Paeds · investigations-procedures-and-technology
Defibrillation, cardioversion and transcutaneous pacing
Also known as Paediatric defibrillation · Synchronised cardioversion · Transcutaneous pacing · External cardiac pacing · Shockable rhythm management
A fellowship approach to delivering an electric shock or an external pacing stimulus to a child's heart, covering the critical distinction between unsynchronised defibrillation for pulseless ventricular fibrillation and pulseless ventricular tachycardia at 4 joules per kilogram, synchronised cardioversion for a perfusing tachyarrhythmia such as supraventricular tachycardia at 1 joule per kilogram escalating to 2 joules per kilogram, and transcutaneous pacing for symptomatic bradycardia from complete heart block. The page teaches the energy doses, the pad positions (anterolateral and anteroposterior), automated external defibrillator use with attenuated paediatric pads in the under-eight-year-old, the sync function that prevents an R-on-T shock, capture thresholds and analgesia for pacing, and the complications of skin burns, myocardial injury and failure to capture. Every dose is anchored to the 2020 American Heart Association Pediatric Advanced Life Support guidance, the 2021 European Resuscitation Council Paediatric Life Support guidelines, and APLS.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old in the emergency department with a heart rate of 250, pale and breathless, the monitor showing a narrow-complex tachycardia you cannot break with vagal manoeuvres. Now picture a different child, collapsed and pulseless, the monitor showing a chaotic writhing trace of ventricular fibrillation. Both need an electric shock, but the shocks are different, and confusing them can kill. This topic teaches the three ways electricity is delivered to a child's heart: defibrillation, cardioversion, and transcutaneous pacing. [1] [6]
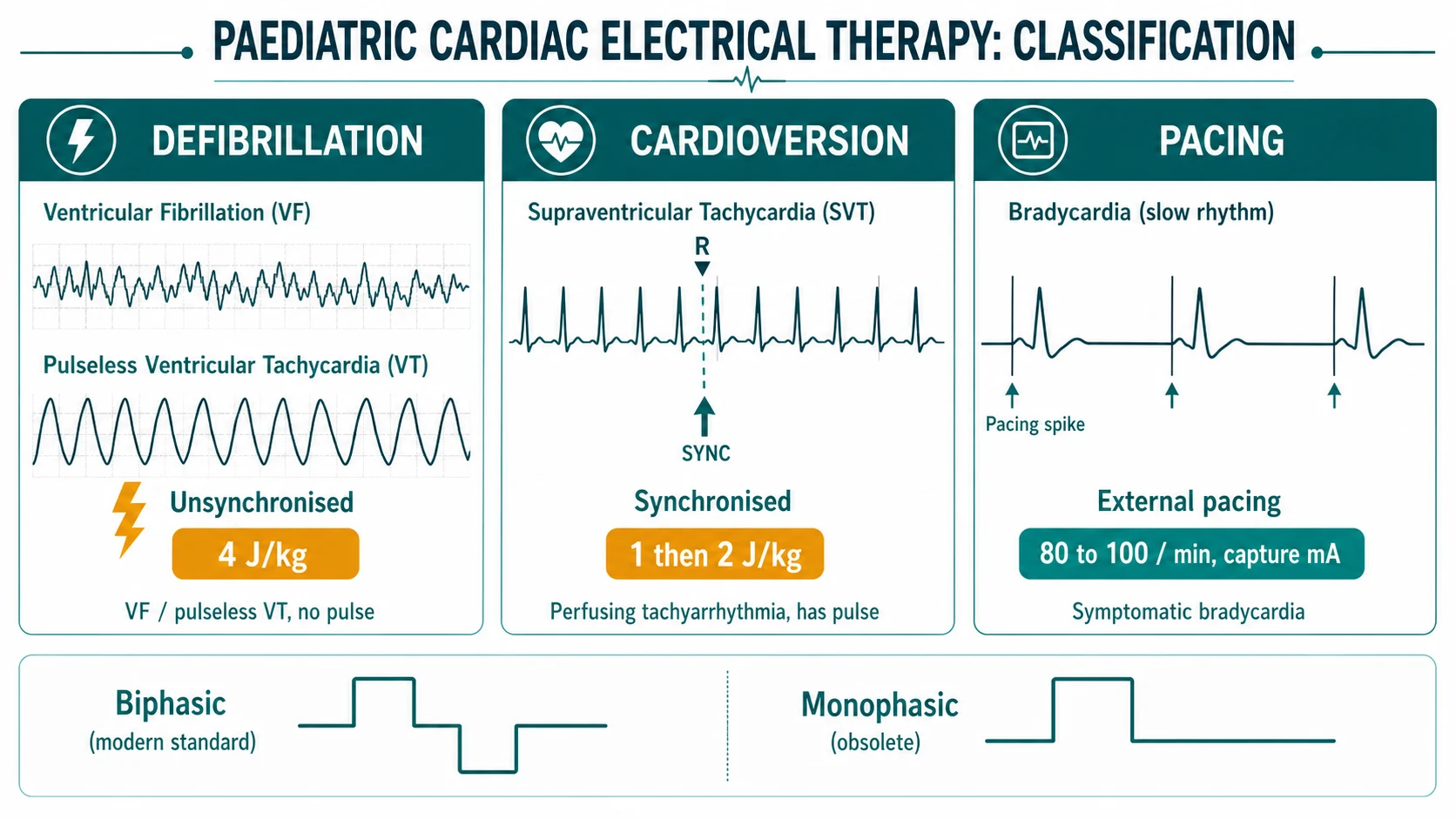
Defibrillation is the unsynchronised delivery of a direct-current shock across the chest to a heart in ventricular fibrillation or pulseless ventricular tachycardia. The goal is to depolarise the whole myocardium at once, extinguish every re-entry circuit, and hand the sinus node a silent heart it can recapture. Synchronised cardioversion is a timed shock, discharged on the R wave, delivered to a heart that still has a perfusing rhythm — supraventricular tachycardia, atrial flutter, or a stable monomorphic ventricular tachycardia with a pulse — when drug therapy has failed or the child is haemodynamically unstable. Transcutaneous pacing is external electrical stimulation of a bradycardic heart through pads on the chest wall, used as a bridge when intrinsic conduction has failed. [1] [5]
