Paeds · investigations-procedures-and-technology
Neuroimaging selection and radiation-aware practice
Also known as Neuroimaging in children · CT versus MRI · PECARN head injury rule · Paediatric radiation safety · ALARA in children · Image Gently
Fellowship guide to choosing between CT, MRI, cranial ultrasound and skull radiograph in infants and children, and to the radiation-aware principles that govern that choice. Covers why CT uses ionising radiation and MRI does not, why the paediatric brain carries a measurably higher lifetime attributable cancer risk per millisievert with the Brenner, Pearce and Meulepas cohort estimates, the ALARA principle and its four levers, the PECARN paediatric head injury prediction rules reproduced verbatim for the under-two and two-and-over arms, the indications for urgent neuroimaging in seizures, stroke, shunt malfunction, raised intracranial pressure and suspected abusive head trauma, the MRI safety issues in children including sedation and gadolinium, the regional guideline differences (NICE, PECARN, Canadian, RCH Melbourne, RCPCH), and how to counsel a parent accurately about the absolute and relative radiation risk of a single head CT.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
Overview & Definition
Picture the toddler who has just fallen from a shopping trolley, crying but alert, or the seven-year-old sent up from the general practitioner with a first-ever afebrile seizure overnight. In both, the team faces the same question: does this child need a picture of the brain, and if so, which picture. That question is the territory this page owns — not the brain itself, but the choice between the modalities that image it, and the radiation-aware reasoning that keeps the child safe while the question is answered. [10] [12]
Neuroimaging is the production of an image of the brain, its coverings, its vessels and the surrounding skull and cerebrospinal-fluid spaces. In modern paediatric practice the four modalities in routine use are computed tomography (CT), magnetic resonance imaging (MRI), cranial ultrasound, and the skull radiograph. Each answers a different question, each carries a different trade-off between speed, cooperation, diagnostic yield and — crucially for the child — radiation dose. The fellowship skill being tested is reading the clinical question, choosing the modality that answers it at the lowest harm, and defending that choice with the evidence. [10] [12]
The reason radiation-aware practice is a distinct skill in children is that children are not small adults when it comes to ionising radiation. A given effective dose delivered to a child carries a measurably higher lifetime attributable cancer risk than the same dose delivered to an adult, both because the child has more rapidly dividing tissue and because the child has many more decades over which a radiation-induced malignancy can emerge. The cohorts that established this — Brenner's risk model, the UK CT-in-childhood study of Pearce, and the Dutch cohort of Meulepas — changed practice: they did not forbid CT, but they made every paediatric CT a deliberate, justified, dose-optimised decision. [2] [3] [4]
Classification
Sort neuroimaging by what it shows, how fast it answers, whether it uses ionising radiation, and whether the child can cooperate — because those four axes decide which modality solves the clinical problem at the lowest harm. [10] [12]
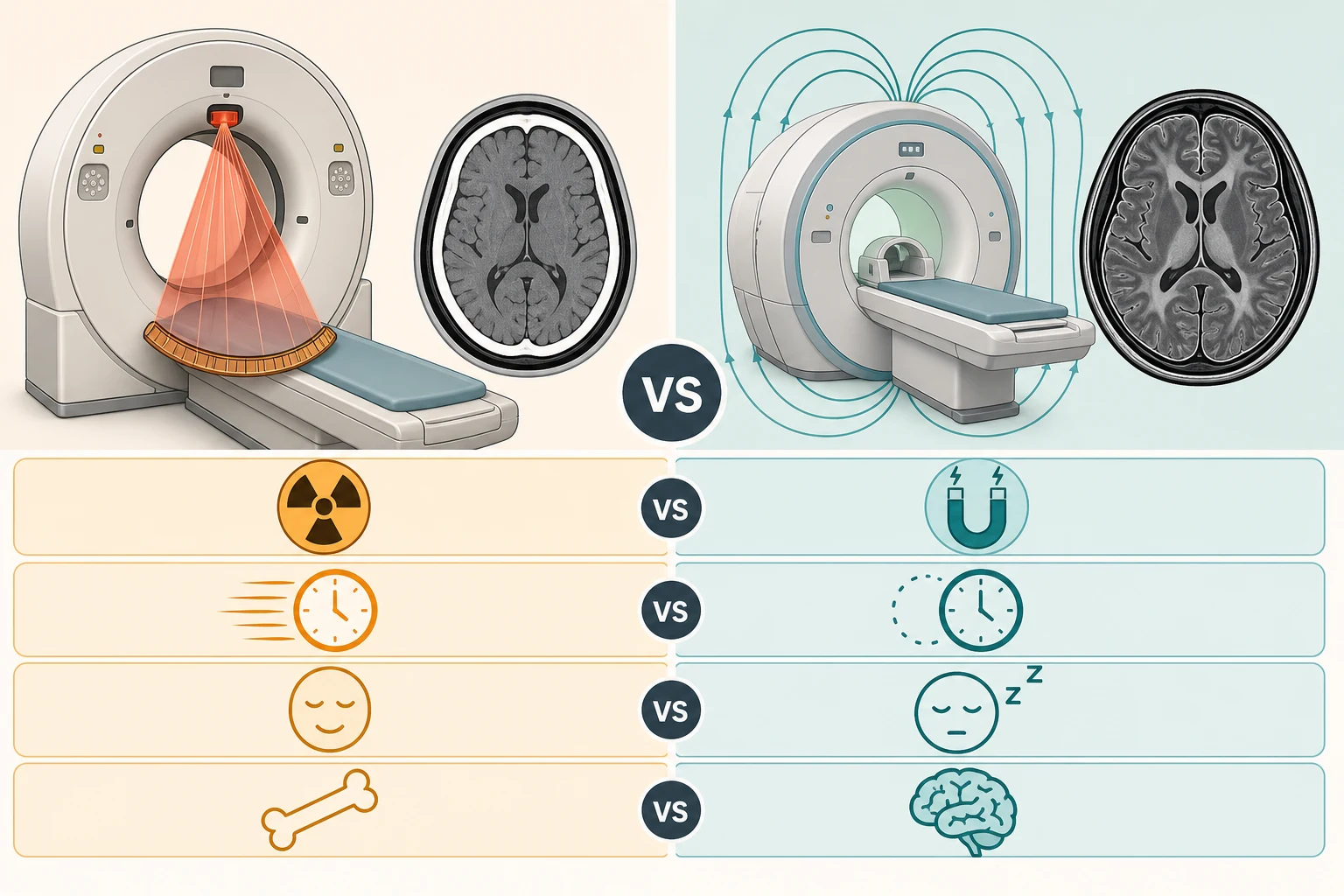
Computed tomography (CT) passes a fan of X-rays around the child and reconstructs, by computer, a Hounsfield-unit map of tissue density. It is fast (seconds), widely available, shows bone and acute haemorrhage with high sensitivity, and almost never requires sedation. Its cost is ionising radiation and a lower soft-tissue contrast than MRI. Magnetic resonance imaging (MRI) places the child in a strong static magnetic field and excites hydrogen nuclei with radiofrequency pulses, reading the relaxation signal to construct images weighted for T1, T2, diffusion, perfusion or flow. It uses no ionising radiation and shows the soft tissues of the brain with unmatched detail, including myelination, cortical architecture, and — through diffusion-weighted imaging — acute ischaemia within minutes. Its costs are time (minutes to an hour), claustrophobia and noise, and the frequent need for sedation or anaesthesia in the child who cannot keep still. [10] [11]
Cranial ultrasound images the brain through the open anterior fontanelle using high-frequency sound, requires no ionising radiation and no sedation, and is the bedside modality of the neonate — the screen for germinal matrix haemorrhage, intraventricular haemorrhage and periventricular leucomalacia in the preterm and unwell term infant. Once the fontanelle closes it has no routine intracranial role. The skull radiograph images bone only and has a narrow modern place: the skeletal survey in suspected non-accidental injury, and occasionally the documentation of a depressed skull fracture. It does not assess the brain, and it has no routine role in minor head injury. [10]
