Paeds · investigations-procedures-and-technology
Chest radiograph interpretation in children
Also known as Chest X-ray · CXR · Paediatric chest film · Chest radiograph · Plain chest imaging · AP chest film
Fellowship guide to interpreting the paediatric chest radiograph. Covers why the child's chest film differs from the adult's — the thymus that reshapes the mediastinum, the cartilaginous skeleton, the projection and inspiration that change everything — the structured technical-quality check that must precede any reading, the ABCDEFGH systematic approach applied zone by zone, the normal cardiothoracic ratio and how rotation and poor inspiration falsely enlarge the heart, the neonatal chest film with its lines and tubes, the radiographic signs of pneumonia, foreign-body aspiration, heart failure and the common pitfalls, and the radiation-aware ALARA principle that governs when a film is justified at all.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
Overview & Definition
Picture the febrile two-year-old with a grunting respiration, the neonate on continuous positive airway pressure whose oxygen need has crept up, or the five-year-old with a wheeze that does not resolve. In each, the chest radiograph is the first and often the only imaging investigation the team will order, and the question that matters is not "what does the film show" but "what does the film show in this child, taken this way". That is the territory this page owns. [1] [2]
A chest radiograph (CXR, chest X-ray) is a two-dimensional projection radiograph of the thorax in which a beam of X-rays passes through the chest and is differentially absorbed by the tissues, producing a shadow image on a digital detector. Dense tissues such as bone absorb most photons and appear white, while air-filled lung absorbs few and appears black, and soft tissues occupy the grey spectrum in between. The standard view in a cooperative older child is the pa posterolateral (PA) film taken erect in full inspiration with the X-ray beam travelling from posterior to anterior; the anteroposterior (AP) film is taken the other way and is the default in the sick, supine or young child who cannot stand or cooperate; a lateral film is added when localisation or a question about the mediastinum or spine is needed. [4] [6]
What makes the paediatric chest film a distinct skill from adult radiography is a set of developmental differences and a set of technical realities. The thymus is large in the infant and young child and reshapes the mediastinal contour, producing the sail sign that is normal and not a mass. The skeleton is largely cartilaginous, so the costophrenic angles and rib detail behave differently and a posterior rib fracture is easily missed. The heart sits more horizontally and the normal cardiothoracic ratio in an infant is up to 0.60, falling toward the adult value of 0.55 by around five years. Most films in the unwell child are AP, supine, and in less than full inspiration, and all three of those artefacts enlarge the apparent heart and crowd the lung fields. The fellowship skill being tested is reading the technical quality first, then applying a systematic method, then folding in the clinical picture. [1] [3]
Classification
Sort the chest radiograph by how it was taken, by what clinical question it answers, and by the child it was taken in, because each axis changes what counts as adequate and what the finding means. [1] [6]
By projection, the PA film (beam posterior to anterior, erect, cooperative patient) is the reference standard in the older child because the heart is least magnified and the ribs are best shown; the AP film (beam anterior to posterior, often supine, the sick or young child) magnifies the heart and widens the mediastinum, so a borderline heart size on an AP film is not cardiomegaly; the lateral film localises masses, fluid and foreign bodies. By position, an erect film best shows the lung apices, the costophrenic angles and a small pleural effusion that layers dependently, while a supine film pools free fluid along the posterior chest wall and can hide a moderate effusion behind the diaphragm. [3] [4]
By the clinical question, the film may be a diagnostic film for respiratory symptoms, a cardiac film for suspected congenital heart disease (looking at heart size, shape and pulmonary vascularity), a neonatal film for respiratory distress (with the added complexity of tubes and lines), a trauma film (often the first of an ATLS sequence), or a line-and-tube check in the intensive care setting. The reading discipline adapts to the question: a film requested to confirm ET tube position is read with the tube position first, a film for suspected pneumonia is read with the lung fields first. [4] [7]
