Paeds · haematology-oncology-and-transfusion
Long-term follow-up and late effects of childhood cancer
Also known as Childhood cancer survivorship · Late effects of childhood cancer therapy · Long-term follow-up after childhood cancer · Paediatric cancer survivor · Anthracycline cardiomyopathy · Radiation-associated second malignancy · Endocrine late effects of cancer therapy · Cancer survivorship transition
Fellowship guide to the long-term follow-up and late effects of childhood cancer. Covers the survivor as the success story of modern oncology with over eighty percent five-year survival and the simultaneous burden of the chronic health conditions that follow the cure, the organ-system late effects of endocrine failure with growth hormone deficiency and hypothyroidism, anthracycline cardiomyopathy, subsequent malignancies, neurocognitive decline and infertility, the treatment-summary-driven and risk-stratified lifelong surveillance built on the Children's Oncology Group and the Dutch Late Effects guidelines, the surveillance for breast cancer after chest radiation and cardiomyopathy after anthracycline exposure, and the structured transition of the adolescent survivor to the adult late-effects service.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A young woman walks into the general paediatric clinic at the age of twenty-two, fifteen years after she received chemotherapy and chest radiation for a Hodgkin lymphoma as a child, and the question that frames her whole visit is not whether the lymphoma will return but what the treatment that cured her is now doing to her heart, her breasts, her thyroid and her fertility. The long-term follow-up of the childhood cancer survivor is the discipline that grew out of the single greatest success of modern paediatric oncology, which is that over eighty percent of children diagnosed with cancer in the high-income countries now survive five years from the diagnosis. The survival that was unimaginable sixty years ago, when fewer than one in ten children with cancer survived, has created a growing population of survivors whose cure was bought at the price of the late effects of the surgery, the radiotherapy and the chemotherapy that saved them. [1][2]
A late effect is defined as a chronic or a late-occurring physical or psychological complication that persists or emerges after the cancer treatment has ended, and it is the direct consequence of the exposure to the cytotoxic therapy and not of the cancer itself. The late effects are distinguished from the long-term effects, which are present during or immediately after the treatment, by their delayed onset, because many declare themselves years or decades after the exposure. The anthracycline cardiomyopathy, the radiation-associated second malignancy, the growth hormone deficiency and the premature ovarian failure are the archetypes, and each follows the specific treatment exposure with a latency that can stretch across the decades of the survivor's adult life. [3][5]
The scale of the burden is what gives the topic its weight, and the single most cited figure is that nearly three quarters of the adult survivors of childhood cancer carry at least one chronic health condition, and that over forty percent carry a condition that is severe, life-threatening or disabling. The cumulative incidence of the chronic conditions rises with the time from the diagnosis, so that the longer the survivor lives the more likely the late effect, and the survivor who reaches the age of fifty carries the health profile of a person a generation older. The late effects are therefore not the rare complications of a fortunate few but the expected companion of the cure, and the task of the clinician is to anticipate, to detect and to mitigate them across the survivor's life. [1]
The framework that organises the whole topic is the link between the treatment exposure and the late effect, because every surveillance decision is driven by what the child received. The anthracycline dose predicts the cardiomyopathy, the chest radiation field and dose predict the breast cancer, the cranial radiation predicts the neurocognitive decline and the growth hormone deficiency, the alkylating agent dose predicts the gonadal failure, and the platinum compound predicts the ototoxicity. The fellow who holds these exposure-to-effect links can build the surveillance plan from the treatment summary alone, and the plan is what separates the child who is followed from the child who is lost to the late effects. [2][12]
Classification
The most useful classification of the late effects at the bedside is by the organ system, because the surveillance and the intervention are organised by the system. The endocrine late effects lead the burden, with the growth hormone deficiency, the central and the primary hypothyroidism, the disorders of puberty, the adrenal insufficiency and the gonadal failure. The cardiac late effects follow, with the anthracycline cardiomyopathy and the radiation-associated valvular and the coronary disease. The subsequent malignancies are the most feared, with the breast cancer after the chest radiation, the thyroid cancer after the neck radiation, the central nervous system tumour after the cranial radiation, and the therapy-related myelodysplasia and leukaemia after the chemotherapy. [3][4]
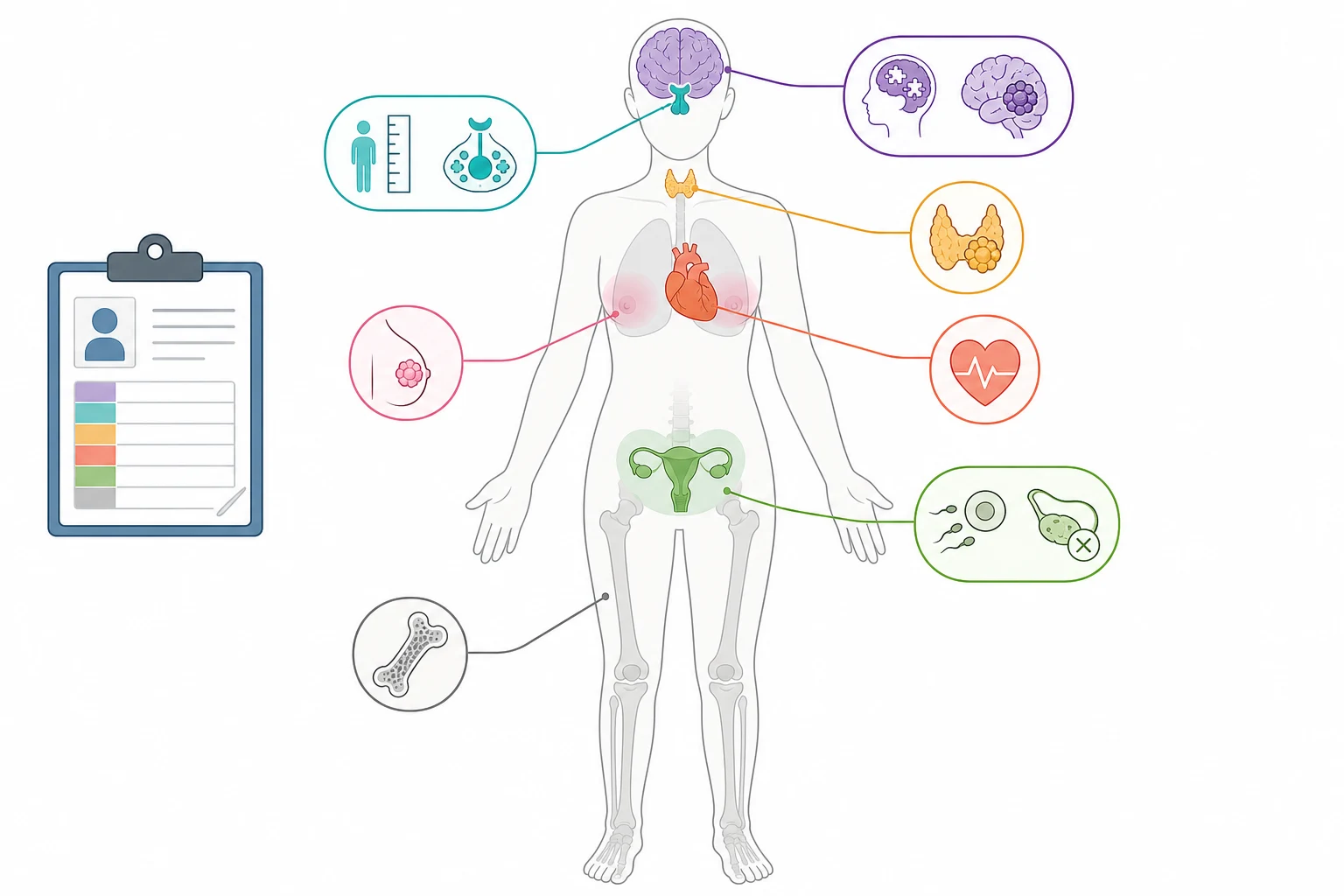
The neurocognitive late effects hold a special place, because they strike the developing brain and they shape the survivor's ability to learn, to work and to live independently. The cranial radiation, the intrathecal chemotherapy and the prolonged absences from the school together produce the attention deficit, the processing-speed slowing, the executive dysfunction and the memory impairment, and the youngest child at the treatment and the highest radiation dose carry the worst burden. The pulmonary, the renal and the musculoskeletal late effects complete the system list, with the pulmonary fibrosis after the bleomycin and the chest radiation, the renal impairment after the nephrotoxic chemotherapy, and the growth failure and the osteoporosis that span the endocrine and the skeletal systems. [8]
A parallel and equally important classification runs through the treatment modality that caused the late effect, because the exposure history is what drives the surveillance. The radiotherapy late effects are field-dependent and dose-dependent, so that the chest radiation predicts the breast and the cardiac disease, the neck radiation predicts the thyroid disease, and the craniospinal radiation predicts the neurocognitive, the endocrine and the second central nervous system tumour. The chemotherapy late effects are drug-dependent and cumulative-dose-dependent, so that the anthracycline predicts the cardiomyopathy, the alkylating agents predict the gonadal failure and the therapy-related leukaemia, the platinum compounds predict the ototoxicity and the renal impairment, and the bleomycin predicts the pulmonary fibrosis. [2][6]
