Paeds · growth-development-and-behaviour
Autism spectrum disorder
Also known as ASD · Autism · Autistic spectrum disorder · Asperger syndrome · Pervasive developmental disorder · PDD-NOS
Fellowship assessment and management of autism spectrum disorder: DSM-5-TR diagnosis, multimodal evaluation, early supports, comorbidity care, irritability pharmacotherapy with monitoring, crisis care, education interfaces and regional pathways.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A caregiver brings a three-year-old who “lives in his own world.” He lines up cars, panics when the route home changes, and does not look when his name is called at childcare. Your job is not only to label or not label. You must decide what is unsafe today, what supports start this week, and how diagnosis will change the plan. Early red-flag surveillance and screening tools live on the sister page Social communication concerns and autism recognition. This page owns assessment, confirmation, medical work-up, intervention ladder and irritability pharmacology. [1] [2] [18]
Overview & Definition
ASD is a neurodevelopmental condition. It is not progressive neurodegeneration and not a personality style. Core features are (1) persistent deficits in social communication and social interaction across contexts, and (2) restricted, repetitive patterns of behaviour, interests or activities. Features are present in the early developmental period. They may not fully show until social demands exceed capacity. They cause clinically significant impairment. They are not better explained by intellectual developmental disorder alone. When both occur, social communication must sit below that expected for the child’s general developmental level. [1] [3]
DSM-5 collapsed older labels (autistic disorder, Asperger disorder, PDD-NOS) into one spectrum with severity levels and clinical specifiers. ICD-11 uses the same broad clinical construct for multi-board candidates. Use the current operational criteria in your exam answer; do not spend viva time defending historical taxonomy. [2] [3]
Classification
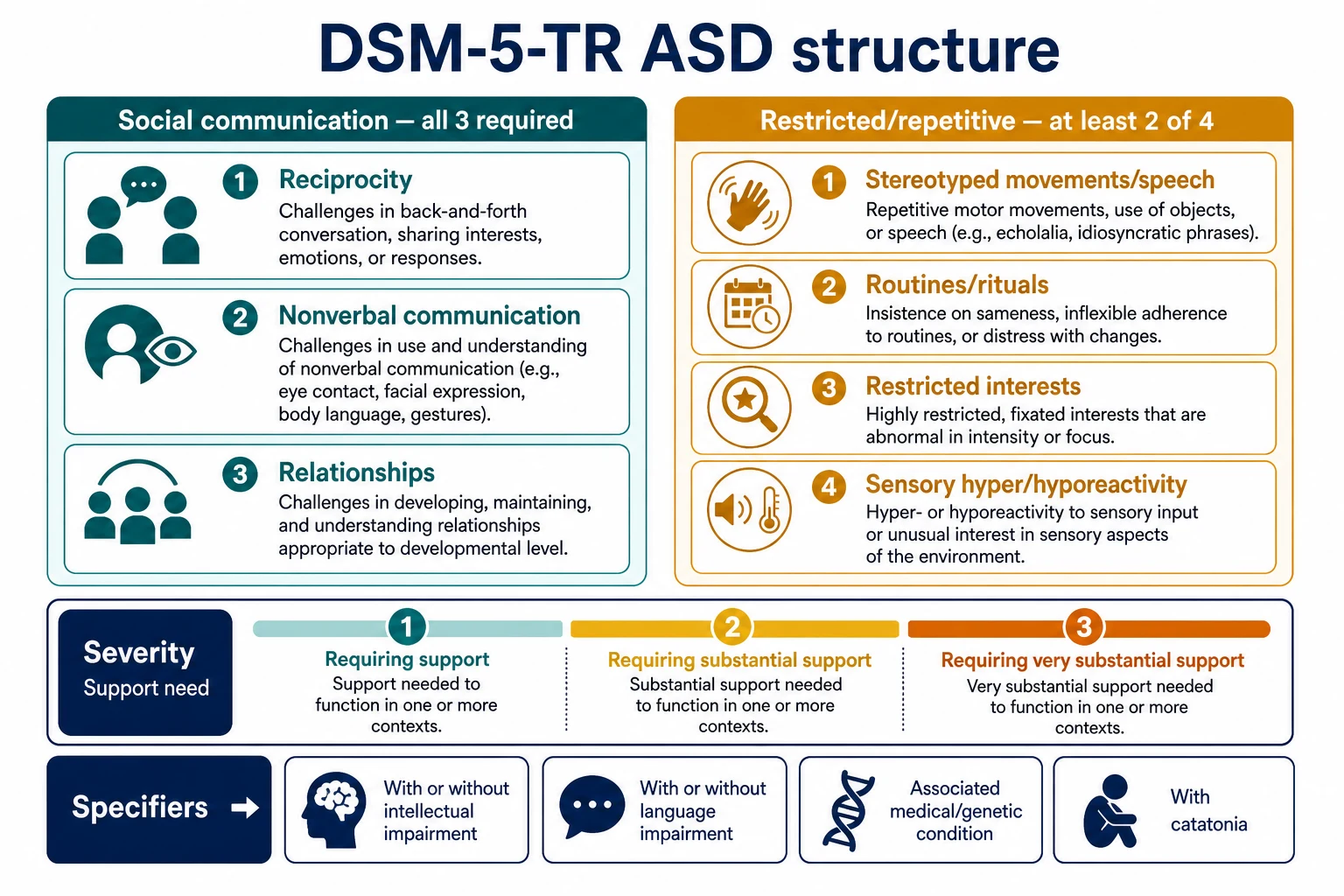
DSM-5-TR structure (must be exam-ready)
A. Social communication and social interaction — all three required (current or by history): [1] [3]
- Social-emotional reciprocity deficits (odd social approach, reduced sharing of interests or emotions, failure of back-and-forth conversation). [1]
- Nonverbal communicative behaviour deficits (poor eye contact, limited gesture, mismatch of verbal and nonverbal signals). [1]
- Developing, maintaining and understanding relationships (difficulty adjusting behaviour to context, making friends, or shared imaginative play). [1] [3]
B. Restricted, repetitive patterns — at least two of four: [1] [3]
- Stereotyped or repetitive motor movements, object use or speech. [1]
- Insistence on sameness, inflexible routines, ritualised patterns. [1]
- Highly restricted, fixated interests abnormal in intensity or focus. [1]
- Hyper- or hyporeactivity to sensory input, or unusual sensory interest. [1] [3]
