Paeds · growth-development-and-behaviour
Visual impairment and development
Also known as Childhood visual impairment · Low vision in children · Cerebral visual impairment · Cortical visual impairment · CVI · Blindness in children · Paediatric vision and development
A fellowship approach to childhood visual impairment: definitions, red-reflex and age-adapted surveillance, critical-period urgency, cerebral versus ocular pathways, developmental consequences, multidisciplinary habilitation and regional screening differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A caregiver says, “She does not look at me.” That sentence can mean cataract, ROP scars, refractive amblyopia, cerebral visual impairment, autism-spectrum difference, delayed visual maturation — or more than one of these at once. Start with what you can see and what you must not miss. Then build a plan that protects both acuity and development. [1] [2] [12]
S.I.G.H.T.
Overview & Definition
Visual impairment is reduced usable vision that limits daily function. Blindness is the severe end of that spectrum. Education systems often use “low vision” for children who need adaptations but still use residual sight. These labels are functional, not a single disease. [5] [6]
In clinic language, you need two parallel classifications. Where is the lesion? Media, retina, optic nerve, alignment/amblyopia pathway, or brain (cerebral visual impairment, CVI). How severe is the functional impact? A child may read large print yet fail in a crowded playground. Acuity alone does not equal functional vision. [8] [9] [10]
Classification
Think in four mechanism buckets, then layer urgency. [1] [8]
Media opacity includes cataract, dense corneal opacity and vitreous haze. These block focused light and can create deprivation amblyopia fast. Retina and optic nerve disease includes ROP sequelae, retinal dystrophies and optic atrophy. Amblyopia pathway includes strabismus, anisometropia and deprivation without total blindness. CVI is disordered visual processing from brain injury or maldevelopment, often with a relatively normal structural eye examination. [8] [9] [17] [21]
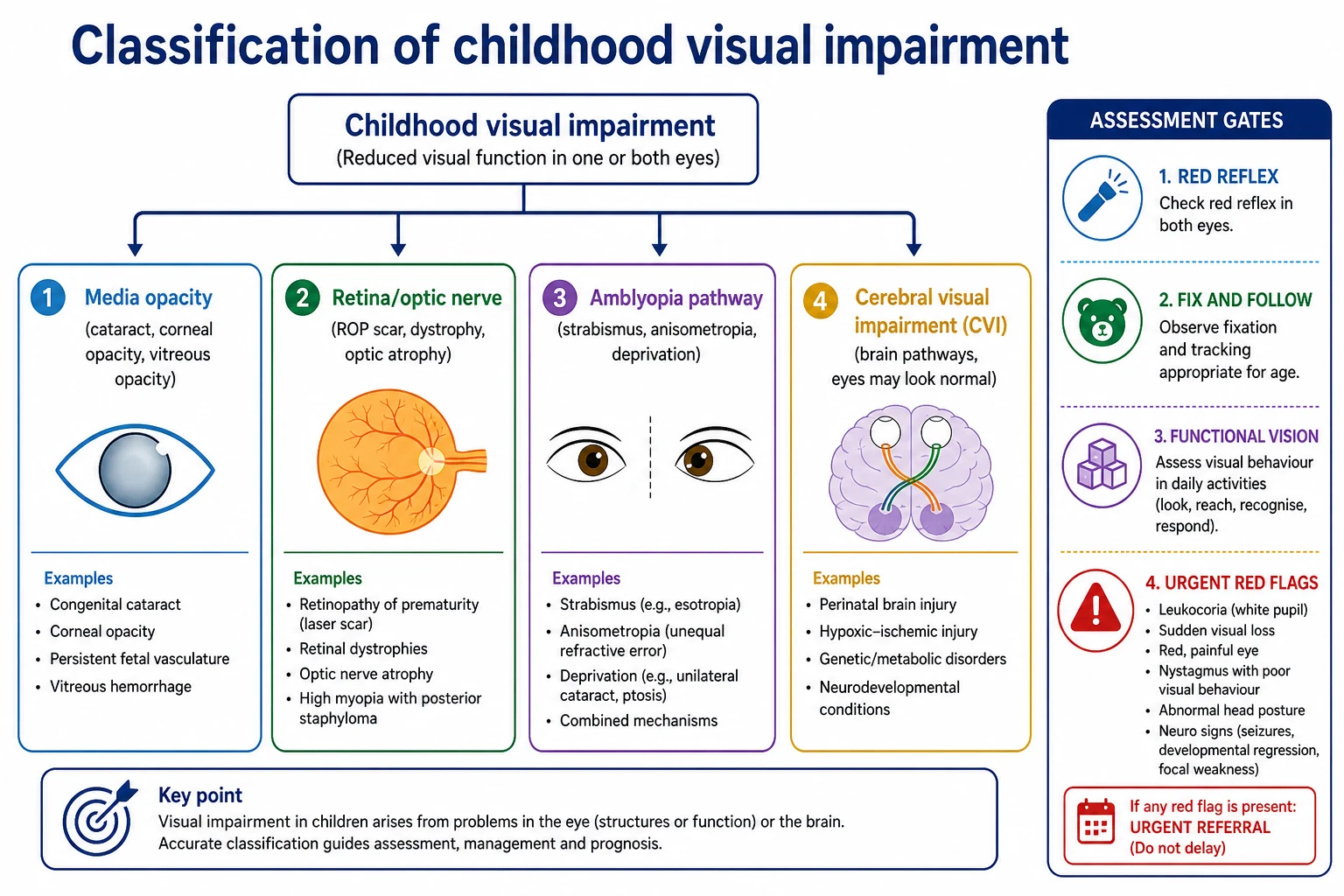
Delayed visual maturation is a temporary lag in visual behaviour in some infants who later improve. It is a diagnosis of careful follow-up, not a first-day label that closes the differential. Progressive loss, abnormal red reflex or neurological red flags never wait for “watchful waiting.” [1] [23]
Epidemiology & Risk Factors
