Paeds · growth-development-and-behaviour
Developmental delay: global diagnostic approach
Also known as Global developmental delay · GDD · Developmental delay multi-domain · Developmental delay diagnostic evaluation
Fellowship diagnostic approach to global developmental delay: multi-domain pattern recognition, threat-first assessment, hearing and vision, evolving genetic testing tiers, selective metabolic and imaging tests, early intervention without waiting for labels, and exam-ready communication.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A parent says, “Our two-year-old still has almost no words and cannot stack blocks like the cousin his age.” That sentence already spans language and fine-motor domains. Your job is not to invent a gene name on day one. Your job is to decide whether this is true multi-domain delay, how dangerous it is today, what treatable contributors you must not miss, and how to help the child while results are pending. [1] [7]
Tool psychometrics and formal test administration live on Developmental assessment: history, examination and standardised tools. True loss of skills belongs on the regression page. Isolated motor, speech or autism pathways have their own leaves. This page owns the global diagnostic approach. [1] [7]
G.L.O.B.A.L. D.D.
Overview & Definition
Global developmental delay (GDD) is a clinical descriptor used mainly in children younger than about five years. It means the child is significantly behind expected skills in two or more developmental domains: gross motor, fine motor, speech and language, cognition, social and personal, or activities of daily living. It is a problem representation. It is not a molecular diagnosis. [1] [2]
Intellectual developmental disorder (IDD), often still called intellectual disability in older papers, is a related but later label. IDD needs deficits in intellectual functioning and adaptive behaviour that begin in the developmental period. Many toddlers with GDD will later meet IDD criteria. Some will not. Do not force an adult-style IQ label on a child who is still too young for valid cognitive testing. Keep the language honest for age. [1] [6]
Moeschler and Shevell’s AAP clinical report remains a core teaching source for comprehensive evaluation of the child with ID or GDD: history, examination, family pedigree, and a structured laboratory approach. Newer AAP and ACMG guidance update the genetic testing tier itself. You need both layers: how to evaluate the child, and which genomic tests are now first-line. [1] [5] [6]
Classification
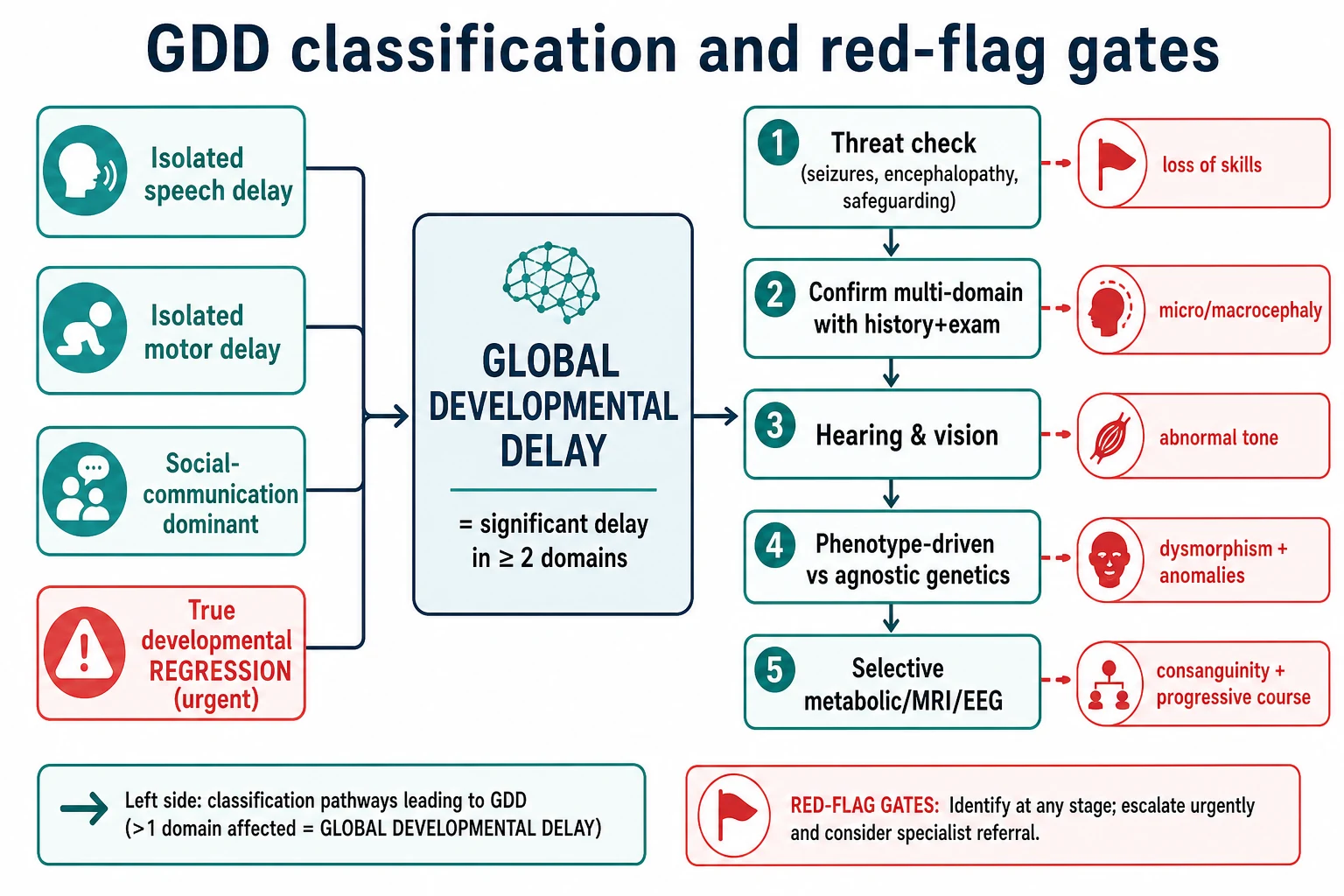
Think in three layers: pattern, threat, and aetiology pathway. [1] [6]
Pattern answers: is this truly global? Isolated speech delay is common and has a different first-line path. Isolated motor delay with hypertonia may be an early cerebral palsy story. Social-communication-dominant concerns need autism-specific assessment in parallel. True regression — skills gained then lost — is urgent and not ordinary GDD. [1] [7]
Threat answers: how dangerous is today? Seizures, reduced consciousness, progressive course, severe microcephaly with encephalopathy, or safeguarding danger outrank a calm outpatient genetics plan. [1] [14]