CT versus MRI at a glance
Computed tomography (CT)
- Ionising X-rays — small but real attributable cancer risk per scan
- Fast acquisition (seconds) — ideal for the unstable or uncooperative child
- Best for bone, acute haemorrhage, calcification, acute hydrocephalus
- Usually no sedation; lower soft-tissue contrast than MRI
- First line: major trauma, acute haemorrhage, shunt malfunction when MRI unavailable
Magnetic resonance imaging (MRI)
- No ionising radiation — no attributable cancer risk
- Slow acquisition (minutes to an hour) — needs a still child
- Best for soft tissue, myelin, water, diffusion, acute ischaemia
- Often needs sedation or general anaesthesia in the young; gadolinium and device issues
- First line: first unprovoked seizure, developmental delay, tumour, stroke, diffuse axonal injury
The numbers that anchor your viva
Epidemiology & Risk Factors
Neuroimaging is among the commonest investigations a paediatrician requests, and head CT is the single largest contributor to the paediatric medical radiation dose. The child at greatest cumulative dose is the one who is scanned repeatedly: the shunted child with hydrocephalus, the oncology patient on surveillance, the complex chronic neurological patient, and the child who re-presents after trauma. For each, the dose accumulates across years, and the request is the unit of harm that must be justified every time. [3] [4]
The child at greatest per-scan risk is not the one you might guess by size alone. The attributable cancer risk from a given effective dose falls with age at exposure, so the infant and young child carry the highest per-scan risk — more rapidly dividing tissue, and a longer remaining lifespan over which a radiation-induced cancer can express. This age-sensitivity is the physiological reason radiation-aware practice matters most in the youngest children, and the reason paediatric protocols must reduce the milliampere-seconds and kilovoltage peak rather than simply apply an adult setting. [2] [12]

Pathophysiology
To explain the radiation risk, follow the dose from the X-ray tube to the DNA. The CT scanner rotates a fan of photons around the child; the photons are attenuated to different degrees by bone, soft tissue, fat and air, and a computer reconstructs that attenuation map into the image you read. The photons that pass through deposit a small amount of energy in the tissue along the way, and that is the dose. After the scan, no residual radiation remains in the child. [2] [10]
The carcinogenic lesion is the misrepaired DNA double-strand break. Ionising radiation injures DNA in two ways: directly, by breaking the phosphodiester backbone, and indirectly, by generating free radicals that damage the bases. Most damage is repaired faithfully; a small fraction is misrepaired, and a misrepaired break in a critical gene can, years to decades later, initiate a malignancy. The modern understanding of low-dose diagnostic risk is stochastic — meaning the probability of harm rises with dose, with no threshold assumed below which the risk is zero. This non-threshold assumption is the scientific basis for the ALARA principle: it is not that a single head CT is dangerous, but that no dose is free of risk, so every dose must be justified and minimised. [2] [3]
Contrast this with MRI, which produces images by a fundamentally different physics. A strong static magnetic field aligns the hydrogen nuclei (protons) in the body's water and fat; radiofrequency pulses tip those aligned protons, and the receiver reads the signal as they relax back to equilibrium. T1-weighting, T2-weighting, diffusion-weighting, susceptibility-weighting and flow-sensitive sequences each exploit a different relaxation property. No ionising radiation is involved at any point, and so the attributable cancer risk of an MRI is zero. The MRI-specific risks are instead mechanical and pharmacological: the ferromagnetic projectile, the implanted device, the gadolinium-based contrast, and — above all in children — the need for sedation or anaesthesia to achieve a still scan. [10] [11]
[2] [3]Clinical Presentation
The child who needs neuroimaging comes to you as a clinical question, not a modality request. The skill is to translate each presentation into the question the imaging must answer, because the question determines the modality. [1] [10]
The trauma child asks: is there intracranial injury. The first seizure child asks: is there a structural lesion underlying this. The focal deficit or altered conscious state child asks: is there a stroke, a haemorrhage, or raised pressure. The shunted child asks: is the shunt working. The developmental delay or regression child asks: is there a structural, metabolic, or myelination abnormality. The suspected non-accidental injury child asks: is there intracranial injury, and is there evidence of inflicted trauma. Each of these is a different question, and each has a preferred modality.