Childhood blindness remains a major global disability, with cause mix that shifts by region and over time. In many high-income settings, prematurity-related disease, CVI and complex neurodisability dominate residual severe impairment. In many lower-resource settings, avoidable causes such as cataract, infection and nutritional pathways still matter heavily. [5] [6] [7]
Risk clusters you must name in exams: extreme prematurity and ROP pathways; perinatal hypoxic–ischaemic injury and periventricular leukomalacia; congenital infection; genetic and syndromic disease; family history of early cataract or retinal dystrophy; delayed access to care. [7] [20] [25]
Inequity is not a soft add-on. Missed newborn red-reflex checks, long waits for paediatric ophthalmology, and school systems without low-vision support convert treatable problems into lifelong disability. Rural, Indigenous, migrant and socioeconomically disadvantaged families carry that burden disproportionately. [5] [6] [24]
Pathophysiology
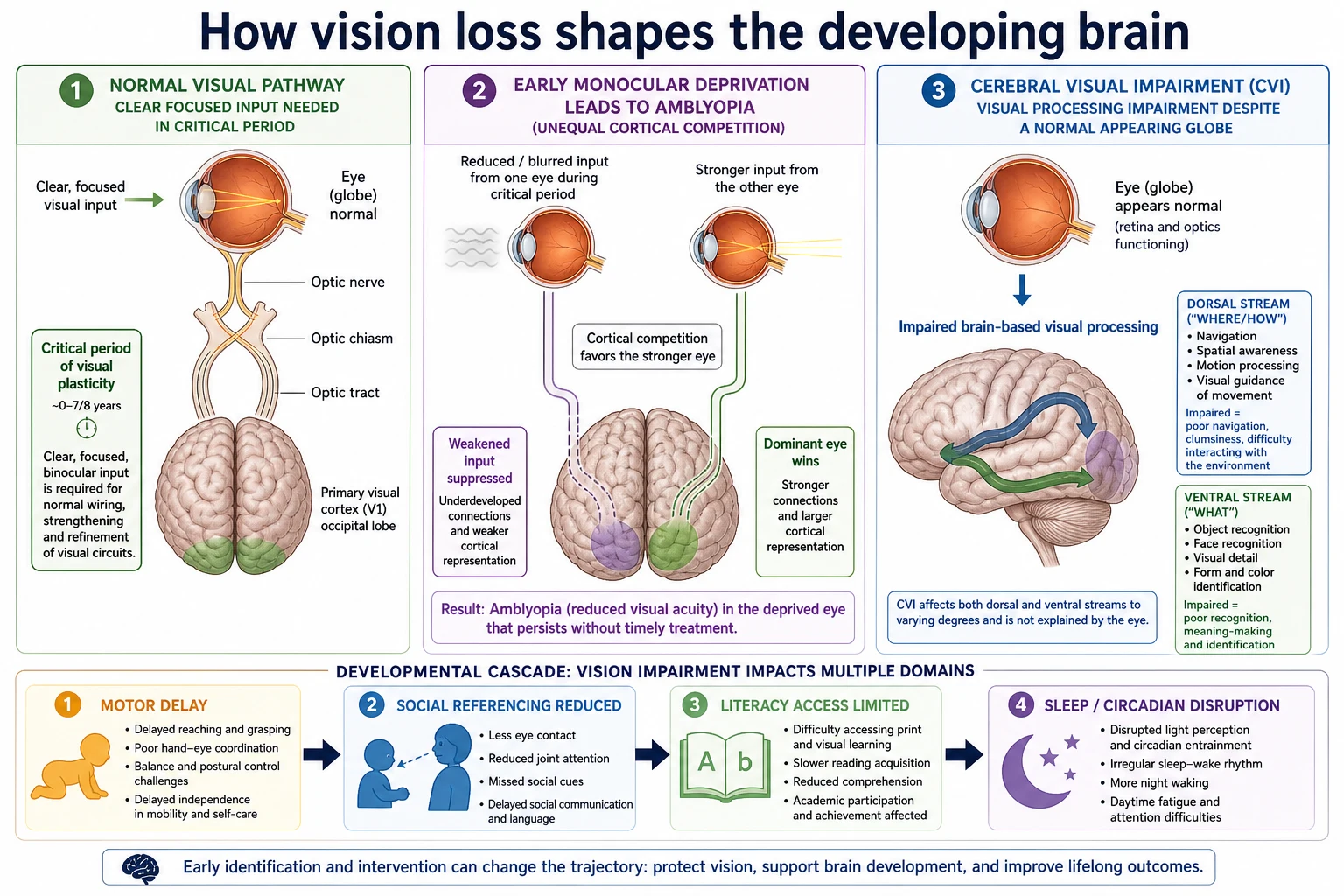
The infant visual cortex expects focused, binocular input during a critical period. If one eye is blocked by dense cataract or ptosis, cortical territory is reassigned. That is amblyopia: a brain consequence of unequal competition, not “lazy character.” Early treatment of the amblyogenic cause protects plasticity. Delay costs acuity that may not fully return. [15] [16]
CVI is different mechanics. The globe may form a clear image, but dorsal-stream networks that guide movement through space, and ventral-stream networks that support recognition, fail after early brain injury. Children may see better in quiet, high-contrast settings and collapse in clutter. That variability confuses families and examiners who only test letter charts in calm rooms. [8] [10] [11]
Reduced vision then cascades. Motor planning relies on visual feedback. Social referencing uses faces. Literacy depends on print access. Severe congenital visual impairment also disrupts light-based circadian cues and sleep. Development is not a side topic after the eye appointment; it is part of the disease course. [18] [19]
Clinical Presentation
Infants may not fix or follow, show roving eye movements, or prefer light gazing. Parents notice missing social smile visual components or “looking through” people. Toddlers may hold objects very close, bump furniture, tilt the head, or avoid fine motor tasks that need vision. [1] [2]
School-age children may present as “behaviour” or “learning difficulty.” They copy slowly from the board, tire with reading, or refuse sports that need depth judgement. CVI-specific clues include trouble finding a toy on a patterned carpet, fear of busy corridors, and better performance with one object at a time. [9] [11] [22]
