Paeds · growth-development-and-behaviour
Behavioural management of defiance and oppositional behaviours
Also known as Oppositional defiant disorder management · Parent training for defiance · Noncompliance in children · Disruptive behaviour parent management · ODD behavioural treatment
Fellowship guide to behavioural management of defiance and oppositional behaviours in general paediatrics: normative noncompliance versus ODD and CD, coercive cycles, multi-informant assessment, parent training first-line, school plans, ADHD comorbidity, limited medication role, safeguarding and regional guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent says, “He never does what he’s told.” The teacher emails about office referrals. The child looks ordinary on the examination couch. Your job is not to argue about whether the child is “naughty.” Your job is to run a behavioural management plan for defiance and oppositional behaviours: decide what is age-expected, what is impairing, what maintains the pattern, and which first-line skills change it. [4] [10]
Defiance here means persistent noncompliance, arguing, and hostile conflict with authority that impairs family, school or peer function. Oppositional defiant disorder (ODD) is the named syndrome when angry/irritable mood, argumentative/defiant behaviour and vindictiveness form a lasting pattern with clear impairment — classically six months or more and severity judged by how many settings are affected. Not every tantrum is ODD. Not every ODD becomes conduct disorder (CD). [4] [16]
This page owns management in general paediatrics: assessment spine, parent training, school plans, comorbidity sequencing and the limited role of medication. Acute tantrum coaching and emotion-dysregulation detail live on the linked tantrums page. Deep ABC functional analysis technique lives on the behavioural-assessment page. Full ADHD ladders live on the ADHD page. Cross-link them. Do not hide second textbooks here. [10] [18]
Clinic spine for defiance
Is anyone unsafe now?
If yes, de-escalate, protect, safeguard — do not start a parenting lecture in a crisis.
Who sees what?
Child, caregivers, school — settings, onset, impairment.
What maintains it?
Coercive cycle, ADHD, language, sleep, trauma, learning, peer ecology.
First-line skills
Behavioural parent training plus school consistency; treat ADHD if present.
Step up only if needed
Specialist behavioural/CAMHS, intensive multi-system care, limited medication for severe aggression.
Classification
Classify three things before you open a treatment plan: severity of the pattern, developmental band, and whether serious rule-breaking has started. [4] [16]