C–E. Symptoms present in the early developmental period; cause clinically significant impairment; not better explained by intellectual disability or global developmental delay alone. [1]
Severity levels and specifiers
Levels 1–3 rate how much support the person needs for social communication and for restricted/repetitive behaviour. Level is not a polite word for IQ. A verbally fluent adolescent can still need substantial support. Specifiers to record: with/without intellectual impairment; with/without language impairment; associated with a known medical or genetic condition; associated with another neurodevelopmental, mental or behavioural disorder; with catatonia. [1] [2] [3]
Social (pragmatic) communication disorder
SCD shares social-communication difficulty but lacks the restricted/repetitive domain. If RRBs are present, think ASD, not SCD. That discriminator is a classic written-exam trap. [1] [2]
Epidemiology & Risk Factors
US ADDM surveillance at age 8 years reported a prevalence on the order of about 1 in 36 children in the 2020 network estimate, with variation by site, sex and identification method. Global reviews show wide ranges because methods differ. Do not memorise one magic percentage as universal truth; state the source and that ascertainment drives the number. [4] [5]
Males are identified more often than females. Girls are under-recognised, especially when language is strong and camouflaging is present. Heritability estimates are high in twin and family designs. Both genetic and environmental factors contribute; there is no single “autism gene” for most children. Advanced parental age and some perinatal adversities associate with higher risk. Syndromic conditions (fragile X, tuberous sclerosis, certain copy-number variants) raise risk and change surveillance. [3] [6] [7]
Vaccines do not cause autism. That statement is exam-ready and clinically necessary. Spend time on evidence and trust repair, not on false balance. [1]
Population-derived samples show very high rates of additional psychiatric diagnoses — ADHD, anxiety, oppositional behaviours and others are common, not exotic. Epilepsy, sleep problems and intellectual disability frequently co-occur. [17]
Pathophysiology
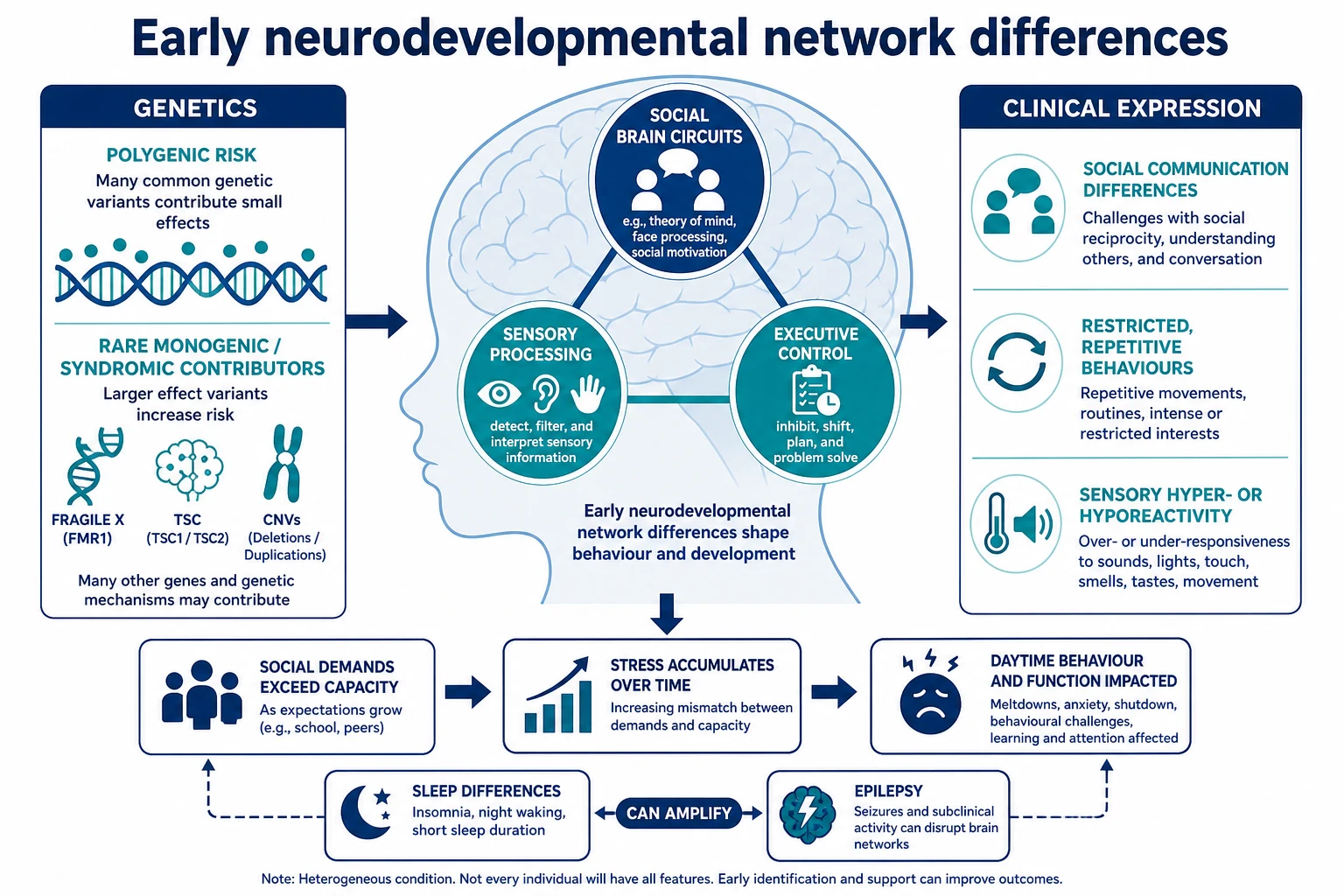
Think early brain development and network organisation, not a lesion you can point to on every MRI. Polygenic risk is common. Rare monogenic and chromosomal findings explain a minority but matter for counselling and multi-organ care. Sensory processing differences and executive function challenges help explain why a child melts down in a noisy supermarket yet settles with predictable routine. Social demands rise with age. That is why some children look “fine” in toddlerhood and then struggle when peer complexity explodes at school. Sleep disruption and epilepsy can worsen daytime behaviour and learning. Treat those drivers; do not label every behaviour as “core autism.” [1] [3] [7] [19]
Clinical Presentation