[10] [11]The red-flag features that mandate urgent imaging rather than observation are constant across presentations: a depressed or deteriorating conscious state, focal neurology, signs of raised intracranial pressure (a bulging fontanelle, papilloedema, or Cushing's triad of bradycardia, hypertension and irregular respirations), a post-traumatic seizure, suspected abusive injury, and the child who is clinically unstable. These are the children for whom the imaging is non-negotiable; the only question is which modality, and how to get the child to it safely. [1] [11]
The atypical and difficult presentations deserve special mention. The non-verbal or developmentally delayed child cannot tell you about headache or visual change, so the threshold to image is set by behaviour and examination. The neonate with an open fontanelle may show only a full fontanelle, apnoea, or a seizure as the sign of an intracranial catastrophe. The child with a pre-existing shunt who decompensates may have obstruction, infection, or overdrainage, and the imaging must be read against the baseline. The immunocompromised child may mount little inflammatory response, so a normal-looking presentation can hide an aggressive lesion; the threshold to image is lower. [10] [11]
Differential Diagnosis
The differential for neuroimaging decisions is best framed as the imaging question itself — for each presentation, the pathology the imaging is looking for, and the modality that shows it. [1] [11]
In trauma, the differential is extradural haematoma, subdural haematoma, traumatic subarachnoid haemorrhage, intraparenchymal contusion or haemorrhage, depressed or basilar skull fracture, and diffuse axonal injury. CT is the first-line modality because it shows acute blood, fracture, and mass effect within seconds, and is safe for the unstable child on a spinal board. MRI is reserved for the child with persistent coma or deficit and a normal early CT, in whom diffuse axonal injury is suspected — the fluid-attenuated inversion recovery and susceptibility-weighted MRI sequences are far more sensitive to the microscopic shearing injury than CT. [1]
In the first unprovoked seizure, the differential is focal cortical dysplasia, a low-grade tumour (ganglioglioma, dysembryoplastic neuroepithelial tumour), a vascular malformation, mesial temporal sclerosis, or a neurocutaneous stigmata of tuberous sclerosis or neurofibromatosis. MRI is the modality of choice, with a dedicated epilepsy protocol that includes high-resolution coronal T2 and fluid-attenuated inversion recovery sequences through the temporal lobes. An urgent CT is indicated only if the seizure is prolonged, focal, or followed by a persistent deficit, in which case an acute haemorrhage or mass must be excluded. [5] [6]
In suspected stroke, the differential is arterial ischaemic stroke, intracranial haemorrhage, cerebral sinovenous thrombosis, and the mimickers of a postictal Todd's paresis or a hemiplegic migraine. The modality is urgent MRI with diffusion-weighted imaging and arterial and venous magnetic resonance angiography, which demonstrates acute ischaemia within minutes of onset — far earlier than CT, which is often normal in the first hours. A CT or CT angiography is reserved for the child who cannot access urgent MRI, or who needs to exclude haemorrhage before an intervention. [11]
Clinical & Bedside Assessment
Before any neuroimaging, run a structured bedside assessment that turns the child's presentation into a modality choice and a safe pathway to the scanner. [1] [10]
Begin with the ABCDE and the paediatric Glasgow Coma Scale, scaled to age. Examine the pupils for size and symmetry, and perform a focused neurological examination looking for a lateralising or localising deficit. In the infant, feel the anterior fontanelle, measure the head circumference against previous measurements, and examine the fundi for papilloedema where feasible. Inspect the skin for neurocutaneous stigmata (ash-leaf macules, café-au-lait patches, port-wine stain) and for bruising in patterns that suggest non-accidental injury. The bedside assessment is what refines the imaging decision: a well child with a normal examination and a low-risk mechanism avoids CT; an abnormal GCS, a focal sign, or a bulging fontanelle escalates it. [1] [8]