Normative noncompliance versus ODD-range pattern
Toddlers test limits. Preschoolers argue. That is development, not disease. You move toward an ODD-range formulation when the pattern is frequent, persistent, multi-setting, and impairs relationships or learning — not when a single stressed parent has a hard Tuesday. [4] [10]
ODD versus conduct disorder
ODD is about mood and defiance toward authority. CD adds aggression to people or animals, destruction of property, deceit or theft, and serious violations of rules. ODD can precede or co-occur with CD, but they are not the same diagnosis. Examiners punish candidates who equate them. [4] [16] [20]
Stringaris dimensions
Oppositionality is not one lump. Stringaris and Goodman separate irritable, headstrong and hurtful dimensions. They have different longitudinal predictions: irritability tracks more toward internalising pathways; headstrong and hurtful track more toward externalising and conduct risk. This split changes what you watch for, not only what you name. [2] [3]
Severity by settings
Mild patterns may be confined largely to one setting. Moderate and severe patterns cross home, school and community. Severity guides intensity of intervention and multiagency need, not how loudly the child argues in clinic. [4]
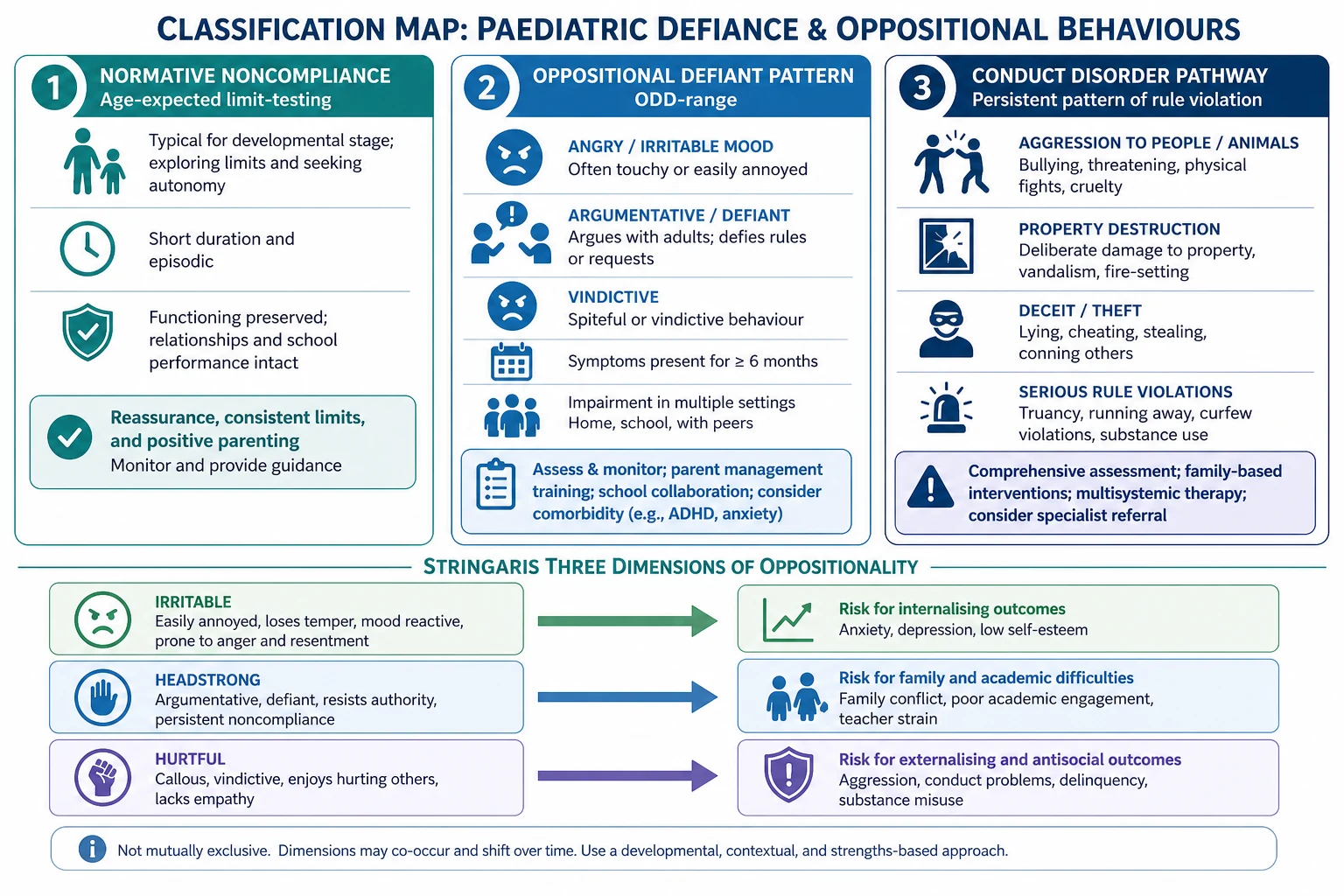
Read the figure like this: if you only hear “defiant,” you will over-treat some toddlers and under-treat emerging CD. Name the band. [2] [4]
Epidemiology & Risk Factors
ODD is common enough that every general paediatrician will manage it. In the National Comorbidity Survey Replication, Nock and colleagues estimated lifetime prevalence of ODD around one in ten people, with substantial comorbidity and variable persistence into adulthood. Male predominance is clearer for aggressive CD phenotypes; girls may show more relational aggression that adults under-detect. [1] [16]
Cross-cultural prevalence estimates for ODD and CD vary, but Canino’s synthesis shows method often drives the scatter more than geography. Do not invent a local “epidemic” from one school’s referral spike without looking at definitions and access. [15]
Risk clusters, not single causes. Harsh inconsistent parenting, coercive family cycles, peer delinquency, neighbourhood disadvantage, prenatal tobacco exposure, ADHD, and maltreatment all raise risk. Callous-unemotional traits mark a higher-risk pathway within externalising disorders. Poverty and racism in systems delay access to parent training — that is a clinical equity problem, not background noise. [9] [13] [16]
