Paeds · growth-development-and-behaviour
General movements assessment and Hammersmith infant neurological examination
Also known as GMA · General Movements Assessment · Prechtl general movements · HINE · Hammersmith Infant Neurological Examination · Brief-HINE · Early detection of cerebral palsy tools
Fellowship approach to Prechtl general movements assessment and the Hammersmith Infant Neurological Examination: timing windows, what each tool assesses, combination with neuroimaging for high-probability cerebral palsy, pitfalls, training limits and counselling.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A four-month corrected-age graduate of extreme prematurity lies on a mat. The video looks “busy,” yet a trained scorer says fidgety movements are absent. The Hammersmith score is low. MRI already showed white-matter injury. Parents ask whether this is cerebral palsy. Your job on this page is not to re-teach the whole CP classification leaf. Your job is to use general movements assessment (GMA/GMs) and the Hammersmith Infant Neurological Examination (HINE) correctly: what they are, when to use them, what they do and do not prove, and how results change counselling and referral. [1] [5] [12]
This leaf owns the tools. Companion pages own CP phenotype/function labels, long-term surveillance, normal motor variation, and hypotonia work-up. [1]
G.M.s + H.I.N.E. early
Overview & Definition
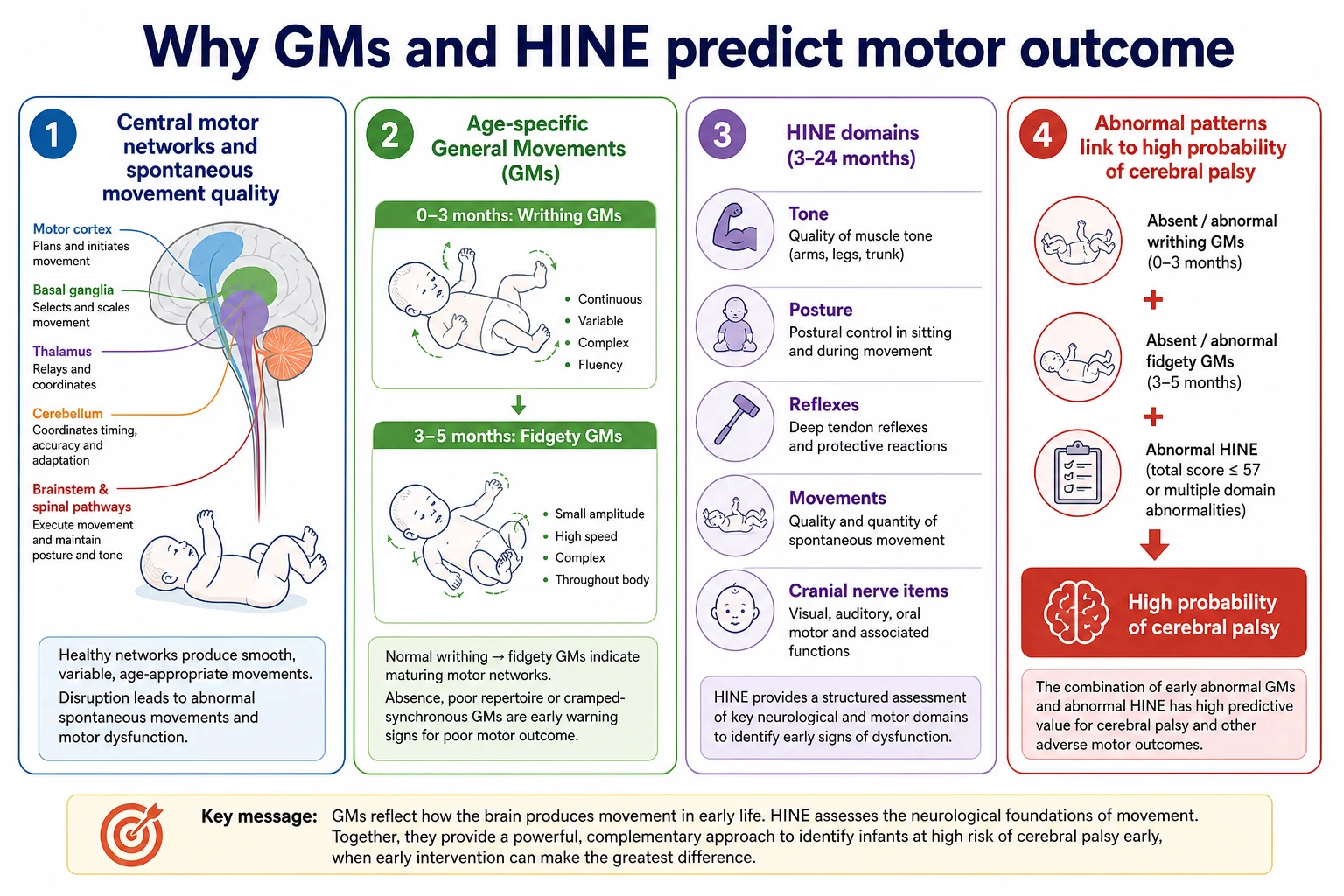
General movements are spontaneous, endogenously generated whole-body movements present from fetal life through early infancy. Prechtl’s functional assessment treats the quality of those movements — fluency, variability, complexity — as a window into central motor network integrity. The method is often called Prechtl’s general movements assessment or GMA. It is not a checklist of milestones. It is a trained observation of how the infant moves when free and alert. [4] [5]
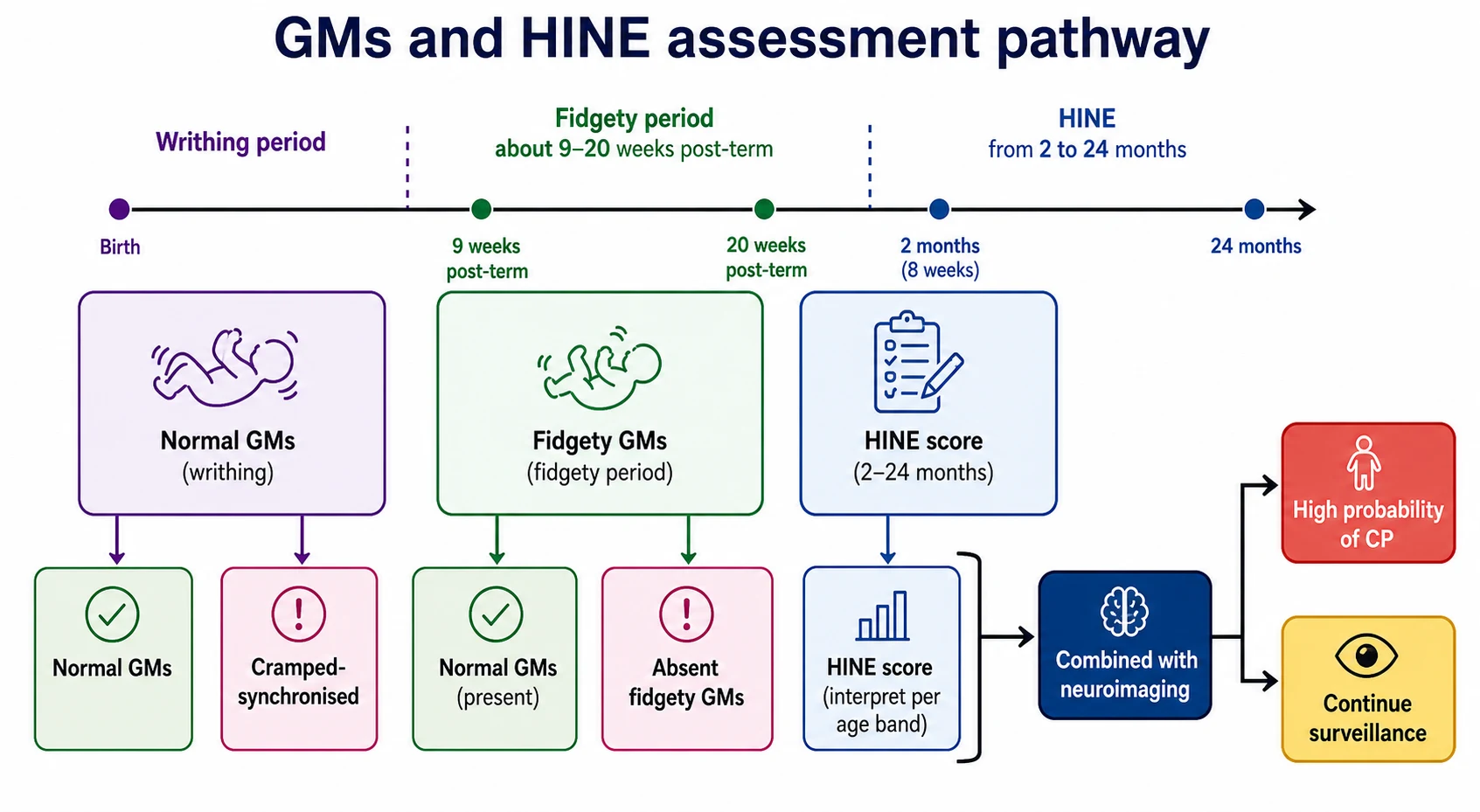
Two broad age periods matter in clinical teaching. In the writhing period (term age into the first weeks post-term), movements have a writhing character. Cramped-synchronised patterns in this window are a high-risk qualitative abnormality. In the fidgety period (commonly taught as roughly 9–20 weeks post-term age, peaking around three to five months corrected), small circular movements of neck, trunk and limbs appear in normal infants. Absent fidgety movements are strongly associated with later cerebral palsy risk when scored by trained assessors. Abnormal fidgety quality can also flag later minor neurological dysfunction pathways. [4] [5] [14]