The numbers a fellowship candidate must hold in one line are these: defibrillate ventricular fibrillation and pulseless ventricular tachycardia at 4 joules per kilogram; cardiovert a perfusing tachyarrhythmia at 1 joule per kilogram, escalating to 2 joules per kilogram; and pace a symptomatic bradycardia at a rate of 80 to 100 per minute, increasing the output until you see electrical and mechanical capture. [1] [2]
Classification
The candidate should classify these three interventions along two axes at once: the rhythm they treat and the mode of shock delivery. The two axes interact, because the mode is dictated entirely by whether the rhythm carries a pulse. [1] [4]
By rhythm, two families are shockable in arrest: ventricular fibrillation and pulseless ventricular tachycardia. Both are non-perfusing and both receive an unsynchronised shock at the same energy. A perfusing tachyarrhythmia — supraventricular tachycardia, atrial flutter, atrial fibrillation (rare in children), and monomorphic ventricular tachycardia with a pulse — receives a synchronised shock. A symptomatic bradycardia from sinus node dysfunction or atrioventricular block is not shocked at all; it is paced. [1] [4]
By mode, the defibrillator delivers energy in one of three waveforms. The modern biphasic waveform (truncated exponential or rectilinear) reverses polarity mid-shock and is standard on every contemporary machine; it achieves defibrillation at lower energy than the older monophasic waveform, which is now rarely seen. For pacing, the machine emits low-energy timed pulses rather than a single shock. The paediatric implication is that biphasic doses are lower than the historical monophasic ones, and the 4 joules per kilogram figure is a biphasic dose. [3] [9]
Epidemiology & Risk Factors
Cardiac arrest in children is overwhelmingly respiratory and asystolic, not cardiac and fibrillatory, which is why defibrillation is needed far less often in children than in adults — but when it is needed, it must be delivered without hesitation. In-hospital paediatric cardiac arrest occurs in roughly 1 to 2 per cent of admissions in large United States series, and a shockable rhythm is present in roughly 5 to 15 per cent of in-hospital arrests and in a comparable minority of out-of-hospital arrests. [11]
The children in whom ventricular fibrillation turns up are predictable. They include the child with a primary cardiac cause — cardiomyopathy, myocarditis, a channelopathy such as long QT, post-operative congenital heart disease, and the Wolff-Parkinson-White pattern — and the child in whom a respiratory arrest has deteriorated into ventricular fibrillation late in the arrest. Resuscitation drugs, profound hypothermia, electrolyte disturbance, and tricyclic poisoning also produce shockable rhythms. [1] [6]
Supraventricular tachycardia, the commonest tachyarrhythmia of childhood, presents most often in infants under one year, who tolerate a rate of 250 poorly and can develop shock within hours. Wolff-Parkinson-White and concealed accessory pathways underlie many cases, and the small infant with a fast narrow-complex tachycardia and pallor is the classic scenario in which synchronised cardioversion is the answer when vagal manoeuvres and adenosine fail. [4] [12]