By the child, the neonatal film demands knowledge of neonatal lung disease and line positions; the infant and toddler film is dominated by the thymus and by the difficulty of obtaining a good inspiration; the school-age and adolescent film approaches the adult film and a near-normal cardiothoracic ratio applies. Each age has its own normal, and reading a child's film with adult normal values is a common source of error. [1] [5]
The numbers that anchor your viva
Epidemiology & Risk Factors
The chest radiograph is the most frequently requested imaging investigation in paediatrics, and it is performed in nearly every acute setting from the emergency department to the neonatal and paediatric intensive care units. Its frequency is precisely why interpretation errors accumulate: the volume is high, the films are often technically imperfect, and the readers range from experienced paediatric radiologists to trainees interpreting at the bedside in the middle of the night. [1] [3]
The risk of a misinterpretation is concentrated in three situations that recur. The first is the technically inadequate film — the rotated, under-inspired, AP, bedside film of the sick child — in which rotation widens the mediastinum and magnifies the heart, and poor inspiration crowds the ribs and elevates the diaphragm, together producing apparent cardiomegaly or consolidation that is artefact. Patient rotation alone has been shown to change the apparent size and contour of the heart and great vessels enough to alter a report. The second is the age-specific normal misread as abnormal — the thymus in the infant, the horizontal heart and generous cardiothoracic ratio, the prominent pulmonary artery segment — each of which is normal in the young child and overcalled by a reader calibrated to the adult chest. The third is the satisfaction-of-search error, the cognitive bias of stopping the search once the first abnormality is found, which is the mechanism by which a second rib fracture, a second lung lesion, or a malpositioned tube is missed. [3] [7]
A specific and important epidemiological point is that the prevalence of radiographic pneumonia in a wheezing child is low, and a systematic review and meta-analysis found that the prevalence of radiographic pneumonia in children presenting with wheeze was substantially lower than historical estimates. The implication is that the chest radiograph adds little in the uncomplicated wheezy child without a clear focal finding, and that routine films in bronchiolitis and wheeze expose children to radiation without changing management — a point the fellowship candidate is expected to make. [10]
Pathophysiology
The teaching model runs from why a chest radiograph looks the way it does, through how the developing child distorts the normal, to the mechanisms by which technical factors mislead — and it rests on physics, on developmental anatomy, and on the geometry of projection radiography. [1] [3]
The single most testable physical principle is that a chest radiograph is a projection, not a slice. Every structure lying along the path of the X-ray beam is summed onto the final image, so overlapping densities add together and a small lesion in front of or behind a rib, the heart, or the hilum can be invisible. The silhouette sign is the practical consequence: when a pathological density of soft-tissue (water) attenuation lies adjacent to a structure of similar density, it obliterates that structure's normal border; consolidation touching the right heart border destroys the right heart border and locates the disease to the right middle lobe, while consolidation touching the diaphragm destroys that border and locates it to the lower lobe. The air bronchogram is the inverse: aerated bronchi seen as dark branching lines against a white background of consolidated alveoli, the radiographic proof that the opacity is within the lung and not a pleural or chest-wall lesion. [1] [6]
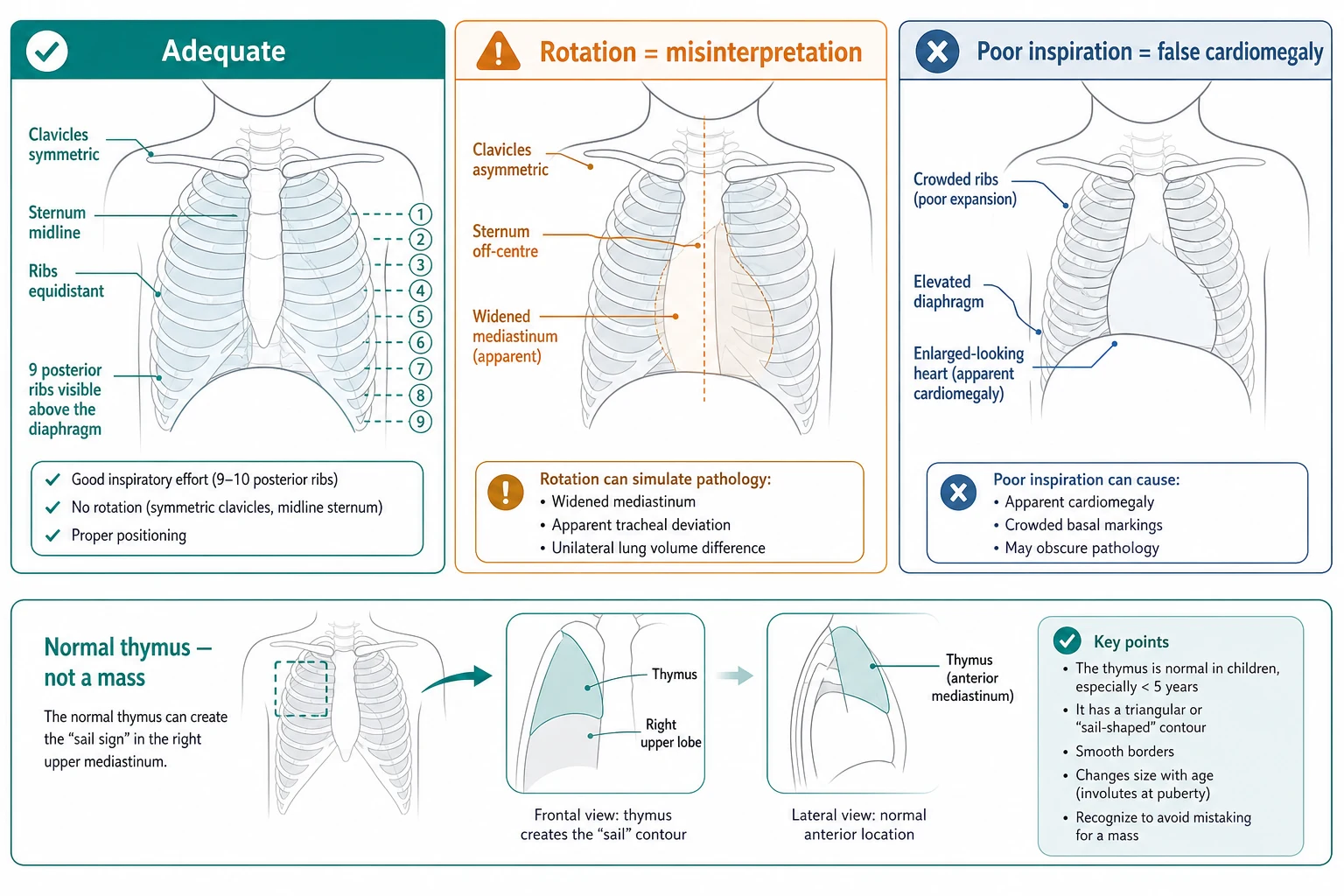
The single most testable developmental principle is that the thymus reshapes the paediatric mediastinum. The thymus is large at birth and remains prominent through infancy and early childhood, sitting in the anterior superior mediastinum and producing the characteristic sail sign — a sharp, angular inferior border in the right upper mediastinum that resembles a ship's sail. Because the thymus is soft and pliable, it changes shape with respiration and position, a feature that distinguishes it from a fixed pathological mass; on a film taken in expiration it appears larger, and on an expiratory or lateral film it drapes over the heart. The thymus involutes with stress (sepsis, steroids) and regrows on recovery, so a vanished thymus in a sick infant is itself a sign of illness, and a reappearing thymus on recovery is not a new mass. Recognising the normal thymus is one of the highest-yield paediatric chest-film skills. [5]
