Paeds · growth-development-and-behaviour
Social communication concerns and autism recognition
Also known as Autism recognition · Autism red flags · Social communication delay · M-CHAT autism screen · Early autism identification
Fellowship approach to recognising social communication concerns and autism risk from infancy through school age: red flags, differential diagnosis, autism-specific screening limits, early referral and family counselling without replacing full ASD diagnostic management.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
These distinctions keep recognition actionable without inventing a full diagnostic chapter here. [1] [3]
S.O.C.I.A.L. at the bedside
Overview & Definition
Parents often notice first: “He does not look when I call,” “She does not point,” or “He was saying words and stopped.” Social communication concern is a clinical problem representation, not a diagnosis. Autism spectrum disorder (ASD) is a neurodevelopmental diagnosis defined by persistent deficits in social communication and interaction plus restricted, repetitive patterns of behaviour, interests or activities, with onset in the early developmental period and functional impact. Your first job is recognition and timely pathway entry — not promising a label from a checklist. [1]
Surveillance is continuous: ask, watch, document. Autism-specific screening uses a validated tool at key ages or on concern. Diagnostic evaluation is the specialist or multidisciplinary process that can establish ASD and open formal supports. This page owns the recognition layer; general developmental surveillance tools and full ASD management are cross-linked rather than duplicated. [1] [3]
Classification
Classify the presentation before you classify the child. Useful bedside bins: [1]