Anthracycline cardiomyopathy
dose-dependent cardiac
- Cumulative doxorubicin-equivalent dose drives the risk
- High risk at two hundred and fifty milligrams per square metre or more
- Progressive and may declare years to decades after the exposure
- Lifelong echocardiographic surveillance is mandatory
Radiation-associated breast cancer
after chest radiation
- Chest radiation of twenty gray or more is the high-risk exposure
- Annual mammography and breast magnetic resonance imaging
- Begins eight years after the radiation or at age twenty five, whichever is later
- The most common subsequent malignancy in the female survivor
Growth hormone deficiency
after cranial radiation
- Cranial radiation of eighteen gray or more raises the risk
- Declares as the growth failure and the short stature
- Recombinant growth hormone replacement if no contraindication
- Younger age at treatment carries the higher risk
Gonadal failure
after alkylating agents
- Cyclophosphamide-equivalent dose predicts the gonadotoxicity
- Premature ovarian failure in the female survivor
- Azoospermia and infertility in the male survivor
- Fertility preservation before the gonadotoxic therapy
Epidemiology & Risk Factors
The epidemiology of the late effects is built on the Childhood Cancer Survivor Study, the St Jude Lifetime Cohort, and the national registries, and it is the reason the burden is now so precisely quantified. The over eighty percent five-year survival of the childhood cancer, across the high-income countries, has created an estimated population of over five hundred thousand survivors in the United States alone, and a comparable and growing population across Europe and Australasia. The age of the survivor at the assessment matters, because the cumulative incidence of the chronic conditions rises steeply with the time from the diagnosis, and the survivor who reaches the age of fifty carries a burden that the non-survivor peer does not encounter until a generation later. [1][2]
The landmark figure that every fellow must carry is that nearly three quarters of the adult survivors of childhood cancer carry at least one chronic health condition, and that over forty percent carry a severe, life-threatening or disabling condition, as the Childhood Cancer Survivor Study reported in the New England Journal of Medicine. The severe conditions include the second malignancy, the congestive heart failure, the cerebrovascular event and the end-stage renal disease, and they are the reason the survivor carries a higher risk of the premature death than the general population. The leading causes of the premature death in the survivor are the second malignancy, the cardiac disease and the recurrence of the original cancer, in that order, and the surveillance is built to intercept each. [1][5]
The risk factors for the late effects are the treatment exposures, the age at the treatment, the sex and the genetic susceptibility, and the treatment exposures are by far the most important. The higher the cumulative anthracycline dose, the higher the chest and the cranial radiation dose, and the higher the alkylating agent dose, the greater the risk of the corresponding late effect. The younger age at the treatment raises the risk of the neurocognitive decline and the growth hormone deficiency, because the developing brain and the growing skeleton are the most vulnerable. The female sex raises the risk of the breast cancer after the chest radiation and the anthracycline cardiomyopathy, and the genetic susceptibility, such as the Li-Fraumeni syndrome, raises the risk of the second and the third malignancy. [3][6]
The contemporary risk profile is changing, because the treatment protocols have been de-escalated to reduce the late effects, and the fellow must hold the historical and the contemporary exposures side by side. The modern protocols use the lower anthracycline doses, the proton therapy to reduce the exit radiation dose, and the avoidance of the cranial radiation in the favourable-risk leukaemia, and the survivor treated in the current era carries a lower late-effect burden than the survivor treated thirty years ago. The surveillance must nonetheless follow every survivor, because even the contemporary exposure carries a non-trivial risk, and the survivor lost to the follow-up is the one whose late effect is detected late. [2][10]
Pathophysiology
The pathophysiology of the late effects is the cellular and the molecular injury that the cytotoxic therapy inflicts on the normal tissue, and it is the reason the late effect follows the specific exposure. The anthracycline cardiomyopathy is the paradigm, and it begins with the uptake of the anthracycline into the cardiomyocyte, where it generates the reactive oxygen species, it damages the mitochondrial DNA, and it injures the topoisomerase two beta, the enzyme that maintains the cardiomyocyte genome. The cardiomyocyte is a terminally differentiated cell that cannot regenerate, so that the cumulative cell loss is irreversible, and the progressive decline in the left ventricular function follows the dose, with the dysfunction that can remain silent for years before the heart failure declares. [5][6]
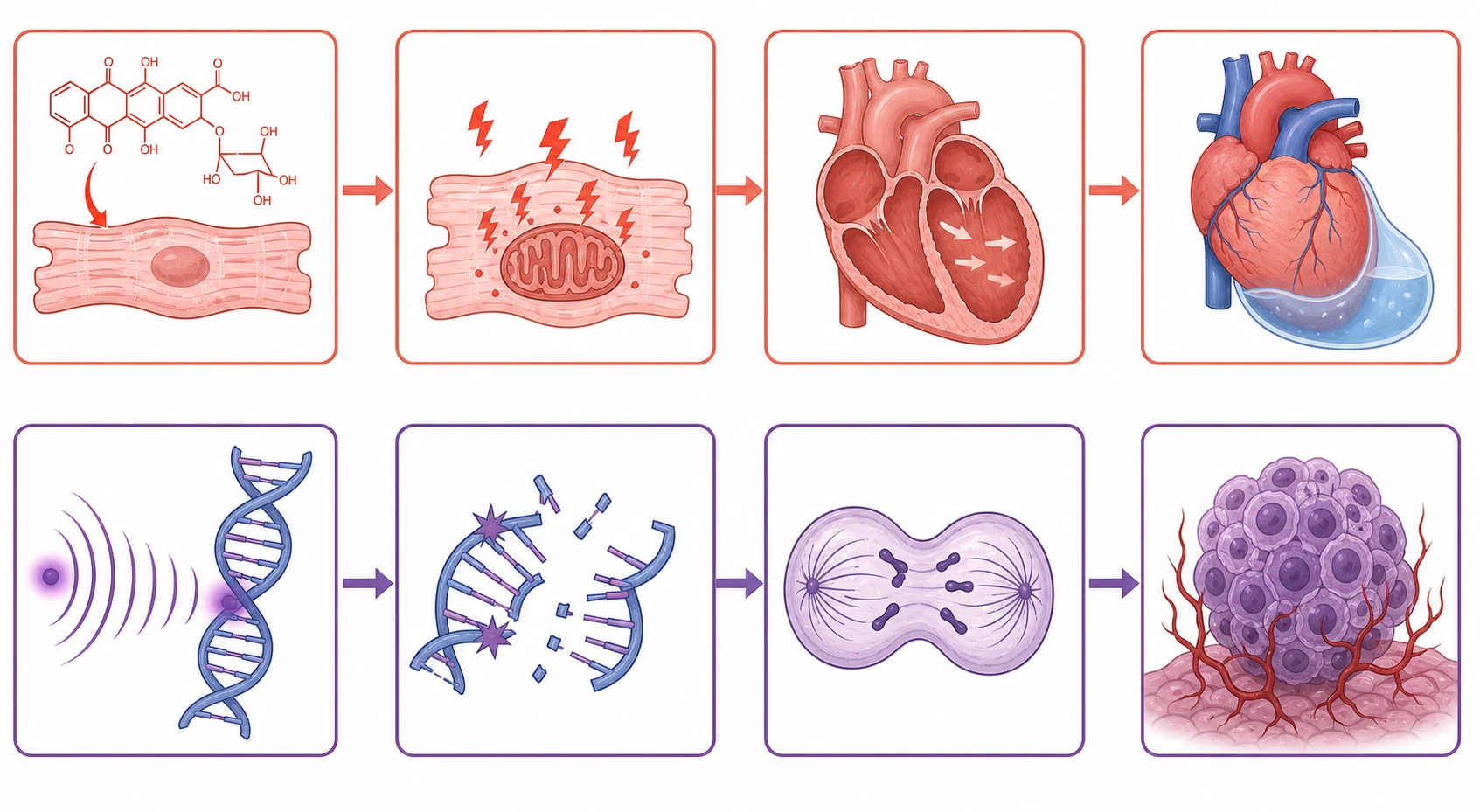
The radiation late effects run through the injury to the vasculature, the growing tissue and the genome, and they explain the breadth of the radiation-associated burden. The radiation damages the small vessels and produces the vascular fibrosis that drives the coronary and the cerebrovascular disease, it injures the growth plate and the hypothalamic-pituitary axis to produce the growth failure, and it induces the DNA double-strand breaks that, if misrepaired, seed the second malignancy in the irradiated field. The breast tissue of the pubertal girl is exquisitely sensitive, so that the chest radiation during the puberty carries the highest breast cancer risk, and the thyroid and the central nervous system carry their own field-specific risks. [4][9]
The endocrine late effects run through the injury to the hypothalamic-pituitary axis and the end-organ glands, and they are the commonest of the late effects because the axis is so vulnerable. The cranial radiation damages the hypothalamic-pituitary cells in a dose-dependent and a hormone-specific pattern, so that the growth hormone deficiency appears at the lower doses, the gonadotropin and the adrenocorticotropin deficiency at the higher doses, and the thyroid-stimulating-hormone deficiency at the highest doses. The radiation and the iodine-based radiotherapy damage the thyroid directly to produce the primary hypothyroidism, and the alkylating agents and the radiation damage the germ cells to produce the gonadal failure. The result is the survivor who may need the growth hormone, the levothyroxine, the hydrocortisone and the sex-steroid replacement across the life. [3][7]