The assessment of stability for transfer is the step most often missed. A child who is unstable — shocked, hypoventilating, or protecting their airway poorly — must be resuscitated and often intubated before leaving the resuscitation bay for the scanner. The scanner is a hostile environment: it is isolated, the child is inaccessible during acquisition, and resuscitation is harder through the gantry. The rule is absolute: resuscitation precedes imaging, and an unstable child is stabilised — or intubated — before transfer, accompanied by a team that can manage the airway and the circulation en route. [1] [10]
Investigations
The investigations section of this topic is the modality-selection rules themselves, reproduced verbatim, because these rules are the examinable content. The two pillars are the PECARN head injury prediction rules for trauma, and the modality-of-choice framework for non-traumatic presentations. [1] [10]
The PECARN head injury prediction rules (reproduced verbatim)
The PECARN (Pediatric Emergency Care Applied Research Network) rules, derived from the landmark prospective cohort of Kuppermann and colleagues, identify children at very low risk of a clinically-important traumatic brain injury in whom CT can be safely avoided. They are designed to reduce CT use, not to find every injury. The rules apply to children with a Glasgow Coma Scale of 14 or 15 after a head injury, and they branch by age. [1]
PECARN — children under two years
Altered mental status (GCS 14, or not acting normally per the team or parent)
Palpable skull fracture (or signs of basilar skull fracture: haemotympanum, racoon eyes, Battle sign, cerebrospinal-fluid rhinorrhoea or otorrhoea)
Scalp haematoma, especially occipital, parietal or temporal
Loss of consciousness for more than 5 seconds
Severe mechanism of injury (fall of more than a metre for this age, motor-vehicle crash with ejection or death of a passenger, or impact from a high-speed object)
Not acting normally according to the parent
PECARN — children two years and over
Altered mental status (GCS 14, or agitated, somnolent, or slow to respond)
Signs of basilar skull fracture (haemotympanum, racoon eyes, Battle sign, cerebrospinal-fluid rhinorrhoea or otorrhoea)
Loss of consciousness (any, in the original rule)
Severe mechanism of injury (fall of more than 1.5 metres, motor-vehicle crash with ejection or death of a passenger, bicycle without a helmet, or impact from a high-speed object)
Severe headache
Vomiting
The disposition follows directly from the count of predictors. A child who meets none of the age-specific predictors is at very low risk of a clinically-important traumatic brain injury (negative predictive value well over 99 percent in the derivation cohort), and CT is not indicated — the child is observed briefly and discharged with written advice. A child with one of several defined isolated findings — for example, an isolated loss of consciousness, an isolated scalp haematoma in a fall, an isolated episode of vomiting, or an isolated severe mechanism — is at intermediate risk; the recommendation is observation for a period of hours, with CT performed only if symptoms evolve, and the decision shared with the family. A child with any of the higher-risk findings — an altered mental status, a palpable skull fracture, or signs of a basilar skull fracture — warrants CT now. [1]
[1]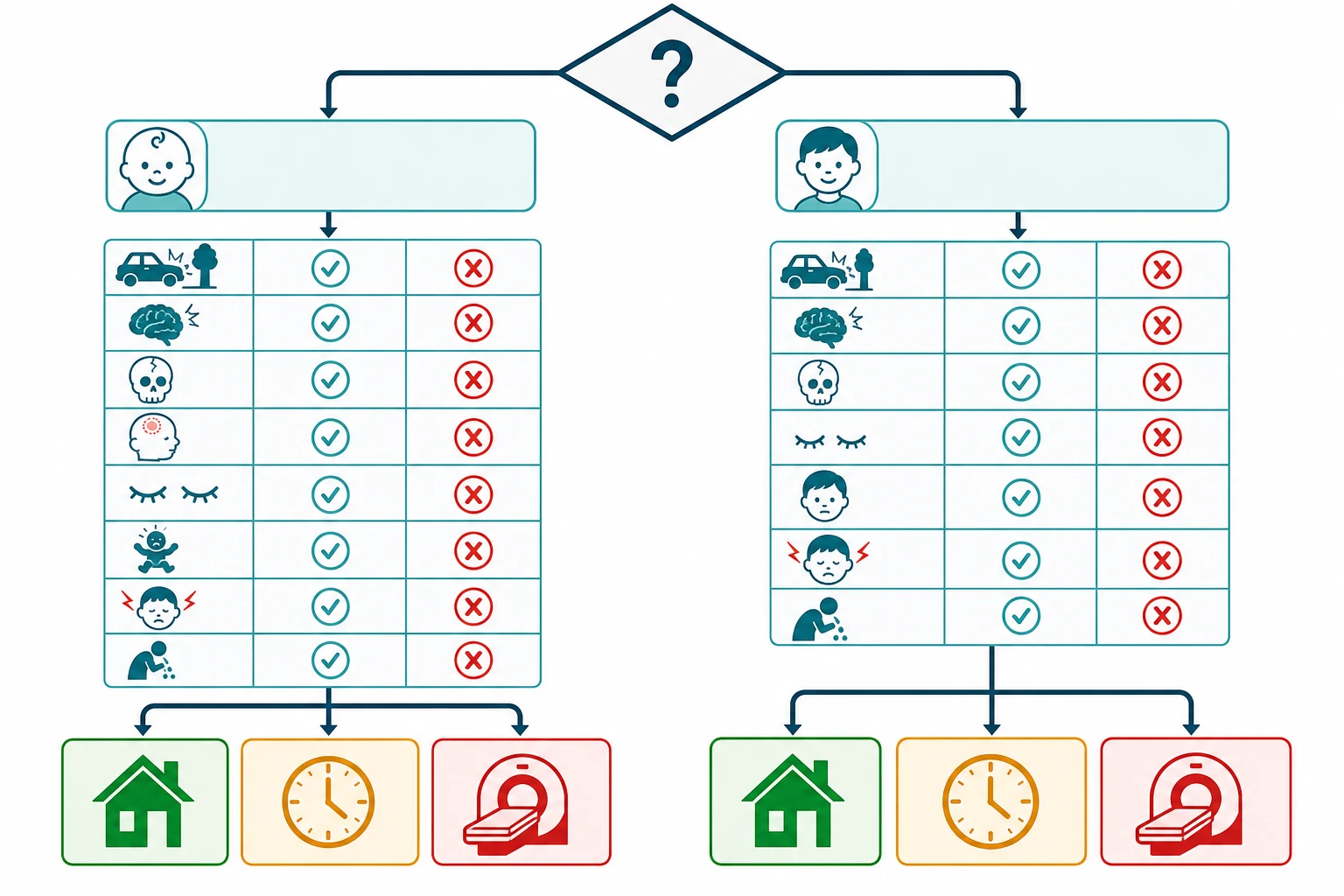
Modality of choice for the non-traumatic presentations
For the child whose imaging question is not trauma, the modality follows the pathology being sought. [5] [10]
| Clinical question | First-line modality | Why, and the caveat |
|---|---|---|
| First unprovoked seizure (well child) | Elective MRI (epilepsy protocol) | Excludes focal cortical dysplasia, tumour, vascular malformation; urgent CT only if focal signs, prolonged postictal state, or altered conscious state (Cite id=5,6). |
| Simple febrile seizure (well child, returned to baseline) | No routine imaging | Imaging is not routinely indicated; the decision is driven by the child's mental state and the possibility of meningitis (Cite id=7). |
| Complex febrile seizure or not back to baseline | Urgent CT or MRI | Imaging when focal, prolonged, or recurrent, or when the child has not returned to baseline; rule out meningitis first (Cite id=7). |