The Hammersmith Infant Neurological Examination (HINE) is a standardised neurological examination for infants, classically used from about two to twenty-four months of age. Items cover cranial nerve function, posture, movements, tone and reflexes. Scores yield an optimality profile: lower optimality associates with higher probability of adverse motor outcomes, including cerebral palsy, when used in trained hands and interpreted with age and population context. A Brief-HINE screening adaptation exists for settings that cannot always complete a full exam. Scoring aids support consistent early-detection practice. Do not invent a single universal numeric cut-off in a viva unless you can defend the exact age band and source. State the principle: suboptimal optimality plus risk plus abnormal movements raises probability. [6] [7] [8] [9]
Together with perinatal risk and neuroimaging, GMs and HINE underpin modern early, high-probability cerebral palsy pathways. They support action before independent walking. They do not replace clinical judgement, family partnership or differential diagnosis for progressive disease. [1] [3] [18]
Classification
Think in tools and risk tiers, not disease subtypes. [1] [4] [6]
| Tool | What it is | Typical teaching window | Output concept |
|---|---|---|---|
| GMs / GMA | Video-based qualitative movement assessment | Writhing then fidgety (post-term ages) | Normal vs abnormal repertoire (e.g. poor repertoire, cramped-synchronised; present vs absent fidgety) |
| HINE | Scored neurological exam | About 2–24 months | Optimality score / profile |
| Brief-HINE | Shorter screening adaptation | First year after birth | Screening signal to trigger full assessment |
| Neuroimaging | MRI preferred when available | Timing clinical | Pattern that supports or challenges the motor story |
Risk tiers for service design: high-risk follow-up (extreme preterm, neonatal encephalopathy, stroke, meningitis, complex multiple birth, known significant brain injury) versus community concern (asymmetric use, stiffness, delayed motor skills without NICU history). Prior probability differs; tool interpretation always sits inside that prior. [1] [13]
General movements (GMs)
- Spontaneous movement quality on video in a quiet alert state
- Emphasises fluency, variability and age-typical fidgety movements
- Requires training and correct age window
HINE
- Hands-on scored neurological exam of posture, tone, reflexes, movements and cranial nerve items