The neurocognitive late effects run through the injury to the developing white matter, and they are the reason the cranial radiation is avoided wherever possible in the youngest children. The radiation and the intrathecal chemotherapy injure the white matter tracts and the hippocampal neurogenesis, and they produce the attention deficit, the processing-speed slowing and the executive dysfunction that declare as the academic decline. The mechanism explains why the youngest child at the treatment carries the worst burden, because the brain is in the phase of the most rapid myelination and the synaptogenesis, and the injury at this window is the most damaging. [8]
Clinical Presentation
The childhood cancer survivor presents to the clinician in one of several ways, and the recognition of the presentation is what decides whether the late effect is anticipated or missed. The first is the routine survivorship visit, where the asymptomatic survivor attends the late-effects clinic for the surveillance, and the late effect is detected by the screening test before it declares clinically. The second is the symptomatic presentation, where the survivor presents with the growth failure, the fatigue, the exercise intolerance or the new mass that is the clinical declaration of a late effect. The third is the acute presentation, where the survivor presents with the decompensated heart failure, the adrenal crisis or the symptomatic second malignancy that is the late effect at its most dangerous. [2][5]
The endocrine presentation is the commonest, and it spans the growth, the thyroid, the puberty, the adrenal and the reproductive axes. The growth failure and the short stature follow the growth hormone deficiency, and they are the presentation that the primary care clinician and the parent notice first. The fatigue, the weight gain and the cold intolerance follow the hypothyroidism. The delayed or the absent puberty and the amenorrhoea follow the gonadal failure, and the young woman with the premature ovarian failure presents with the infertility that is the late effect most distressing to the survivor. The adrenal insufficiency presents with the fatigue and the hypotension, and the adrenal crisis presents with the shock and the hyponatraemia that is the preventable death if unrecognised. [3][7]
The cardiac presentation spans the asymptomatic dysfunction, the symptomatic heart failure and the arrhythmia. The survivor with the anthracycline cardiomyopathy may present with the exercise intolerance, the dyspnoea, the peripheral oedema or the orthopnoea of the congestive heart failure, or with the palpitations and the syncope of the arrhythmia. The survivor with the radiation-associated cardiac disease may present with the valvular disease, the pericardial disease or the premature coronary disease, depending on the radiation field and the dose. The cardiac late effect is one of the leading causes of the premature death in the survivor, which is why the cardiac surveillance is among the most heavily weighted in the examination. [5]
The subsequent malignancy is the most feared presentation, and it is the one that the surveillance is built to intercept at the earliest stage. The breast cancer after the chest radiation presents with the palpable mass or the screening abnormality, and the surveillance mammography and the magnetic resonance imaging are designed to catch it before it becomes palpable. The thyroid cancer after the neck radiation presents with the palpable thyroid nodule, and the annual thyroid examination and the ultrasound are the surveillance. The central nervous system tumour after the cranial radiation presents with the new headache, the seizure or the focal deficit, and the magnetic resonance imaging is the test. The therapy-related myelodysplasia and leukaemia present with the cytopenia and the marrow dysplasia, and they carry a poor prognosis. [4][9]
Differential Diagnosis
The differential diagnosis of the symptom in the childhood cancer survivor is built around the principle that the late effect is not the default diagnosis until the recurrence and the unrelated disease are excluded. The fatigue in the survivor sits on a differential that includes the hypothyroidism, the anaemia, the adrenal insufficiency, the depression and the recurrence, and each is excluded by the targeted test. The growth failure sits on a differential that includes the growth hormone deficiency, the hypothyroidism, the constitutional delay and the skeletal late effect. The exercise intolerance sits on a differential that includes the cardiomyopathy, the pulmonary fibrosis and the deconditioning. [3][5]
The critical distinction is between the late effect and the recurrence, because treating a recurrence as a late effect is as dangerous as missing a late effect. The new mass in the survivor may be a second malignancy, a recurrence of the original cancer, or a benign late effect such as the radiation-induced osteochondroma. The new neurological symptom may be a second central nervous system tumour, a leukaemic infiltration, or a late effect such as the radiation necrosis or the white matter disease. The cytopenia may be the therapy-related myelodysplasia, the marrow recurrence, or the benign cytopenia of the nutritional deficiency. The biopsy and the imaging are the tests that resolve the question, and the default is to exclude the malignancy first. [4][9]
The benign conditions that mimic the late effect must be recognised, because the over-investigation of the survivor is itself a harm. The benign thyroid nodule, the benign breast mass and the functional heart murmur are common in the young adult, and they must be distinguished from the radiation-associated malignancy by the standard diagnostic pathway. The benign causes of the fatigue, such as the iron deficiency and the sleep deprivation, are common in the student-age survivor and are excluded by the simple blood test and the history. The fellow who can distinguish the late effect from the benign mimic and from the recurrence demonstrates the reasoning that protects the survivor from both the missed diagnosis and the over-investigation. [1]
The diagnostic pitfalls are the cases in which the late effect is missed because the symptom is attributed to the psychosocial or the lifestyle cause. The fatigue attributed to the study stress, the exercise intolerance attributed to the deconditioning, the amenorrhoea attributed to the weight loss, and the cognitive decline attributed to the anxiety are the classic misattributions, and they are the reason the treatment summary and the exposure history are taken at every visit. The fellow who asks what the survivor received, and who maps the symptom onto the exposure, is the one who catches the late effect that the attribution to the lifestyle would have missed. [10]
Clinical & Bedside Assessment
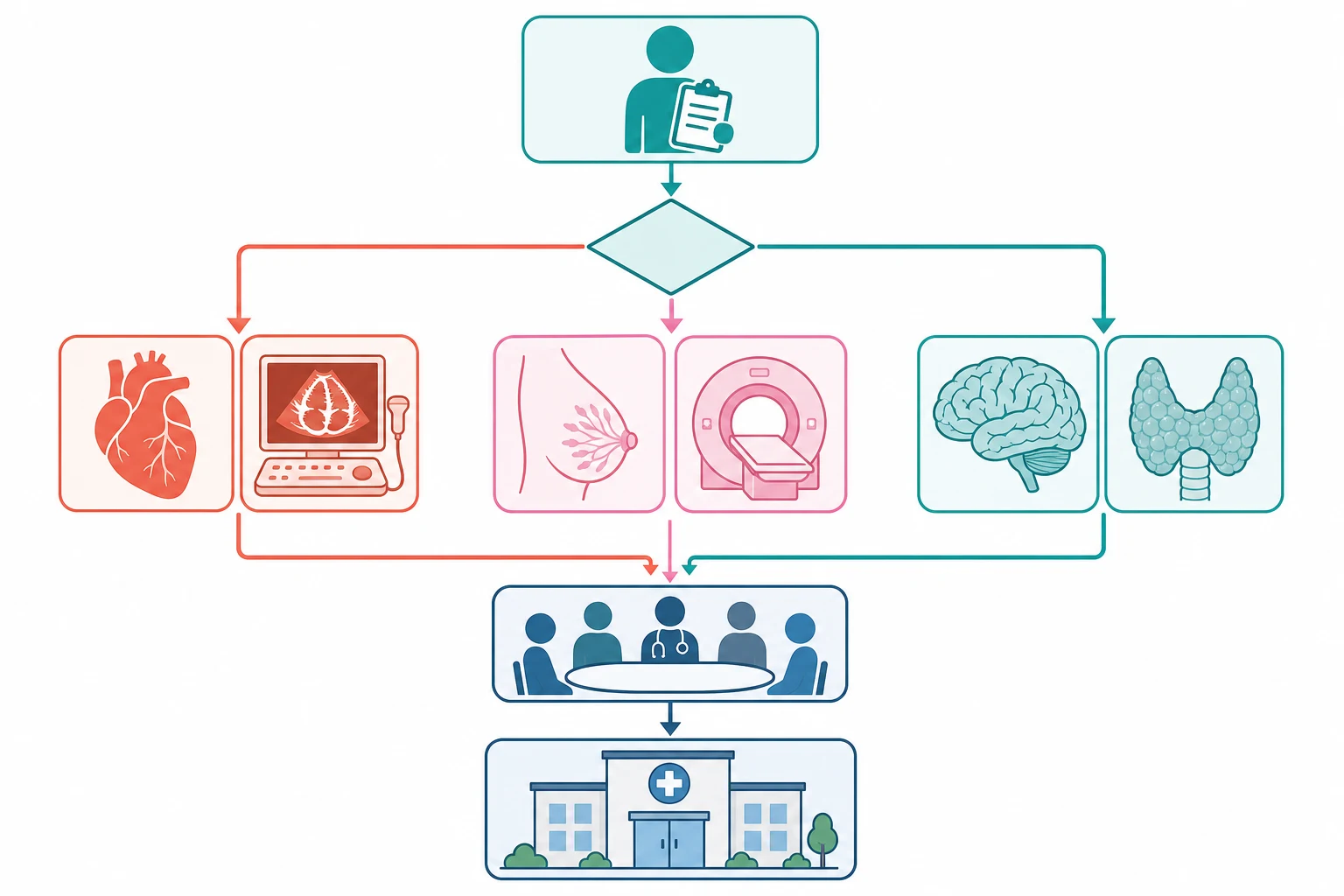