Time-critical presentations include leukocoria, acute strabismus with neurological signs, sudden visual behaviour collapse, and the neonate with an absent red reflex. These are not routine clinic deferrals. [3] [17]
Differential Diagnosis
Rank by threat and mechanism. First exclude media opacity and neuro-ophthalmic emergencies. Then separate refractive/amblyopia risk factors, retinal or optic-nerve disease, delayed visual maturation, and CVI. Always ask whether hearing and global development are also off track. [1] [8] [12]
Poor eye contact is a differential item, not a diagnosis. Autism-spectrum social-communication difference can reduce eye contact with preserved visual acuity. CVI and intellectual disability can co-occur with autism features. Dual labels are common and must not cancel vision assessment. [12]
Progressive night vision loss raises retinal dystrophy concern. Raised intracranial pressure or compressive lesions enter when there is headache, sixth-nerve palsy, optic disc swelling or progressive field-like behaviour. Neurodegenerative disease is uncommon but cannot be ignored when regression accompanies visual loss. [5] [10]
Clinical & Bedside Assessment
Structure the visit. Start with caregiver concern in their words. Ask about fixing, following, eye preference, photophobia, night vision, head posture, navigation at home, school performance and family eye disease. Add perinatal risk: gestation, ROP screening, HIE, seizures, brain imaging. [1] [2]
Examine the red reflex in a darkened room using a direct ophthalmoscope. Symmetric red or orange glow is reassuring; white, dark, or asymmetric reflexes need urgent ophthalmology. Age-adapt the rest: fix-and-follow in infants, preferential looking concepts in toddlers, and symbol or letter acuity when the child can participate. Check pupils, lids, alignment, nystagmus and external eye. [2] [3] [24]
Then test functional vision, not only chart acuity. Watch reaching accuracy, obstacle negotiation, face interest and performance in clutter. In children with cerebral palsy or PVL history, keep CVI high on the pretest list even if the globe looks quiet. [9] [14] [20]
Investigations
For most primary and general paediatric presentations, the first “test” is a competent eye examination by ophthalmology or an established paediatric eye pathway. Abnormal red reflex, leukocoria concern, suspected congenital cataract, and acute neuro signs are referral triggers, not invitations to order random bloods first. [1] [3] [17]
Instrument-based vision screening can help in primary care when age-appropriate optotype testing is not yet possible, but it does not replace red-reflex checks or clinical judgement. A “normal” instrument screen does not cancel caregiver concern or neurological red flags. [4]