- Yields optimality information
- Complements, does not replace, GMs
Epidemiology & Risk Factors
Who should be prioritised? Infants with extreme prematurity, very low birth weight, hypoxic–ischaemic encephalopathy (including after therapeutic hypothermia), perinatal stroke, neonatal meningitis or encephalitis, significant intracranial haemorrhage or white-matter injury, and complicated multiple pregnancy pathways. Postneonatal early brain insults also need structured follow-up. Waiting until a late motor milestone is missed delays intervention in children who already carry high prior risk. [1] [2] [13]
Population screening of every well term infant with formal GMs is not the same problem as high-risk clinic use. Resources, training and video pathways concentrate where base-rate of CP is higher. Equity gaps matter: rural families, First Nations communities, language discordance and poverty reduce access to trained assessors and early intervention even when tools exist. Telehealth video pathways can widen access for GMs filming when protocols and training are in place, but they are not a free pass for untrained scoring. [12] [13] [16]
Pathophysiology
Why do spontaneous movements matter? Early motor behaviour is generated by central pattern networks that require intact and maturing brain connectivity. When early injury disrupts those networks, movements lose complexity, fluency and age-appropriate fidgety character. Prechtl framed this as a functional assessment of the young nervous system and an early predictor of cerebral palsy. Age-dependent expression means the same infant can look different in the writhing and fidgety windows — which is why timing is part of validity. [4] [5]
HINE items map clinical domains — tone, posture, reflexes, movements — that also reflect network integrity rather than a single muscle disease. Lower optimality tracks higher risk of later motor disability in studied cohorts, including pathways beyond pure CP labels in some term populations. Imaging complements the bedside: basal ganglia–thalamic injury after asphyxia relates to abnormal general movements in term infants; white-matter injury after prematurity often pairs with bilateral motor risk. Tools and MRI answer different questions; the combination is stronger than either alone in early high-risk diagnosis frameworks. [3] [6] [7] [15]
Clinical Presentation