Toddler. Limited response to name, reduced joint attention, delayed pointing or showing, limited pretend play, language delay or plateau, intense lining-up or spinning, distress with small routine changes. Caregivers may say “he is in his own world.” [1] [18]
Language regression in the second year can occur in ASD. True progressive multi-domain regression with seizures or focal neurology is a different emergency pathway — do not call every word loss “just autism.” [1]
Preschool and school age. Peer entry failure, one-sided conversations about special interests, rigid rules, sensory overload in assemblies, meltdowns after school when masking collapses. Academic skills may be strong or uneven. [1] [3]
Adolescent, especially girls. Camouflaging, internalising anxiety or depression, social exhaustion, late first diagnosis after school refusal or self-harm. Do not stop at “shy” or “anxious” without a developmental history. [3] [20]
With intellectual disability. Social communication must still fall below developmental expectation. Self-injury and severe irritability are more common and need careful medical and functional analysis. [1] [2]
Differential Diagnosis
| Working alternative | What helps you tell it apart |
|---|---|
| Hearing impairment | Audiology first; social interest may be preserved once hearing is restored |
| Isolated speech-language disorder | Social intent and nonverbal reciprocity relatively stronger; RRBs absent |
| Social (pragmatic) communication disorder | Social-communication difficulty without RRBs |
| ADHD alone | Inattention/hyperactivity across tasks; social intent present though impulsive |
| Social anxiety / selective mutism | Speaks and relates normally in comfortable settings; onset often later |
| Intellectual disability alone | Social communication matches developmental level |
| Attachment/trauma-related difficulties | Care history, recovery in safe caregiving, pattern differs from pervasive RRB profile |
| Epileptic encephalopathy / metabolic disease | Regression with neurology, systemic clues, progressive course |
| Psychosis / catatonia | New break, hallucinations/delusions, posturing, mutism, food refusal |
Dual diagnoses are allowed. ASD + ADHD is common. ASD + anxiety is common. Name both when both impair function. [17]
Clinical & Bedside Assessment
Lead with multi-setting history. Ask home, childcare and school the same core questions: How does the child share interest? How do they use gesture and eye contact for communication? How do they play with peers? What happens when routines change? What sensory triggers exist? What is sleep, feeding, toileting and safety like? [1] [2]
Observe play and interaction yourself when possible. Watch for joint attention, response to name, pointing, reciprocal smile, flexibility and repetitive behaviours. Examine growth, dysmorphism, skin (for neurocutaneous clues), neurology, hearing and vision pathways. Assess developmental level. Document strengths as carefully as deficits — that changes educational planning. [1] [2]
