Paeds · growth-development-and-behaviour
Augmentative communication, assistive technology and adaptive equipment
Also known as AAC · Speech-generating devices · Assistive technology children · Adaptive equipment paediatric · Complex communication needs · Powered mobility children
Fellowship-level prescription and coordination of AAC, assistive technology and adaptive equipment for children with complex communication and motor needs — feature-matching, trials, partner training, powered mobility, seating, and participation outcomes.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A preschooler with autism is “non-speaking.” A school-aged child with cerebral palsy is intelligent and frustrated, pointing and crying in class. A family was told to “wait and see if speech comes.” Your job is to stop that wait when complex communication needs are already clear. [3] [13]
Augmentative and alternative communication (AAC) supports or replaces spoken speech. It includes unaided methods (gesture, sign, facial expression) and aided methods (picture boards, books, speech-generating devices). Assistive technology (AT) is broader: any product or system that improves function or participation. Adaptive equipment includes seating, wheeled mobility, bathroom and self-care devices, and access tools. [12] [14]
Complex communication needs (CCN) means speech alone is not meeting daily communication demands. AAC is indicated by need, not by a failed waiting period. [13]
Classification
Classify tools by purpose and access, not by how expensive they look. [14]
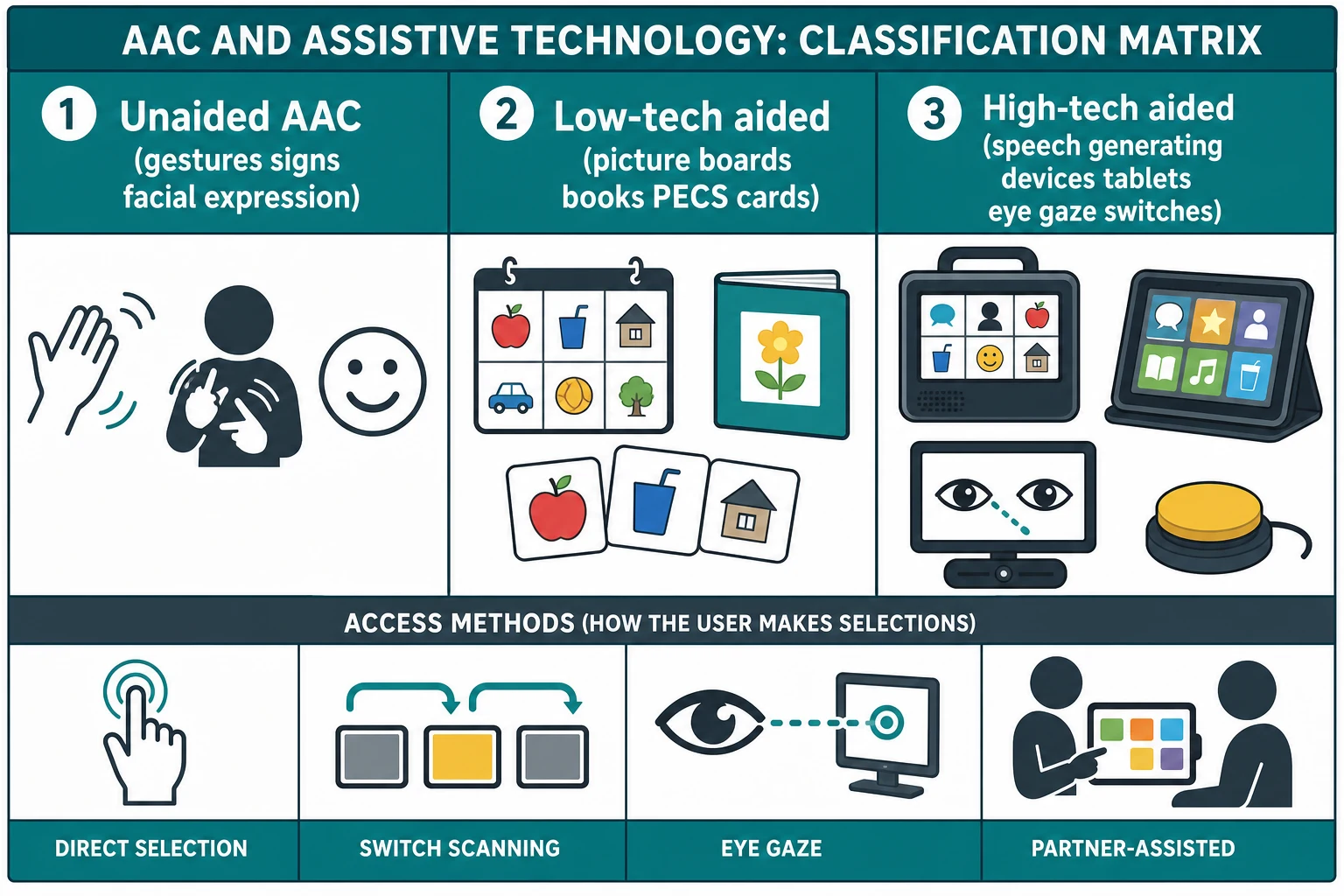
Tool classes you must keep straight
- Gesture, sign, facial expression, body movement
- Always available; no battery
- May be limited by motor or partner skill
- Picture boards, books, PECS-style cards, alphabet boards
- Backup when high-tech fails
- Often essential in hospital and outdoors
- Speech-generating devices and tablet systems
- Larger vocabulary and independence potential
- Needs charging, training and maintenance
Also classify access: direct selection (touch/point), switch scanning, eye gaze, head pointer, and partner-assisted scanning. Wrong access method looks like “the child cannot learn AAC.” [14]