Pulseless VF or VT
Cardiac arrest, no pulse
- Unsynchronised shock at 4 J/kg
- Resume CPR immediately, no pulse check
- Up to 3 stacked shocks if the rhythm persists
- Amiodarone 5 milligrams per kilogram after the third shock if refractory
SVT with a pulse
Unstable, vagal/adenosine failed
- Synchronised shock at 1 J/kg
- Escalate to 2 J/kg if first shock fails
- SYNC must be ON or you risk VF
- Sedate if time permits but do not delay
Symptomatic bradycardia
Complete heart block, no response to adrenaline
- Transcutaneous pacing at 80 to 100/min
- Increase mA until electrical and mechanical capture
- Analgesia and sedation — pacing is painful
- Bridge to transvenous pacing
Infant under 1 year
AED available, no manual defibrillator
- Manual defibrillator preferred so 4 J/kg is deliverable
- AED acceptable if no manual machine
- Use paediatric attenuated pads if available
- Anteroposterior pads if chest too small
Pathophysiology
Ventricular fibrillation is a lethal re-entry phenomenon. Instead of a single organised wave of depolarisation flowing from the sinus node through the atria and ventricles, the myocardium hosts many small, disordered wavelets that circle and fragment, so that no coordinated contraction occurs. Cardiac output falls to zero within seconds. The only way to stop it is to depolarise the whole myocardium at once, blotting out every wavelet and giving the sinus node a silent, refractory heart it can recapture. That is what the defibrillation shock does. [1] [6]
The success of the shock depends on enough current reaching enough myocardium. Current is determined by the energy selected and by transthoracic impedance, the electrical resistance of the chest wall. Impedance is higher in children relative to their mass than the raw energy would suggest, which is one reason the dose is weight-based, and it falls with each successive shock. This is also why pads must be applied firmly with good gel coupling, why anterior chest hair is shaved if it interferes, and why the pads must not touch each other or arc across the chest of a small infant. [3] [7]
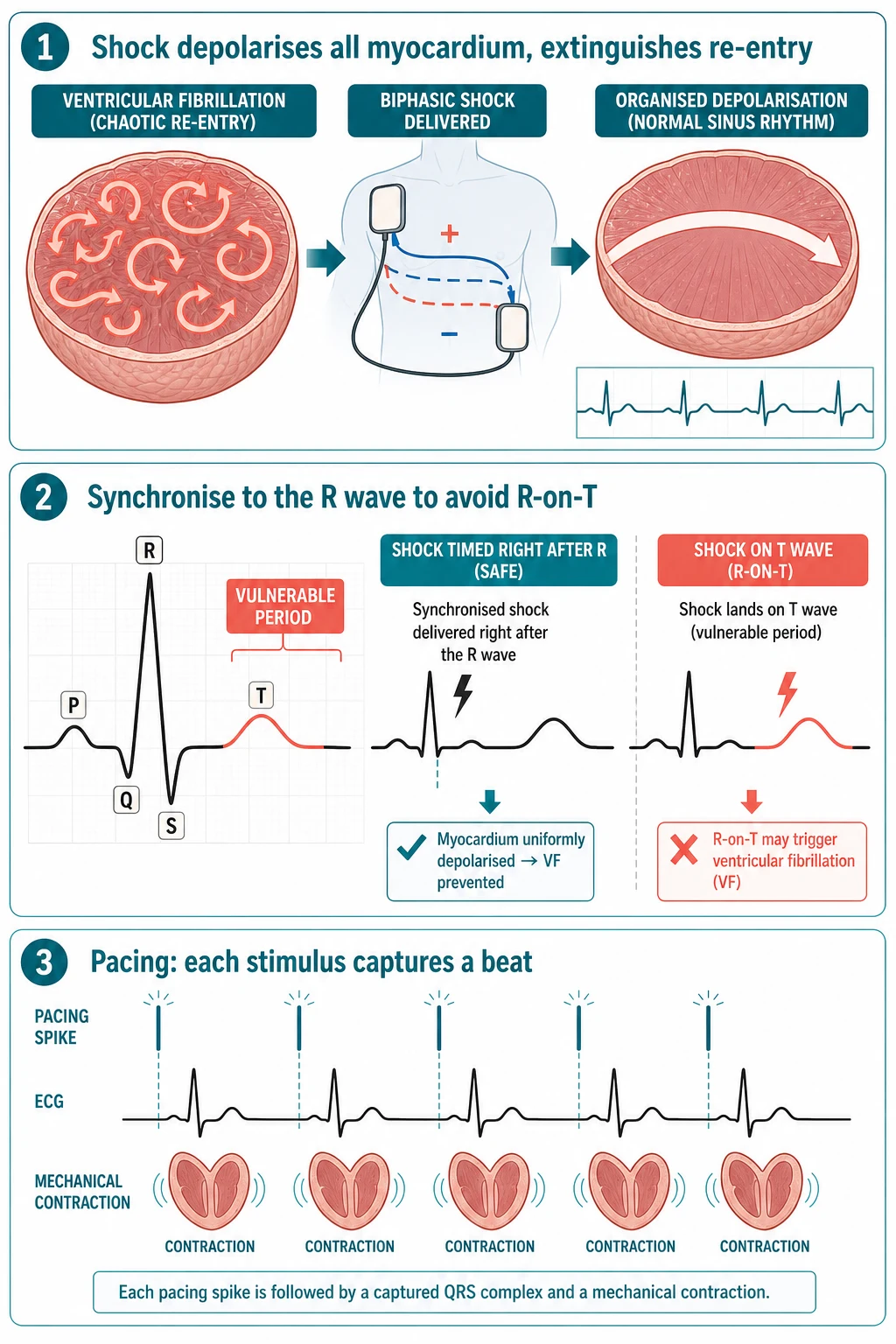
The reason synchronisation matters is the vulnerable period. The few milliseconds of the T wave, particularly its upstroke, are the interval in which a stray stimulus can fragment an organised rhythm into ventricular fibrillation — the so-called R-on-T phenomenon. A perfusing tachyarrhythmia has a recognisable R wave, so the defibrillator can be told to wait for it and discharge just afterwards, dodging the T wave. Ventricular fibrillation has no organised R wave, so synchronisation is impossible and the shock is delivered unsynchronised. [1] [6]