The bedside assessment of the childhood cancer survivor begins not at the examination but at the treatment summary, because the exposure history is what directs every subsequent step. The treatment summary is the document that records the diagnosis, the date, the chemotherapy agents and their cumulative doses, the radiation fields and their doses, the surgery, the stem cell transplant, and the complications. The summary is the single most important tool in the survivorship care, and the fellow who builds it, reviews it and updates it at every visit is the one who delivers the risk-based surveillance. The summary is mapped onto the surveillance guidelines to generate the plan, and the plan is what the survivor carries forward. [2][12]
The history is taken with the treatment summary in hand, and it probes the symptoms that the specific exposures predict. The growth and the pubertal history are taken in every survivor, with the height velocity and the Tanner staging, because the growth failure and the pubertal disorder are the commonest endocrine presentations. The exercise tolerance, the dyspnoea and the palpitations are asked of every survivor exposed to the anthracycline or the chest radiation. The menstrual history and the fertility intentions are taken in every female survivor exposed to the alkylating agents or the pelvic radiation. The cognitive function, the mood and the educational progress are asked of every survivor exposed to the cranial radiation or the intrathecal chemotherapy. [3][8]
The examination is systematic and it targets the systems that the exposures predict, and it takes only a few minutes when it is focused. The height and the weight are measured and plotted, because the crossing of the centiles is the sign of the growth hormone deficiency or the hypothyroidism. The thyroid is palpated for the nodule, because the thyroid cancer follows the neck radiation. The breasts are examined in the female survivor exposed to the chest radiation, because the breast cancer is the commonest subsequent malignancy. The heart is auscultated for the gallop and the murmur, because the cardiomyopathy follows the anthracycline. The skin is examined for the new lesion, because the second malignancy and the radiation-associated tumour may declare in the skin. [3][4]
The focused assessment of the childhood cancer survivor
Review the treatment summary: the diagnosis, the chemotherapy cumulative doses, the radiation fields and doses, the surgery and the transplant
Take the history with the exposures in mind: the growth and pubertal history, the exercise tolerance, the menstrual and fertility history, the cognitive and the mood status
Measure and plot the height and weight, and note the height velocity and the Tanner stage
Examine the thyroid for the nodule, the breasts for the mass, the heart for the gallop, and the skin for the new lesion
Order the risk-stratified surveillance tests: the endocrine panel, the echocardiogram, the mammography and the breast magnetic resonance imaging, the neuropsychological assessment
Build and communicate the surveillance plan, and prepare the transition to the adult late-effects service
The severity of the late effect and the urgency of the response are judged at the bedside, and they decide whether the survivor is managed in the outpatient clinic or moved to the acute setting. The survivor with the stable growth failure and the borderline echocardiogram is managed in the routine clinic, with the endocrine referral and the follow-up imaging. The survivor with the decompensated heart failure, the adrenal crisis or the symptomatic second malignancy is moved to the acute setting, with the admission and the urgent investigation. The teaching of the survivor and the family is part of the assessment, because a survivor who knows the late-effect symptoms and the surveillance plan is the one who returns at the right time. [5][10]
Investigations
The investigation of the childhood cancer survivor is the risk-stratified surveillance, and it is driven entirely by the treatment summary and the surveillance guidelines. The endocrine surveillance includes the annual thyroid function, the growth hormone stimulation test when the deficiency is suspected, and the hypothalamic-pituitary panel of the insulin-like growth factor one, the luteinising hormone, the follicle-stimulating hormone, the oestradiol or the testosterone, and the morning cortisol. The endocrine testing is tailored to the exposure, so that the cranial radiation survivor is tested for the growth hormone and the hypothalamic-pituitary deficiency, and the neck radiation survivor is tested for the primary hypothyroidism. [3][7]
The cardiac surveillance is built on the longitudinal echocardiography, and it is the test that catches the subclinical cardiomyopathy before it declares clinically. The echocardiogram measures the left ventricular ejection fraction and the shortening fraction, and it is repeated at the interval that the anthracycline dose and the chest radiation dose dictate, from the annual to the less frequent. The electrocardiogram looks for the arrhythmia and the conduction abnormality, and the troponin and the natriuretic peptide are the emerging biomarkers that complement the imaging. The cardiac magnetic resonance imaging is the more sensitive test for the early cardiomyocyte injury, and it is used in the high-risk survivor and the discordant echocardiogram. [5]
The subsequent malignancy surveillance is the highest-stakes of the investigations, and it is built on the radiation field and the chemotherapy exposure. The female survivor who received the chest radiation of twenty gray or more receives the annual mammography and the breast magnetic resonance imaging, beginning at eight years after the radiation or at age twenty five, whichever occurs later, because the breast cancer risk approaches that of the BRCA carrier. The survivor who received the neck radiation receives the annual thyroid examination and the thyroid ultrasound for the thyroid cancer. The survivor who received the cranial radiation receives the periodic magnetic resonance imaging for the second central nervous system tumour. The survivor exposed to the high-dose chemotherapy or the radiation receives the annual full blood count for the therapy-related myelodysplasia. [4][9]
The neuropsychological assessment is the investigation that quantifies the neurocognitive late effect, and it is the test that the cranial radiation and the leukaemia survivor needs at the key educational transitions. The formal assessment measures the intelligence quotient, the attention, the processing speed, the executive function and the memory, and it identifies the deficits that the classroom observation alone misses. The assessment drives the educational support plan, the examination accommodations and the vocational guidance, and it is the investigation that protects the survivor's ability to learn and to work. The bone density scan, the audiology and the pulmonary function test complete the surveillance for the osteoporosis, the ototoxicity and the pulmonary fibrosis respectively. [8][10]
Management — Resuscitation