Parents may notice stiffness when dressing, paucity of movement, early hand preference, scissoring on lift, or that “one arm never opens.” Video GMs capture movement quality that casual observation may miss, especially absent fidgety movements in a quiet alert infant at the right corrected age. A trained clinic may document abnormal repertoire in the writhing period or absent/abnormal fidgety movements later. [5] [14]
HINE findings present as suboptimal optimality: reduced spontaneous movements, abnormal posture, tone asymmetry, or persistent primitive patterns inappropriate for age. Asymmetric findings raise unilateral CP concern and should trigger careful comparison of hand and leg use. Abnormal tools with or without imaging both occur — each combination needs a different counselling script. [7] [8]
Differential Diagnosis
Transient neurological abnormalities of prematurity can worry families and examiners. Serial assessment and tool combination reduce the error of either over-calling or under-calling. Central versus peripheral hypotonia is a different localisation problem: GMs and HINE support central risk pathways but do not replace a floppy-infant work-up when peripheral signs dominate. Global developmental delay without a CP motor pattern remains possible with mixed findings. High probability of CP with an evolving phenotype is common — the original brain disturbance is non-progressive, but the clinical picture still changes as the infant grows. Progressive disease red flags (true regression, continuously worsening course) reopen the differential away from simple static CP pathways. [1] [13] [18]
Clinical & Bedside Assessment
1. Corrected age and window. For preterm infants, use corrected age for GMs windows. Do not film a “fidgety” assessment at the wrong post-term age and call it definitive. [4] [5]
2. Film GMs properly. Quiet alert state. Infant supine, lightly dressed, free limbs, no pacifier if it suppresses movement, adequate recording length for trained review (local protocols typically use several minutes of continuous spontaneous movement). Avoid just after a feed that puts the infant to sleep or during crying storms. Formal scoring requires training; untrained staff should escalate abnormal-looking movement rather than invent labels. [4] [5]
3. Perform or arrange HINE. Structured items; score optimality; interpret with age norms and training. Brief-HINE can screen when full capacity is limited, with a clear path to full assessment. Scoring aids improve consistency for early high-probability detection pathways. [6] [8] [9]