Transcutaneous pacing works on a different principle: a series of timed electrical pulses, each strong enough to depolarise the ventricular myocardium directly through the chest wall, takes over the role of the absent or blocked intrinsic pacemaker. The muscle contracts once per pulse, producing mechanical capture — a palpable pulse — as long as the myocardium is not profoundly ischaemic or hypoxic. This is why pacing works in conduction disease but fails in end-stage arrest with a dying myocardium. [5]
Clinical Presentation
The child who needs a shock or pacing pad never presents with a label; the team recognises the rhythm on the monitor and the clinical state of the child at the same moment. The presentations cluster around four rhythms, each with its own story. [1] [6]
The first is the collapsed, pulseless child with ventricular fibrillation or pulseless ventricular tachycardia on the monitor. The child is in cardiac arrest, cardiopulmonary resuscitation is in progress, and the rhythm strip shows either the chaotic, shapeless trace of fibrillation or the wide, regular complexes of pulseless tachycardia. The team must pause compressions for the shortest possible rhythm check, confirm the trace, charge, and shock. [1]
The second is the infant with supraventricular tachycardia and early shock — typically under one year, pale, irritable, tachypnoeic, refusing feeds, with a heart rate fixed at 220 to 250 and a narrow QRS. Vagal manoeuvres and adenosine may terminate it, but a child who is haemodynamically compromised — hypotensive, altered consciousness, cool peripheries — needs synchronised cardioversion without delay. [4] [12]
The third is the child with stable monomorphic ventricular tachycardia with a pulse — often a known cardiac patient, post-operative or with cardiomyopathy — who is wide-complex and fast but still perfusing. If unstable, synchronised cardioversion is the answer; if stable, an antiarrhythmic such as amiodarone is tried first. The fourth is the child with symptomatic bradycardia and complete heart block — congenital heart block in the infant of a mother with autoantibodies, or acquired block after cardiac surgery or from drug toxicity — whose rate fails to rise with adrenaline and who needs external pacing. [5] [6]
Differential Diagnosis
There is no differential diagnosis of the procedure itself — you deliver a shock or a pacing stimulus when the rhythm demands it. The differential the candidate must hold is which rhythm is on the monitor, because the choice between defibrillation, cardioversion, and pacing is made entirely on that reading. [1]
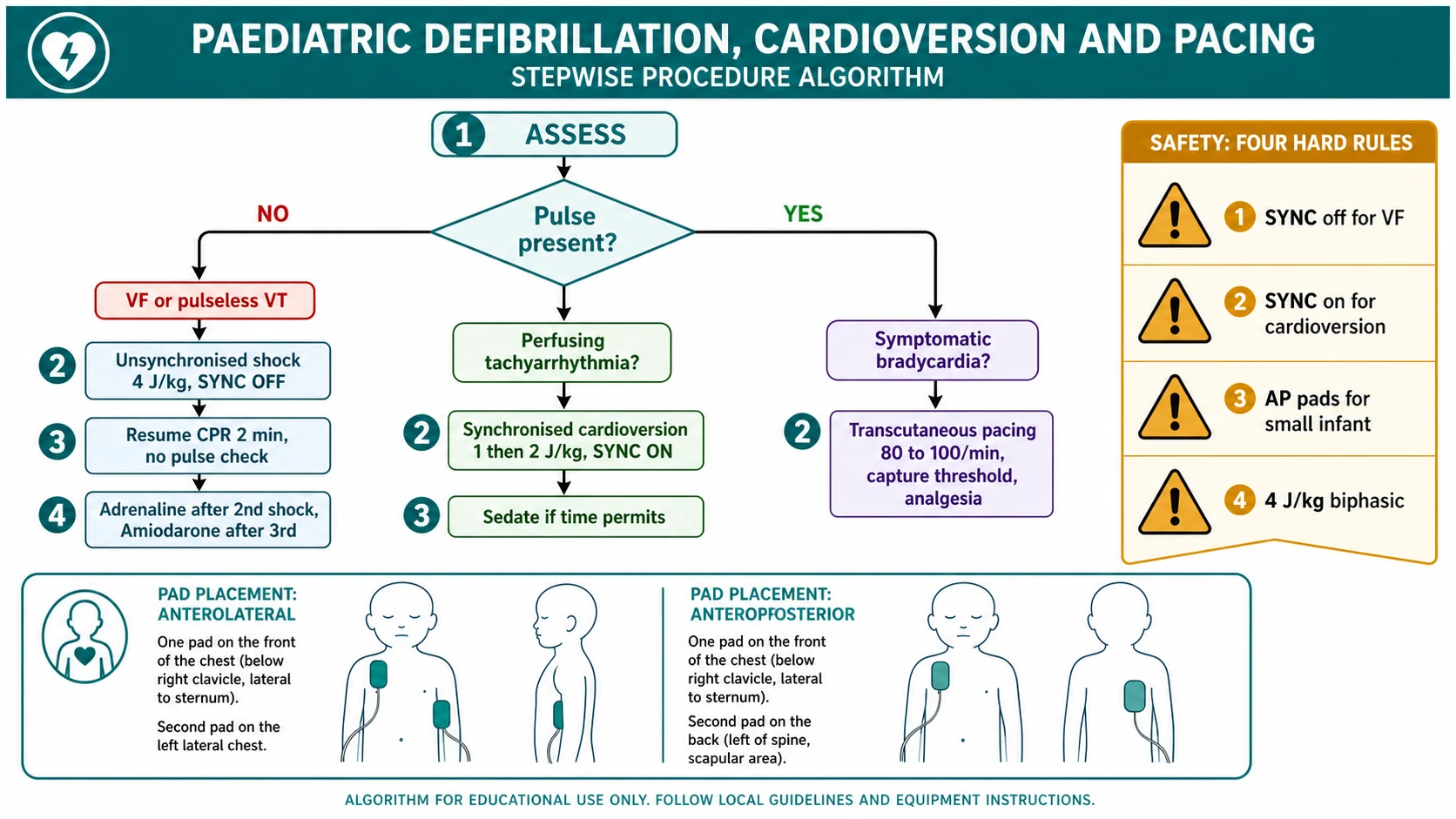
The first task is to decide whether the tachyarrhythmia is pulseless or perfusing. Ventricular fibrillation and pulseless ventricular tachycardia are pulseless and take defibrillation. Supraventricular tachycardia, atrial flutter, and ventricular tachycardia with a pulse are perfusing and take synchronised cardioversion if drugs have failed or the child is unstable. A pulse check during the rhythm pause settles it. [1] [6]