- Isolated language lag with preserved social engagement — still needs hearing and speech-language pathways, but autism risk may be lower.
- Social communication pattern concerning for autism — reduced joint attention, limited gesture, atypical reciprocity ± restricted interests.
- Multi-domain developmental delay with or without social features.
- Plateau versus true regression of previously acquired skills.
- School-age late presentation with pragmatic language and friendship difficulties, sometimes after camouflaging. [1] [4]
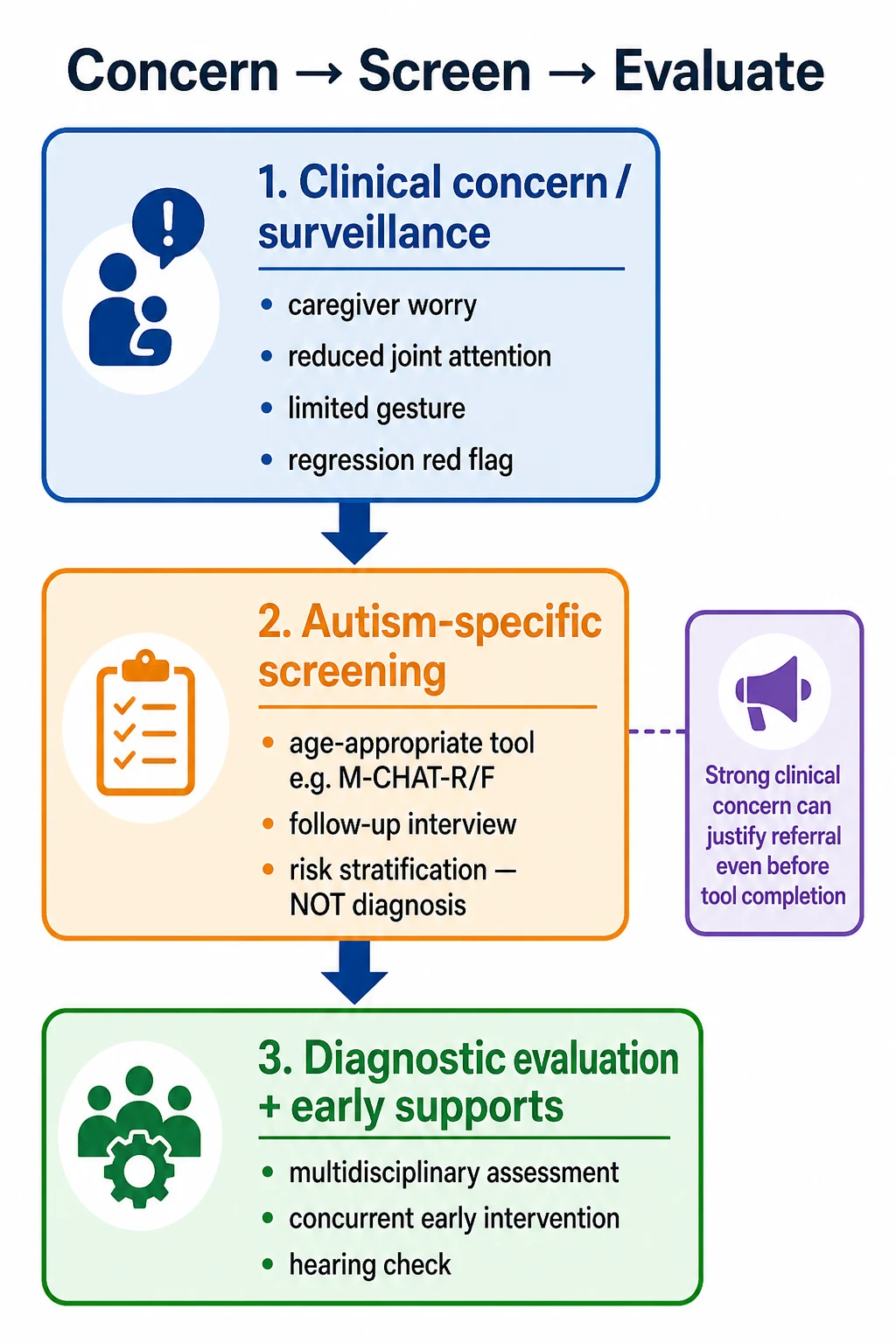
Autism-specific tools such as M-CHAT-R/F are risk-stratification instruments with a follow-up interview pathway; they are not general developmental screens and they are not diagnostic. [2]
Epidemiology & Risk Factors
Recognition is improving, yet late identification still occurs when visits are rushed, services are fragmented, or families face language, transport and cost barriers. Sibling history increases surveillance intensity. Children with medical complexity risk diagnostic overshadowing: clinicians attribute social differences only to the known condition and stop looking. Girls and intellectually able children may present later with subtler social camouflage. [1] [9]
Caregiver concern is a high-value signal. Language discordance without professional interpreting degrades both history quality and counselling about results. [5]
Pathophysiology
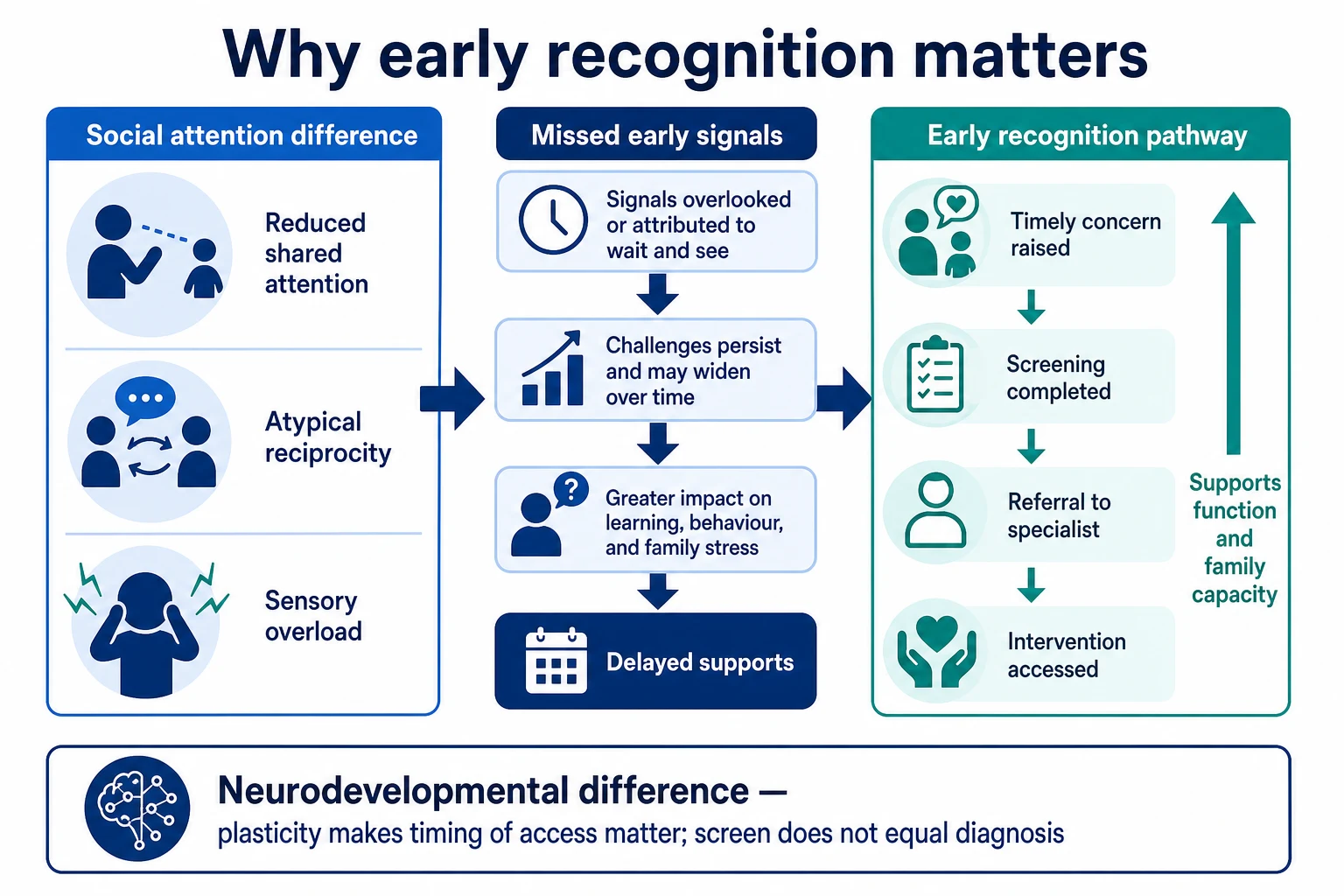
ASD reflects differences in social attention, reciprocity and sensory processing that emerge across early development. Early childhood is a high-plasticity window: earlier access to supports can change functional trajectories even though screening does not change the underlying neurobiology overnight. Sensory overload can look like “behaviour” and trauma can alter social engagement — both need careful assessment without collapsing into a single label. [1] [6]