The acute presentation of the late effect is the one that demands the resuscitation, and it is the scenario that the fellow must recognise because the late effect is not the default diagnosis in the survivor who presents acutely. The decompensated anthracycline cardiomyopathy is the archetype, and it presents with the dyspnoea, the hypoxia, the gallop and the pulmonary oedema of the acute heart failure. The resuscitation follows the standard paediatric heart failure pathway, with the oxygen, the diuretics, the afterload reduction and the inotrope, and the urgent echocardiogram confirms the cardiomyopathy. The cardio-oncology and the heart failure teams are involved early, because the anthracycline cardiomyopathy carries a poorer prognosis than the idiopathic. [5][6]
The adrenal crisis is the second acute presentation, and it is the one that is the most preventable and the most easily missed. The survivor with the hypothalamic-pituitary damage from the cranial radiation may present with the adrenal crisis at the time of the intercurrent illness, the surgery or the stress, and the presentation is the shock, the hypotension, the hyponatraemia and the hypoglycaemia. The resuscitation is the intravenous hydrocortisone at the stress dose, the intravenous fluid and the glucose, and the recognition that the adrenal insufficiency is the cause. The survivor with the known adrenal insufficiency carries the emergency hydrocortisone and the management plan, and the family is taught the intramuscular injection for the crisis. [3][7]
The symptomatic second malignancy is the third acute presentation, and it is the one that carries the highest stakes because the new malignancy is the leading cause of the premature death. The survivor who presents with the acute severe headache, the new seizure or the focal deficit may have the second central nervous system tumour, and the magnetic resonance imaging and the dexamethasone follow the standard brain tumour pathway. The survivor who presents with the acute back pain and the progressive weakness may have the spinal cord compression from a second malignancy, and the emergency imaging and the steroids follow. The survivor who presents with the symptomatic anaemia or the bleeding may have the therapy-related myelodysplasia, and the blood film and the marrow biopsy follow. [4][9]
Management — Definitive & Stepwise
The definitive management of the childhood cancer survivor is the risk-based lifelong surveillance, and it is built on three legs: the treatment summary, the surveillance guidelines, and the multidisciplinary team. The treatment summary documents every exposure, the guidelines map the exposure to the surveillance test, and the multidisciplinary team delivers the surveillance and the intervention. The Children's Oncology Group Long-Term Follow-Up Guidelines and the Dutch Late Effects guidelines are the two frameworks that the fellow must know, and they provide the exposure-specific and the dose-specific recommendations for every late effect. The surveillance is lifelong, and it is the reason the survivor is never discharged from the follow-up. [2][12]
[2] [12]The endocrine management rests on the replacement of the deficient hormone, and it is the intervention that restores the growth, the metabolism and the reproductive function. The growth hormone deficiency is treated with the recombinant growth hormone, with the careful assessment of the risk, because the growth hormone may stimulate the growth of a residual or a recurrent tumour, and the decision is made with the oncology team. The hypothyroidism is treated with the levothyroxine. The adrenal insufficiency is treated with the hydrocortisone and the sick-day plan. The gonadal failure is treated with the sex-steroid replacement for the pubertal induction and the bone health, and the fertility is addressed with the reproductive medicine referral and the consideration of the fertility preservation before any gonadotoxic therapy. [3][7]
The cardiac management rests on the early detection and the cardioprotection, and it begins with the subclinical dysfunction that the surveillance echocardiogram catches. The survivor with the falling ejection fraction or the diastolic dysfunction is referred to the cardio-oncology service, and the angiotensin-converting-enzyme inhibitor or the angiotensin-receptor blocker is started to reduce the afterload and to slow the progression. The symptomatic heart failure is managed with the standard heart failure therapy, and the survivor with the end-stage cardiomyopathy may require the heart transplantation, which carries an excellent outcome in the selected survivor. The avoidance of the additional cardiotoxic exposure, the blood-pressure control and the lifestyle form the preventive layer. [5]
Risk-stratified surveillance for the anthracycline cardiomyopathy
Dose
The echocardiographic surveillance is built on the cumulative doxorubicin-equivalent dose: the standard risk at a cumulative dose below two hundred and fifty milligrams per square metre receives the less frequent surveillance, and the high risk at two hundred and fifty milligrams per square metre or more, or with the chest radiation, receives the more frequent lifelong echocardiography
The transition to the adult late-effects service is the management step that protects the survivor from the loss to the follow-up, and it is the one that is most often failed. The transition is prepared in the adolescence, with the survivor taught the diagnosis, the exposures, the surveillance plan and the late-effect symptoms, and the written treatment summary and the care plan are handed to the named adult provider. The transition is a clinical act, and the fellow who builds the transition plan demonstrates the care that extends the surveillance beyond the paediatric service and into the adult life. The survivor who transitions well carries the surveillance forward, and the survivor who is lost to the follow-up is the one whose late effect is detected late. [11]
Specific Subtypes & Scenarios
Anthracycline cardiomyopathy
The anthracycline cardiomyopathy is the cardiac late effect that every fellow must know in detail, because it is the one that is most predictable, most surveilled and most deadly when missed. The risk is dose-dependent, with the cumulative doxorubicin-equivalent dose of two hundred and fifty milligrams per square metre marking the conventional high-risk threshold, and the chest radiation and the younger age at the treatment adding to the risk. The cardiomyocyte is a terminally differentiated cell, so the anthracycline injury is irreversible, and the dysfunction progresses silently before it declares as the heart failure years or decades later. [5][6]
The surveillance is the lifelong echocardiography, and the management begins at the subclinical dysfunction. The survivor with the falling ejection fraction is referred to the cardio-oncology service, and the angiotensin-converting-enzyme inhibitor or the angiotensin-receptor blocker is started to slow the progression. The symptomatic heart failure is managed with the standard therapy, and the end-stage cardiomyopathy may require the heart transplantation. The prevention is the dose-reduction in the contemporary protocols, the avoidance of the additional cardiotoxicity, and the dexrazoxane cardioprotection in the high-dose anthracycline protocol. The fellow who holds the dose, the surveillance and the cardioprotection together has the framework that carries the cardiac late effect. [5]