Early childhood emotional and behavioural problems are common enough that Gleason’s AAP clinical report places the paediatric medical home as a front-line leader, not a spectator waiting for CAMHS. [10]
Pathophysiology
Why does shouting make next week worse? Because many oppositional patterns are learned and maintained, not merely “chosen.” [9]
Coercive family process
In the Oregon-model lineage, parent and child train each other. A parent issues a demand. The child refuses or escalates. The parent withdraws the demand (escape for the child) or explodes (modelling aggression). Short-term peace is bought. Long-term noncompliance is strengthened. Parenting then becomes more harsh, more inconsistent, or more avoidant. That cycle is the mechanism you treat. [9] [11]
Social learning and peers
Children also learn from observed aggression and from delinquent peer groups. Adolescence can amplify opportunity for rule-breaking even when early temperament was not extreme. [8] [16]
Moffitt dual pathways
Moffitt’s developmental taxonomy separates life-course-persistent antisocial behaviour (early onset, neurodevelopmental and adversity load, higher adult risk) from adolescence-limited pathways (peer and maturity-gap driven, more likely to desist). You do not need a forensic lab to use the idea: early multi-problem onset with ADHD and harsh environments deserves earlier multi-system intensity than a late peer-clustered spurt. [8]
ADHD and language pathways
Impulsivity and working-memory limits make “won’t” look like “can’t wait.” Language disorder makes instructions incomprehensible; the child who does not understand is mislabelled oppositional. Sleep debt, pain, hunger and sensory overload raise the probability of noncompliance without proving wilful spite. [18] [10]
Stringaris dimensions as mechanism-linked phenotypes
Irritability, headstrongness and hurtfulness are not cosmetic subtypes. They track different outcome risks and should shape what you monitor (mood and anxiety versus conduct and peer harm). [2] [3]
Callous-unemotional traits
Reduced guilt and empathy, and reward-dominant learning, mark a pathway with different treatment response profiles. Frick’s review is the conceptual anchor. In general paediatrics, treat this as a risk flag for intensity and multiagency care — not as a casual brand on a preschooler after one visit. [13]
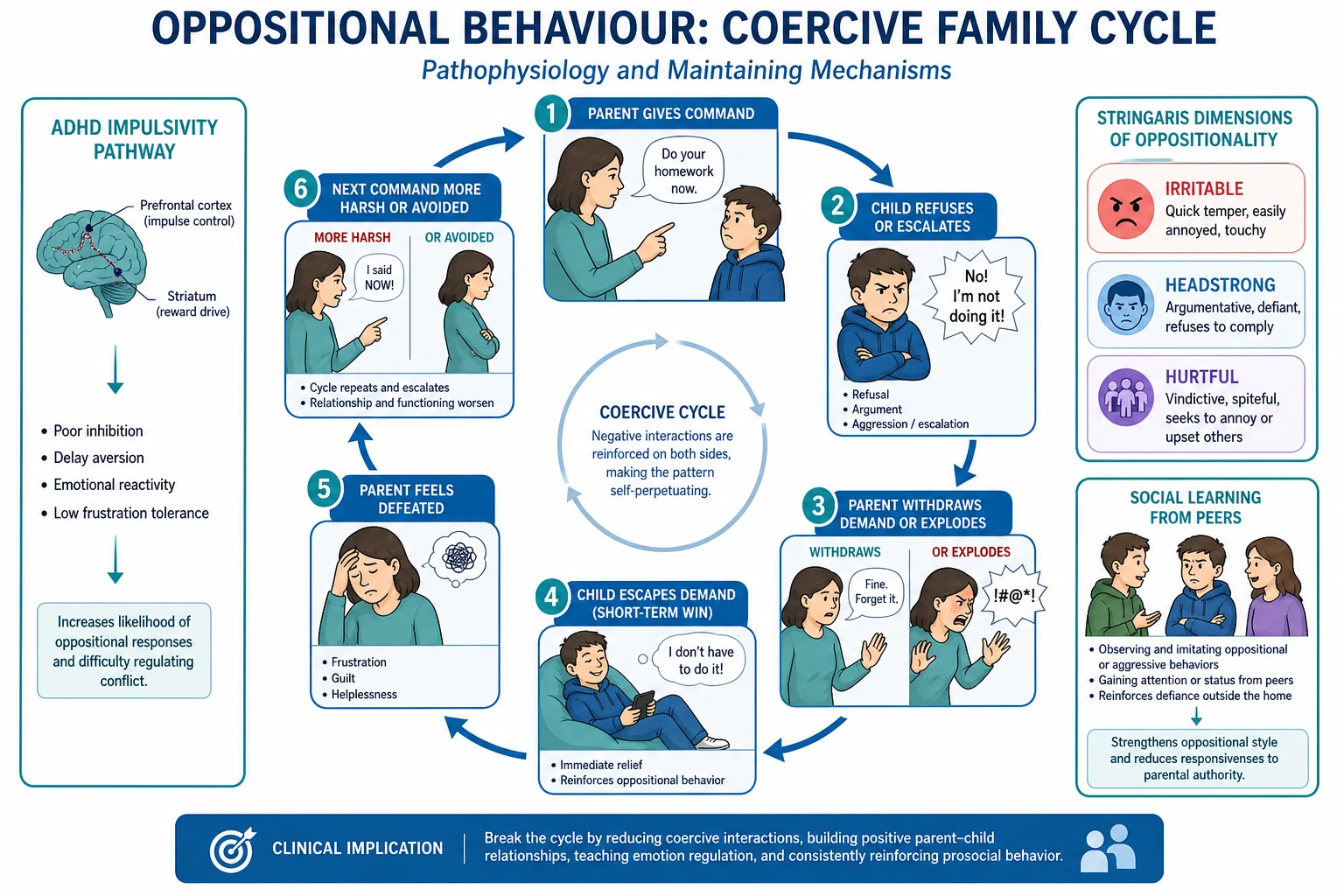
Read the figure like this: if your plan only punishes the child and never changes parent–child contingencies, you are treating the wrong node. [9] [11]
Clinical Presentation
How families walk in
- “Nothing works. Time-out makes it worse.”