The second task is to decide whether a broad-complex tachycardia is supraventricular with aberrancy or genuinely ventricular. In the unstable child this does not delay treatment — a broad-complex tachycardia with haemodynamic compromise is treated as ventricular tachycardia and synchronised. In the stable child, a 12-lead electrocardiogram, the response to adenosine, and evidence of atrioventricular dissociation help separate the two. [4]
The third task, in the bradycardic child, is to decide whether the slow rate is reversible. Hypoxia is the commonest cause of paediatric bradycardia, and oxygenation and ventilation come before pacing. Hyperkalaemia, hypothermia, drug toxicity (beta-blocker, calcium-channel blocker, digoxin), and raised intracranial pressure all produce bradycardia with specific treatments, and each must be sought and corrected alongside the decision to pace. Pacing is reserved for bradycardia from intrinsic conduction failure — sinus node dysfunction or high-grade atrioventricular block — that has not responded to adrenaline. [5]
Clinical & Bedside Assessment
The bedside assessment turns on two things: reading the rhythm correctly and placing the pads correctly. Get both right and the shock will reach the myocardium at the dose you intend. [1]
Read the rhythm from a clean trace. Attach monitoring electrodes or pads, check the gain and the lead, and run a rhythm strip long enough to see the pattern. Confirm ventricular fibrillation (chaotic, no organised complexes) versus pulseless ventricular tachycardia (wide, regular, fast) versus a perfusing tachyarrhythmia (narrow or wide, regular, with a measurable blood pressure). Perform a pulse check during the brief pause in compressions. State the rhythm and the pulse status aloud so the whole team hears the decision. [1] [6]
Place the pads in one of two positions. The anterolateral position places one pad to the right of the sternum below the clavicle and the other on the left mid-axillary line at the level of the nipple, with the heart sandwiched between them. The anteroposterior position places one pad on the anterior chest to the left of the sternum and the other on the back between the scapulae. Both are effective; anteroposterior is preferred for small infants, for cardioversion of atrial arrhythmias, and when the anterolateral pads would touch each other on a tiny chest. Never place pads over the breast tissue of an adolescent, over an implanted pacemaker (move at least eight centimetres away and use anteroposterior), or over a transdermal medication patch. [2] [7]
Mode, dose, pads
Investigations
No investigation is required before delivering an emergency shock or starting external pacing — the decision is clinical and the treatment is immediate. The rhythm on the monitor and the presence or absence of a pulse are the only data needed to act. [1]