| Developmental delay or regression | MRI | Detects structural, myelination, and leucodystrophic abnormalities; CT has no role unless MRI is unavailable. |
| Suspected brain tumour | MRI | Characterises the lesion; CT may show calcification or acute hydrocephalus in the unstable child (Cite id=8). |
| Suspected arterial ischaemic stroke | Urgent MRI with diffusion-weighted and MR angiography | Diffusion-weighted MRI shows ischaemia within minutes; CT or CT angiography if MRI is delayed (Cite id=11). |
| Suspected cerebral sinovenous thrombosis | MRI with MR venography | MR venography demonstrates the occluded sinus; CT venography is an alternative. |
| Suspected shunt malfunction | Rapid cranial CT, or rapid MRI | CT excludes acute hydrocephalus in seconds; rapid MRI protocols (HASTE, BLADE) reduce the cumulative dose in the repeatedly scanned child. |
| Suspected abusive head trauma | CT acutely, then MRI | CT for acute haemorrhage and fracture; MRI for diffuse axonal injury and dating of injuries; plus skeletal survey and ophthalmology. |
| Neonatal intracranial surveillance | Cranial ultrasound | The bedside screen of the preterm and unwell term infant through the open fontanelle. |
The simple febrile seizure is the presentation most often over-imaged, and the rule is worth stating explicitly: in a child who has had a simple febrile seizure and has returned to baseline, neuroimaging is not routinely indicated. The imaging decision is driven instead by the child's mental state, the possibility of meningitis, and any focal features — and it is the meningitis that must be excluded, not a structural lesion. [7]
For the first unprovoked seizure, the American Academy of Neurology practice parameter establishes that an elective MRI is the modality of choice in the well child, and that emergent imaging is reserved for the child with a focal deficit, a prolonged postictal state, or an altered conscious state. Shinnar and colleagues showed that a meaningful proportion of children with an apparent first unprovoked seizure have structural abnormalities on MRI, which underpins the recommendation to image. [5] [6]
The effective dose in context
The risk discussion depends on a grasp of the dose. A paediatric head CT delivers an effective dose of the order of 1 to 2 mSv with modern dose-optimised protocols, comparable to several months of natural background radiation (around 2 to 3 mSv per year in most regions). An adult head CT is similar. The attributable cancer risk from a single paediatric head CT is small and stochastic — of the order of one excess cancer per 10,000 scans in the cohort estimates — and is higher in the youngest children. MRI delivers zero ionising-radiation dose. [2] [3] [4]
Management — Resuscitation
The immediate priority when a child needs urgent neuroimaging is the order of operations: resuscitation first, imaging second. An unstable child must never be transferred to the scanner before the airway and the circulation are secured, because the scanner is an isolated, inaccessible environment in which resuscitation is harder. [1] [10]
A child with a falling conscious state, raised intracranial pressure, or a compromised airway is intubated before transfer to CT, using a rapid-sequence technique with a neuroprotective induction. The neuroprotective bundle is applied throughout: the head is kept midline, the bed is head-up to 30 degrees, and normocapnia, normoglycaemia and normothermia are maintained. If there are clinical signs of herniation — a falling conscious state, an asymmetric or dilated pupil, decerebrate or decorticate posturing, or Cushing's triad — an immediate osmolar agent is given while imaging is arranged. The accepted options are 3 percent hypertonic saline (commonly 2 to 5 mL per kg intravenously over 10 to 30 minutes) or mannitol (commonly 0.25 to 1 g per kg intravenously), per the local protocol, alongside urgent neurosurgical referral. [1] [10]
The modality in this resuscitation setting is almost always CT, because CT is fast, available, and shows the acute haemorrhage, the mass effect, and the hydrocephalus that drive the immediate surgical decision. MRI is reserved for the stable child in whom the question is soft tissue, diffusion, or myelin.
