm histological remission on biopsy, and then to address the residual behavioural aversion with structured intervention, because treating the gut alone often leaves a child who still refuses to eat. [4] [12]
Across Australia, Aotearoa New Zealand and the United Kingdom, paediatric feeding disorder is managed by a multidisciplinary team built around the paediatrician or gastroenterologist, the dietitian, the speech-language therapist or speech pathologist, the occupational therapist and psychology, with the ESPGHAN guidance informing gastrostomy decisions and the consensus four-domain framework shared internationally. Intensive day-program and inpatient feeding programs are concentrated in tertiary centres, and in rural, remote and low-resource settings the burden of untreated feeding difficulty and tube dependency falls more heavily on Indigenous, migrant and disadvantaged children. Telehealth-supported shared care with the local team, attention to the practicalities of feeding equipment and modified foods, and culturally safe family engagement are what make a multidisciplinary plan achievable for families far from a specialist centre. [1] [11]
Complications & Pitfalls
The complications of untreated paediatric feeding disorder run through the growth chart, the gut and the family. Faltering growth and specific nutrient deficiencies, particularly iron deficiency anaemia, follow from a narrow or insufficient intake. Aspiration and chronic lung injury follow when the feeding-skill domain is compromised and oral intake is pushed without swallow assessment. Feeding tube dependency develops when a tube placed for a short-term need is left without a weaning plan. Mealtime distress, family exhaustion and impaired quality of life follow from prolonged, difficult mealtimes, and a qualitative review has shown this burden to be substantial and persistent in families of children with cerebral palsy. [11] [10]
The diagnostic pitfalls are the failures the examiner rewards for naming. The first is labelling faltering growth as behavioural food refusal while a treatable medical driver such as reflux, eosinophilic oesophagitis or constipation goes unaddressed. The second is failing to distinguish paediatric feeding disorder from avoidant/restrictive food intake disorder, which leads to the wrong team and the wrong treatment. The third is pushing oral intake to improve nutrition before aspiration has been excluded by an instrumental swallow study, which risks worsening the lung injury. The fourth is assuming that treating the medical driver alone will resolve a conditioned feeding aversion, when the behavioural layer needs its own intervention. [1] [9]
The management pitfalls cut both ways. Over-treating a child whose feeding could be managed with medical optimisation, behavioural support and oral nutritional supplementation by moving straight to a gastrostomy imposes an unnecessary intervention and may entrench tube dependency, while under-treating a child with significant faltering growth or aspiration by reassurance and watchful waiting allows harm to accumulate. The safeguard is always the four-domain assessment and a genuine multidisciplinary plan that treats the medical, nutritional, feeding-skill and psychosocial drivers together, with clear escalation triggers and an active tube-weaning plan where a tube is used. [4] [12]
Prognosis & Disposition
The prognosis depends on the underlying cause, the severity of the feeding disorder, and how early and how completely the four domains are addressed. The typically developing child with a conditioned food aversion or a narrow diet often responds well to medical optimisation and structured behavioural intervention, and many children expand their diet and resume adequate intake within a focused program. The child with a correctable medical driver such as eosinophilic oesophagitis or food allergy improves once the mucosal disease or allergy is treated and the residual behavioural aversion is addressed. [4] [7]
The child with severe, permanent neurodisability carries a chronic or progressive feeding disorder in which the goal shifts from cure to protecting the lung, securing nutrition and preserving as much safe oral feeding and quality of life as possible. In cerebral palsy the feeding outcome tracks the motor severity, and feeding difficulty and malnutrition are recognised contributors to reduced survival in the most severely affected, which is why early gastrostomy in carefully selected children is associated with improved nutrition and carer quality of life. The tube-dependent child who completes an intensive weaning program has a good chance of transitioning to oral feeding, but the longer the dependency the harder the weaning. [11] [10]
Disposition follows the severity and the risk. The straightforward case is managed jointly by the general paediatrician, the dietitian and the speech-language therapist in the community or outpatient clinic, with behavioural support from psychology and the general practitioner supporting ongoing care. The child with moderate to severe feeding disorder, significant faltering growth, an unsafe swallow or entrenched tube dependency is managed in a tertiary centre with a dedicated intensive multidisciplinary feeding program, paediatric gastroenterology and the allied health feeding team, with a planned transition of care through childhood and adolescence. [5] [12]
Special Populations
The child with cerebral palsy is the first special population, because the burden of feeding disorder is greatest here and all four domains are often compromised. A structured four-domain assessment, the Eating and Drinking Ability Classification System grade, the instrumental swallow study when the bedside is uncertain, aggressive treatment of reflux and constipation, and early gastrostomy when oral intake cannot be made safe or sufficient are the standard of care, with carer support and respite built into the plan. [11] [12]