The cranial radiation and the neurocognitive and endocrine late effects
The cranial radiation produces a cluster of late effects that strike the brain and the hypothalamic-pituitary axis, and the fellow must hold the cluster together because they appear in the same survivor. The neurocognitive late effect follows the injury to the developing white matter, and it declares as the attention deficit, the processing-speed slowing, the executive dysfunction and the academic decline, with the youngest child at the treatment and the highest dose carrying the worst burden. The growth hormone deficiency is the commonest endocrine late effect, and it appears at the lower cranial radiation doses, while the gonadotropin, the adrenocorticotropin and the thyroid-stimulating-hormone deficiency appear at the higher doses. [3][8]
SURVIVOR
The management of the neurocognitive late effect is the educational support and the cognitive rehabilitation, and the formal neuropsychological assessment drives the plan. The growth hormone deficiency is treated with the recombinant growth hormone, with the oncology clearance, and the hypothyroidism and the adrenal insufficiency are treated with the levothyroxine and the hydrocortisone. The second central nervous system tumour is the feared late effect of the cranial radiation, and the survivor with the new headache, the seizure or the focal deficit is imaged without delay. The fellow who holds the neurocognitive, the endocrine and the oncologic late effects of the cranial radiation together demonstrates the reasoning the boards reward. [7][9]
The chest radiation and the breast cancer
The breast cancer after the chest radiation is the commonest subsequent malignancy in the female survivor, and it is the one that the surveillance is built to intercept at the earliest stage. The breast tissue of the pubertal girl is exquisitely sensitive to the radiation, so that the chest radiation of twenty gray or more during the childhood or the adolescence carries a breast cancer risk that approaches that of the BRCA carrier by the age of fifty. The surveillance is the annual mammography and the breast magnetic resonance imaging, beginning at eight years after the radiation or at age twenty five, whichever occurs later, and the early detection is the intervention that changes the outcome. [4][9]
The gonadotoxicity and the infertility
The gonadotoxicity and the infertility are the late effects that the survivor reports as the most distressing, and they follow the alkylating agent and the radiation exposure. The alkylating agent dose, expressed as the cyclophosphamide-equivalent dose, predicts the gonadotoxicity, with the male survivor more vulnerable to the germ-cell injury than the female survivor at the equivalent dose. The premature ovarian failure in the female survivor and the azoospermia in the male survivor are the presentations, and the fertility preservation before the gonadotoxic therapy is the intervention that must be offered. The oocyte or the embryo cryopreservation in the female and the sperm cryopreservation in the male are the established methods, and the discussion is held before the gonadotoxic therapy begins. [3][10]
Complications & Pitfalls
The complications of the late effects are the chronic conditions themselves, and the fellow must hold the breadth of the burden because the late effects rarely appear in isolation. The survivor may carry the growth hormone deficiency, the cardiomyopathy, the breast cancer risk and the infertility together, and the surveillance plan must address each. The complications that drive the premature death are the second malignancy, the cardiac disease and the recurrence, and they are the reason the surveillance is the lifelong and the multidisciplinary. The psychosocial complications, the depression, the anxiety and the post-traumatic stress, are the ones that the survivor reports as the most disabling, and they are addressed with the psychological support and the peer network. [1][8]
The chief pitfall for the fellow is the loss of the survivor to the follow-up, because most survivors do not receive the risk-based surveillance, and the preventable late effects are the ones that the surveillance was designed to catch. The survivor who is lost to the follow-up at the transition to the adult care is the one whose cardiomyopathy progresses undetected, whose breast cancer declares at the advanced stage, and whose adrenal crisis is the preventable death. The adherence to the surveillance is the single greatest determinant of the late-effect outcome, and the fellow who builds the transition plan and the patient-held summary is the one who keeps the survivor in the care. [10][11]
The over-investigation is the opposite pitfall, and it is the harm that the anxious survivor and the uninformed clinician can inflict. The survivor who is over-investigated for the benign symptom carries the radiation from the unnecessary imaging, the anxiety from the false-positive result, and the cost of the unnecessary test. The risk-based surveillance, driven by the treatment summary and the guidelines, is the framework that delivers the right test at the right interval, and it is the discipline that protects the survivor from both the missed late effect and the over-investigation. [2]
Prognosis & Disposition
The prognosis of the childhood cancer survivor is the story of the survival and the burden, and it is determined by the original cancer, the treatment exposure, and the adherence to the surveillance. The over eighty percent five-year survival is the headline, and the growing population of the long-term survivors is the consequence. The premature mortality, however, remains higher than the general population, and the leading causes are the second malignancy, the cardiac disease and the recurrence, in that order. The survivor who receives the risk-based surveillance carries a better prognosis than the survivor who is lost to the follow-up, because the surveillance intercepts the late effect at the treatable stage. [1][5]
The disposition of the survivor is the lifelong late-effects clinic, and it is the setting where the multidisciplinary care is delivered. The clinic brings the endocrinology, the cardiology, the neuropsychology, the reproductive medicine, the primary care and the social work together, and it is the home of the surveillance. The survivor who is managed in the late-effects clinic carries the treatment summary, the surveillance plan and the transition plan, and the clinic is the bridge from the paediatric to the adult service. The regional and the rural survivor is supported by the telehealth and the shared care with the local provider, and the long distances are the reason the patient-held summary is so important. [2][11]