Epidemiology & Risk Factors
Children who need these tools include those with cerebral palsy, autism with minimal verbal speech, Down syndrome, intellectual disability, acquired brain injury, and progressive neuromuscular disease. Functional communication profiles in cerebral palsy associate with impairment patterns and school therapy goals. Communication modality relates to participation. [7] [8]
Risks for poor outcomes include late referral, unfunded equipment, rural service gaps, culturally mismatched symbol systems, untrained school staff, and seating that blocks hand or visual access. Caregiver load is real — training must be practical. [12] [14]
Pathophysiology
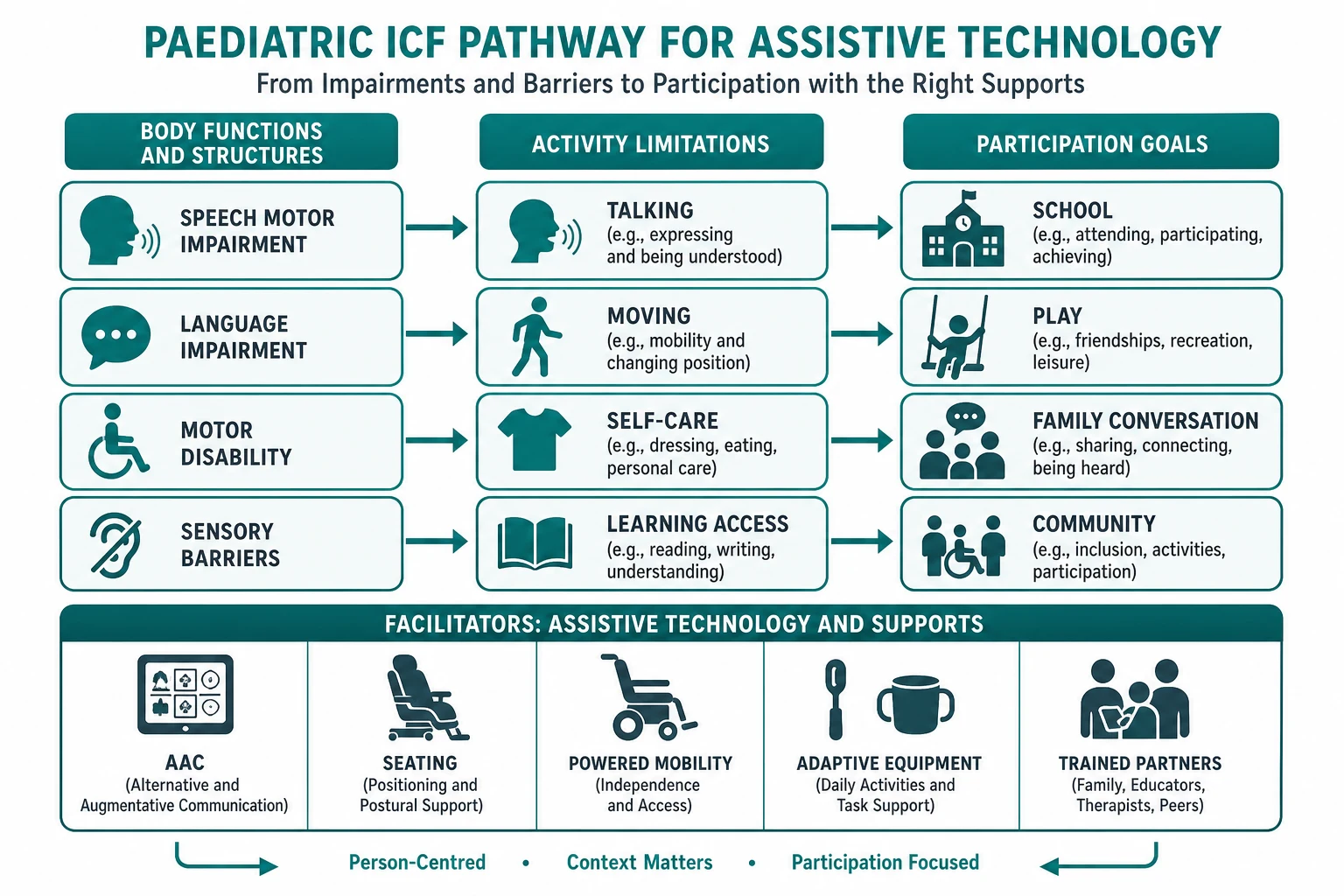
Think in ICF terms. Impairment of speech motor control, language, cognition, vision or hearing limits activities such as talking, reading access, self-care and mobility. Those limits shrink participation in school, play and family life. AAC and AT are environmental facilitators that reopen activity and participation pathways. [8] [12]
Speech motor impairment (for example dysarthria in cerebral palsy) may leave language comprehension relatively strong — a classic AAC indication. Language impairment needs vocabulary and language-system design, not only louder speech therapy. Autism-related social communication differences need systems that support initiation, requesting and social engagement with naturalistic teaching. [2] [3] [6]
Posture and seating change upper-limb and visual access. Adaptive seating can improve postural control and activity performance; without it, “failed AAC trials” are often failed positioning. [11]
Powered mobility changes what a young child can explore. Developmental change associated with powered mobility use is the reason early trials are discussed for severe motor impairment, not only older “transport” prescriptions. [9] [10]
Clinical Presentation
Families present with frustration, school letters, behaviour concerns, or “he understands everything but cannot speak.” Teachers report meltdowns at request time. Some arrive after years of speech-only therapy. [7] [13]