Once the acute event is controlled, a focused set of investigations explains why the rhythm occurred and shapes definitive care. Run a 12-lead electrocardiogram to define the arrhythmia, look for pre-excitation (a delta wave and short PR interval in Wolff-Parkinson-White), and measure the corrected QT interval. Send blood for potassium, magnesium, calcium, glucose, and a venous gas to exclude electrolyte disturbance and acidosis, and a troponin if myocarditis or ischaemia is suspected. An echocardiogram assesses structural and functional heart disease — cardiomyopathy, anomalous coronary origin, post-surgical status. In the child with recurrent or unexplained arrhythmia, inherited cardiac panels and cardiology referral follow. [4] [6]
For the paced child, the investigations serve the same purpose but with an added question: why has conduction failed? Congenital complete heart block in the neonate should prompt testing of maternal autoantibodies (anti-Ro and anti-La), and acquired block after cardiac surgery demands urgent cardiology review for surgical injury to the conduction tissue. [5]
Management — Resuscitation
The resuscitation rules for shockable arrest are short and worth memorising as an algorithm. When the rhythm is ventricular fibrillation or pulseless ventricular tachycardia, deliver one unsynchronised shock at 4 joules per kilogram and immediately resume cardiopulmonary resuscitation for two minutes without pausing for a pulse check. [1] [2]
After two minutes, reassess the rhythm. If ventricular fibrillation persists, deliver a second shock at 4 joules per kilogram and resume compressions. Give adrenaline 10 micrograms per kilogram after the second shock, and repeat it every three to five minutes. If a third shock is needed, give amiodarone 5 milligrams per kilogram (or lidocaine 1 milligram per kilogram if amiodarone is unavailable) immediately after the shock, followed by a flush. The American Heart Association guidance accepts an initial dose of 2 to 4 joules per kilogram, but the taught and widely practised standard, and the European Resuscitation Council figure, is 4 joules per kilogram from the first shock. [1] [3]
Defibrillation (ventricular fibrillation or pulseless ventricular tachycardia)
Dose
4 joules per kilogram (initial and subsequent doses)
For a perfusing tachyarrhythmia that has not responded to vagal manoeuvres and adenosine, or in which the child is haemodynamically unstable, deliver a synchronised shock at 1 joule per kilogram. If the rhythm persists, increase to 2 joules per kilogram. SYNC must be ON, and the team should press the sync button and watch the markers flash on each R wave before discharging. If the child is conscious and time permits, give sedation or anaesthesia, but never delay a shock in an unstable child to achieve it. [1] [4]
Management — Definitive & Stepwise
Once the decision is made, delivering the shock is an ordered sequence. Run through it the same way every time, on a simulator until it is automatic, and it will hold together in a real arrest. [1]