In Australia and Aotearoa New Zealand, the childhood cancer survivor is managed in the tertiary paediatric late-effects clinic, with the transition to the adult late-effects service prepared in the adolescence. The surveillance is built on the treatment summary and the Children's Oncology Group guidelines, and the multidisciplinary team spans the endocrinology, the cardiology, the neuropsychology and the reproductive medicine. The long distances and the rural and the remote populations are the reason the shared care with the local provider and the telehealth are so heavily emphasised, and the Indigenous and the migrant survivors are supported by the cultural and the language services. The fellow who builds the transition plan and the patient-held summary is the one who keeps the survivor in the care across the distances.
[2][11]The prognosis of the specific late effect is the one the survivor asks about, and the fellow must hold the range. The anthracycline cardiomyopathy carries a poorer prognosis than the idiopathic, and the early detection and the cardioprotection improve it. The breast cancer after the chest radiation carries a prognosis that is driven by the stage at the detection, and the surveillance mammography and the magnetic resonance imaging improve it. The growth hormone deficiency is fully corrected by the replacement. The infertility is addressed by the fertility preservation and the reproductive medicine. The fellow who can give the honest and the evidence-based prognosis for each late effect is the one the survivor trusts. [4][5]
Special Populations
The very young child treated for the cancer holds a special position, because the developing brain, the growing skeleton and the maturing endocrine axis are the most vulnerable to the late effects. The cranial radiation is avoided wherever possible in the youngest child because of the devastating neurocognitive injury, and the chemotherapy-first strategy is used to defer or to replace it. The growth hormone deficiency and the growth failure are the commonest late effects in the very young, because the growing skeleton is the most affected by the growth hormone and the thyroid deficiency. The very young survivor needs the closest surveillance of the growth, the puberty and the neurocognition, and the fellow who follows the very young survivor across the childhood holds the late-effect burden that is unique to the age. [3][8]
The adolescent and the young adult survivor is the population at the transition, and it is the one that is most at risk of the loss to the follow-up. The transition to the adult late-effects service is prepared in the adolescence, with the survivor taught the diagnosis, the exposures, the surveillance plan and the late-effect symptoms, and the reproductive and the genetic counselling, the fertility preservation and the vocational support are addressed before the handover. The young person leaves the paediatric service with the treatment summary, the surveillance plan and the named adult provider, and the transition is the clinical act that keeps the survivor in the care. The fellow who builds the transition plan demonstrates the care that extends the surveillance beyond the paediatric clinic. [11]
Socioeconomic disadvantage, remoteness and the migrant or refugee status shape the access to the surveillance and the transition, and they are the reason the loss to the follow-up is so unevenly distributed. The survivor far from the late-effects clinic, the survivor without the transport or the insurance, and the survivor with the language or the cultural barrier is the one whose late effect is detected late. The shared care with the local provider, the telehealth, the patient-held summary and the cultural support are the interventions that bridge the gap, and the fellow who uses them is the one who reaches the survivor across the distance and the disadvantage. [10]
The survivor with the inherited cancer predisposition syndrome is the special population that carries the highest risk of the second and the third malignancy, and the surveillance is intensified accordingly. The Li-Fraumeni syndrome survivor carries the risk of the sarcoma, the breast cancer and the brain tumour, and the whole-body magnetic resonance imaging surveillance is built into the care. The genetic counselling and the testing are offered to the survivor and the family, and the surveillance plan is built around the predisposition as well as the treatment exposure. These survivors are sought in every late-effects clinic because they change the surveillance and the counselling. [4][9]
Evidence, Guidelines & Regional Differences
The landmark evidence that underpins the modern survivorship care is the product of the Childhood Cancer Survivor Study, the St Jude Lifetime Cohort and the national registries, and it is the reason the late-effect burden is so precisely quantified. The Childhood Cancer Survivor Study, begun in 1994, is the cohort of over thirty-five thousand survivors diagnosed between 1970 and 1999, and it has produced the seminal estimates of the chronic health conditions, the subsequent malignancies, the cardiac disease and the premature mortality. The St Jude Lifetime Cohort adds the systematic clinical assessment of the adult survivor, and it has refined the prevalence and the trajectory of the late effects. [1][9]
The contemporary evidence addresses the risk reduction, the surveillance optimisation and the cardioprotection. The studies of the lower anthracycline dose, the proton therapy and the dexrazoxane cardioprotection have shown the late-effect reduction, and the contemporary protocols are built around them. The studies of the surveillance adherence have shown that most survivors do not receive the risk-based follow-up, and the interventions to improve the adherence and the transition are the active research. The studies of the biomarkers, the troponin and the natriuretic peptide, and the cardiac magnetic resonance imaging are refining the early detection of the cardiomyopathy, and the targeted therapies are changing the late-effect profile of the new treatments. [5][10]
The Children's Oncology Group Long-Term Follow-Up Guidelines, used across the United States, Canada and parts of Australasia, and the Dutch Late Effects guidelines, used across the Netherlands and parts of Europe, are the two principal frameworks for the risk-based surveillance of the childhood cancer survivor. Both are exposure-specific and dose-specific, and they agree on the high-yield surveillance: the echocardiography after the anthracycline, the mammography and the breast magnetic resonance imaging after the chest radiation, and the endocrine panel after the cranial radiation. The detail of the interval and the threshold varies, and the International Late Effects Guidelines harmonises the recommendations across the regions. The fellow should know the local guideline and the shared principles.