Standardised tools (for example ADOS-2, ADI-R, cognitive and adaptive testing) support diagnosis. They do not replace clinical judgment. A tool score without multi-setting impairment is not a diagnosis. A clear clinical picture should not wait forever for a perfect battery when supports are already needed. [1] [2] [20]
Screening instruments such as M-CHAT-R/F belong mainly to the recognition pathway. Positive screens still need full assessment; negative screens do not erase strong clinical concern. [18]
Investigations
| Situation | Action | Why |
|---|---|---|
| Language delay or suspected ASD | Audiology | Never skip hearing |
| After ASD diagnosis (especially with ID, dysmorphism, family history) | Chromosomal microarray; fragile X testing as per genetics pathways | Aetiologic yield and counselling |
| Seizures, atypical regression, focal signs | EEG / neurology pathway | Not routine for classic ASD |
| Before antipsychotic for irritability | Weight/BMI, BP, glucose or HbA1c, lipids; FBC, U&E, LFT as indicated; ECG if cardiac risk; prolactin baseline for risperidone | Safety monitoring |
| Behaviour change | Dental, ENT, constipation, reflux, sleep apnoea, pain screen | Common missed medical drivers |
| Typical ASD, no neuro red flags | MRI not routine | Low yield, avoid false reassurance or false alarms |
Counsel families that genetic testing looks for a cause in a minority, may guide surveillance, and does not remove the clinical ASD diagnosis if criteria are met. [19]
Management — Resuscitation
In ED or on the ward, a meltdown is not a moral failure. Reduce sensory load. Use sparse language. Offer two clear choices. Keep familiar carers close when safe. Avoid crowded noisy corridors if you can. Check for pain, delirium, seizure, intoxication, constipation, dental disease and hunger. [1] [16]
Use least-restrictive safety measures. Physical intervention and chemical restraint are last resorts for imminent harm, not first-line behaviour management. Antipsychotics are not the first response to a transient overload meltdown. [2] [16]
Management — Definitive & Stepwise
Core principle
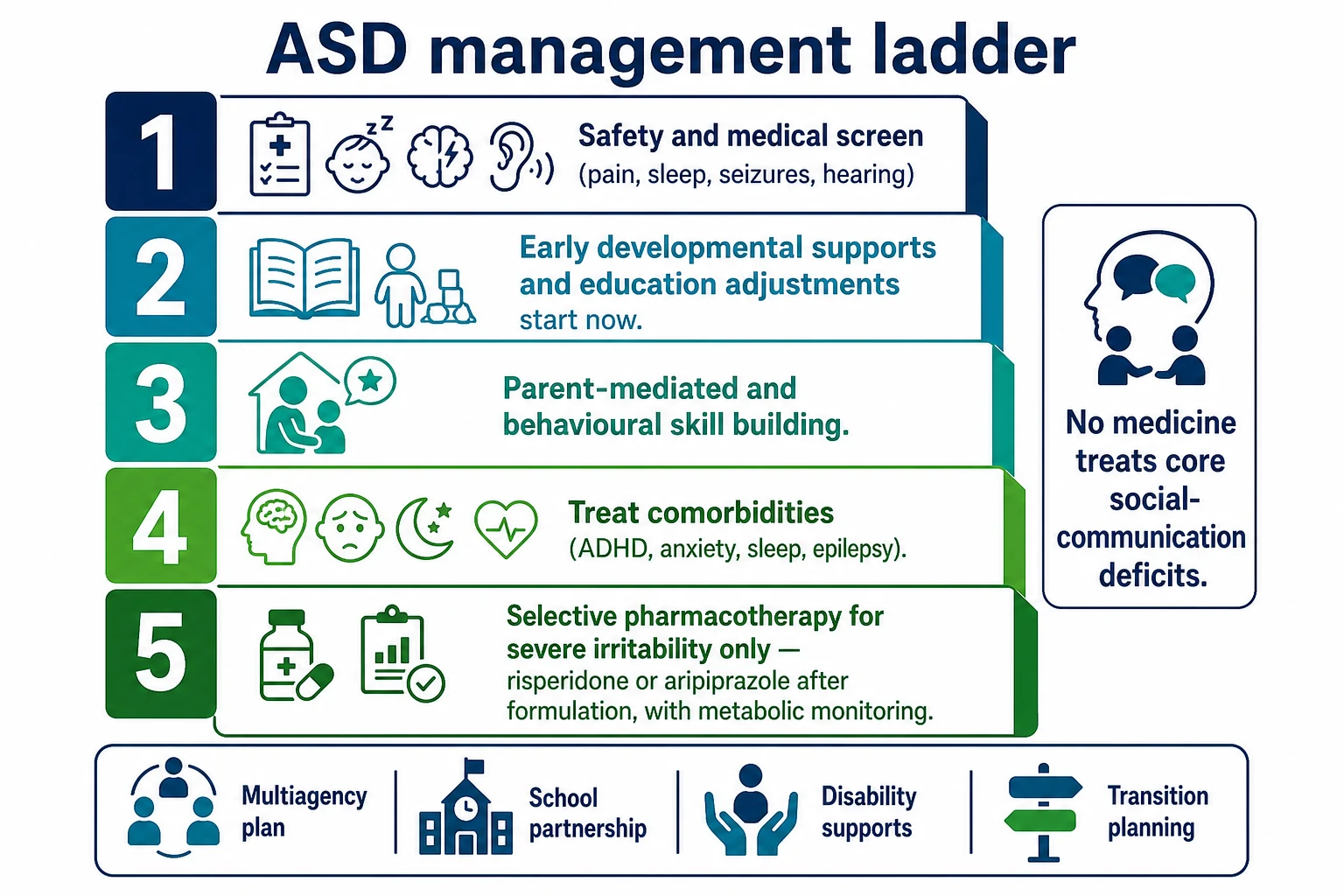
No medication treats core ASD social-communication deficits as a primary indication. Primary treatments are developmental, educational, behavioural and environmental. Pharmacotherapy targets comorbidities and severe irritability when criteria are met. [1] [2] [16]
Start supports early
When clinical concern is high, begin early intervention, speech-language therapy, occupational therapy and educational adjustments while diagnostic assessment proceeds. Waiting months for a final report before any support is a systems failure, not caution. [1] [20]
Landmark early intervention evidence
Early Start Denver Model (ESDM). A randomised trial in toddlers with autism showed gains in IQ, adaptive behaviour and diagnostic severity markers versus community referral — the classic intensive early developmental intervention landmark. [11]