The mechanism by which technical factors mislead is geometric. In patient rotation, the sternum and the spinous processes no longer sit in the same plane relative to the detector, the clavicles become asymmetric, the mediastinum is thrown obliquely and appears widened, and the side to which the child is rotated shows an apparently larger heart and prominent pulmonary vessels — the film is effectively of a child turned partly sideways. In poor inspiration, the diaphragm does not descend, the ribs crowd, the heart is compressed from below and appears larger, and the lung bases look opaque from under-aeration — the basis of the rule that a heart enlarged only on a poor film is not enlarged at all. In over-penetration the fine lung detail and the posterior ribs are burned out and a subtle interstitial pattern is missed; in under-penetration the film is too white, the mediastinal detail and the retrocardiac space are lost, and a small effusion behind the heart is hidden. [3]
Clinical Presentation
The clinical scenarios that prompt a paediatric chest radiograph are few and well defined, and the first task is to decide which question the film is being asked to answer, because the reading priority and the threshold for the film both change with it. [1] [2]
The commonest scenario is the child with respiratory symptoms — fever and cough, tachypnoea, increased work of breathing, hypoxia, or a focal chest finding — in whom the film is requested to confirm or exclude pneumonia, to identify an effusion, or to characterise atelectasis. The second is the neonate with respiratory distress in the first hours of life, in whom the film distinguishes respiratory distress syndrome, transient tachypnoea of the newborn, meconium aspiration, congenital pneumonia, and a pneumothorax, and in whom it also checks the position of the endotracheal tube, the umbilical venous and arterial catheters, and the chest drain. The third is the suspected inhaled foreign body in the toddler with sudden-onset cough, choking, or persistent unilateral signs, in whom an inspiratory film may be normal and the diagnosis rests on air-trapping shown on an expiratory film or a lateral decubitus film. The fourth is the suspected cardiac presentation — the cyanotic or acyanotic infant, the child with heart failure — in whom the film looks at heart size, shape and the pulmonary vascular pattern. The fifth is the trauma setting as part of a structured approach, and the sixth is the intensive-care line and tube check. [4] [12]
The urgency is graded by the clinical state. The child in respiratory failure or with a tension pneumothorax is the one in whom the film is interpreted immediately at the bedside, often as a point-of-care image, and in whom a deteriorating child cannot wait for a formal report. The stable child with a clear clinical picture can have the film requested, performed, and read in a controlled way with a formal radiologist's report. The child with a chronic or recurrent problem can have a planned film with comparison to prior films to track change over time. [1] [7]
The presenting features that should prompt the reader to distrust the film and request a repeat or a different view are obvious rotation (asymmetric clavicles, spinous process off-centre), a clearly poor inspiration (fewer than nine posterior ribs crossing the diaphragm), a film that is over- or under-penetrated, and any film taken in a position or projection that does not match the clinical question. A film that does not answer the question is not a finished investigation. [3] [6]
| Scenario | Priority on the film | What it dictates |
|---|---|---|
| Fever, cough, focal findings | Lung fields first | Confirm or exclude consolidation, effusion, atelectasis; read with the clinical picture and oxygenation |
| Neonatal respiratory distress | Lung pattern and lines | Distinguish RDS, TTN, meconium aspiration, pneumonia; check ET tube, UVC, UAC, chest drain positions |
| Suspected inhaled foreign body | Air-trapping | Inspiratory film alone may miss it; add expiratory film or lateral decubitus to show the hyperlucent, over-inflated side |
| Suspected congenital heart disease | Heart and vascularity | Heart size and shape, pulmonary oligoemia versus plethora, rib notching in older coarctation |
| Intensive-care tube check | Lines and tubes first | ET tube midway between clavicles and carina; central line tip in the correct vessel; rule out pneumothorax post-procedure |
The trap is the film that looks normal in a child who is clearly unwell — the well-appearing radiograph that hides an early pneumonia, a small effusion, a foreign body, or a mediastinal mass behind the thymus. The discipline is to read the film and the child together, and to escalate to a senior or to a different modality (lateral film, decubitus film, ultrasound, or CT) when the two do not fit. [1] [7]
Differential Diagnosis