Delivering a defibrillation shock, in order
1 · Confirm
Confirm ventricular fibrillation or pulseless ventricular tachycardia on the monitor and the absence of a pulse. State the rhythm aloud.
2 · Select energy and mode
Select 4 joules per kilogram. Confirm SYNC is OFF. Biphasic waveform is standard.
3 · Place pads
Apply pads anterolateral or anteroposterior, firm and coupled with gel. Ensure pads do not touch and are clear of pacemakers and patches.
4 · Charge and clear
Charge the machine while compressions continue. Call 'stand clear', confirm no one is touching the child or the bed.
5 · Deliver
Press the shock button. The shock is delivered instantly as SYNC is off.
6 · Resume CPR
Resume chest compressions immediately without a pulse check. Continue for 2 minutes, then reassess the rhythm and repeat or move to the next algorithm step.
A few technique points separate a clean shock from a failed or dangerous one. Charge while compressions continue to minimise the pause; the pre-charge can be done by the person at the chest without breaking contact. Confirm SYNC is off before every defibrillation, because a leftover SYNC setting from a previous cardioversion will stop the machine firing. Call stand clear and look before pressing the button — oxygen should be moved away from the chest, and no team member should be touching the child. After the shock, do not pause for a pulse check; resume compressions at once and reassess after two minutes. [1] [7]
For transcutaneous pacing, the sequence differs. Place the pacing pads anteroposterior. Set the rate to 80 to 100 per minute. Start the output at zero and increase the milliamperes until each pacing spike is followed by a broad captured QRS — electrical capture — and a palpable pulse confirms mechanical capture. The current needed is the capture threshold; add a small margin above it. Give a conscious child analgesia and sedation, because each pacing stimulus is painful. Plan transvenous pacing as soon as the child is stable enough, because transcutaneous pacing is uncomfortable, unreliable over hours, and only a bridge. [5]
| Rhythm | Pulse | Mode | Energy or setting |
|---|---|---|---|
| Ventricular fibrillation | None | Unsynchronised (defibrillation) | 4 J/kg, repeat as needed |
| Pulseless ventricular tachycardia | None | Unsynchronised (defibrillation) | 4 J/kg, repeat as needed |
| Supraventricular tachycardia | Present, unstable | Synchronised (cardioversion) | 1 J/kg, then 2 J/kg |
| Stable monomorphic VT | Present | Synchronised (cardioversion) if drugs fail | 1 J/kg, then 2 J/kg |
| Sinus bradycardia or heart block | Present, symptomatic | Transcutaneous pacing | Rate 80 to 100/min, capture threshold mA |
[1] [5] The 4 J per kg dose is the biphasic standard taught by APLS and the European Resuscitation Council; the American Heart Association accepts an initial range of 2 to 4 J per kg.