- non-speaking or minimally verbal autistic preschooler needing AAC pathway [3] [15]
- cerebral palsy with limited intelligibility and strong comprehension [6] [8]
- Down syndrome with language and literacy support needs where AAC can scaffold [4] [5]
- equipment abandoned: “we have a device but nobody uses it” [13]
- hospitalised AAC user whose device was left at home [13]
Red flags include progressive loss of speech skills (investigate regression), sudden refusal of a previously used system (pain, vision change, device fault, trauma), and severe distress from inability to communicate needs. [13]
Differential Diagnosis
Do not treat “needs AAC” as a single diagnosis. The underlying communication profile changes the plan. [14]
| Profile | What you may see | AAC implication |
|---|---|---|
| Speech motor disorder | Effortful speech, better comprehension | AAC for efficiency; speech therapy continues |
| Language disorder | Limited vocabulary/grammar | Language-rich aided systems |
| Autism / social communication difference | Limited initiation, restricted interests | Naturalistic SGD/PECS pathways; partner training |
| Hearing loss | Missed input | Audiology first; dual sensory plan |
| Intellectual disability | Slower learning rate | Robust vocabulary still; avoid underestimating |
| CVI / visual impairment | Looking away, need for display design | Vision-informed AAC layout |
Behaviour that looks like aggression is often communicative protest when requests and refusals have no reliable channel. Fix the communication system before only escalating behaviour plans. [13]
Clinical & Bedside Assessment
Lead with goals, then body functions, then tools. [14]
Paediatrician AAC/AT assessment spine
Goals
What must this child say, choose, refuse and share this month — at home and school?
Current means
Speech attempts, gesture, pictures, devices, who understands them, where communication fails.
Access body
Posture, hand function, head control, vision, hearing, switch sites, fatigue.
Language profile
Comprehension vs expression; literacy emerging; multilingual needs.
Team and trial
Refer/co-assess with SLP/OT/PT; plan feature-match trial and partner training.