- “He is an angel at grandma’s and a nightmare at home.”
- “School says he is fine; we are the problem.”
- “She argues every instruction for an hour.”
- “He hits his brother when told no.”
Age bands
Preschool: frequent temper loss, defiance of routine care (dressing, leaving the park), spiteful acts that blow up daycare. Gleason’s early-childhood framing keeps you from either medicalising every meltdown or ignoring impairing patterns. [10]
School-age ODD-range: chronic arguing, blame-shifting, teacher conflict, unfinished work, recess fights without clear criminal rule-breaking. [4] [16]
Adolescent: authority conflict plus peer delinquency, truancy, substance use, or justice contact — watch for CD criteria. [20] [8]
Atypical and easy-to-miss presentations
Opposition only with one caregiver can still be real if that dyad runs the coercive cycle. Girls may show relational aggression that schools under-code. Trauma-driven hyperarousal looks “defiant” when the child is actually unsafe. ASD rigidity and sensory meltdowns look “wilful” when demands are poorly adapted. [4] [10]
Collateral mismatch
Home-only versus school-only impairment changes formulation. Multi-setting impairment raises ODD confidence and treatment intensity. Single-setting patterns push you to look at that environment’s contingencies and skills. [4]
Differential Diagnosis
You are not choosing one label from a list. You are ranking what best explains the noncompliance and what must be treated first. [4]
| Pattern | What tips you toward it | First move |
|---|---|---|
| Normative noncompliance | Age-expected, limited impairment, short history | Anticipatory guidance and ordinary consistency |
| ODD-range | Multi-month, multi-setting, angry/defiant/vindictive cluster | Parent training + school plan |
| ADHD (often comorbid) | Impulsive noncompliance, inattention, hyperactivity across tasks | ADHD assessment and treatment pathway |
| Language/hearing/learning | Does not follow multi-step instructions; academic failure | Hearing, speech-language, psychoeducation |
| Anxiety/PTSD | Avoidance, hyperarousal, startle, trauma history | Safety, trauma-informed care, anxiety treatment |
| ASD | Rigidity, sensory triggers, social-communication profile | Adapt demands; autism pathway as indicated |
| Depression / severe chronic irritability | Mood change, anhedonia, or DMDD-range outbursts | Mood assessment; do not pure-ODD treat |
| Conduct disorder | Aggression, theft, destruction, serious rule breaks | Multiagency intensity; CD parameters |
| Substance effects (adolescents) | New behaviour change, peer context, intoxication signs | Substance assessment and safety |
| Safeguarding presentation | Injury patterns, fear, secrecy, caregiver coercion | Protect first; behaviour plan later |
Clinical & Bedside Assessment
Multi-informant history
Ask the same timeline of caregivers, the child (developmentally adapted), and school. Onset age, settings, frequency, triggers, parent responses, and what has already been tried matter more than a single “how bad is it from 1 to 10.” [4]
Map the coercive cycle at the bedside
What is the demand? What does the child do? What does the adult do next? Who “wins” the short game? That five-minute map often explains more than a rating scale. [9]
Comorbidity screen
ADHD, learning and language, sleep, mood, anxiety, trauma, substances (adolescents), autism features when relevant. Wolraich’s ADHD guideline is the operational bridge when attention and hyperactivity co-travel with defiance. [18] [4]
Risk and safeguarding
Violence, weapons, absconding, self-harm, exploitation, sibling injury, and caregiver violence. Mandatory reporting thresholds are jurisdiction-specific; the clinical duty to protect is not optional. [4] [20]
Observation and tools
Watch warmth, commands, follow-through and child response in the room when safe. Structured tools (SDQ, CBCL externalising bands, Conners when ADHD is suspected) support, not replace, diagnosis. [4]
Shared problem list
Agree the top two functional goals with the family (for example: morning routine without hitting; fewer office referrals). Plans without shared goals die on the fridge. [5] [11]
Investigations
There is no blood test for defiance. Investigations serve differential diagnosis and pre-treatment safety, not the ODD label. [4]
- Hearing and vision when communication or attention is in question.