PACT (parent-mediated communication-focused treatment). A randomised trial improved parent–child dyadic social communication. Long-term follow-up reported sustained benefits on autism symptom trajectories beyond the active treatment window. [12] [13]
Early intensive behavioural intervention (EIBI). Cochrane synthesis supports gains for some young children, with important caveats about study quality and individualisation. Name EIBI as one evidence-informed approach, not a single mandatory brand. [23]
Parent training for disruptive behaviour. Structured parent training outperformed parent education alone for reducing disruptive behaviours in children with ASD. Skill-building for carers is clinical care, not optional soft advice. [14]
Practical package examiners expect: speech and language therapy (including AAC when needed), OT for sensory and adaptive skills, structured teaching approaches, educational adjustments, family psychoeducation, and disability-support planning. Cross-link early-intervention and AAC leaves for full system detail. [1] [20]
Irritability pharmacotherapy
Indication. Severe irritability — aggression, severe tantrums, self-injury — causing safety risk or major impairment after environmental and behavioural measures. Not mild frustration. Not social awkwardness. [8] [9] [16]
Risperidone — RUPP landmark. In the Research Units on Pediatric Psychopharmacology Autism Network trial, risperidone substantially reduced serious behavioural problems versus placebo in children with autism, with weight gain and other adverse effects. Practical dosing is weight-based and low-start: for many school-age children, start around 0.25–0.5 mg/day, titrate slowly; RUPP mean doses were typically in the 1–2 mg/day range under protocol by weight band. Always check current local product information and age licensing. [8] [16]
Monitoring for risperidone: weight and BMI every visit initially; fasting glucose/HbA1c and lipids at baseline and serially; extrapyramidal signs; prolactin-related symptoms; sedation; ECG if cardiac risk. Plan review for dose minimisation once behaviour stabilises. [8] [16]
Aripiprazole. Owen and colleagues showed efficacy for irritability in children and adolescents with autistic disorder versus placebo. Related programmes included fixed-dose arms such as 5, 10 and 15 mg/day. Common clinical start is 2 mg daily with titration toward the effective trial range. Watch for akathisia, activation and metabolic effects. Weight gain is often milder than risperidone but not absent. [9] [10] [16]
Meta-analytic evidence supports risperidone and aripiprazole for severe irritability/problem behaviours, with adverse-effect trade-offs that mandate monitoring and time-limited goals. [16]
What not to do with medicines
Do not prescribe SSRIs expecting reduction of core RRBs. Citalopram was ineffective for high levels of repetitive behaviour in a large randomised trial and caused more adverse events than placebo. Treat co-occurring anxiety or OCD on their own merits with adapted psychological care and careful SSRI use when indicated — not as a stealth core-ASD drug. [15]