Assess participation, not only sounds produced. Ask about playground, classroom, mealtime, toileting and pain communication. For mobility and bathroom equipment in cerebral palsy, real-world device use patterns matter for school inclusion planning. [8] [16]
Investigations
AAC prescription is not a blood-test pathway. Investigate the underlying developmental diagnosis on its own merits. [13]
Do first when indicated: hearing assessment, vision/CVI-informed assessment, and seating/positioning review before declaring AAC failure. [11] [14]
Trials are the functional “investigation.” Feature-match, trial low- and high-tech options, and measure communication and participation during the trial — not after a rushed purchase. Assessment practice reviews emphasise structured participation-model thinking for children with limited speech and motor skills. [14]
Management — Resuscitation
In acute care, communication is a safety tool. [13]
- Keep or recreate access to the child’s usual AAC system during ED and ward care. [13]
- If the device is unavailable, provide low-tech boards for pain, toilet, breathlessness and family contact. [13]
- Do not delay oxygen, seizure care or sepsis treatment while “finding the iPad” — assign a partner to set up communication in parallel. [13]
- Document how this child signals yes/no and distress in the medical record. [13]
Management — Definitive & Stepwise
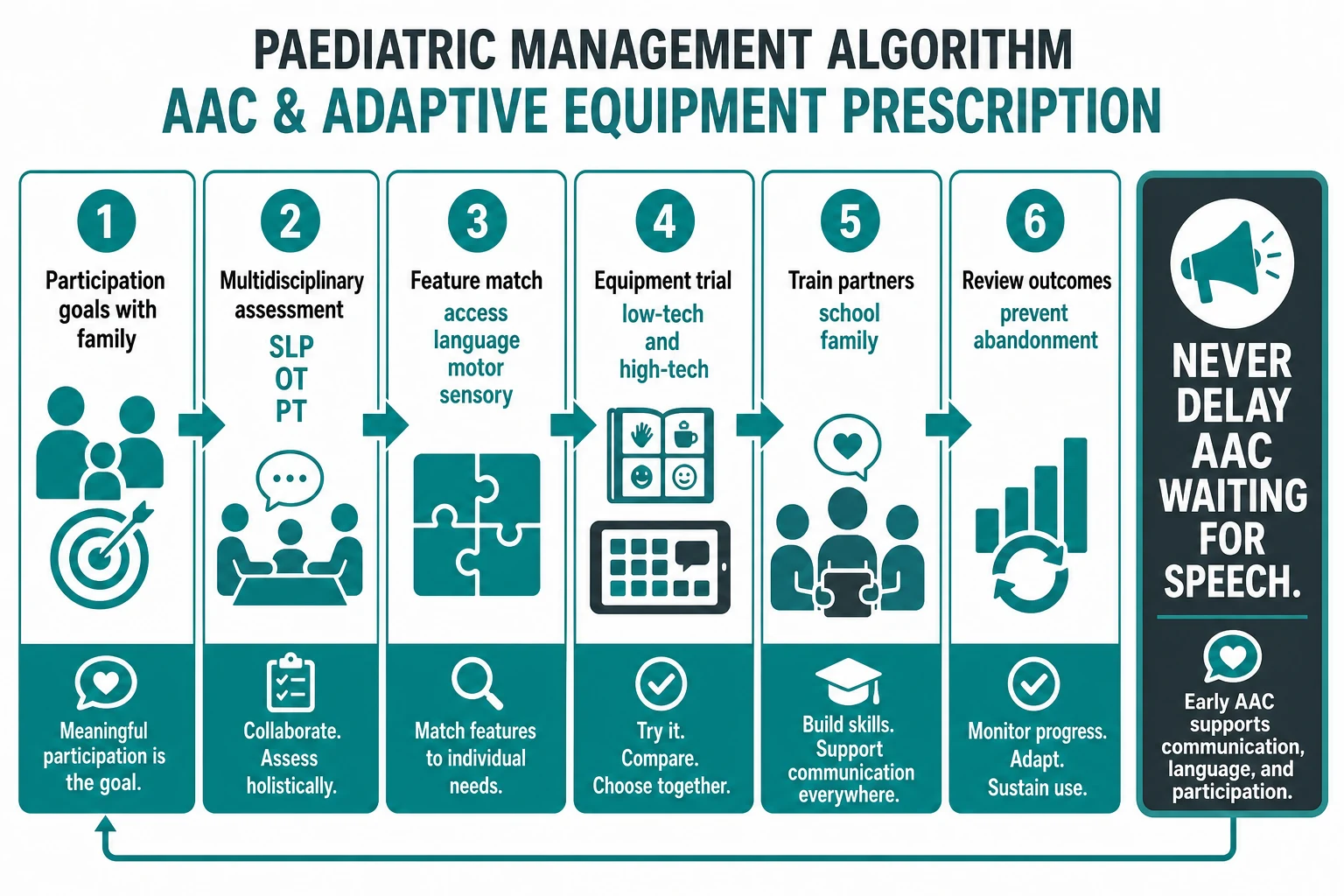
Step 1 — Goals and early offer
When CCN is clear, offer multi-modal AAC promptly. Continue speech therapy where appropriate; do not force a false choice between speech and AAC. Best-practice scoping work supports structured healthcare-based interventions for children and adolescents with CCN. [2] [13]
Step 2 — Feature-match with the team
Speech pathology leads language system and symbol design. OT/PT solve access, seating and mobility. Paediatricians integrate medical constraints, funding letters, vision/hearing, tone management and school advocacy. [14] [16]
Step 3 — Choose and trial systems
PECS has meta-analytic support for requesting skills in autism; speech gains are limited or variable — counsel honestly. [1]
Naturalistic SGD interventions have single-subject evidence for children with CCN. [2]
SGD programmes for autistic preschoolers are synthesised in recent systematic review — use them as early supports, not last resorts. [3]
Down syndrome AAC literature supports language and literacy scaffolding roles. [4] [5]
Cerebral palsy needs concurrent speech-language therapy evidence awareness plus AAC for functional participation. [6] [7] [8]
Always keep a low-tech backup. Batteries die. Rain happens. Hospitals confiscate gadgets. [13]
Step 4 — Seating, mobility and daily living equipment
Adaptive seating can improve postural control and activity performance and should be considered when posture limits function. [11]
Assistive devices and technologies influence activities and participation for children with cerebral palsy across everyday life. [12]
Wheeled mobility, seating and bathroom devices are common real-world needs — plan school and home environments together. [16]
Powered mobility can support developmental change and therapeutic goals in young children with severe cerebral palsy; discuss early trials with therapy teams rather than automatic age exclusion. [9] [10]
Step 5 — Train partners and fund sustainably