4. Integrate the story. Perinatal risk, prior imaging, seizures, caregiver concerns, serial exams. Build a problem representation: risk + movement quality + HINE + imaging = probability statement. [1] [3]
5. Communicate while assessing. Explain that you are watching how the brain organises movement, not grading parenting. Avoid catastrophic certainty and avoid false reassurance. [12]
Investigations
GMs and HINE are clinical tools, not laboratory tests. Neuroimaging — preferably MRI when available and safe — synergises with them for early CP diagnosis frameworks. Hearing and vision surveillance still matter because sensory loss changes developmental support. Do not substitute an informal milestone checklist for standardised tools in high-risk infants. Do not delay therapy solely to complete every investigation if probability is already high. [1] [2] [3]
Management — Resuscitation
These tools are not resuscitation instruments. If the infant has evolving encephalopathy, seizures, respiratory failure or acute deterioration during a follow-up window, use standard emergency pathways first. Urgent escalation beats completing a video. [1]
Management — Definitive & Stepwise
Step 1 — Stratify risk and set a surveillance schedule in the first year for high-risk graduates and for community infants with motor red flags. [1] [13]
Step 2 — Combine GMs + HINE + neuroimaging according to early detection frameworks (Novak synthesis; Bosanquet predictive-test review; Morgan pooled accuracy work). Highest predictive performance comes from combination, not from a single normal early glance. [1] [2] [3]
Step 3 — Name high probability carefully when tools converge. Implementation data support that early high-risk classification predicts CP at two years in organised pathways. Use “high probability of cerebral palsy” language and explain that phenotype and function still refine. [1] [16] [18]
Step 4 — Refer to early intervention now. International guideline work for infants 0–2 years at high risk of CP supports active early motor intervention. Systematic reviews support motor intervention and enriched environments over passive waiting. Investigations continue in parallel. [10] [11] [17]
Step 5 — Serial reassessment. A single early normal exam does not erase residual high risk. Re-examine through infancy. Link to CP recognition/classification and long-term surveillance leaves for phenotype labels, hip surveillance and tone care. [1] [12]
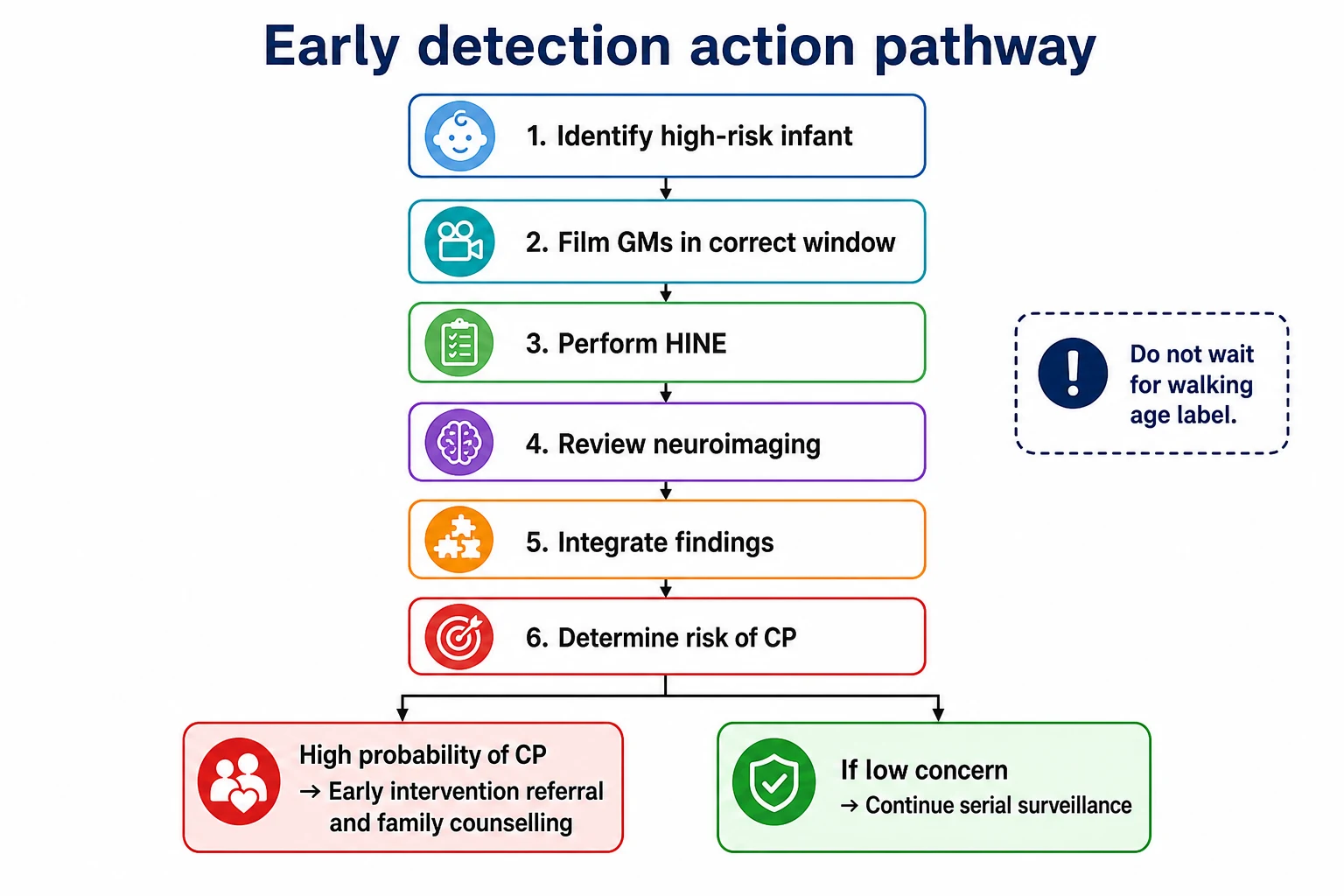
First-year early detection moves
Identify risk
Identify perinatal or postneonatal risk and set follow-up.