Comorbidity-targeted care
Treat ADHD with behavioural supports and, when indicated, stimulants or non-stimulants with careful titration. Extended-release guanfacine has randomised evidence for hyperactivity in children with ASD and can be considered in that comorbidity pathway under specialist guidance. Treat epilepsy. Treat sleep problems; melatonin has randomised evidence for sleep problems in children with neurodevelopmental disorders, used with behavioural sleep care and local product guidance. Treat anxiety and depression with autism-adapted psychological approaches; ask about suicide risk directly. [1] [17] [24] [25] [22]
Specific Subtypes & Scenarios
Toddler with high concern. Audiology, parallel early intervention referral, diagnostic pathway, caregiver coaching — same week priorities, not sequential waiting lists only. [1] [18]
School-age ASD + ADHD. Dual diagnosis is allowed. The classroom plan must address attention and social-communication needs together. [17]
ASD with severe ID and self-injury. Functional analysis first. Medical pain screen first. Antipsychotic only if severe ongoing risk after behavioural measures. [14] [16]
Adolescent girl, late diagnosis. Revisit developmental history. Screen mental health. Avoid pure “anxiety” closure. [3] [20]
Suspected catatonia. Emergency medical-psychiatric pathway. [2]
Syndromic ASD. Genetics and multi-organ surveillance (for example fragile X, TSC) change the long-term plan. [19]
Rural/telehealth. History and collateral can start remotely; direct observation and hearing assessment still need a concrete plan. [1]
ED meltdown after missed dental pain. Fix the medical driver; do not escalate chronic antipsychotic for an acute tooth abscess. [1] [16]
Complications & Pitfalls
- Watchful waiting that delays support after clear red flags. [1]
- Diagnostic overshadowing of medical illness, abuse, ADHD, depression or psychosis. [17] [2]
- Premature antipsychotic without functional analysis or medical screen. [16]
- Chronic risperidone without metabolic review. [8]
- Using citalopram/SSRIs as core RRB treatment despite negative evidence. [15]
- Skipping audiology. [1]
- Ignoring suicide risk and premature mortality data. [21] [22]
- Confrontational vaccine counselling that destroys trust instead of teaching evidence. [1]
- Abrupt service drop at 18 without transition. [20]
Prognosis & Disposition
Outcomes vary widely. Better adaptive outcomes associate with stronger early language, higher cognitive ability, earlier access to supports, lower comorbidity burden and stable environments. None of that licenses therapeutic nihilism for children with high support needs. Population data show premature mortality risk in ASD, with neurological and psychiatric comorbidity contributing — physical health and mental health both matter across the lifespan. [3] [20] [21]