Train family, teachers and aides. Write simple modelling scripts. Schedule review. Funding pathways (for example NDIS in Australia, education systems elsewhere) are jurisdiction-specific — state the need functionally; do not invent entitlement rules. [12] [13]
Step 6 — Review against participation
Ask: Can the child request, refuse, comment and repair breakdowns across settings? Has frustration behaviour fallen? Is school including the system? Upgrade vocabulary and access as the child grows. [8] [13]
Specific Subtypes & Scenarios
Scenario map
- Minimally verbal autistic preschooler: early SGD/PECS pathway, naturalistic teaching, parent coaching; monitor speech without delaying AAC. [1] [3] [15]
- CP with dysarthria: intelligibility strategies + AAC for classroom participation; seating enables access. [6] [8] [11]
- Down syndrome language support: AAC to expand language/literacy opportunities, not only “backup.” [4] [5]
- Early powered mobility: therapy-led trial for severe motor impairment; measure exploration and engagement. [9] [10]
- Device abandonment clinic: re-check goals, access, seating, training and cultural fit before blaming the child. [13] [14]
- Multilingual family: symbol language and partner modelling in home languages. [13]
- Ward admission: bring device, low-tech backup, documented yes/no and pain signals. [13]
Complications & Pitfalls
- Underestimating comprehension because speech is limited. [7]
- Over-promising that PECS will create fluent speech. [1]
- Prescribing high-tech only and leaving the family without low-tech backup. [13]
- Forgetting bathroom and classroom equipment when focusing only on the tablet. [16]
- Cultural or linguistic mismatch of symbol sets. [13]
Prognosis & Disposition
Prognosis for participation improves when AAC/AT is early, feature-matched, trained and reviewed. Speech outcomes vary by diagnosis; participation outcomes are the primary target. [8] [13]
Disposition after clinic: written goals, trial plan, training schedule, therapy referrals, school letter, funding support letter, and a review date. Escalate earlier if distress behaviour escalates or access is lost. [13] [14]
Special Populations
Infants and toddlers may need early access tools and powered mobility developmental trials — age alone is not a veto. [9]
Severe motor impairment needs creative access (switch, eye gaze) and excellent seating. [11] [14]
Visual impairment/CVI needs display design changes, not abandonment of AAC. [14]
Intellectual disability still deserves robust vocabulary and dignity of communication. [13]
Rural families need telehealth training plans and durable low-tech systems. [12]
Indigenous and multilingual families need culturally safe goal-setting and language-congruent systems. [13]
Evidence, Guidelines & Regional Differences
Evidence spans PECS meta-analysis, naturalistic SGD reviews, autistic preschooler SGD synthesis, Down syndrome AAC review, cerebral palsy communication and participation studies, powered mobility developmental work, adaptive seating systematic review, and assistive-device participation scoping reviews. Use these to defend early multi-modal support. [1] [2] [3] [4] [9] [11] [12]
[12] [13]Exam Pearls
- Behaviour may be a communication emergency. [13]
- Comprehension can far exceed speech output. [7]
- Low-tech backup is non-negotiable. [13]
- Team sport: SLP, OT, PT, school, family, paediatrician. [14]
References