Aetiology pathway answers: phenotype-driven or agnostic? If the examination screams a recognisable syndrome, congenital anomalies cluster, or a family history points to a specific inheritance pattern, test in a directed way and involve genetics early. If the child is non-dysmorphic with unexplained multi-domain delay, use an agnostic genomic strategy informed by current AAP and ACMG guidance. [1] [5] [6]
Severity language in clinic is pragmatic. Mild multi-domain lag in a well child can start in the community with tight review. Moderate or severe delay, abnormal neurology, or social risk needs faster specialist input and broader same-day supports. Severity does not equal aetiology. A mild-looking delay can still have a genetic diagnosis that changes recurrence counselling. [1] [6]
Epidemiology & Risk Factors
GDD is common enough that every general paediatrician will assess it repeatedly. Prevalence estimates vary with definition, screening access and cultural recognition of delay. What matters for exams is risk structure, not a single magic percentage. [1] [7]
Perinatal risks include prematurity, hypoxic–ischaemic injury, congenital infection, growth restriction and neonatal encephalopathy. Family risks include consanguinity, previous children with developmental disability, and X-linked patterns that raise fragile X concern in selected families. [1] [3]
Social risks matter twice: they can contribute to delayed skill acquisition, and they can block access to assessment and therapy. Poverty, food insecurity, caregiver mental health strain, out-of-home care and family violence all change detection and support. Language discordance without a professional interpreter produces false reassurance and incomplete histories. [10] [12]
Missed hearing or vision impairment is a classic reversible contributor. A failed newborn hearing screen that never completed diagnostic audiology can present later as “speech delay” that is actually multi-domain lag. Do not close the case until sensory testing is done or already reliable. [1] [7]
Pathophysiology
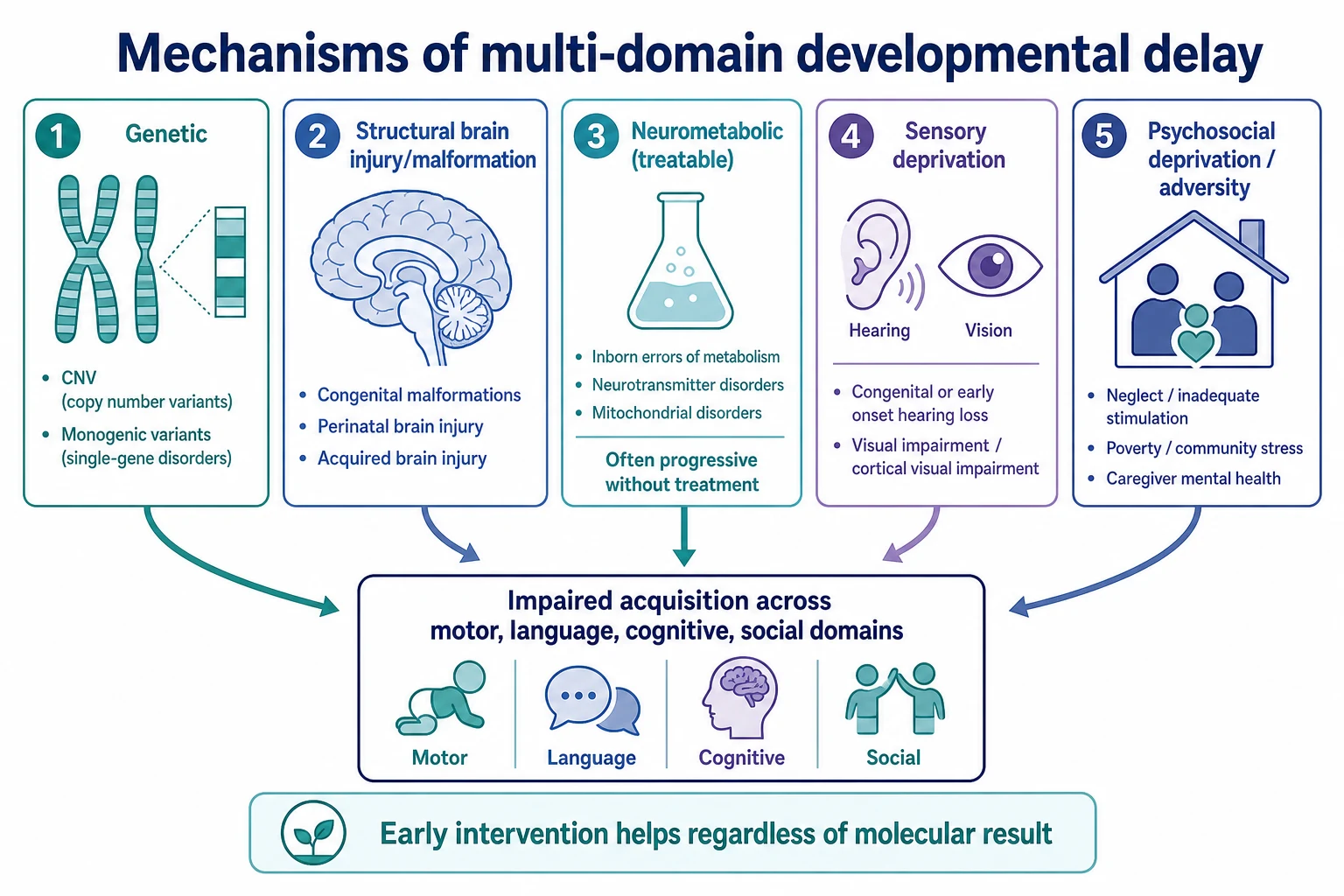
Development is the acquisition of skills on a biological and environmental scaffold. When that scaffold fails in more than one system, multi-domain delay appears. [1]
Genetic mechanisms include chromosomal aneuploidy, copy-number variants detectable by microarray, and monogenic disorders better detected by exome or genome sequencing. These lesions can disrupt neuronal migration, synaptic function, myelination or broader developmental programmes. Yield of chromosomal microarray in unexplained developmental disability historically sat well above standard karyotype for submicroscopic CNVs, which is why Miller and colleagues made CMA first-tier cytogenetic testing for unexplained DD/ID, ASD or multiple congenital anomalies. [3] [4]
Structural brain injury or malformation after prenatal, perinatal or early postnatal insults can impair motor, language and cognitive streams together. Neurometabolic disease may present with progressive or fluctuating course, decompensation with illness, or specific examination clues; some of these are treatable if recognised. [1] [3]