[1] [10]Management — Definitive & Stepwise
The definitive skill is a stepwise framework that turns the clinical question into the modality at the lowest harm. The framework has four steps, and it encodes the ALARA principle at each one. [10] [12]
Step 1 — Justify every request
Ask whether any imaging is needed, whether it is needed now, and what question it will answer. A justified request names the clinical question and the expected change in management. An unjustified request — for reassurance, for defensive medicine, or to satisfy a parent — is the commonest source of avoidable paediatric radiation. The PECARN rules are the worked example: they justify not scanning the very-low-risk child. [1] [10]
Step 2 — Choose the lowest-harm modality that answers the question
Where a non-ionising modality answers the question as well as CT, choose it. MRI in place of CT for shunt surveillance, for developmental delay, for the first unprovoked seizure, and for elective tumour follow-up is the single most effective radiation-aware substitution. Cranial ultrasound in place of CT in the neonate is another. Where CT is the modality that answers the question — acute trauma, acute haemorrhage in the unstable child — choose it without hesitation; the radiation risk is real but it is not a reason to delay a necessary scan. [10] [11]
Step 3 — Optimise the dose when CT is the choice
When CT is the modality, the dose is optimised to the child. This means a paediatric protocol that scales the milliampere-seconds and the kilovoltage peak to the child's size, limits the scan to the region of interest, avoids multiphase acquisitions where a single phase answers the question, and uses the iterative reconstruction that modern scanners provide. The Image Gently alliance and the ALARA consensus built these principles into routine practice; the requesting paediatrician's contribution is to communicate the clinical question clearly so the radiographer can apply the right protocol. [10] [12]
Step 4 — Limit repeat scanning
Cumulative dose accumulates across years in the child who is scanned repeatedly. The shunted child, the oncology patient, and the complex chronic neurological patient are the highest-cumulative-dose groups, and each repeat request must be justified on its own merits. The modern shift is to rapid MRI protocols (single-shot fast spin-echo sequences such as HASTE or BLADE) for shunt surveillance, which deliver a diagnostic image of the ventricles in seconds without ionising radiation, accepting the trade-off of reduced detail in the brain parenchyma. [3] [10]
The MRI workflow in the young child
The practical barrier to MRI in the young child is cooperation. A brain MRI takes minutes to an hour and demands stillness; a moving child produces a non-diagnostic scan, and a repeat scan doubles the cost and the anaesthetic burden. The age-stratified approach has three tiers. In the neonate and young infant, a feed-and-wrap technique — feeding the child, swaddling, and using foam immobilisation — succeeds in a high proportion without sedation. In the cooperative preschool child, play therapy and a mock scanner programme desensitises the child to the noise and the bore and achieves a still scan without sedation in many centres. In the child who cannot cooperate, procedural sedation or general anaesthesia is required, and the trade-off is explicit: the small but real risk of sedation is weighed against the benefit of the diagnostic information, with the principle that a justified MRI is worth a carefully conducted anaesthetic, and an unjustified one is not. [10] [11]
Communicating the radiation risk to a parent
The communication is the fellowship skill that the viva station examines, and it hinges on two numbers in plain language. A single paediatric head CT carries an effective dose of the order of 1 to 2 mSv, comparable to several months of natural background radiation, and an attributable lifetime cancer risk of the order of one in 10,000 — a real but very small increase over the background lifetime cancer risk of roughly one in three. The framing that lands is the comparison: the risk of the scan is far smaller than the risk of missing the injury the scan is looking for, and far smaller than the everyday risks a family accepts. The paediatrician documents the discussion and the justification, and offers the alternative (observation, or MRI) where it answers the question. [2] [3] [4]
Specific Subtypes & Scenarios
Each subtype is the imaging question applied to a specific presentation; the rules above resolve each one. [1] [10]
Paediatric head trauma is the worked example of PECARN. For a given vignette — the toddler who falls from a shopping trolley, the school-age child who falls off a bicycle without a helmet, the infant dropped from a carer's arms — apply the age-specific predictors and state the disposition: no CT, observe, or CT now. The higher-risk findings (altered mental status, palpable skull fracture, signs of basilar skull fracture) drive CT; the isolated intermediate-risk findings drive observation. [1]
First afebrile seizure in the well child is an elective MRI with an epilepsy protocol. Urgent imaging — CT or MRI — is reserved for the focal, the prolonged, the postictally persistent, or the child with an altered conscious state, in whom an acute haemorrhage or mass must be excluded. The ILAE Commission of Pediatrics Task Force recommendations and the American Academy of Neurology practice parameter converge on this. [5] [9]
Complex febrile seizure drives imaging when the seizure is focal, prolonged, or recurrent, or when the child has not returned to baseline — and the first question is whether meningitis must be excluded before the imaging question is pursued. The simple febrile seizure, by contrast, does not routinely require imaging. [7]
Suspected stroke is the urgent-MRI scenario. Diffusion-weighted MRI demonstrates acute ischaemia within minutes of onset, and arterial and venous MR angiography define the vascular lesion. CT or CT angiography is reserved for the child in whom urgent MRI is unavailable or in whom haemorrhage must be excluded before an intervention. The Mirsky pathway document codifies this. [11]
Suspected shunt malfunction is the scenario in which the cumulative-dose principle bites hardest. A rapid cranial CT excludes acute hydrocephalus in seconds, but the shunted child will be scanned many times across a lifetime; the modern shift is to rapid MRI protocols that deliver a diagnostic ventricular image without ionising radiation. A shunt tap and a shunt series (plain radiographs of the shunt tubing) are adjuncts to, not substitutes for, the cross-sectional image. [10]