Regression of language or social skills after prior acquisition is a distinct red-flag pathway that must not be handled as routine “wait and see.” [1] [3]
Clinical Presentation
Infancy. Reduced social smile, limited response to name, reduced shared enjoyment, and weak joint-attention precursors should prompt structured watching rather than reassurance alone. [1] [4]
Toddler years. Limited pointing or showing, reduced imitation, preference for solitary or highly repetitive play, echolalia that is not used communicatively, and poor response to name are classic concern patterns. Vocabulary count alone is not enough — a child can have words without social use of those words. [1] [2]
Preschool. Pragmatic language gaps, rigid routines, intense interests, and sensory-seeking or avoidance may dominate. Peers notice first at childcare. [1]
School age and adolescence. Late presentations include social naivety, friendship difficulty, exhaustion after camouflaging, and secondary anxiety. Do not dismiss because the child is academically able. [1]
Regression. Loss of words or social skills needs prompt evaluation for autism-related regression, hearing problems and neurological disease. [1] [3]
Differential Diagnosis
Separate isolated speech-language delay (social engagement often preserved) from an autism social communication pattern. Always consider hearing impairment when a child seems not to respond. Consider global developmental delay / intellectual developmental disorder when adaptive and cognitive skills are broadly affected. Consider selective mutism, social anxiety, trauma-related withdrawal, ADHD with social impulsivity, and severe psychosocial deprivation — each can mimic pieces of the picture without fulfilling an autism pattern. Safeguarding concerns and medical evaluation can run in parallel. [1] [3] [6]