Sensory deprivation is mechanical and merciful to remember: a child who cannot hear well will not build spoken language on schedule, and vision loss blunts exploration and fine-motor practice. Severe psychosocial deprivation can slow skill acquisition without a primary genetic lesion, and trauma-informed care shapes how you take that history. [7] [12]
Early intervention still matters while you wait for a molecular answer. Plasticity and skill practice do not pause for the laboratory. That is the practical pathophysiology of “treat while you test.” [1] [7]
Clinical Presentation
Some families arrive with a clear worry. Others are referred after a failed screen or a preschool concern. Common entry points include late sitting or walking, few words by the second birthday, poor fine-motor play, limited social engagement, and comparison with siblings or peers. Caregiver concern is data, not noise. [7] [14]
Age bands help you picture the child. In late infancy you notice delayed sitting, limited transfer, sparse babble and reduced social smile reciprocity. In toddlers you notice delayed walking, few single words, absent two-word phrases, limited pretend play and clumsy fine-motor tasks. In preschoolers you notice multi-domain lag that threatens school readiness. Correct for prematurity until the accepted cut-off for the domain and local practice; otherwise you invent disease. [1] [7]
Red-flag companions include seizures, staring spells, loss of skills, microcephaly or progressive macrocephaly, abnormal tone, dysmorphism with anomalies, and a progressive rather than static course. Inconsistent history, missed care and multi-domain lag together raise safeguarding concern. [1] [12]
Do not accept false reassurance scripts. “Boys talk late” does not cancel a failed hearing pathway. “Wait and see” after a positive developmental screen is usually the wrong exam answer when multi-domain delay is already clear. Surveillance and screening exist to trigger action, not endless observation. [7] [7]
Differential Diagnosis
Hold the common and the dangerous together. [1]
Genetic developmental disorders are a major aetiological group once sensory and environmental contributors are addressed. CNVs, monogenic syndromes and chromosomal disorders sit here. [4] [5] [6]
Structural brain disorders and cerebral palsy pathways enter when tone, posture, motor asymmetry or early brain injury history dominate. Cross-link CP recognition leaves rather than forcing every motor delay into GDD language. [1]
Neurometabolic and progressive neurological disease enter with regression, decompensation, consanguinity, organomegaly, unusual odours, movement disorders or unexplained encephalopathy. This is where selective metabolic testing earns its place. [1] [3]
Sensory impairment can mimic or compound GDD. Hearing and vision assessment are not optional extras. [1] [7]
Autism spectrum presentations can coexist with GDD or dominate social-communication concern. Assess in parallel when indicated; do not wait for an exome to notice joint attention failure. Cross-link the autism recognition leaf. [7]
Psychosocial adversity and neglect can produce multi-domain lag. Trauma-informed assessment keeps the child safe without premature blame. [12]
Idiopathic residual GDD remains after a thorough negative work-up. That is an interim clinical label, not a reason to stop supports or future re-analysis as genomic technology advances. [1] [6]