The differential at the bedside is not "what is the cause of the opacity" — it is what pattern the film shows, what that pattern localises to, and whether it fits the child in front of you. Frame the reading around a small number of named patterns and the localisation follows. [1] [6]
Alveolar consolidation
air-space pattern
- Fluffy, confluent opacity with air bronchograms
- Silhouette sign localises the lobe — obliterates adjacent soft-tissue border
- Acute bacterial pneumonia is the prototype; also atelectasis, haemorrhage, oedema
- Read with the child: fever and focal signs support infection
Atelectasis
- Volume loss — shifted fissure, mediastinum or hilum pulled toward it
- Crowded ribs and elevated hemidiaphragm on the affected side
- May mimic consolidation but the volume loss is the discriminator
- Common after intubation, mucous plugging, or in the postoperative child
Pleural effusion
- Dependent opacity blunting the costophrenic angle; meniscus sign
- Large effusion causes mediastinal shift away from the side
- Supine film under-calls: fluid layers posteriorly
- Ultrasound characterises and guides drainage
Hyperinflation
- Flattened, low diaphragms; increased lung lucency
- Unilateral: foreign-body air-trapping until proven otherwise
- Bilateral: bronchiolitis, asthma, or COPD-equivalent
- Add expiratory or decubitus film if a foreign body is suspected
Cardiomegaly with pulmonary oedema
- Enlarged CTR on a good film; pulmonary venous congestion
- Bat-wing perihilar oedema, Kerley B lines, pleural fluid
- Differentiate from thymic spurious enlargement and AP magnification
- Read with the cardiac and volume history
A second layer of differential is the pattern within the neonatal lung. A fine, symmetric, reticulogranular pattern with low lung volumes and air bronchograms points to surfactant deficiency (respiratory distress syndrome); streaky perihilar densities with fluid in the fissures and good lung volumes points to transient tachypnoea of the newborn; coarse, patchy infiltrates with hyperinflation and possible pneumothorax points to meconium aspiration; and a uniform white-out of one hemithorax with mediastinal shift in the first hours of life raises a congenital diaphragmatic hernia until proven otherwise. [4]
A third layer is the mediastinal contour. A widened mediastinum on a rotated film is artefact; a sail sign in an infant is the normal thymus; a true anterior mediastinal mass in the older child raises lymphoma or a germ-cell tumour; a posterior mediastinal mass raises neurogenic tumour; and a global cardiac enlargement with a specific shape (boot-shaped in tetralogy, egg-on-a-string in transposition) points to congenital heart disease. [5] [11]
The inhaled foreign body deserves a specific question because it is common and often missed. The classic teaching is that an inspiratory film is frequently normal, because the foreign body acts as a ball-valve allowing air in on inspiration but trapping it on expiration; the diagnosis rests on showing air-trapping on the affected side, either on an expiratory film (the hyperlucent, over-inflated lung fails to deflate) or on a lateral decubitus film (the dependent lung should deflate, and failure to do so on the suspected side is abnormal). A child with a persistent unilateral wheeze or hyperlucency has an inhaled foreign body until proven otherwise by bronchoscopy. [12]
Clinical & Bedside Assessment
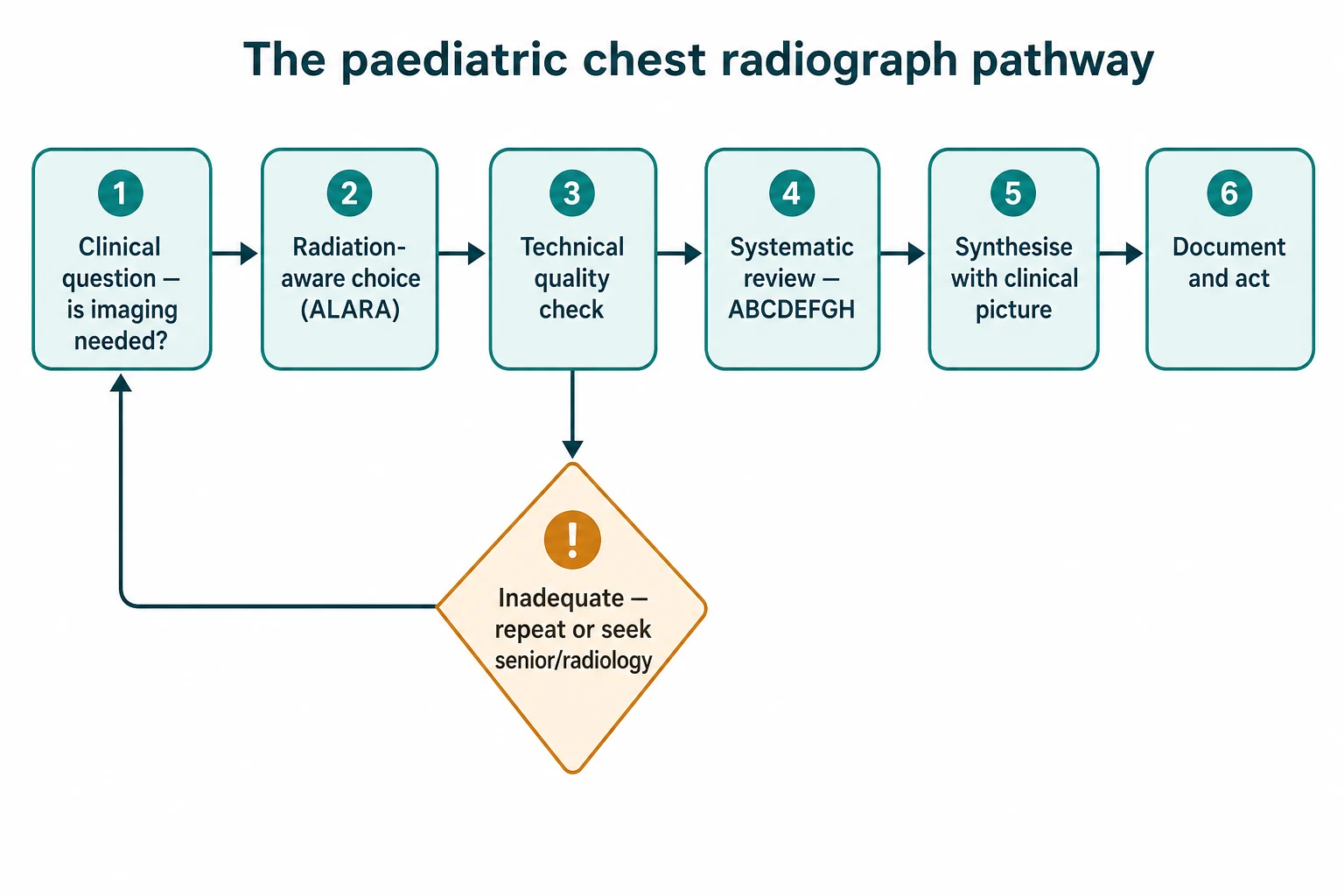
Assessment of the chest radiograph is a two-pass exercise: a structured technical-quality check, then a systematic zone-by-zone review. The aim is never to jump to the obvious finding, because the obvious finding is what stops the search and hides the second abnormality. [1] [3]
Begin with the technical quality, asking five explicit questions. Projection: is the film PA, AP, or lateral, and does the projection match the clinical question? Position: is the child erect or supine, and is the position appropriate for the question being asked? Rotation: are the medial ends of the clavicles symmetric and equidistant from the spinous processes — if not, the child is rotated and the mediastinum and heart are unreliable. Inspiration: do at least nine posterior ribs cross the diaphragm at the midclavicular line on a good film — fewer indicates under-inflation, which enlarges the heart and opacifies the bases. Penetration: is the thoracic spine just visible through the cardiac shadow, and are the lower thoracic vertebrae and the intervertebral discs visible — if the film is too white the mediastinum is lost, if too black the lung detail is burned out. A film that fails the quality check is flagged as limited, and the key findings are interpreted with that limitation stated. [3] [6]
The technical-quality check before you read the fields
Projection: PA, AP, or lateral? Does it match the clinical question?