Clinical & Bedside Assessment
Start open: “Do you have any concerns about how your child is learning, playing, speaking or connecting with others?” Then watch the child. Note eye contact quality (not a single forced glance), response to name, pointing and showing, joint attention, imitation, play quality, and how the child uses the caregiver for comfort or sharing. [1] [4]
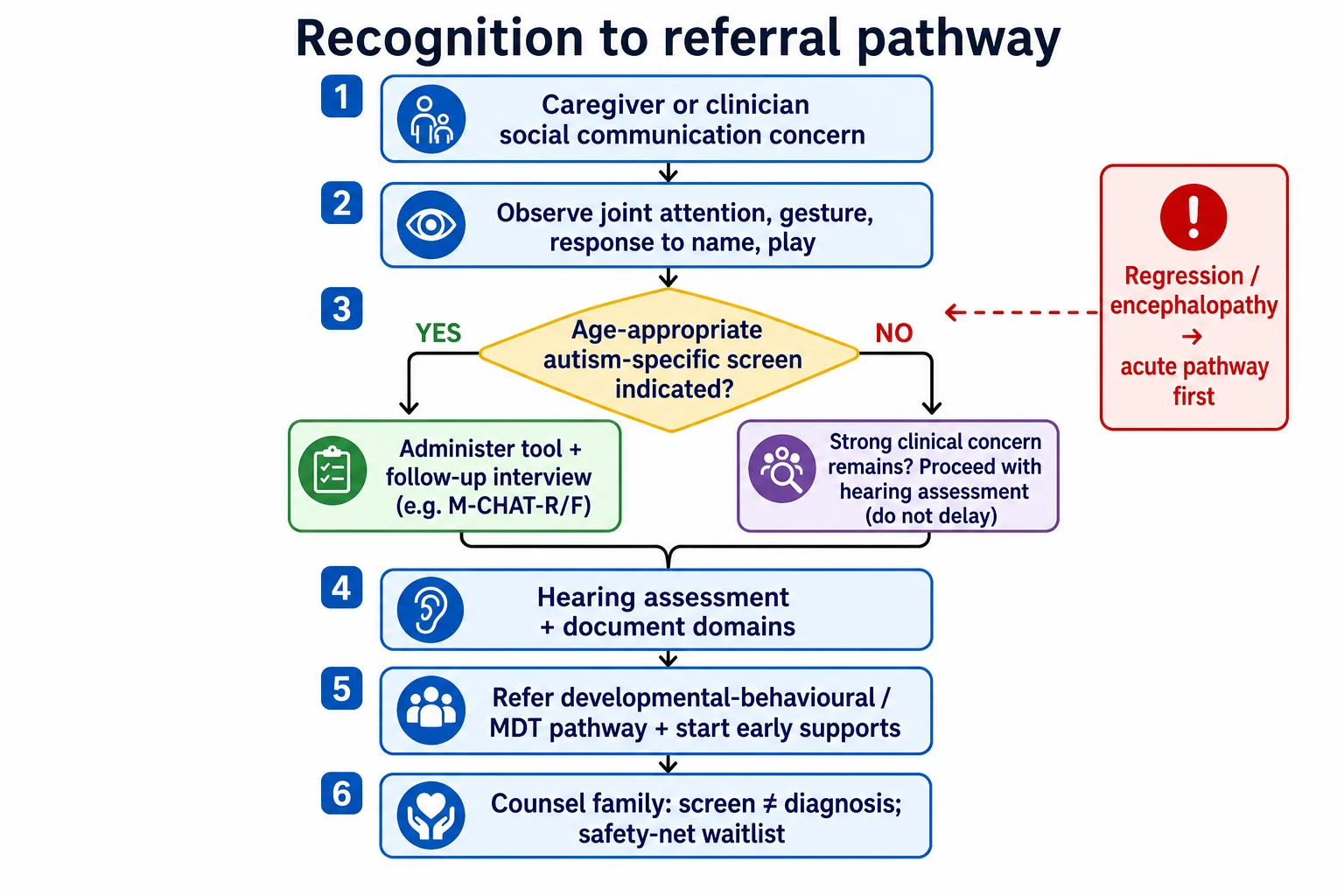
Use evidence-informed milestone lists rather than personal folklore cut-offs. When age and concern indicate, administer an autism-specific screen used by your service. For toddler risk screening supported by validation work, M-CHAT-R/F includes a follow-up interview; a single checkbox form is not a diagnosis. Strong clinical concern can justify referral even if a family declines a tool or a score is borderline. [2] [3] [4]
Document domain by domain and source-attribute who reported each skill. Hand over clearly if another clinician will complete screening. [10]
Investigations
Hearing assessment is first-line in communication concern. Vision checks when indicated. Screening guides referral; diagnostic autism instruments and most aetiology testing belong with evaluation teams unless red flags demand urgent neurology review. Avoid shotgun genetics from a single missed social skill without context. [1] [3]
Management — Resuscitation
Recognition is usually outpatient. Exceptions: acute regression with encephalopathy, new seizures, severe dehydration with collapse, or safeguarding emergencies. Those use acute paediatric pathways first; developmental referral continues after stabilisation. [1] [6]
Management — Definitive & Stepwise
- Complete surveillance and targeted observation every relevant visit.