Clinical & Bedside Assessment
1. Stability first. Look at the child before the pedigree. Breathing, colour, interaction, seizures, glucose risk and signs of injury outrank a calm discussion of microarrays. A caregiver who says “this is not my child today” raises urgency. [14]
2. Build a domain-by-domain history. Ask what the child can do now in gross motor, fine motor, speech and language, social interaction and self-care. Ask when skills appeared. Ask whether any skill was gained and then lost. Correct for prematurity. Use a professional interpreter when language discordance exists. [1] [10]
3. Take a medical and family history that could change testing. Pregnancy, birth, neonatal course, congenital infections, seizures, growth, hearing screens, vision concerns, medications, toxin exposures and three-generation pedigree including consanguinity and learning disability. [1]
4. Examine with purpose. Plot weight, length or height and head circumference. Look for dysmorphism, skin findings, organomegaly, spine and limb anomalies. Do a careful neurological examination: tone, power, reflexes, posture, movement quality, cranial nerves and gait if walking. Watch vision behaviour and response to sound. Observe play and social communication without overclaiming a formal autism diagnosis in five minutes. [1] [6]
5. Document social determinants and safeguarding risk without humiliation. Who cares for the child, housing stability, food security, caregiver mental health, prior child-protection involvement and barriers to attending therapy. Trauma-informed posture improves disclosure. [12]
Detailed standardised tool choice lives on the assessment tools page. Use clinic observation and validated screens to structure concern; refer for formal developmental or cognitive testing when age and question demand it. [7]
Investigations
Investigations answer three questions: what treatable factor is active now, what aetiology explains the pattern, and what information changes recurrence counselling or surveillance? They should not delay therapy. [1] [6]
Hearing and vision. Treat these as first-line in almost every GDD evaluation. Confirm newborn hearing pathway completion. Arrange diagnostic audiology and age-appropriate vision assessment early. [1] [7]
Genetic testing has evolved — know the eras so you do not give a 2005 answer in a 2026 viva. [1] [5] [6]
- Karyotype still has roles for obvious aneuploidy phenotypes, family rearrangements and selected reproductive contexts, but it is no longer the default first cytogenetic test for unexplained GDD. [4]
- Chromosomal microarray (CMA) became first-tier cytogenetic testing for unexplained developmental disabilities or congenital anomalies because diagnostic yield for pathogenic CNVs exceeded karyotype in that population. Miller’s consensus statement is the landmark for that shift. Michelson’s AAN evidence report summarised genetic and metabolic test yields in GDD and supported microarray utility in that era. [3] [4]
- Fragile X testing remains relevant in selected clinical contexts, especially with suggestive family history or phenotype, rather than as an unthinking universal for every child. Follow current genetics advice rather than inventing local rules. [1] [3]