[2][7]The controversies and the open questions are the live ones. The optimal interval of the echocardiographic surveillance in the lower-risk survivor, balanced against the cost and the false-positive rate, is one. The role of the biomarkers and the cardiac magnetic resonance imaging in the early detection of the cardiomyopathy is another. The intensity of the breast surveillance and the age at which it begins, balanced against the radiation from the mammography in the young breast, is a third. The place of the growth hormone replacement in the survivor of the brain tumour, balanced against the theoretical tumour-growth risk, is a fourth. The fellow holds these as the open questions and cites the guidelines and the trials rather than the dogma. [5][7]
Exam Pearls
The high-yield facts for the exam are the ones that change a decision at the bedside, and they are worth carrying as sharp statements. Over eighty percent of children diagnosed with cancer now survive five years, and the majority carry at least one chronic health condition by adulthood, with over forty percent carrying a severe, life-threatening or disabling condition. The treatment summary is the foundation of the surveillance, and every exposure is mapped to the late effect and the surveillance test. The anthracycline cardiomyopathy is dose-dependent, with two hundred and fifty milligrams per square metre as the conventional high-risk threshold, and the lifelong echocardiographic surveillance is mandatory. [1][5]
The breast cancer after the chest radiation is the commonest subsequent malignancy in the female survivor, and the surveillance is the annual mammography and the breast magnetic resonance imaging from eight years after the radiation or at age twenty five, whichever occurs later. The growth hormone deficiency is the commonest endocrine late effect, and it follows the cranial radiation of eighteen gray or more. The infertility is the late effect the survivor reports as the most distressing, and the fertility preservation is offered before the gonadotoxic therapy. The second malignancy is the leading cause of the premature death, followed by the cardiac disease and the recurrence. [3][4]
The final pearls are the ones that catch the candidate who has learned the headline and forgotten the corner. The adrenal crisis from the hypothalamic-pituitary failure is the preventable death, and the stress-dose hydrocortisone is given at the presentation of the shock in the survivor with the cranial radiation exposure. The therapy-related myelodysplasia and leukaemia carry a poor prognosis, and the survivor with the cytopenia is investigated without delay. The loss to the follow-up is the greatest threat to the late-effect outcome, and the transition plan and the patient-held summary are the interventions that keep the survivor in the care. The message for the exam is that the corners are where the marks are won, and the reasoning that holds the treatment exposure and the risk-based surveillance at the centre is the one the boards reward. [2][11]
References
- [1]Oeffinger KC, Mertens AC, Sklar CA Chronic health conditions in adult survivors of childhood cancer N Engl J Med, 2006.PMID 17035650
- [2]DeVine A, Landier W, Hudson MM The Children's Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers: A Review JAMA Oncol, 2025.PMID 39976936
- [3]Chemaitilly W, Cohen LE, Mostoufi-Moab S Endocrine Late Effects in Childhood Cancer Survivors J Clin Oncol, 2018.PMID 29874130
- [4]Friedman DL, Whitton J, Leisenring W Subsequent neoplasms in 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study J Natl Cancer Inst, 2010.PMID 20634481
- [5]Leerink JM, de Baat EC, Feijen EAM Cardiac Disease in Childhood Cancer Survivors: Risk Prediction, Prevention, and Surveillance: JACC CardioOncology State-of-the-Art Review JACC CardioOncol, 2020.PMID 34396245
- [6]Bates JE, Howell RM, Liu Q Therapy-Related Cardiac Risk in Childhood Cancer Survivors: An Analysis of the Childhood Cancer Survivor Study J Clin Oncol, 2019.PMID 30860946
- [7]van Iersel L, Mulder RL, Denzer C Hypothalamic-Pituitary and Other Endocrine Surveillance Among Childhood Cancer Survivors Endocr Rev, 2022.PMID 34962573
- [8]Stefanski KJ, Anixt JS, Goodman P Long-Term Neurocognitive and Psychosocial Outcomes After Acute Myeloid Leukaemia: A Childhood Cancer Survivor Study Report J Natl Cancer Inst, 2021.PMID 32797189
- [9]Armstrong GT, Liu W, Leisenring W Occurrence of multiple subsequent neoplasms in long-term survivors of childhood cancer: a report from the childhood cancer survivor study J Clin Oncol, 2011.PMID 21709189
- [10]Yan AP, Chen Y, Henderson TO Adherence to Surveillance for Second Malignant Neoplasms and Cardiac Dysfunction in Childhood Cancer Survivors: A Childhood Cancer Survivor Study J Clin Oncol, 2020.PMID 32142393
- [11]Fardell JE, Wakefield CE, Signorelli C Transition of childhood cancer survivors to adult care: The survivor perspective Pediatr Blood Cancer, 2017.PMID 28436208
- [12]Landier W, Bhatia S, Eshelman DA Development of risk-based guidelines for pediatric cancer survivors: the Children's Oncology Group Long-Term Follow-Up Guidelines from the Children's Oncology Group Late Effects Committee and Nursing Discipline J Clin Oncol, 2004.PMID 15576413