- Speech-language and psychoeducational assessment when school failure or comprehension concerns dominate.
- Developmental evaluation when global delay or autism is plausible.
- Drug screen when adolescent substance use is clinically suspected.
- Metabolic baseline and ECG planning only if specialist pharmacotherapy for severe aggression is truly contemplated.
- EEG or neuroimaging only with neurological red flags — never “because he is oppositional.” [4] [6]
School data are investigations: attendance, office referrals, learning plans, exclusions. Youth justice or welfare collateral, when involved, is obtained lawfully and with appropriate consent frameworks. [4] [6]
Management — Resuscitation
Acute severe aggression is a safety problem first. De-escalate. Protect others. Use local seclusion/restraint policy only when needed and trained. Convert to ED pathways if the child or environment cannot be made safe. Do not start a parenting curriculum during active violence. [4] [6]
Immediate safeguarding takes priority when abuse, neglect, or imminent serious harm appears. Create a crisis plan with family and school: who to call, when to leave, how to reduce audience and weapons access. Do not medicate as the sole acute fix for a parenting skill gap or untreated ADHD. [6] [18]
Medical mimics (delirium, intoxication, acute encephalopathy) convert the visit from “behaviour clinic” to medical resuscitation. [4]
Management — Definitive & Stepwise
Step 1 — Behavioural parent training first-line
High-quality psychosocial treatments for disruptive behaviour are well established. Eyberg’s evidence review and later Kaminski updates place behavioural parent programmes at the centre. Core effective components from Kaminski’s meta-analysis include positive parent–child interaction training, consistent discipline responses, emotional communication, and practice with the child rather than lecture-only groups. [17] [11] [19]
Programme families you should be able to name at viva: [17] [9]
- Oregon model / behaviour family therapy lineage — contingency management and coercive-cycle interruption at scale. [9]
- Incredible Years-type group parent training — widely studied early-onset conduct problem pathway. [17]
- Parent–Child Interaction Therapy (PCIT) — especially for younger children with live coaching of parent skills. [17]
Scott’s multicentre BMJ trial showed parenting groups work in real clinical practice for childhood antisocial behaviour — not only in boutique research clinics. That is the line examiners want. [5]
Step 2 — School behavioural plan
Same rules across adults beat perfect rules used by one adult. Clear, calm, specific commands; contingent praise; planned responses to noncompliance; reduced public power struggles; learning supports if academic failure fuels conflict. Collaborative problem-solving approaches can adjunct, not replace, contingency skills when rigidity and lagging skills dominate. [4] [19]
Step 3 — Treat comorbid ADHD
When ADHD is present, treat it. Wolraich’s AAP clinical practice guideline is the paediatric operational standard for ADHD care. Stimulant and non-stimulant pathways often reduce secondary oppositional symptoms driven by impulsivity. Do not withhold ADHD treatment because “the real problem is behaviour.” [18] [6]
Step 4 — Specialist and multi-system intensity
Severe, multiagency, or justice-involved conduct patterns may need intensive family- and community-based models. Multisystemic therapy (MST) is the named exemplar: home-based, ecological, high-intensity work across family, school and peers. Henggeler’s overviews are the viva anchors. [12] [20]
Step 5 — Limited medication role
Medication is not first-line for core ODD defiance. Canadian guidance (Gorman et al.) prioritises psychosocial care and ADHD treatment; pharmacotherapy for disruptive/aggressive behaviour is selective, specialist-led, and monitored. [6]