- Exome or genome sequencing is now recommended by ACMG as a first- or second-tier test for paediatric patients with congenital anomalies or intellectual disability, with strong evidence for diagnostic utility. The 2025 AAP clinical report by Rodan and colleagues updates paediatric genetic evaluation of ID/GDD and centres exome or genome sequencing as first-tier testing in most unexplained cases, with continued attention to copy-number detection and phenotype-driven exceptions. Local access and funding still vary — say that out loud in regional answers. [5] [6]
Metabolic testing is not a ritual mega-panel for every mild static GDD. Yield rises with red flags: regression, episodic decompensation, consanguinity with progressive course, specific examination clues, or unexplained biochemical abnormalities. Michelson’s evidence report framed metabolic testing yields in selected populations; modern practice keeps testing selective. [1] [3] [6]
Neuroimaging (usually MRI when available) is indicated for abnormal neurological examination, microcephaly or progressive macrocephaly, seizures, regression, focal signs or other features that raise structural disease. It is lower yield as a blank ritual in isolated non-progressive GDD with normal exam. [1] [6]
EEG is for spells, suspected seizures, regression with epileptic encephalopathy concern — not a default GDD screen. [1]
Other directed tests follow the phenotype: creatine disorders, thyroid function when indicated, lead testing in high-risk exposure settings, and infection work-up when history demands. Omit rather than invent uncited local panels. [1] [3]
Management — Resuscitation
Most GDD clinic visits are not resuscitations. When they are, abandon the microarray conversation and treat threat. [14]
Protect airway and breathing if the child is obtunded or seizing. Treat status epilepticus on local emergency pathways. Check glucose. Consider meningitis or encephalitis when fever and encephalopathy coexist. For suspected abusive injury, secure safety and follow mandatory reporting pathways while you stabilise. Severe neglect with an unsafe care environment is a safety emergency, not only a developmental referral. [12]
Handover must be explicit: what domains are delayed, what red flags you found, what tests are pending, and what early intervention was started. Structured handoff reduces error when multiple teams share the child. [11]
Management — Definitive & Stepwise
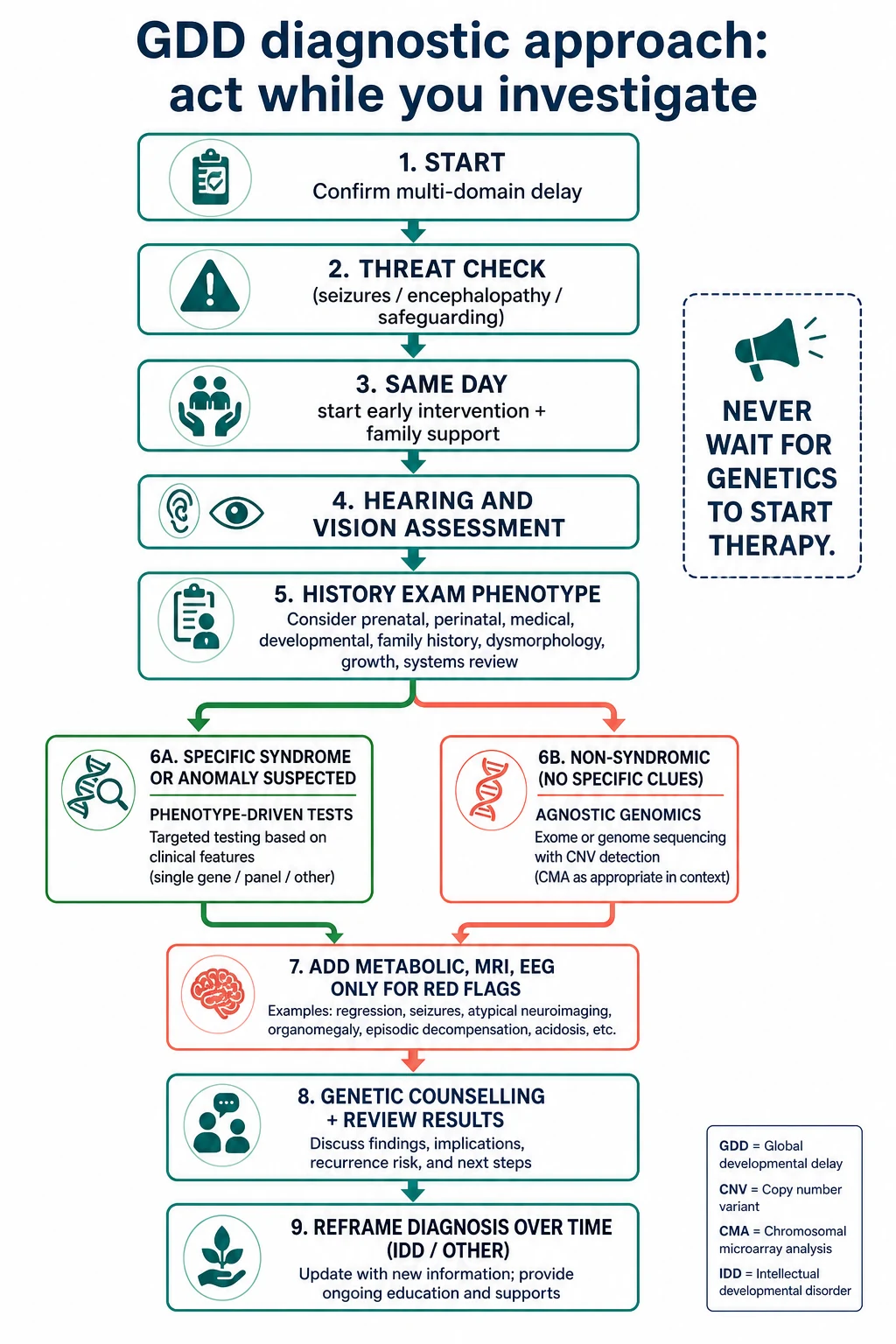
Step 1 — Name the problem representation. “Global developmental delay affecting language and fine-motor domains in a corrected-age 26-month-old, no regression, examination non-dysmorphic so far.” That sentence guides the team. [1]
Step 2 — Start early intervention now. Refer to local early childhood intervention, physiotherapy, occupational therapy, speech and language therapy, and education supports as indicated by domain profile. In Australia this often interfaces with NDIS early childhood approaches; in the US with IDEA Part C; in the UK with local therapy and EHCP pathways. Do not wait for genetics. [7]
Step 3 — Complete sensory assessment. Hearing and vision pathways with dates and owners. [1]