Film GMs
Film GMs in the correct post-term window with trained scoring.
Perform HINE
Perform HINE (or Brief-HINE then full exam) and document optimality.
Integrate imaging
Integrate MRI already done or arrange if it changes management.
Act on high probability
Counsel carefully, start early intervention, and plan serial review.
Specific Subtypes & Scenarios
Extremely preterm graduate at fidgety age. Corrected age, trained GMs, HINE, prior cranial imaging, early therapy if abnormal. Common bilateral white-matter risk pathway. [1] [5]
Term HIE after cooling. Serial neurology, MRI, GMs quality (including links to deep grey injury patterns), honest uncertainty with clear follow-up. [15] [1]
Unilateral lesion and asymmetric HINE. Compare hand use and kick; early hand preference is a warning, not a quirk. [1] [5]
Normal GMs but abnormal imaging. Do not discharge risk; continue HINE and developmental surveillance; counsel residual risk and reasons for ongoing follow-up. [3]
Absent fidgety movements. Treat as high-concern signal in trained assessment: imaging review, HINE, early intervention referral, careful family counselling. [5] [14]
Brief-HINE only available. Use as screen; arrange full HINE and specialist pathway rather than false finality. [9]
Complications & Pitfalls
- Untrained GMs video scoring treated as definitive. [4] [5]
- Filming in wrong behavioural state or wrong age window. [4]
- False reassurance from one early normal exam with ongoing high risk. [1] [3]
- Delaying support until a definitive CP label at walking age. [1] [13]
- Quoting HINE cut-offs without age band, population and training context. [6] [8]
- Ignoring progressive disease red flags because “tools said CP risk.” [18]
Prognosis & Disposition
Predictive performance is strongest when neuroimaging, GMs and neurological examination are combined in high-risk infants. Early high-risk classification in implementation cohorts predicts later CP diagnosis, supporting action rather than endless waiting. Disposition: early intervention services, specialist developmental or CP early-detection follow-up, serial exams, family support, and realistic hope that early active therapy matters. Motor phenotype may still evolve — surveillance continues. [3] [10] [16]
Special Populations
Preterm versus term timing uses corrected age for GMs windows; HINE interpretation respects age. First Nations and remote families need culturally safe conversations and practical video pathways without racialised assumptions. Technology-dependent infants still deserve movement assessment adapted to lines and devices. Resource-limited settings without MRI can still use clinical tools and act on high probability while arranging imaging access. [1] [12] [9]
Evidence, Guidelines & Regional Differences
Novak 2017 synthesised early accurate diagnosis and early intervention advances. Bosanquet’s systematic review compared predictive tests for CP in young children. Morgan’s pooled accuracy work supports combining neuroimaging, GMs and neurological examination in high-risk infants. Morgan 2021 provides an international clinical practice guideline for early intervention in 0–2 years with or at high risk of CP. Prechtl and Einspieler frames establish GMs as early markers. Haataja’s optimality scoring underpins HINE. Romeo and Fehlings update HINE applications, including non-CP outcomes, Brief-HINE and scoring aids. Te Velde documents historical barriers and clinic implementation. Kwong 2025 supports predictive value of early high-risk classification in practice. [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [12] [13] [16]
Australian early-detection clinics and follow-up programmes operationalise GMs and HINE within high-risk infant pathways; culturally safe access for Aboriginal and Torres Strait Islander families and Te Tiriti-informed care in Aotearoa New Zealand are service requirements. [12] [16]
Neonatal follow-up and neurodevelopmental services route high-risk infants; tool combination language is shared internationally even when clinic names differ. [1] [2]
High-risk infant follow-up and Early Intervention systems interact; access varies by state and insurance, so tool-positive infants still need active navigation into services. [1] [10]