Position: erect or supine? Erect best shows the apices, angles and small effusions
Rotation: clavicles symmetric and equidistant from the spinous processes? If not, the heart and mediastinum are unreliable
Inspiration: at least nine posterior ribs crossing the diaphragm? Fewer means the heart is falsely enlarged and the bases falsely opaque
Penetration: thoracic spine just visible through the heart? Then the film is readable; flag and re-image if not
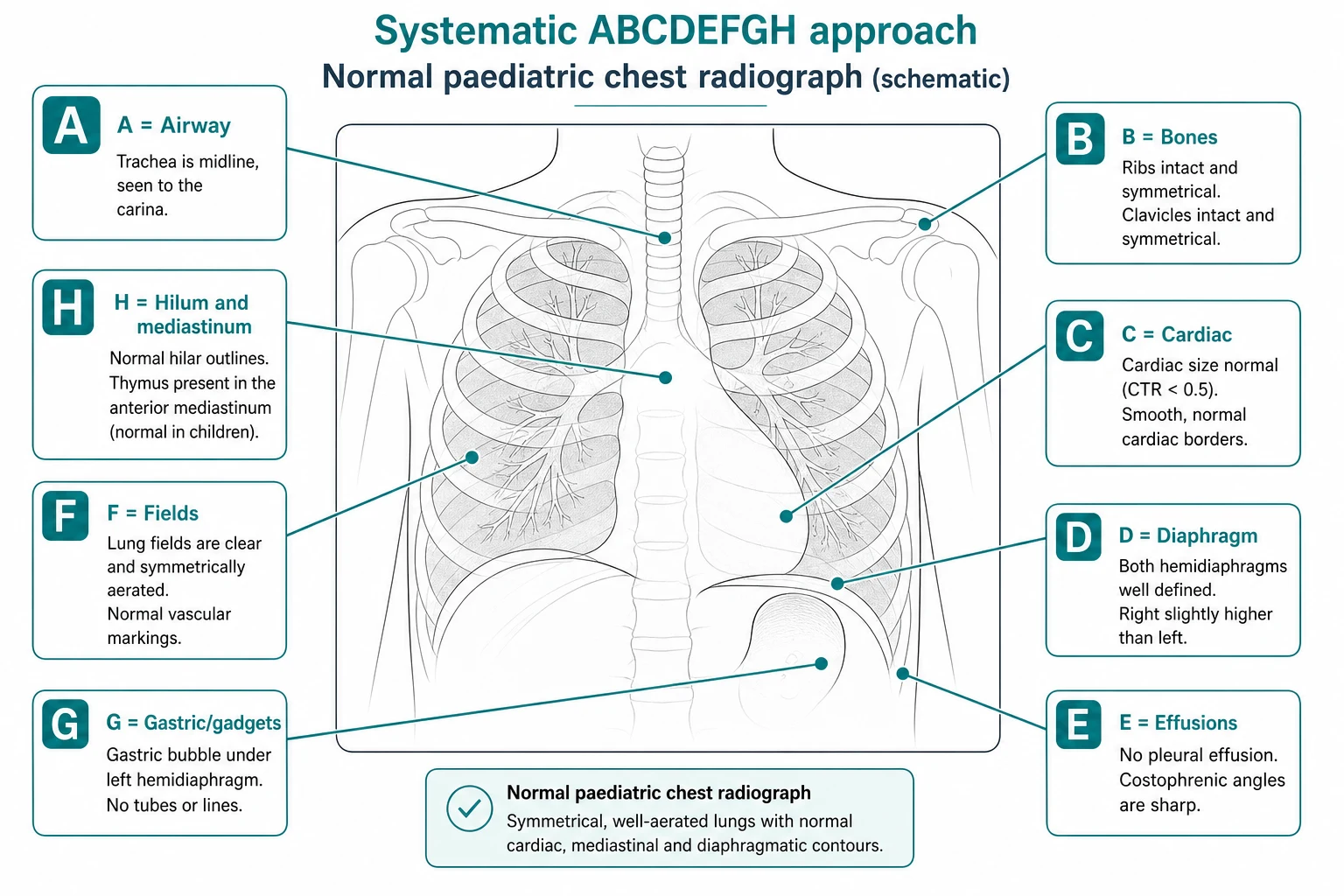
Once the quality is accepted, apply the ABCDEFGH systematic review. A — Airway: the trachea should be midline and the carina visible; deviation suggests a tension process, a mass, or volume loss. B — Bones: trace every rib, the clavicles and the spine for fractures, lytic or sclerotic lesions; in suspected non-accidental injury look for posterior rib fractures near the costovertebral junctions, which are highly specific. C — Cardiac: the heart size, shape and borders; the CTR on a good film, and the silhouette sign localising any adjacent consolidation. D — Diaphragm: both hemidiaphragms should be sharp, the right slightly higher than the left, and the costophrenic angles clear; a blunted angle is an effusion until proven otherwise. E — Effusions: look in the dependent spaces and behind the heart; remember that a supine film hides free fluid. F — Fields: the lung zones for aeration, consolidation, nodules, interstitial change, and air-trapping; compare side with side, zone with zone. G — Gastric and gadgets: identify every tube and line and confirm its position — the endotracheal tube, the central venous line, the nasogastric tube, the umbilical catheters, and the chest drains. H — Hilum and mediastinum: the hila should be symmetric and the left slightly higher, the mediastinal contour should be traced, and the thymus recognised as normal. [1] [4]
ABCDEFGH
Investigations
The chest radiograph is itself an investigation, and the candidate must know when it is the right test, when it is insufficient, and when a different modality is better. The choice rests on the clinical question, on the radiation cost, and on what each modality adds. [1] [9]
The standard views are the PA film (older child, erect, cooperative), the AP film (young or sick child, often supine at the bedside), and the lateral film (added for localisation, masses, and to confirm a foreign body or a small effusion). Special views include the lateral decubitus film (the child lying on the side), used to show a small pleural effusion that layers along the dependent chest wall, and to show air-trapping on the non-dependent side in a suspected foreign body when an expiratory film cannot be obtained; and the expiratory film, the key view for an inhaled foreign body. [4] [12]
| Clinical question | Best next modality | Why |
|---|---|---|
| Suspected foreign body with normal inspiratory film | Expiratory film or lateral decubitus film | Shows air-trapping on the affected side; bronchoscopy is both diagnostic and therapeutic |
| Characterising a pleural effusion or empyema | Chest ultrasound | Shows loculation, guides drainage; no radiation; performed at the bedside |
| Complex congenital heart disease | Echocardiography and cardiac MRI | Anatomy and function in detail; the CXR is a screening tool only |
| Complicated pneumonia, abscess, or necrosis | Contrast CT of the chest | Defines the parenchymal complication when management depends on it |
| Suspected mediastinal mass | Contrast CT or MRI | Localises, characterises, and shows vascular and airway relationship before biopsy or surgery |
| Interstitial lung disease or bronchiectasis | High-resolution CT of the chest | The CXR is insensitive; HRCT defines the pattern and extent |
The interpretation turns on a few named signs. The silhouette sign localises disease to a lobe by the border it erases — disease touching the right heart border is right middle lobe, the diaphragm is lower lobe, the aortic knuckle is upper lobe. The air bronchogram confirms that an opacity is alveolar and within the lung. The meniscus sign at the costophrenic angle indicates a pleural effusion. The deep sulcus sign on a supine film — an abnormally deep, lucent costophrenic angle — indicates a pneumothorax that has collected anteriorly and inferiorly. The spine sign — the failure of the thoracic spine to appear progressively darker inferiorly as the diaphragm is approached — indicates a lower-lobe consolidation behind the heart. [1] [6]
The radiation-aware choice is the final layer of the investigation. A paediatric chest radiograph is a low-dose study with an effective dose of roughly 0.02 mSv, equivalent to a few days of natural background radiation, and the lifetime attributable cancer risk from a single paediatric CXR is extremely low. The principle is nonetheless one of justification and ALARA (as low as reasonably achievable): the film is requested only when it will change management, the dose-reduction features of modern digital radiography are used, and alternative modalities without ionising radiation (ultrasound, MRI) are preferred where they answer the question. Children are more radiosensitive than adults per unit dose because of their longer remaining life expectancy and the higher proportion of dividing cells, which is the biological basis for the ALARA principle in paediatrics. [8] [9]
Management — Resuscitation
When the chest radiograph reveals an immediately life-threatening finding, the reading itself drives the resuscitation, and the ordered response is the same as for any acutely ill child: airway, breathing, circulation, with the specific intervention that the film demands. [4]
The findings that demand immediate action at the moment of reading are few and named. A tension pneumothorax — a lung collapsed toward the hilum, the mediastinum shifted to the opposite side, and the hemidiaphragm flattened and depressed — requires immediate needle decompression and an intercostal drain, and in the deteriorating child the decision is clinical and precedes the film. A malpositioned endotracheal tube — a tip in the right main bronchus over-expanding the right lung and collapsing the left, or a tip above the clavicles failing to ventilate — requires immediate repositioning and re-imaging. A collapsed lung from a mucous plug or a blocked tube in the ventilated child requires suction, repositioning, and escalation. A central venous line or umbilical catheter in a dangerous position — a UAC crossing into a renal or iliac artery, a central line tip in the heart — requires immediate withdrawal and re-siting. [4]