Step 4 — Choose the genetic strategy. Phenotype-driven if examination or family history points. Agnostic genomic testing per ACMG/AAP guidance when unexplained. Consent for genetic testing needs plain-language discussion of possible results, variants of uncertain significance, secondary findings policies where applicable, and implications for relatives. Katz’s informed-consent framing still applies: capacity, disclosure, understanding and voluntariness scaled to paediatric decision-making. [5] [6] [8]
Step 5 — Add selective tests. Metabolic, MRI, EEG only with indication. [1] [3] [6]
Step 6 — Support the family system. Explain that a label of GDD is a starting point. Offer written plans, interpreter-supported teach-back, social work and caregiver mental health links. Trauma-informed posture matters when adversity is part of the story. [10] [12]
Step 7 — Review and reframe. Reassess development, review results, escalate if regression appears, and convert language toward IDD or other diagnoses when age-valid cognitive and adaptive testing supports that step. Genomic re-analysis may become appropriate later as knowledge expands. [1] [6]
Safety-net clearly: new seizures, loss of skills, progressive head-size change, acute encephalopathy, or a family that cannot access therapy all need earlier return. Safety-netting improves care for acute illness in children and the same communication discipline helps developmental follow-up. [13]
Specific Subtypes & Scenarios
Failed hearing pathway with multi-domain lag. Treat audiology as urgent. Speech therapy alone is not a hearing test. [1] [7]
Ex-preterm toddler without age correction. Recalculate corrected age before you label GDD. Still act if delay remains after correction. [7]
Consanguineous family with progressive course. Raise neurometabolic and recessive genetic priors. Involve genetics early and keep metabolic red flags active. [1] [3]
Dysmorphism plus congenital anomalies. Phenotype-driven genetics and early clinical genetics referral. CMA and genomic sequencing decisions follow current guidance and local pathways. [4] [5] [6]
Regression after normal skills. Leave the ordinary GDD algorithm. Use the urgent regression pathway. [1]
Motor-dominant hypertonia. Think cerebral palsy evaluation and neuroimaging indications; cross-link CP leaves. [1]
Social-communication dominant. Parallel autism assessment; genetics still often indicated when global delay coexists. [6] [7]
Refugee or language-discordant family. Interpreter first. Interrupted records mean you reconstruct the timeline carefully and avoid assumptions about “cultural lateness.” [10]
Medical complexity. Baseline disability plus new plateau needs a fresh problem list, not diagnostic overshadowing. Kuo’s medical complexity framing helps teams coordinate. [9]
Complications & Pitfalls
- Waiting for an exome or microarray before starting therapy. [1] [7]
- Calling isolated speech delay “GDD” without multi-domain assessment. [1]
- Missing hearing or vision impairment. [1] [7]
- Missing regression and treatable epileptic encephalopathy. [1]
- Ordering broad metabolic panels without red flags while under-supporting the family. [3] [6]
- Using “wait and see” after clear multi-domain delay or failed screens. [7]