Suspected abusive head trauma is the mandatory-multimodality scenario. A CT in the acute setting excludes subdural, subarachnoid and intraparenchymal haemorrhage and fracture. An MRI, performed when the child is stable, characterises diffuse axonal injury and contributes to the dating of injuries. A skeletal survey and an ophthalmology examination complete the workup, and the imaging must be reported by a radiologist with paediatric and safeguarding expertise. [10]
The neonate and young infant is the ultrasound scenario. Cranial ultrasound through the open fontanelle is the bedside screen for germinal matrix haemorrhage, intraventricular haemorrhage and periventricular leucomalacia in the preterm and the unwell term infant, graded by the Papille system. As the fontanelle closes and as the question shifts to cortical detail, myelination, or a structural lesion, MRI takes over. [10]
Complications & Pitfalls
The complications and pitfalls of neuroimaging in children fall into four categories: the missed injury, the over-imaged child, the sedation-related harm, and the contrast and implant issues. [1] [10]
The missed injury is the trap of the normal early CT. A CT in the first hours after a moderate or severe head injury can be normal even when diffuse axonal injury is present, because the microscopic shearing injury is below the resolution of CT. A child with a persistent depressed conscious state or a focal deficit and a normal early CT warrants an MRI to look for diffuse axonal injury. The corollary is that a normal CT is reassuring only when the child is also clinically well. [1]
The over-imaged child is the trap of cumulative dose. The shunted, oncology, and complex chronic neurological child accumulates dose across years of surveillance scanning; each request must be justified, and the substitution of a rapid MRI protocol for shunt surveillance is the single most effective intervention. The request that is not justified by a change in management is the request to question. [3] [4]
The sedation-related harm is the trap of the MRI in the young. A child who cannot keep still needs procedural sedation or general anaesthesia, each of which carries a small but real risk of respiratory depression, hypoxia, and aspiration. The counterweight is the justification: a justified MRI is worth a carefully conducted anaesthetic, but the sedation risk is the reason to attempt feed-and-wrap, play therapy, and mock-scanner desensitisation first. [10]
The contrast and implant issues are the trap of the modality's physics. Repeated doses of gadolinium-based contrast leave trace deposits in the brain; the request is justified, and a macrocyclic agent is preferred where contrast is needed. Iodinated CT contrast carries extravasation, allergy, and contrast-associated nephropathy risks, with the renal precaution of hydrating the dehydrated child. The ferromagnetic implant and the cardiac device are contraindications to MRI, screened by a documented safety questionnaire before the child enters the controlled zone of the MRI suite. [10] [11]
The incidental finding is the trap of the scan that answered the question but also found something else. White-matter signal change, an arachnoid cyst, and a pineal cyst are common and usually benign; a choroidal fissure cyst and an enlarged perivascular space are normal variants. The principle is to communicate the finding without causing harm: state what it is, what it is not, and the follow-up (if any), and avoid cascading into further unnecessary imaging. [10]
Prognosis & Disposition
The disposition after neuroimaging follows the result and the child's clinical state. [1] [10]
After a normal head CT in minor head injury, the disposition is observation at home with written advice, and the return precautions are explicit: persistent or repeated vomiting, a worsening headache, increasing drowsiness, a seizure, or any focal neurology. The duration of observation in the emergency department is driven by the child's clinical course, and a child who returns to baseline and remains well is discharged with this safety-net. [1]
After an abnormal head CT, the disposition is driven by the lesion. A mass effect, a depressed or compound fracture, an intracranial haemorrhage with shift, or acute hydrocephalus drives an immediate neurosurgical referral and, where indicated, intensive care for the child with raised pressure. The threshold for a repeat scan is a clinical deterioration, and the repeat scan is justified by a change in management. [1] [10]
After an elective MRI, the disposition is the communication of the result by the requesting clinician, with a clear pathway for a significant unexpected finding — a tumour, a vascular malformation, or a metabolic-leucodystrophic pattern — that triggers the appropriate subspecialty referral. [5] [8]
Special Populations
Several populations carry a distinct imaging trade-off, and the fellowship viva examines the reasoning. [3] [10]
The neonate and young infant is the population in whom cranial ultrasound through the open fontanelle replaces CT for routine intracranial surveillance, and in whom feed-and-wrap techniques allow MRI without sedation. The threshold to image is set by the fontanelle, the head circumference, and the neurological examination, and the modality is the lowest-harm one that answers the question. [10]
The shunted child is the population at greatest cumulative dose, and the radiation-aware intervention is the shift from serial CT to rapid MRI protocols for surveillance. Each request is justified on its own merits, and the baseline scan against which an acute change is read is documented and accessible. [3] [10]
The developmentally delayed or autistic child is the population for whom MRI sedation is the hardest decision, and the value of a mock-scanner programme, play therapy, and a specialist sedation service is highest. The trade-off is the sedation risk against the diagnostic yield, and the threshold to scan is the expected change in management. [10]
The oncology patient is the population in whom the balance between surveillance dose and the detection of recurrence is most acute. The shift towards MRI-based surveillance, and the use of dose-optimised CT where CT is unavoidable, is the radiation-aware strategy. [3] [4]
The pregnant adolescent is the population in whom the modality choice includes the fetus. MRI without gadolinium is preferred over CT where it answers the question, and a single head CT in pregnancy — when it is the modality that answers the question — is not an indication for pregnancy termination; the radiation dose to the fetus from a head CT is negligible due to shielding and distance. [10]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric neuroimaging selection and radiation-aware practice rests on four landmark contributions, and the regional guidelines converge on a shared core with local variation. [1] [10]