The premature and technology-dependent infant is the second. An active oral-feeding pathway that advances feeding as the infant matures is the strategy that prevents feeding tube dependency, and a structured multidisciplinary approach supports the high-risk infant through the transition from tube to oral feeding. The technology-dependent child with a tracheostomy or long-term ventilation adds oromotor and secretory challenges that demand a specialist airway and feeding team, and an intensive multidisciplinary feeding intervention has been described for high-risk infants in the perinatal period. [6] [10]
The Indigenous, remote, migrant and disadvantaged child is the third. The burden of untreated feeding difficulty and tube dependency falls unevenly on these children, the intensive feeding programs and the specialist teams are distant, and the cost and logistics of oral nutritional supplements and modified foods are harder to sustain. Culturally safe shared-care pathways, telehealth support for the local team, and attention to the practicalities of feeding equipment and supplies are what make a multidisciplinary plan achievable for families far from a specialist centre. [1] [11]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric feeding disorder rests on the 2019 consensus definition and the framework papers that followed it. The Goday consensus paper proposed the unifying term paediatric feeding disorder, defined as impaired oral intake that is not age-appropriate and is associated with medical, nutritional, feeding skill and/or psychosocial dysfunction, built on the World Health Organization International Classification of Functioning, Disability and Health framework, and this definition is the backbone of the whole topic. The Sharp framework paper then operationalised that definition into a case report form for characterising patients across the four domains, giving clinicians and researchers a common assessment standard. [1] [3]
The epidemiological evidence is anchored by the Kovacic nationwide prevalence study, which estimated that the annual prevalence of paediatric feeding disorder in 2014 was around one in thirty-seven children under five in a privately insured United States cohort and as high as one in twenty-three in a publicly insured cohort, with a significant increasing trend over time, placing the disorder on a par with commonly diagnosed conditions. The current state of the field is captured in the Silverman review of feeding disorders and the intensive multidisciplinary intervention literature, which frames the management approach for the gastroenterologist and the generalist. [2] [4]
The treatment evidence is the part examiners probe. The Sharp systematic review and meta-analysis of intensive multidisciplinary intervention established that structured, behaviour-based feeding programs produce substantial gains in oral intake and represent the effective standard of care for moderate to severe paediatric feeding disorders. The Peterson randomised comparison of a modified sequential oral sensory approach with an applied behaviour-analytic approach in children with autism and food selectivity found the behaviour-analytic method more effective for expanding food acceptance. The Sharp paper on intensive multidisciplinary feeding intervention for high-risk infants extends this to the perinatal population, and the Krom paper on feeding tube dependency frames the prevention and treatment of this specific complication. [5] [7] [6] [10]
[1] [5]Regional practice differs chiefly in access to intensive multidisciplinary feeding programs and the specialist teams rather than in the diagnostic principle. In well-resourced settings the four-domain framework, the intensive day-program and inpatient feeding interventions, and the ESPGHAN-guided gastrostomy pathway are routinely available, while in many low-resource, rural and remote settings the programs are distant and telehealth-supported shared care is the practical answer. The pharmacological evidence is thin: a systematic review found cyproheptadine may stimulate appetite and weight gain, but appetite stimulants are adjuncts to, not substitutes for, the multidisciplinary treatment of the underlying feeding disorder. [8] [11]
Exam Pearls
The stepped management of paediatric feeding disorder, MEALS mnemonic
References
- [1]Goday PS; Huh SY; Silverman A Pediatric Feeding Disorder: Consensus Definition and Conceptual Framework. J Pediatr Gastroenterol Nutr, 2019.PMID 30358739
- [2]Kovacic K; Rein LE; Szabo A Pediatric Feeding Disorder: A Nationwide Prevalence Study. J Pediatr, 2021.PMID 32702429
- [3]Sharp WG; Silverman A; Arvedson JC Toward Better Understanding of Pediatric Feeding Disorder: A Proposed Framework for Patient Characterization. J Pediatr Gastroenterol Nutr, 2022.PMID 35687655
- [4]Silverman A; Wall MA; Begotka A Feeding Disorders: Current State and Future Directions. Gastroenterol Clin North Am, 2025.PMID 41238275
- [5]Sharp WG; Volkert VM; Scahill L A Systematic Review and Meta-Analysis of Intensive Multidisciplinary Intervention for Pediatric Feeding Disorders: How Standard Is the Standard of Care? J Pediatr, 2017.PMID 27843007
- [6]Sharp WG Intensive Multidisciplinary Feeding Intervention for High-Risk Infants. Clin Perinatol, 2023.PMID 36868708
- [7]Peterson KM; Piazza CC; Volkert VM A comparison of a modified sequential oral sensory approach to an applied behavior-analytic approach in the treatment of food selectivity in children with autism spectrum disorder. J Appl Behav Anal, 2016.PMID 27449267
- [8]Harrison ME; Norris ML; Robinson A Use of cyproheptadine to stimulate appetite and body weight gain: A systematic review. Appetite, 2019.PMID 30825493
- [9]Katzman DK; Norris ML; Zucker N Avoidant Restrictive Food Intake Disorder. Psychiatr Clin North Am, 2019.PMID 30704639
- [10]Krom H; de Winter JP; Kindermann A Development, prevention, and treatment of feeding tube dependency. Eur J Pediatr, 2017.PMID 28409284
- [11]Taylor C; Badawi N; Novak I Caregivers' experiences of feeding children with cerebral palsy: a systematic review of qualitative evidence. JBI Evid Synth, 2025.PMID 40012369
- [12]Homan M; Hauser B; Romano C Percutaneous Endoscopic Gastrostomy in Children: An Update to the ESPGHAN Position Paper. J Pediatr Gastroenterol Nutr, 2021.PMID 34155150