- Ignoring safeguarding when multi-domain lag and social red flags coincide. [12]
- No interpreter for developmental history. [10]
- Failing to correct prematurity. [7]
- Overclaiming a final molecular diagnosis from a variant of uncertain significance. [5] [6]
Prognosis & Disposition
Prognosis depends on cause, severity, comorbidities, therapy access and the caregiving environment. Some children with sensory or psychosocial drivers improve trajectory once those drivers are fixed. Many children with genetic or structural causes need long-term developmental supports even when a molecular diagnosis is clear. A genetic answer can still change surveillance, recurrence counselling and family planning even if it does not “cure” the delay. [1] [6]
Safe disposition from clinic means: early intervention referrals made, sensory tests booked, genetic consent and samples planned or drawn, red-flag advice given, and a review date that matches severity and social risk. Safe disposition from acute care after seizure or encephalopathy means the developmental plan is part of the discharge, not an afterthought. [11] [13]
Special Populations
Preterm graduates need corrected-age interpretation and high-risk follow-up programmes, while still receiving timely intervention when delay is real. [7]
Children with medical complexity need coordinated plans, realistic goal-setting and attention to diagnostic overshadowing when a new plateau appears. [9]
Indigenous families need culturally safe conversations that never racialise delay and that partner with community supports. [12]
Migrant and refugee children need interpreters, reconstructed timelines and dual attention to infection, nutrition, trauma and missed screens. [10] [12]
Out-of-home care populations need growth and development treated as welfare-relevant data with clear information sharing. [12]
Rural and remote families need telehealth for parts of assessment, honest limits of remote neurological soft signs, and early retrieval or travel planning when red flags appear. [7]
Evidence, Guidelines & Regional Differences
Moeschler and Shevell (AAP 2014) set the comprehensive clinical evaluation frame for ID/GDD. [1]
Shevell’s 2003 AAN/CNS practice parameter is historical and retired, but it still appears in older stems as the first structured GDD evaluation parameter. Michelson’s 2011 evidence report updated genetic and metabolic testing yields and is also marked retired — cite it as evidence history, not as the sole current rule book. [2] [3]
Miller 2010 established CMA as first-tier cytogenetic testing for unexplained DD/ID, ASD or MCA compared with karyotype. [4]
Manickam 2021 (ACMG) recommends exome or genome sequencing as a first- or second-tier test for paediatric congenital anomalies or intellectual disability. Rodan 2025 (AAP) updates the paediatric genetic evaluation of ID/GDD toward first-tier exome or genome sequencing in most unexplained cases, with concurrent attention to copy-number variation and phenotype-driven exceptions. Local funding and laboratory models still differ. [5] [6]
Lipkin 2020 anchors developmental surveillance and screening as the entry ramp into diagnostic pathways. [7]