- Deploy autism-specific screening on schedule or on concern; complete follow-up interview pathways.
- Interpret with clinical judgement — strong concern can justify referral without waiting for perfect paperwork.
- Refer early to developmental-behavioural, community paediatric and multidisciplinary pathways per local systems.
- Start concurrent early intervention and speech-language supports while diagnostic evaluation is pending.
- Counsel with teach-back: screen ≠ diagnosis; explain next steps and interim strategies.
- Safety-net the wait: what to watch for, when to return, how to chase appointments. [1] [2] [3] [7]
Consent and information-sharing principles still apply when discussing school or agency referral. [8]
Specific Subtypes & Scenarios
18–24 month well-child visit with social concern. Observe, document, use autism-specific screening with follow-up, refer early, do not book “review at three” as the only plan. [1] [2]
Late talker with warm social engagement. Prioritise hearing and speech-language pathways; still reassess social communication, not vocabulary alone. [3] [4]
School-age girl with camouflaging. Take teacher and peer-context history seriously; academic ability does not exclude autism. [1]
Medical complexity. Ask what is new for this child; avoid attributing every social difference to the known diagnosis alone. [9]
Language-discordant family. Use professional interpreters for screening questions and result counselling; never use the child as interpreter. [5]
Regression at 20–24 months. Urgent structured pathway; not routine surveillance rebooking. [1] [3]
Complications & Pitfalls
“Wait and see” after clear red flags. Treating a screen as a diagnosis. Ignoring hearing. Reassuring because the child is “bright” or “will grow out of it.” Losing families on long diagnostic waitlists without interim supports. Pathologising bilingual language patterns or cultural interaction styles without careful assessment. Incomplete handover of screening results. [1] [2] [5] [10]
Prognosis & Disposition
Earlier access to appropriate supports improves functional outcomes for many children. Disposition is refer plus interim plan, not refer-and-forget. Give concrete strategies, community contacts and a chase plan for appointments while evaluation is pending. [1] [7]
Special Populations
Siblings of autistic children need heightened surveillance. Indigenous families need culturally safe pathways and trusted local services. Migrant and refugee families need interpreters and continuity after interrupted care. Children in out-of-home care need active watching, not passive assumptions. Children with intellectual disability or sensory impairment still deserve autism-informed assessment when social communication is atypical for their baseline. Neurodiversity-affirming language can coexist with timely referral for supports. [1] [5] [6] [9]
Evidence, Guidelines & Regional Differences
Hyman and colleagues (AAP clinical report) frame identification, evaluation and management of children with ASD, including the primacy of early recognition and referral. [1] Robins and colleagues validated M-CHAT-R/F with follow-up for toddler autism risk screening. [2] Lipkin and colleagues set the broader surveillance-plus-screening framework for developmental disorders. [3] Zubler and colleagues provide evidence-informed milestone content that reduces false reassurance from outdated lists. [4]
Use jurisdictional child health books, local autism assessment pathways and early childhood intervention entry points. Cultural safety and interpreter access are part of valid recognition, not optional extras. [5]
NICE CG128 shapes recognition, referral and diagnosis thresholds; map local community paediatric, SALT and autism assessment services rather than inventing cut-offs. [1]
Bright Futures and AAP schedules drive autism screening ages; provincial and state tools vary — name the local instrument and its limits. [1] [2] [3]
Exam Pearls
- Screen is not diagnosis. [1] [2]
- Joint attention and gesture often discriminate better than word count alone. [1] [4]
- Always consider hearing in communication concern. [1] [3]
- Strong concern can justify referral even if paperwork is incomplete. [1]
- Regression is never routine wait-and-see. [1] [3]
- Safety-net the diagnostic wait with interim supports. [7]
- Document domains and hand over screening results clearly. [10]
References
- [1]Hyman SL Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics, 2020.PMID 31843864
- [2]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [3]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [4]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [5]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [6]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [7]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [8]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [9]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [10]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088