After ophthalmology triage, neuroimaging, electrophysiology (VEP/ERG) and genetics are selected for the working diagnosis — for example, CVI with brain injury context, suspected dystrophy, or optic neuropathy — not as a shotgun panel for every low acuity. [10] [11]
Management — Resuscitation
Start with threat. Leukocoria is retinoblastoma until proven otherwise in the exam mindset: urgent specialist review the same day or next available emergency eye pathway, not a routine waitlist. Acute visual behaviour change with systemic illness needs ABCDE, glucose and neurology/ophthalmology escalation. [3] [5]
The neonate or young infant with absent red reflex or suspected dense cataract needs time-critical ophthalmology. Critical-period biology means “soon” is not a soft word. Stabilise the child, arrange transfer if local capability is thin, and document the handoff. [16] [17]
Safeguarding sits in parallel when unexplained injury, neglected follow-up of known disease, or care refusal blocks sight-saving treatment. Stabilise vision care and escalate welfare pathways factually. [1]
Management — Definitive & Stepwise
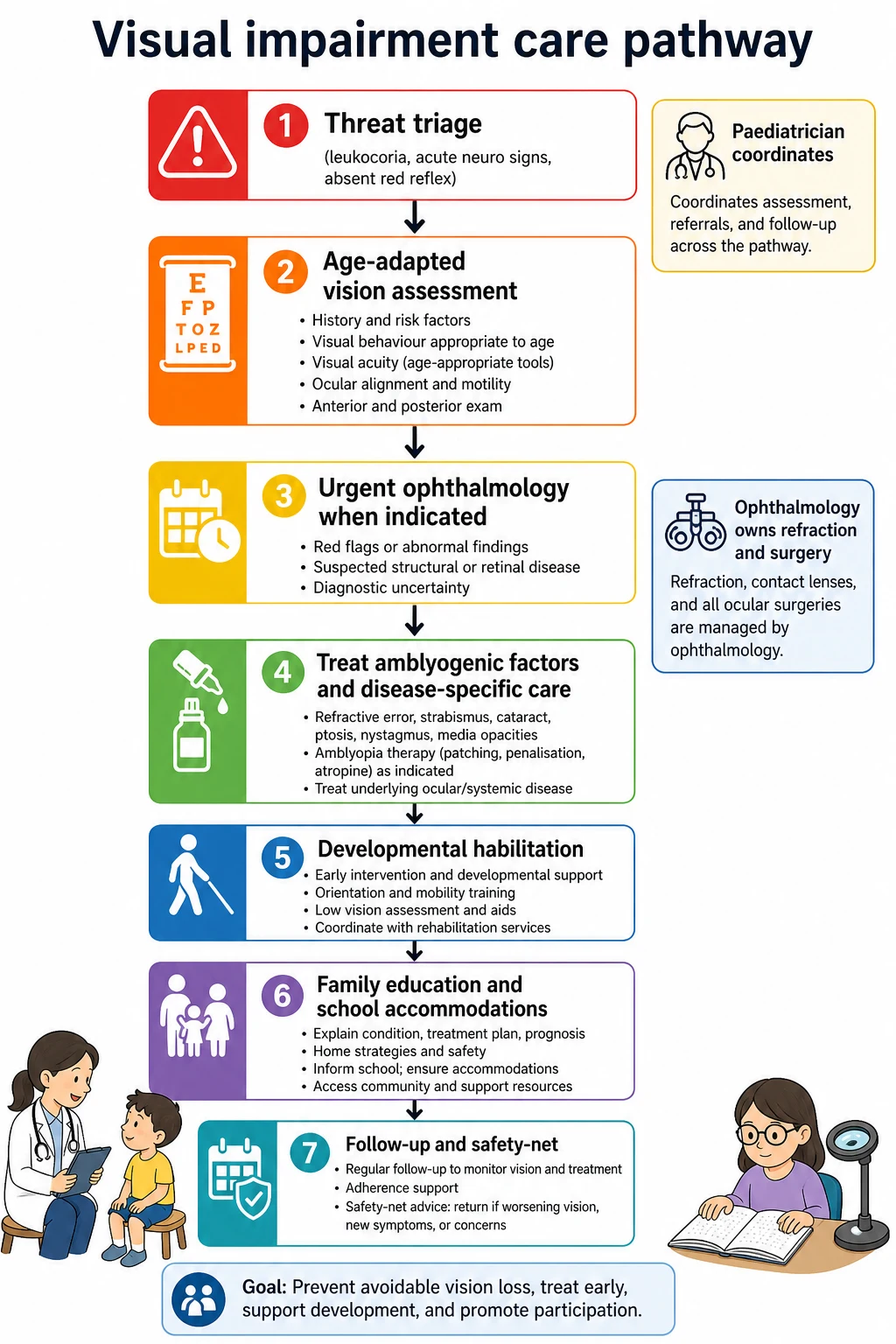
After threat is gated, run a stepwise plan. Confirm measurements and functional impact. Secure specialty diagnosis and treat amblyogenic factors (optics, occlusion strategies as directed by ophthalmology, timely cataract pathways). Start developmental habilitation without waiting for a perfect final acuity number. [13] [15]
The paediatrician’s ongoing role is coordination: early intervention referral, orientation and mobility supports, low-vision aids through specialist services, sleep review, hearing check, and school accommodations. Write goals in functional language: “navigate classroom safely,” “access large-print or audio curriculum,” “recognise caregivers in quiet lighting.” [13] [18]
Set follow-up by age and diagnosis. Young infants need short-interval review of visual behaviour. School-age children need planned checks around curriculum transitions. Safety-net any new white pupil, new nystagmus, sudden drop in function, or caregiver concern. [1] [19]
High-yield anchors
Specific Subtypes & Scenarios
Congenital cataract. Early dense bilateral cataract is a plasticity emergency. Arrange specialist surgery pathways promptly and plan intensive amblyopia care after. Unilateral dense cataract also needs urgency because monocular deprivation is highly amblyogenic. [16] [17]
ROP graduate. Residual field or acuity limits can coexist with broader neurodevelopmental risk. Screening history is not the whole story; follow function and development after discharge from ROP clinics. [25]