- [1]Flippin M Effectiveness of the Picture Exchange Communication System (PECS) on communication and speech for children with autism spectrum disorders: a meta-analysis. American journal of speech-language pathology, 2010.PMID 20181849
- [2]Gevarter C Naturalistic Speech-Generating Device Interventions for Children With Complex Communication Needs: A Systematic Review of Single-Subject Studies. American journal of speech-language pathology, 2018.PMID 29971336
- [3]Therrien MCS A Systematic review of AAC interventions using speech generating devices for autistic preschoolers. Augmentative and alternative communication (Baltimore, Md. : 1985), 2025.PMID 40164143
- [4]Barbosa RTA Augmentative and alternative communication in children with Down's syndrome: a systematic review. BMC pediatrics, 2018.PMID 29751828
- [5]Barton-Hulsey A Augmentative and Alternative Communication Supports for Language and Literacy in Preschool: Considerations for Down Syndrome and Autism Spectrum Disorder. Seminars in speech and language, 2021.PMID 34311485
- [6]Pennington L Speech and language therapy to improve the communication skills of children with cerebral palsy. The Cochrane database of systematic reviews, 2004.PMID 15106204
- [7]Koopmans C Functional Communication Abilities in Youth With Cerebral Palsy: Association With Impairment Profiles and School-Based Therapy Goals. Language, speech, and hearing services in schools, 2022.PMID 34767477
- [8]Allison KM Relation of Speech-Language Profile and Communication Modality to Participation of Children With Cerebral Palsy. American journal of speech-language pathology, 2024.PMID 38215219
- [9]Logan SW Powered Mobility Device Use and Developmental Change of Young Children with Cerebral Palsy. Behavioral sciences (Basel, Switzerland), 2023.PMID 37232636
- [10]Rosenberg L Evaluating a Therapeutic Powered Mobility Camp for Children with Severe Cerebral Palsy. Canadian journal of occupational therapy. Revue canadienne d'ergotherapie, 2021.PMID 34435918
- [11]Acharya BD Effect of Adaptive Seating Systems on Postural Control and Activity Performance: A Systematic Review. Pediatric physical therapy : the official publication of the Section on Pediatrics of the American Physical Therapy Association, 2023.PMID 37747975
- [12]Hoekstra D The role of assistive devices and technologies in the activities and participation in everyday life of children with cerebral palsy - a scoping review. Disability and rehabilitation. Assistive technology, 2025.PMID 40928660
- [13]Resina P Identifying and Describing Best Clinical Practices for Children and Adolescents With Complex Communication Needs: A Scoping Review of Healthcare-Based Interventions. Journal of intellectual disability research : JIDR, 2025.PMID 40745993
- [14]Coan-Brill J Exploring augmentative & alternative communication assessment practices for children with limited functional speech & motor skills: a scoping review utilizing the Participation Model of AAC. Disability and rehabilitation. Assistive technology, 2025.PMID 39891921
- [15]Sterrett K The effect of responsiveness to speech-generating device input on spoken language in children with autism spectrum disorder who are minimally verbal. Augmentative and alternative communication (Baltimore, Md. : 1985), 2023.PMID 36267016
- [16]Livingstone RW Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy. Canadian journal of occupational therapy. Revue canadienne d'ergotherapie, 2026.PMID 41719113