Child health records and local surveillance tools feed referral. NDIS early childhood approaches and state therapy services often run in parallel with paediatric diagnostics. Pair genomic testing access via local genetics services with culturally safe practice for Aboriginal, Torres Strait Islander and Māori whānau. [6] [7]
Community paediatric pathways, local therapy services and education health care plans structure support. Genomic testing access follows UK genetics service models; do not invent a single national lab menu in a viva — describe the clinical indications and referral. [5] [7]
AAP surveillance/screening guidance and AAP/ACMG genetic evaluation recommendations dominate exam answers. Early Intervention (IDEA Part C) and school services proceed without waiting for a molecular diagnosis. [5] [6] [7]
Provincial early intervention and genetics pathways operationalise similar clinical principles; name local access limits rather than inventing pan-Canadian lab rules. [5] [7]
Exam Pearls
- GDD = multi-domain significant delay in a young child; not a final aetiology. [1]
- Never delay early intervention for a pending genetic result. [1] [7]
- Hearing and vision first. [1]
- Regression is a different emergency pathway. [1]
- Know the genetic eras: karyotype → CMA first-tier cytogenetics → ES/GS first-tier genomics with CNV awareness. [4] [5] [6]
- Metabolic tests and MRI are red-flag driven. [1] [3] [6]
- Caregiver concern is data. [14]
- Correct for prematurity; use an interpreter; keep safeguarding open. [7] [10] [12]
- Consent for genomics is a clinical skill, not a formality. [8]
High-yield anchors
References
- [1]Moeschler JB Comprehensive evaluation of the child with intellectual disability or global developmental delays. Pediatrics, 2014.PMID 25157020
- [2]Shevell M Practice parameter: evaluation of the child with global developmental delay [RETIRED]: report of the Quality Standards Subcommittee of the American Academy of Neurology and The Practice Committee of the Child Neurology Society. Neurology, 2003.PMID 12578916
- [3]Michelson DJ Evidence report: Genetic and metabolic testing on children with global developmental delay [RETIRED]: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology, 2011.PMID 21956720
- [4]Miller DT Consensus statement: chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies. American journal of human genetics, 2010.PMID 20466091
- [5]Manickam K Exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability: an evidence-based clinical guideline of the American College of Medical Genetics and Genomics (ACMG). Genetics in medicine : official journal of the American College of Medical Genetics, 2021.PMID 34211152
- [6]Rodan LH Genetic Evaluation of the Child With Intellectual Disability or Global Developmental Delay: Clinical Report. Pediatrics, 2025.PMID 40545261
- [7]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [8]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [9]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [10]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [11]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [12]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [13]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [14]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224