Paediatric neurology and rehabilitation pathways commonly integrate standardised infant neurology with early therapy planning. [1] [8]
Controversies: telehealth limits for formal GMs reliability, exact service eligibility language for “high probability,” and how aggressively to pursue genetics when tools and MRI diverge. State uncertainty; still act on converging high probability. [1] [13]
Exam Pearls
- Fidgety window is roughly 9–20 weeks post-term; absent fidgety movements are highly concerning in trained hands. [4] [5]
- Cramped-synchronised patterns in the writhing period are high risk. [4] [5]
- HINE is scored; lower optimality associates with higher CP probability — do not invent cut-offs without source. [6] [8]
- Best early detection = GMs + HINE + neuroimaging together. [1] [3]
- Do not wait for 12–24 month late diagnosis if probability is already high. [1] [13]
- Tools support high-probability CP language before final phenotype is locked. [1] [16] [18]
- Training and correct behavioural state are part of validity. [4] [5]
References
- [1]Novak I Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA pediatrics, 2017.PMID 28715518
- [2]Bosanquet M A systematic review of tests to predict cerebral palsy in young children. Developmental medicine and child neurology, 2013.PMID 23574478
- [3]Morgan C The Pooled Diagnostic Accuracy of Neuroimaging, General Movements, and Neurological Examination for Diagnosing Cerebral Palsy Early in High-Risk Infants: A Case Control Study. Journal of clinical medicine, 2019.PMID 31694305
- [4]Prechtl HF State of the art of a new functional assessment of the young nervous system. An early predictor of cerebral palsy. Early human development, 1997.PMID 9467689
- [5]Einspieler C Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome. Journal of clinical medicine, 2019.PMID 31590221
- [6]Haataja L Optimality score for the neurologic examination of the infant at 12 and 18 months of age. The Journal of pediatrics, 1999.PMID 10431108
- [7]Romeo DM Hammersmith Infant Neurological Examination in infants born at term: Predicting outcomes other than cerebral palsy. Developmental medicine and child neurology, 2022.PMID 35201619
- [8]Fehlings D The Hammersmith Infant Neurological Exam Scoring Aid supports early detection for infants with high probability of cerebral palsy. Developmental medicine and child neurology, 2024.PMID 38818710
- [9]Romeo DM Neurological assessment tool for screening infants during the first year after birth: The Brief-Hammersmith Infant Neurological Examination. Developmental medicine and child neurology, 2024.PMID 38287208
- [10]Morgan C Early Intervention for Children Aged 0 to 2 Years With or at High Risk of Cerebral Palsy: International Clinical Practice Guideline Based on Systematic Reviews. JAMA pediatrics, 2021.PMID 33999106
- [11]Morgan C Effectiveness of motor interventions in infants with cerebral palsy: a systematic review. Developmental medicine and child neurology, 2016.PMID 27027732
- [12]Te Velde A Age of Diagnosis, Fidelity and Acceptability of an Early Diagnosis Clinic for Cerebral Palsy: A Single Site Implementation Study. Brain sciences, 2021.PMID 34439692
- [13]te Velde A Early Diagnosis and Classification of Cerebral Palsy: An Historical Perspective and Barriers to an Early Diagnosis. Journal of clinical medicine, 2019.PMID 31623303
- [14]Einspieler C Are abnormal fidgety movements an early marker for complex minor neurological dysfunction at puberty? Early human development, 2007.PMID 17129688
- [15]Ferrari F General movements in full-term infants with perinatal asphyxia are related to Basal Ganglia and thalamic lesions. The Journal of pediatrics, 2011.PMID 21232764
- [16]Kwong AK Early high risk of cerebral palsy classification is predictive of cerebral palsy at 2 years: an implementation cohort study. Archives of disease in childhood, 2025.PMID 40877021
- [17]Morgan C Enriched environments and motor outcomes in cerebral palsy: systematic review and meta-analysis. Pediatrics, 2013.PMID 23958771
- [18]Rosenbaum P A report: the definition and classification of cerebral palsy April 2006. Developmental medicine and child neurology. Supplement, 2007.PMID 17370477