The PECARN head trauma cohort of Kuppermann and colleagues, published in The Lancet in 2009, is the foundational evidence for the head injury prediction rules. Derived from a prospective cohort of more than 42,000 children, it established the age-specific predictors and their very high negative predictive value for a clinically-important traumatic brain injury, and it gave clinicians a validated tool to reduce CT use in very-low-risk children. It changed practice across North America and informed the United Kingdom, Australian and Canadian guidelines. [1]
The radiation-risk cohorts quantify the harm the PECARN rule exists to reduce. Brenner and colleagues, in the American Journal of Roentgenology in 2001, modelled the lifetime attributable cancer mortality from paediatric CT and put the risk on the map, with an estimate that a single head CT in a young child carries an attributable risk of the order of a fraction of a per cent. Pearce and colleagues, in The Lancet in 2012, reported the UK retrospective cohort of CT scans in childhood and subsequent leukaemia and brain tumour risk, demonstrating a dose-response with cumulative brain dose and bone-marrow dose. Meulepas and colleagues, in the Journal of the National Cancer Institute in 2019, reported the Dutch cohort with longer follow-up and refined dose estimates, confirming the small but real attributable risk and quantifying it as of the order of one excess cancer per thousand to ten thousand paediatric CT scans. These studies do not forbid CT; they justify ALARA. [2] [3] [4]
The ALARA consensus of Frush and Frush, and the Image Gently ALARA CT summit of Goske and colleagues, codified the four levers — justification, optimisation, substitution, and limitation — into routine paediatric practice, and built the paediatric protocol and the dose-reduction technology into modern scanners. They are the bridge between the evidence and the bedside. [10] [12]
For the non-traumatic presentations, the American Academy of Neurology practice parameter of Hirtz and colleagues (2000) established the MRI-first approach to the first unprovoked seizure, reinforced by Shinnar's MRI-yield data. The AAP Subcommittee on Febrile Seizures (2011) codified the no-routine-imaging rule for the simple febrile seizure. The HeadSmart guideline of Wilne and colleagues (2010) gave the primary-care pathway for the child who may have a brain tumour, with the imaging-when-reddflags-are-present principle. The Mirsky pathway document (2017) codified the stroke-imaging sequence, and the ILAE Commission of Pediatrics Task Force (2015) summarised the infantile-seizure recommendations. [5] [6] [7] [8] [9] [11]
The controversies are real but bounded. The magnitude and the extrapolation of the low-dose risk — the linear-no-threshold assumption versus a possible threshold — is debated, but the consensus is to operate on the non-threshold assumption because it is the conservative one. The role of rapid MRI in place of CT for shunt surveillance is expanding, accepting the trade-off of reduced parenchymal detail. The trade-off between sedation risk and radiation risk in the young child who needs imaging is a per-child decision, made with the family and documented.
[2] [3] [10]Exam Pearls
A candidate who holds these one-liners answers the viva and the single-best-answer question. [1] [10]
- PECARN is a rule-out tool. A child who meets none of the age-specific predictors is at very low risk of a clinically-important traumatic brain injury and CT can be avoided; the rules reduce CT, they do not find every injury.
- A single paediatric head CT carries an effective dose of the order of 1 to 2 mSv — comparable to several months of natural background radiation — and a small stochastic attributable lifetime cancer risk of the order of one in 10,000. The risk is real, small, and higher in the youngest children.
- MRI delivers zero ionising-radiation dose and is the modality of choice for the first unprovoked seizure, developmental delay or regression, suspected tumour, stroke, and diffuse axonal injury.
- CT is the modality of choice for acute trauma, acute haemorrhage in the unstable child, suspected skull fracture, and acute hydrocephalus or shunt malfunction when MRI is unavailable.
- Cranial ultrasound is the bedside modality of the neonate with an open fontanelle, screening for germinal matrix and intraventricular haemorrhage and periventricular leucomalacia.
- ALARA — As Low As Reasonably Achievable — through justification, optimisation, substitution of a non-ionising modality, and limitation of repeat scanning.
- A simple febrile seizure in a child who has returned to baseline does not routinely require neuroimaging; the decision is driven by the child's mental state and the possibility of meningitis.
- A normal early CT does not exclude diffuse axonal injury; a persistent depressed conscious state or a focal deficit warrants an MRI.
- A skull radiograph has no routine role in minor head injury; it shows bone only and does not assess the brain.
- Resuscitation precedes imaging. An unstable child is never transferred to the scanner before the airway and the circulation are secured.
References
- [1]Kuppermann N, Holmes JF, Dayan PS, et al Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study Lancet, 2009.PMID 19758692
- [2]Brenner D, Elliston C, Hall E, Berdon W Estimated risks of radiation-induced fatal cancer from pediatric CT AJR Am J Roentgenol, 2001.PMID 11159059
- [3]Pearce MS, Salotti JA, Little MP, et al Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study Lancet, 2012.PMID 22681860
- [4]Meulepas JM, Ronckers CM, Smets AMJB, et al Radiation Exposure From Pediatric CT Scans and Subsequent Cancer Risk in the Netherlands J Natl Cancer Inst, 2019.PMID 30020493
- [5]Hirtz D, Ashwal S, Berg A, et al Practice parameter: evaluating a first nonfebrile seizure in children Neurology, 2000.PMID 10980722
- [6]Shinnar S, O'Dell C, Mitnick R, Berg AT, Moshe SL Neuroimaging abnormalities in children with an apparent first unprovoked seizure Epilepsy Res, 2001.PMID 11248538
- [7]Subcommittee on Febrile Seizures, American Academy of Pediatrics Neurodiagnostic evaluation of the child with a simple febrile seizure Pediatrics, 2011.PMID 21285335
- [8]Wilne S, Koller K, Collier J, Kennedy C, Grundy R, Walker D The diagnosis of brain tumours in children: a guideline to assist healthcare professionals in the assessment of children who may have a brain tumour Arch Dis Child, 2010.PMID 20371594
- [9]Wilmshurst JM, Gaillard WD, Vinayan KP, et al Summary of recommendations for the management of infantile seizures: Task Force Report for the ILAE Commission of Pediatrics Epilepsia, 2015.PMID 26122601
- [10]Frush DP, Frush KS The ALARA concept in pediatric imaging: building bridges between radiology and emergency medicine Pediatr Radiol, 2008.PMID 18810422
- [11]Mirsky DM, Beslow LA, Amlie-Lefond C, et al Pathways for Neuroimaging of Childhood Stroke Pediatr Neurol, 2017.PMID 28274641
- [12]Goske MJ, Strauss KJ, Westra SJ, Frush DP The Image Gently ALARA CT summit on new CT technologies for children Pediatr Radiol, 2014.PMID 25304694