Risperidone has RCT evidence for reducing conduct and disruptive behaviours in children with subaverage IQs (Snyder et al.). TOSCA-related analyses integrate stimulant plus adjunctive antipsychotic strategies for severe childhood aggression in specialist contexts. These are not licences for primary-care antipsychotic starts for mild arguing. Monitor metabolic effects, extrapyramidal symptoms and prolactin-related issues when antipsychotics are used. Avoid benzodiazepines as behaviour management. [7] [14] [6]
Follow-up metrics
Fewer injuries and office referrals, improved morning routines, warmer parent–child interaction, better learning access, and safety. Review fidelity of strategies — not only “is he still naughty?” [5] [11]
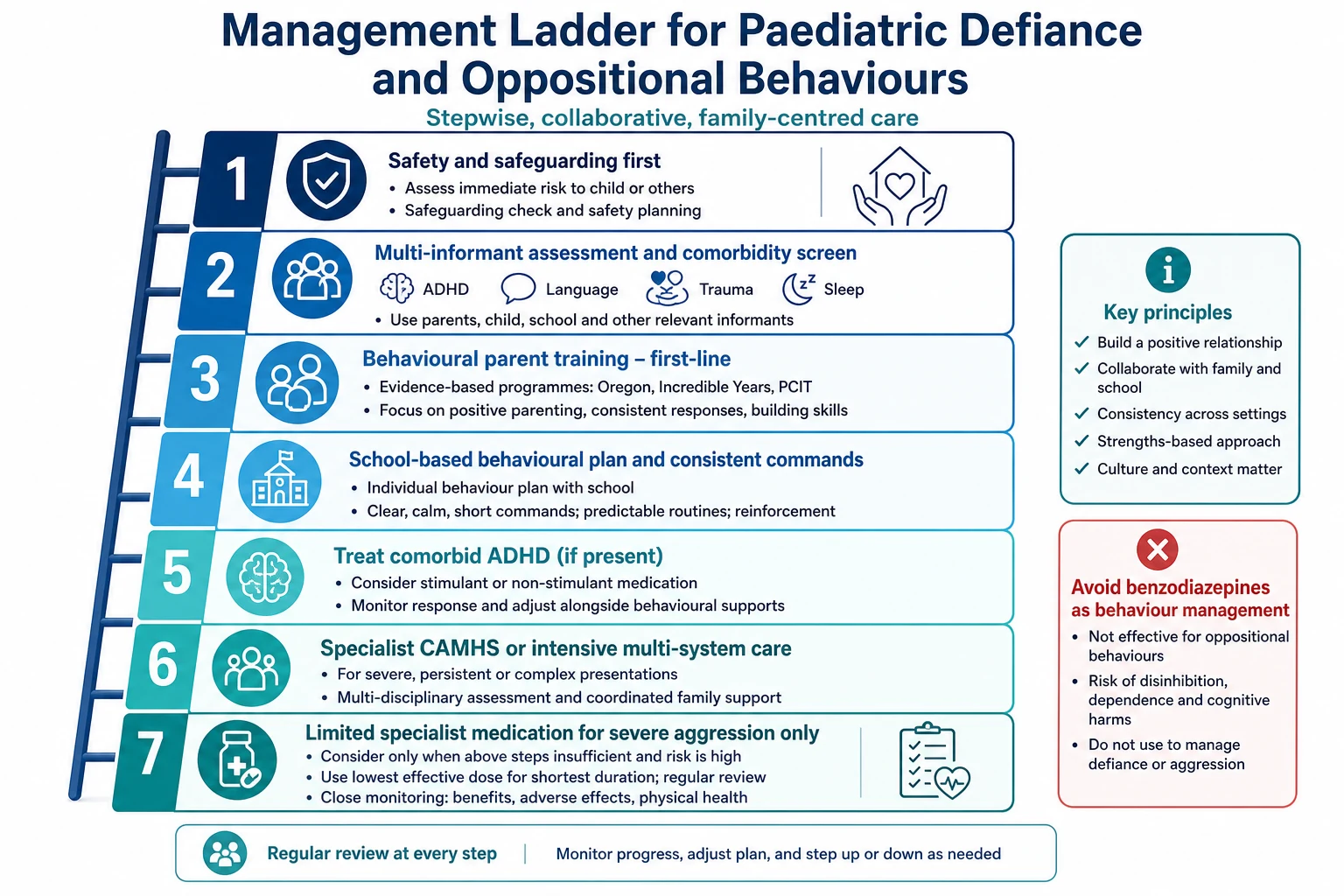
Read the figure like this: skipping to medication because parent training “is hard to access” is a system failure you should name and advocate around, not a clinical first principle. [5] [6]
Specific Subtypes & Scenarios
Preschool ODD-range
Lead with PCIT or equivalent parent coaching. Avoid early antipsychotic for defiance alone. Support daycare consistency. [17] [10]
ODD + ADHD
Assess and treat ADHD in parallel with parent training. Expect partial improvement in oppositional symptoms when impulsivity falls; residual coercive cycles still need skills work. [18] [6]
Language-driven secondary opposition
If the child cannot parse instructions, speech-language intervention and simplified commands come first. Labelling ODD alone fails the child. [4]
Trauma-informed presentation
Safety and stabilisation before pure compliance drills. Coercive-looking behaviour may be fear. Safeguarding overrides behaviour contracts. [4] [10]
Emerging CD / CU-trait risk
Escalate to multiagency care. Parent handouts alone are inadequate. Use CD practice-parameter thinking for aggression, theft and serious rule-breaking. [20] [13]
Adolescent peer-delinquency pathway
Address peer ecology, opportunity structure, substances and school exclusion cycles. Adolescence-limited patterns may desist with changed context; do not assume destiny. [8] [12]
Intellectual disability with disruptive behaviour
Environmental supports, communication systems and specialist behaviour plans. Historical risperidone evidence is strongest in subaverage IQ disruptive disorders under specialist care — not a general paediatric default. [7] [6]
ASD with demand avoidance phenotype
Adapt demands, sensory load and predictability. Do not run a pure ODD protocol that ignores autism. Cross-link neurodiversity-affirming care. [4]
Looked-after / kinship care
Incomplete history, placement moves and trauma load are common. Dual medical and relational assessment; avoid blaming the current carer alone. [10]
Rural and telehealth delivery
Parent coaching and school liaison can run by telehealth when travel is the barrier. Fidelity still needs live practice, not only pamphlets. [5] [19]
Complications & Pitfalls
- Labelling cultural assertiveness or bilingual family dynamics as ODD. [15]
- Missing ADHD, hearing loss, language disorder or trauma. [18] [4]
- Antipsychotics as first-line for mild defiance. [6]
- Blaming the child while ignoring the coercive cycle. [9]
- Punishment-only plans that escalate coercion. [11]
- Open-loop school exclusions with no review date. [4]
- Equating CD with inevitable adult antisocial personality. [8]
- Metabolic neglect on risperidone. [6] [7]
- Diagnostic overshadowing in disability. [7]
- Failing mandatory reporting when safeguarding thresholds are met. [4]
Prognosis & Disposition