CVI with cerebral palsy or PVL. Expect mixed motor and visual disability. Teach families that “the eyes look fine” does not equal safe navigation. Environmental simplification and specialist CVI strategies help. [14] [20]
School-age refractive amblyopia. Behaviour and reading complaints may be optical. Correct refractive error before long behavioural labels stick. [15]
Leukocoria pathway. Same-day urgency. Do not dilate and discharge without a clear specialist plan if retinoblastoma remains plausible. [3] [5]
Dual sensory impairment. Vision plus hearing multiplies developmental risk. Escalate specialised early intervention early. [1] [18]
Complications & Pitfalls
Missing an abnormal red reflex is the classic catastrophe. Labelling poor eye contact as autism without vision assessment is the modern twin trap. Assuming a normal structural eye exam excludes CVI is the third. [3] [12] [22]
Other pitfalls: delaying cataract referral; treating chart acuity only and ignoring mobility and literacy access; missing sleep disruption in severe VI; failing to use interpreters when taking visual history; and fragmenting care so ophthalmology, paediatrics and school never share one plan. [16] [18] [19]
Prognosis & Disposition
Prognosis follows cause, timing and habilitation. Early treated amblyogenic factors can recover substantial function. Some retinal and optic-nerve diseases progress despite best care. CVI trajectories vary; many children gain usable strategies even when acuity remains limited. [10] [14] [15]
Discharge to community care only after threat is excluded or specialist ownership is clear, a functional plan exists, and caregivers know return triggers. Long-term planning includes education access, orientation–mobility, mental health, and adolescent transition of eye and disability supports. [13] [18]
Special Populations
Preterm and ROP-screened infants need ongoing developmental vision surveillance after acute ROP risk fades. [25]
Children with cerebral palsy and PVL carry high CVI pretest probability. [14] [20]
Autism and intellectual disability populations need dual-diagnosis thinking without diagnostic overshadowing. [12]
Indigenous, rural, migrant and refugee families need culturally safe communication, interpreters and active barrier-busting for ophthalmology access. [5] [6] [24]
Adolescents need identity-sensitive low-vision technology plans and transition of care, not only paediatric clinic letters. [18]
Evidence, Guidelines & Regional Differences