Disposition is multiagency: health, education, disability supports and family. After a new diagnosis, give a written problem representation, support plan, crisis contacts and review date. After medication start, book monitoring before the family leaves. [1] [20]
Special Populations
Infants and toddlers. Parallel supports and diagnosis; parent-mediated work is central. [11] [12]
Girls and women. Later diagnosis, camouflaging, internalising comorbidity. [3]
ASD with intellectual disability and medical complexity. Higher genetic yield; adapt communication and capacity supports. [1] [19]
Indigenous and culturally diverse families. Use interpreters, cultural consultation and community-informed collateral. Do not lower the impairment bar. Do not racialise behaviour. [20]
Migrant and refugee families. Tool validity and language access matter; professional interpreters beat family translation for assessment. [1]
Out-of-home care and safeguarding. Elevated vulnerability; growth, behaviour and school exclusion can be welfare signals. [20]
Gender-diverse autistic young people. Both identities can be true; provide dual affirming care without collapsing one into the other. [20]
Transition. Plan early from mid-teens: diagnosis summary, communication profile, risk formulation, medication plan, education/employment and named adult services. [20]
Evidence, Guidelines & Regional Differences
Practice aligns with multidisciplinary diagnosis, early childhood intervention access, education adjustments and judicious psychopharmacology. In Australia, NDIS and school interfaces shape service access after diagnosis — teach principles of functional support needs, not invented form codes. In Aotearoa New Zealand, uphold Te Tiriti principles and whānau-centred planning. Physical health monitoring with antipsychotics is non-negotiable. [1] [2]
NICE pathways for autism recognition/diagnosis and support/management emphasise multi-professional assessment, post-diagnostic support, and caution with medication for core features. UK exam answers should name multiagency assessment and educational support, not US brand-only frameworks. [20]
AAP clinical report (Hyman 2020) and AACAP practice parameter remain core references. FDA-labelled indications for risperidone and aripiprazole for irritability associated with autistic disorder drive many exam items — know the indication, not off-label improvisation for core social deficits. [1] [2] [8] [9]
Canadian paediatric pathways emphasise multidisciplinary diagnosis, educational supports and family-centred care aligned with the same DSM construct and early-support principles. [1] [20]
Landmark list for viva: Hyman AAP 2020; AACAP Volkmar 2014; Lai Lancet 2014; Maenner ADDM; Zeidan prevalence; Sandin heritability; McCracken RUPP risperidone; Owen/Marcus aripiprazole; Dawson ESDM; Green/Pickles PACT; Bearss parent training; King citalopram negative trial; Fung meta-analysis; Simonoff comorbidity; Schaefer genetics; Lord Lancet Commission; Hirvikoski mortality; Cassidy suicide; Reichow EIBI; Scahill guanfacine; Gringras melatonin. [1] [8] [11] [20]
Exam Pearls
[1] [8] [9] [22]S.P.E.C.T.R.U.M.