The single most important rule in the intensive-care film is that the lines and tubes are read first, not last, because a misplaced tube is the immediately correctable cause of a child failing to improve, and because the rest of the film is often confounded by the artefact of the support. The endotracheal tube tip should sit midway between the clavicles and the carina, ideally at the level of the interclavicular line, because flexion and extension of the neck move the tip by several centimetres and a tube that looks adequate in flexion may be bronchial in extension. [4] [3]
No drug dose applies — this section is about interpretation that drives the action
If the film is read as normal but the child is deteriorating, abandon reliance on the film and treat the child: a normal chest radiograph does not exclude a life-threatening condition, and the pathway is to escalate the airway and breathing management, to obtain a senior and an intensive-care review, and to repeat the imaging or move to a more sensitive modality. [1] [3]
Management — Definitive & Stepwise
Once the technical quality is accepted and the immediately life-threatening findings are excluded, the interpretation is a structured stepwise sequence that runs the same way every time, concludes with a synthesised impression that folds in the clinical picture, and is documented clearly. [1] [6]
Begin with the clinical context: the child's age, the indication, the projection and position, and any prior films for comparison — a finding that is unchanged from a film years ago is a different clinical problem from one that is new. State the technical quality explicitly in the report: adequate or limited, the reasons if limited, and the implications for the confidence of the findings. Apply the ABCDEFGH review systematically and document the relevant positives and negatives — it is not enough to describe the obvious finding, because the negative findings (no pneumothorax, no effusion, no mediastinal shift) are part of the answer. [1] [3]
RIPIT
The synthesis is the impression, not a re-description of the findings. The impression answers the clinical question: "This is a right lower-lobe pneumonia with a small pleural effusion, in a febrile three-year-old, with no pneumothorax and a normal heart size; the endotracheal tube is correctly positioned." The impression names the limitations of the film — "limited by rotation and poor inspiration" — and the recommended next step — "a lateral decubitus film if a foreign body is suspected" or "comparison with prior films recommended". The discipline is that the report is actionable: a colleague reading it knows what was seen, what was not seen, and what to do next. [1]
Handle the common interpretive problems deliberately. A borderline heart size on an AP film is not cardiomegaly — state the limitation and recommend a PA film if it matters. A possible thymic mass in an infant is almost certainly the normal thymus — describe the sharp inferior border and the change with respiration, and recommend clinical correlation rather than escalation. A persistent opacity after treatment for pneumonia may be atelectasis or residual consolidation — recommend a follow-up film in four to six weeks to confirm resolution and to exclude an underlying lesion. A normal inspiratory film in a coughing child does not exclude a foreign body — recommend an expiratory or decubitus film, and bronchoscopy if clinical suspicion is high. [1] [12]
Specific Subtypes & Scenarios
The approach to the paediatric chest radiograph changes with the child and the clinical question, and the fellowship candidate must adjust the reading priority and the differential to the subtype in front of them. [4] [7]
In the neonate, the chest film is most often for respiratory distress in the first hours of life. The reading priority is the lung pattern and the lines. Respiratory distress syndrome shows a symmetric, fine reticulogranular pattern with low lung volumes and air bronchograms; transient tachypnoea of the newborn shows streaky perihilar densities, fluid in the fissures, and good lung volumes; meconium aspiration shows coarse, patchy infiltrates with hyperinflation and possible pneumothorax; neonatal pneumonia is often patchy and asymmetric. The umbilical venous catheter should run through the umbilical vein, the portal vein, and the ductus venosus to the inferior vena cava at the level of the diaphragm, and the umbilical arterial catheter should sit low (L3 to L5) or high (T6 to T10), avoiding the origin of the renal and mesenteric arteries. [4]
In the child with suspected pneumonia, the film confirms or excludes the diagnosis, localises the consolidation by the silhouette sign, and identifies complications — effusion, empyema, necrosis, or pneumatocele. The systematic review confirmed that the prevalence of radiographic pneumonia in wheezing children is low, so the film is justified when there is a focal finding, hypoxia, or an unclear diagnosis, and is not routine in uncomplicated bronchiolitis or wheeze. [2] [10]
In the child with a suspected inhaled foreign body, the reading priority is air-trapping. An inspiratory film alone is frequently normal, and the diagnostic view is the expiratory film (the affected lung fails to deflate and remains hyperlucent and over-inflated) or the lateral decubitus film (the dependent lung should deflate, and failure to do so on the suspected side is abnormal). A child with a persistent unilateral wheeze, hyperlucency, or a history of a choking episode has a foreign body until bronchoscopy proves otherwise. [12]
In the child with suspected congenital heart disease, the film looks at the heart size, shape, and the pulmonary vascular pattern. Pulmonary plethora (engorged, clearly visible pulmonary vessels extending to the periphery) indicates a left-to-right shunt such as a ventricular septal defect; pulmonary oligoemia (dark, under-perfused lung fields) indicates a right-to-left shunt or right-sided obstruction such as tetralogy of Fallot; pulmonary venous congestion and oedema indicate obstruction or left-heart failure. The cardiac shape offers clues — the boot-shaped heart of tetralogy, the egg-on-a-string of transposition, the snowman of total anomalous pulmonary venous return — but the echocardiogram is the definitive test. [11]