AAP statements define what paediatricians must do at the bedside: structured visual system assessment, procedure detail, red-reflex examination, and the place of instrument-based screening. These are high-yield primary sources for multi-board exams. [1] [2] [3] [4]
Solebo, Gilbert and Kong frame epidemiology and preventable burden. CVI literature from Dutton through Chang, Ortibus, Chokron, Delay and Galli builds modern recognition and habilitation thinking. Amblyopia PPP and cataract timing papers defend urgency language. [5] [6] [7] [8] [10] [13] [15] [16]
Use local newborn and child health record checks, state vision programmes and paediatric ophthalmology pathways. Pair vision concern with culturally safe family support and school learning-access plans. [1] [3]
Expect newborn and child surveillance language plus special educational needs frameworks for classroom adaptations. Keep red-flag urgency identical even when service names differ. [5] [8]
Lean on AAP visual system assessment, red-reflex policy and instrument-based screening statements for primary-care structure; AAO amblyopia PPP for treatment principles. [1] [3] [4] [15]
Provincial screening access varies; defend the same clinical red flags and early habilitation principles while following local referral routes. [1] [10]
Exam Pearls
- Red reflex first: asymmetry or white is urgent. [3]
- Critical period: early dense cataract is time-sensitive. [16]
- CVI: normal-looking eyes can still mean major functional vision loss. [8] [22]
- Quiet-room acuity ≠ busy-world vision. [11]
- Poor eye contact ≠ skip the eye exam. [12]
- Amblyopia is cortical plasticity disease — treat drivers early. [15]
- Habilitate while you investigate; do not wait for perfect labels. [13]
- Sleep is part of severe VI care. [19]
- ROP graduates need developmental follow-through. [25]
- Safety-net caregiver concern that vision is worse. [1]
References
- [1]Donahue SP Visual System Assessment in Infants, Children, and Young Adults by Pediatricians. Pediatrics, 2016.PMID 29756730
- [2]Donahue SP Procedures for the Evaluation of the Visual System by Pediatricians. Pediatrics, 2016.PMID 26644488
- [3]American Academy of Pediatrics Red reflex examination in neonates, infants, and children. Pediatrics, 2008.PMID 19047263
- [4]Miller JM Instrument-based pediatric vision screening policy statement. Pediatrics, 2012.PMID 23109679
- [5]Solebo AL Epidemiology of blindness in children. Archives of disease in childhood, 2017.PMID 28465303
- [6]Gilbert C Childhood blindness in the context of VISION 2020--the right to sight. Bulletin of the World Health Organization, 2001.PMID 11285667
- [7]Kong L An update on progress and the changing epidemiology of causes of childhood blindness worldwide. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus, 2012.PMID 23237744