Many ODD-range presentations improve with high-quality parent training and school consistency. A subset progresses toward CD. Early multi-problem onset with ADHD, adversity and callous-unemotional traits carries higher adult externalising and substance risk along life-course-persistent lines. Adolescence-limited pathways often improve when peer and opportunity structures change. [5] [8] [13] [1]
Disposition ladder: primary-care structured plan → specialist behavioural/CAMHS → intensive multi-system models for complex CD. Safety-net for escalating aggression, self-harm, weapons, or safeguarding. Transition planning matters for adolescents with persistent multi-system impairment. Measure outcomes in function, not only in labels. [12] [4]
Special Populations
Indigenous and culturally diverse families: use culturally safe parenting programmes; avoid deficit framing of parenting styles; partner with community services. [15]
Migrant and refugee families: professional interpreting for parent training — a tool in the wrong language is not the validated intervention. [5]
Neurodisability and autism: adapt communication and sensory load; specialist behaviour support. [7]
Out-of-home care and youth justice: multiagency plans, placement stability, and trauma-informed care. [12] [20]
Socioeconomic disadvantage: transport, childcare and appointment timing decide whether parent training is real or theoretical. Advocate for access. [5]
Rural/remote: telehealth coaching and school-based delivery. [19]
Evidence, Guidelines & Regional Differences
| Anchor | What it gives you |
|---|---|
| Steiner & Remsing AACAP ODD parameter (2007) | Assessment breadth; psychosocial first-line framing |
| Steiner AACAP CD parameters (1997) | Exam-cited CD management skeleton |
| Scott BMJ 2001 | Parenting groups work in ordinary clinical practice |
| Kaminski 2008 / 2017 | Which parent-training components matter; evidence updates |
| Dishion Oregon model 2016 | Coercive-cycle therapy lineage at system scale |
| Eyberg 2008 | Evidence-based psychosocial treatments for disruptive behaviour |
| Henggeler MST overviews | Intensive multi-system care for severe complex cases |
| Gorman Canadian 2015 | Pharmacotherapy principles: selective, monitored, ADHD-first |
| Snyder 2002; TOSCA integration | Risperidone/specialist aggression evidence boundaries |
| Wolraich AAP ADHD 2019 | Comorbid ADHD operational care |
| Stringaris 2009 papers | Dimensional oppositionality and outcomes |
| Nock 2007; Canino 2010 | Epidemiology and cross-cultural method caution |
In Australia and Aotearoa New Zealand, general paediatricians often start formulation and parent-skill coaching in the medical home while linking to public parenting programmes, CAMHS/ICAMHS, school behaviour supports and disability services. Access waitlists are a clinical risk: interim safety plans and school liaison cannot wait for the perfect programme. Youth justice and child-protection interfaces are jurisdiction-specific — know your mandatory reporting pathway. [4] [5]
Canadian Gorman guidance is the cleanest named pharmacotherapy synthesis for disruptive/aggressive behaviour with ADHD/ODD/CD. Use it when examiners ask “when is a medicine justified?” Psychosocial care remains first-line globally. [6] [5]
Controversies worth defending: ODD overdiagnosis; antipsychotic creep for mild defiance; clinical utility of CU traits in general paediatrics; school exclusion as iatrogenic harm that maintains the very behaviour it punishes. [6] [13] [4]
Exam Pearls
- ODD ≠ CD. CD needs criterion behaviours beyond oppositionality. [4] [16]
- Parent training first; medication is adjunct for severe aggression or ADHD — not a defiance cure. [5] [6]
- Stringaris: irritable vs headstrong vs hurtful — different outcome bets. [2] [3]
- Moffitt LCP vs adolescence-limited for trajectory questions. [8]
- Coercive cycle: short-term escape reinforces long-term worse behaviour. [9]