In the intensive-care setting, the film is read with the tubes and lines first. The endotracheal tube tip midway between the clavicles and the carina; the central venous line tip in the superior vena cava just above the right atrium; the nasogastric tube tip in the stomach below the diaphragm; and the chest drain in the pleural space. A pneumothorax after line insertion is looked for specifically, and on a supine film the deep sulcus sign is the clue. [3] [4]
In the suspected non-accidental injury, the chest film is part of a skeletal survey, and the high-specificity finding is a posterior rib fracture near the costovertebral junction, which results from squeezing compression and is not seen in accidental injury. The bones are read with this specific question in mind, alongside the clavicles and the spine. [6]
Complications & Pitfalls
The complications of chest-radiograph interpretation are cognitive errors and overcalls, and the discipline is to anticipate them through the structured method and through honest acknowledgement of the film's limitations. [1] [3]
The common interpretive pitfalls are the ones that recur and are testable. Overcalling cardiomegaly on an AP, supine, under-inspired film is the classic error of ignoring technical quality; the CTR is only meaningful on a good film. Calling the normal thymus a mediastinal mass is the classic error of applying adult norms to the infant chest; the sail sign, the sharp inferior border, and the change with respiration identify the thymus. Missing the inhaled foreign body on a normal inspiratory film is the classic error of accepting an inadequate investigation; an expiratory or decubitus film is needed. Reading the lung fields before the tubes and lines in the intensive-care setting is the classic error of the wrong reading priority; a malpositioned tube is the immediately correctable cause of a failing child. [3] [12]
The satisfaction-of-search error is the cognitive bias of stopping the search once the first abnormality is found, and it is the mechanism by which a second rib fracture, a second lung lesion, a contralateral pneumothorax, or a malpositioned line is missed. The protection is the systematic method applied in full regardless of how obvious the first finding seems. [1]
A frequently tested misconception is that the chest radiograph is a sensitive test. It is not. A CXR can be normal in early pneumonia, in a small foreign body, in early heart failure, in a mediastinal mass hidden behind the thymus, and in many interstitial lung diseases. The corollary is that a normal film never overrides an unwell child, and the pathway is to escalate clinically and to a more sensitive modality rather than to be falsely reassured. [1] [10]
The reverse misconception is that the chest radiograph is harmless and should be requested liberally. Although the dose of a single CXR is very low, the cumulative dose from repeated imaging matters over a childhood, and the principle of justification applies — the film is requested when it will change management, not to reassure, and not as a reflex. The substitution of ultrasound for many paediatric chest questions is a deliberate radiation-reduction strategy. [8] [9]
Prognosis & Disposition
The prognosis after a well-interpreted chest radiograph is driven entirely by the underlying diagnosis, not by the imaging itself. The disposition is driven by what the film, read with the child, tells the team to do. [1] [2]
For a child with a clear radiographic pneumonia and a good clinical response to antibiotics, the disposition is guided by the clinical course, with a follow-up film in four to six weeks only if the radiograph is not normal at the expected time of recovery, to confirm resolution and to exclude an underlying lesion such as a sequestration or a foreign body. [2] [10]
For a child with a normal film and a clear viral illness, the disposition is supportive care and safety-netting advice; the film does not need repeating, and the principle of justification argues against it. [10]
For the child in whom the film and the clinical picture do not fit, the disposition is escalation — a senior review, a different modality (ultrasound, CT, MRI), or a repeat film in a better position — because the film that does not fit is not a finished investigation. [1]
For the intensive-care child, the disposition is serial films to track the lung disease and to monitor the lines and tubes, read with the ventilatory and gas-exchange data, and integrated into the daily plan. [4]
Special Populations
The approach to the chest radiograph is adjusted for the child in front of you, and the fellowship candidate must show that they can match the reading priority and the differential to the population. [4] [7]
In the neonate and preterm infant, the film is dominated by surfactant deficiency, the lines and tubes of intensive care, and the risks of both barotrauma and volutrauma. The chronic lung disease of prematurity shows a cystic, hyperinflated pattern over weeks, and the film is read to track the evolution and to detect complications such as a pneumothorax or a pulmonary interstitial emphysema. [4]
In the immunocompromised child, including the oncology patient and the transplant recipient, the differential of a pulmonary opacity broadens to include opportunistic infection (Pneumocystis, fungal), atypical presentation of bacterial pneumonia, drug toxicity, and relapse of malignancy. The film is read with a lower threshold to escalate to high-resolution CT, and with the knowledge that the CXR is insensitive and may lag the clinical picture. [7]
In the child with cystic fibrosis or chronic lung disease, serial films track the progression of bronchiectasis, hyperinflation, and the characteristic upper-lobe predominance. The film is one part of a multi-modal surveillance that includes CT for finer detail and lung function in the cooperative child. [7]
In the child with complex congenital heart disease, the film is read for the heart size and shape, the pulmonary vascular pattern, and the position of surgical hardware (struts, stents, valves). The echocardiogram and the cardiac MRI are the definitive tests, and the CXR is a screening and surveillance tool. [11]