- [8]Dutton GN Cerebral visual impairment in children. Seminars in neonatology : SN, 2001.PMID 12014888
- [9]Philip SS Identifying and characterising cerebral visual impairment in children: a review. Clinical & experimental optometry, 2014.PMID 24766507
- [10]Chang MY Advances in the evaluation and management of cortical/cerebral visual impairment in children. Survey of ophthalmology, 2020.PMID 32199940
- [11]Ortibus E Cerebral Visual Impairment and Clinical Assessment: The European Perspective. Seminars in pediatric neurology, 2019.PMID 31548019
- [12]Chokron S The inter-relationships between cerebral visual impairment, autism and intellectual disability. Neuroscience and biobehavioral reviews, 2020.PMID 32298709
- [13]Delay A Interventions for children with cerebral visual impairment: A scoping review. Developmental medicine and child neurology, 2023.PMID 36217216
- [14]Galli J Natural history of cerebral visual impairment in children with cerebral palsy. Developmental medicine and child neurology, 2025.PMID 39316724
- [15]Wallace DK Amblyopia Preferred Practice Pattern. Ophthalmology, 2018.PMID 29108744
- [16]Birch EE The critical period for surgical treatment of dense congenital bilateral cataracts. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus, 2009.PMID 19084444
- [17]Chan WH Congenital and infantile cataract: aetiology and management. European journal of pediatrics, 2012.PMID 22383071
- [18]Erickson KA Literacy and visual impairment. Seminars in speech and language, 2007.PMID 17340383
- [19]Ingram DG Sleep Challenges and Interventions in Children With Visual Impairment. Journal of pediatric ophthalmology and strabismus, 2022.PMID 34435902
- [20]Petri S Visual impairment and periventricular leukomalacia in children: A systematic review. Research in developmental disabilities, 2023.PMID 36796269
- [21]Khetpal V Cortical visual impairment: etiology, associated findings, and prognosis in a tertiary care setting. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus, 2007.PMID 17459745
- [22]Bowman R Cerebral visual impairment. Community eye health, 2024.PMID 38836256
- [23]Ospina LH Cortical visual impairment. Pediatrics in review, 2009.PMID 19884281
- [24]Mndeme FG Red reflex examination in reproductive and child health clinics for early detection of paediatric cataract and ocular media disorders: cross-sectional diagnostic accuracy and feasibility studies from Kilimanjaro, Tanzania. Eye (London, England), 2021.PMID 32546747
- [25]Karmouta R Neurodevelopmental Outcomes in Infants Screened for Retinopathy of Prematurity. JAMA ophthalmology, 2023.PMID 37883103