Recognition leaf versus this assessment/management leaf
Recognition/surveillance/screening detail belongs on Social communication concerns and autism recognition. This page owns confirmation, medical evaluation, intervention ladder, irritability pharmacology, crisis care and long-term multiagency planning. [1] [18]
This page owns ASD assessment and management depth. Cross-link ADHD, intellectual disability, sensory processing, early intervention, neurodiversity-affirming care and transition leaves rather than hiding second full chapters here. [1] [20]
References
- [1]Hyman SL Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics, 2020.PMID 31843864
- [2]Volkmar F Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 2014.PMID 24472258
- [3]Lai MC Autism. Lancet, 2014.PMID 24074734
- [4]Maenner MJ Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. MMWR. Surveillance summaries, 2023.PMID 36952288
- [5]Zeidan J Global prevalence of autism: A systematic review update. Autism research, 2022.PMID 35238171
- [6]Sandin S The Heritability of Autism Spectrum Disorder. JAMA, 2017.PMID 28973605
- [7]Bai D Association of Genetic and Environmental Factors With Autism in a 5-Country Cohort. JAMA psychiatry, 2019.PMID 31314057
- [8]McCracken JT Risperidone in children with autism and serious behavioral problems. The New England journal of medicine, 2002.PMID 12151468
- [9]Owen R Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder. Pediatrics, 2009.PMID 19948625
- [10]Marcus RN Aripiprazole in the treatment of irritability in pediatric patients (aged 6-17 years) with autistic disorder: results from a 52-week, open-label study. Journal of child and adolescent psychopharmacology, 2011.PMID 21663425
- [11]Dawson G Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model. Pediatrics, 2010.PMID 19948568
- [12]Green J Parent-mediated communication-focused treatment in children with autism (PACT): a randomised controlled trial. Lancet, 2010.PMID 20494434
- [13]Pickles A Parent-mediated social communication therapy for young children with autism (PACT): long-term follow-up of a randomised controlled trial. Lancet, 2016.PMID 27793431
- [14]Bearss K Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: a randomized clinical trial. JAMA, 2015.PMID 25898050
- [15]King BH Lack of efficacy of citalopram in children with autism spectrum disorders and high levels of repetitive behavior: citalopram ineffective in children with autism. Archives of general psychiatry, 2009.PMID 19487623
- [16]Fung LK Pharmacologic Treatment of Severe Irritability and Problem Behaviors in Autism: A Systematic Review and Meta-analysis. Pediatrics, 2016.PMID 26908468
- [17]Simonoff E Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 2008.PMID 18645422
- [18]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [19]Schaefer GB Clinical genetics evaluation in identifying the etiology of autism spectrum disorders: 2013 guideline revisions. Genetics in medicine, 2013.PMID 23519317
- [20]Lord C The Lancet Commission on the future of care and clinical research in autism. Lancet, 2022.PMID 34883054
- [21]Hirvikoski T Premature mortality in autism spectrum disorder. The British journal of psychiatry, 2016.PMID 26541693
- [22]Cassidy S Understanding and prevention of suicide in autism. The Lancet. Psychiatry, 2017.PMID 28551299
- [23]Reichow B Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). The Cochrane database of systematic reviews, 2018.PMID 29742275
- [24]Scahill L Extended-Release Guanfacine for Hyperactivity in Children With Autism Spectrum Disorder. The American journal of psychiatry, 2015.PMID 26315981
- [25]Gringras P Melatonin for sleep problems in children with neurodevelopmental disorders: randomised double masked placebo controlled trial. BMJ, 2012.PMID 23129488