- Treat comorbid ADHD; oppositional symptoms often fall. [18]
- Multi-informant collateral is non-negotiable. [4]
- PCIT for younger children; group parent training widely evidenced; MST for severe complex CD. [17] [12]
- Avoid benzos for behaviour; monitor metabolic effects if antipsychotic used. [6]
- Safeguarding and cultural safety sit inside every behaviour plan. [4] [15]
PARENTS
Viva one-liner set
Define ODD without calling every tantrum a disorder. Name three parent-training lineages. Explain the coercive cycle in 20 seconds. Say when risperidone is and is not justified. Distinguish ODD from CD. Treat ADHD when comorbid. Never leave a positive safeguarding signal for “behaviour clinic next month.” [4] [9] [6] [18]
References
- [1]Nock MK Lifetime prevalence, correlates, and persistence of oppositional defiant disorder: results from the National Comorbidity Survey Replication. J Child Psychol Psychiatry, 2007.PMID 17593151
- [2]Stringaris A Three dimensions of oppositionality in youth. J Child Psychol Psychiatry, 2009.PMID 19166573
- [3]Stringaris A Longitudinal outcome of youth oppositionality: irritable, headstrong, and hurtful behaviors have distinctive predictions. J Am Acad Child Adolesc Psychiatry, 2009.PMID 19318881
- [4]Steiner H Practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry, 2007.PMID 17195736
- [5]Scott S Multicentre controlled trial of parenting groups for childhood antisocial behaviour in clinical practice. BMJ, 2001.PMID 11473908
- [6]Gorman DA Canadian guidelines on pharmacotherapy for disruptive and aggressive behaviour in children and adolescents with attention-deficit hyperactivity disorder, oppositional defiant disorder, or conduct disorder. Can J Psychiatry, 2015.PMID 25886657
- [7]Snyder R Effects of risperidone on conduct and disruptive behavior disorders in children with subaverage IQs. J Am Acad Child Adolesc Psychiatry, 2002.PMID 12218423
- [8]Moffitt TE Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev, 1993.PMID 8255953
- [9]Dishion T The Oregon Model of Behavior Family Therapy: From Intervention Design to Promoting Large-Scale System Change. Behav Ther, 2016.PMID 27993335
- [10]Gleason MM Addressing Early Childhood Emotional and Behavioral Problems. Pediatrics, 2016.PMID 27940734
- [11]Kaminski JW A meta-analytic review of components associated with parent training program effectiveness. J Abnorm Child Psychol, 2008.PMID 18205039
- [12]Henggeler SW Multisystemic Therapy: Clinical Overview, Outcomes, and Implementation Research. Fam Process, 2016.PMID 27370172
- [13]Frick PJ Research review: the importance of callous-unemotional traits for developmental models of aggressive and antisocial behavior. J Child Psychol Psychiatry, 2008.PMID 18221345
- [14]Barterian JA Clinical Implications From the Treatment of Severe Childhood Aggression (TOSCA) Study: A Re-Analysis and Integration of Findings. J Am Acad Child Adolesc Psychiatry, 2017.PMID 29173736
- [15]Canino G Does the prevalence of CD and ODD vary across cultures? Soc Psychiatry Psychiatr Epidemiol, 2010.PMID 20532864
- [16]Loeber R Oppositional defiant and conduct disorder: a review of the past 10 years, part I. J Am Acad Child Adolesc Psychiatry, 2000.PMID 11128323
- [17]Eyberg SM Evidence-based psychosocial treatments for children and adolescents with disruptive behavior. J Clin Child Adolesc Psychol, 2008.PMID 18444059
- [18]Wolraich ML Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics, 2019.PMID 31570648
- [19]Kaminski JW Evidence Base Update for Psychosocial Treatments for Disruptive Behaviors in Children. J Clin Child Adolesc Psychol, 2017.PMID 28459280
- [20]Steiner H Practice parameters for the assessment and treatment of children and adolescents with conduct disorder. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry, 1997.PMID 9334568