In the Indigenous, remote, or under-resourced setting, the access to paediatric radiology reporting and to alternative modalities may be limited. The equity intervention is a careful clinical assessment, a single well-indicated film where it will change management, and the use of the WHO chest-film reading standard for pneumonia and tuberculosis surveillance — the film is a tool, not a substitute for examining the child. [2] [7]
In the technology-dependent or neurodivergent child, the film is obtained with attention to positioning, to the minimisation of repeats, and to the communication with the family about what the film will and will not show. [4]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric chest-radiograph interpretation has matured in three areas: the prevalence of pneumonia in the wheezing child, the consequences of patient rotation, and the radiation-aware movement. The candidate should know each one and the regional deltas that follow from them. [1] [10]
The prevalence of radiographic pneumonia in wheezing children was quantified in a systematic review and meta-analysis, which found a substantially lower prevalence than historical estimates. The implication is that the routine chest radiograph in the uncomplicated wheezy child adds little to management and exposes the child to radiation without benefit, and current guidelines recommend against routine films in bronchiolitis and uncomplicated wheeze. [10]
The consequences of patient rotation were the subject of a focused review showing that rotation alone changes the apparent size and contour of the heart and great vessels enough to alter a report, and that the asymmetric clavicles and the off-centre spinous process are the reliable markers of rotation. The teaching is that a rotated film is a limited film, and the heart and mediastinum are not reliable on it. [3]
The radiation-aware movement — Image Gently, the ICRP paediatric publication, and the ALARA principle — has driven dose reduction in paediatric radiography, the substitution of ultrasound and MRI for many chest questions, and the principle of justification: the film is requested when it will change management. Children are more radiosensitive than adults per unit dose, which is the biological basis for the principle. [8] [9]
Radiographic pneumonia in wheezing children — systematic review and meta-analysis (Acad Emerg Med 2024)
PMID 39189186
Population: Children presenting with wheeze
Comparator: Prevalence of radiographic pneumonia
Key finding
The prevalence of radiographic pneumonia in wheezing children was substantially lower than historical estimates, supporting the recommendation against routine chest radiographs in uncomplicated wheeze and bronchiolitis.
Where the evidence is weak or contested: the exact threshold for a follow-up film after pneumonia, the role of routine pre-operative chest radiographs in elective surgery, the optimal modality for the suspected foreign body when the expiratory film is equivocal, and the value of artificial-intelligence-assisted reading in low-resource settings. Each is a defensible topic for the viva. [1] [12]
Exam Pearls
The fellowship examiner expects a candidate who reads the technical quality first, applies a systematic method, recognises the paediatric-specific normal, and folds in the clinical picture. [1] [3]
The single most testable principle is that the technical quality is checked before the lung fields are read. Patient rotation is recognised by asymmetric clavicles and an off-centre spinous process and makes the heart and mediastinum unreliable; a poor inspiration is recognised by fewer than nine posterior ribs crossing the diaphragm and enlarges the heart; and a borderline CTR on an AP, supine, under-inspired film is not cardiomegaly. [3] [6]
The single most testable developmental fact is that the normal paediatric thymus produces the sail sign and is not a mass. The thymus is large in the infant, has a sharp angular inferior border, changes shape with respiration, involutes with stress and regrows on recovery, and must be recognised as normal to avoid unnecessary escalation. [5]
The named radiographic signs the exam rewards for knowing: the silhouette sign (localises disease by the border it erases), the air bronchogram (confirms alveolar disease), the meniscus sign (a pleural effusion), the deep sulcus sign (a pneumothorax on a supine film), the spine sign (retrocardiac lower-lobe consolidation), and the sail sign (the normal thymus). [1] [4]
The classic distractors the exam rewards for naming: reading the lung fields before the tubes and lines; overcalling cardiomegaly on an AP film; calling the thymus a mass; accepting a normal inspiratory film in a coughing child with suspected foreign body; treating a normal film as reassuring in an unwell child; and requesting films reflexively without justification. Each is wrong for a specific reason. [1] [12]
References
- [1]Bramson RT, Griscom NT, Cleveland RH Interpretation of chest radiographs in infants with cough and fever Radiology, 2005.PMID 15983074
- [2]Shah SN, Bachur RG, Simel DL, et al Does This Child Have Pneumonia?: The Rational Clinical Examination Systematic Review JAMA, 2017.PMID 28763554
- [3]Marais J, Venkatakrishna SSB, Calle-Toro JS, et al Patient rotation chest X-rays and the consequences of misinterpretation in paediatric radiology Paediatr Respir Rev, 2023.PMID 37244797
- [4]Barnes N, Pilling DW Interpretation of the neonatal chest X-ray Hosp Med, 1999.PMID 10707187
- [5]Wee T, Lee AF, Nadel H, et al The paediatric thymus: recognising normal and ectopic thymic tissue Clin Radiol, 2021.PMID 33762135
- [6]Rosendahl K Pediatric chest and hand radiographs revisited Acta Radiol, 2005.PMID 16134306
- [7]Pitcher RD, Beningfield SJ, Zar HJ The chest X-ray features of chronic respiratory disease in HIV-infected children--a review Paediatr Respir Rev, 2015.PMID 25736908
- [8]Connolly B, Racadio J, Towbin R Practice of ALARA in the pediatric interventional suite Pediatr Radiol, 2006.PMID 16862417
- [9]Strauss KJ, Goske MJ Estimated pediatric radiation dose during CT Pediatr Radiol, 2011.PMID 21847725
- [10]Shah SN, Monuteaux MC, Neuman MI Prevalence and predictors of radiographic pneumonia in children with wheeze: A systematic review and meta-analysis Acad Emerg Med, 2024.PMID 39189186
- [11]Chaudhary S, Jeevika, Jha S The Cardiothoracic Ratio on Trial Acad Radiol, 2025.PMID 40947292
- [12]Sehgal A, Singh V, Chandra J, et al Foreign body aspiration Indian Pediatr, 2002.PMID 12466569