Specific Subtypes & Scenarios
Four scenarios recur in fellowship vivas and resuscitation assessments, and each carries a specific trap. The first is the infant under one year and the automated external defibrillator. A manual defibrillator is preferred in infants because it allows the exact 4 joules per kilogram dose, but an automated external defibrillator is acceptable when a manual machine is not available. Attenuated paediatric pads, which reduce the delivered energy, should be used for children under eight years; if only adult pads are available, they are used rather than withholding the shock. [8] [10]
The second is the small chest and the touching pads. On a tiny infant, two standard adult pads placed anterolaterally can meet or overlap, and the current arcs between them rather than crossing the heart. The fix is anteroposterior placement, which separates the pads on opposite sides of the chest and guarantees a transcardiac vector. This is the taught default for the smallest infants and for atrial arrhythmias. [2] [7]
The third is the child with an implanted pacemaker or defibrillator. Place the pads at least eight centimetres away from the device, use the anteroposterior position, and after the arrest, check the device function, because a shock can reset or damage the generator. The fourth is the channelopathy and the recurrent shockable rhythm — long QT, Brugada, catecholaminergic polymorphic ventricular tachycardia — where the child may need multiple shocks, magnesium for torsades, beta-blockade, and urgent electrophysiology referral. [4] [6]
The scenario the examiner most often builds is the infant with supraventricular tachycardia. The path is vagal manoeuvres, then adenosine 0.1 milligram per kilogram (maximum 6 milligrams) by rapid bolus followed by a flush, repeated at 0.2 milligram per kilogram (maximum 12 milligrams) if the first dose fails. If the child is shocked or adenosine is ineffective or unsafe (asthma, severe heart failure), synchronised cardioversion at 1 joule per kilogram is the next step. The candidate who can walk this path and name the doses will answer any SVT question. [1] [12]
Complications & Pitfalls
Complications are uncommon when the shock is delivered correctly, but the candidate must be able to name and prevent each one, because two — the wrong mode and the failed capture — are directly under the operator's control. [1] [6]
The commonest dangerous pitfall is a mode error. Delivering a perfusing tachyarrhythmia without SYNC risks an R-on-T shock that converts supraventricular tachycardia into ventricular fibrillation, and delivering ventricular fibrillation with SYNC left on means the machine never fires at all. The safeguard is to call the mode aloud — "SYNC on for cardioversion, SYNC off for defibrillation" — and to watch the sync markers flash on the R wave before a cardioversion. [1]
Skin burns at the pad sites are common and usually trivial, caused by poor pad coupling or arcing between pads that touch. Prevent them with firm application, adequate gel, correct pad size, and anteroposterior placement in the small infant. Myocardial injury, reflected in a troponin rise and transient ST changes, can follow high or repeated shocks but is rarely clinically significant in isolation. Omitted or delayed resuscitation drugs — forgetting adrenaline after the second shock or amiodarone after the third — is a systems error prevented by the structured algorithm. [1] [3]
For pacing, the two pitfalls are failure to capture and failure to recognise it. Failure to capture means the pacing spike is not followed by a QRS or a pulse, usually because the output is too low, the pads are poorly coupled, or the myocardium is profoundly hypoxic or ischaemic. Increase the output, reposition the pads, correct hypoxia and acidosis, and move to transvenous pacing early. The second pitfall is treating the monitor rather than the child: electrical capture without a pulse is not enough, and a pulse must be confirmed. [5]
Prognosis & Disposition
The outcome of a shockable cardiac arrest in a child is determined by the underlying cause and the speed of the resuscitation, not by the shock alone. Witnessed in-hospital ventricular fibrillation, with an early shock and good bystander cardiopulmonary resuscitation, carries a markedly better survival than out-of-hospital arrest, and children who arrest in a monitored bed do better than those who arrest unwitnessed. The shock buys the chance of a perfusing rhythm; the rest of the resuscitation and the definitive care of the cause decide survival. [1] [11]
After return of spontaneous circulation, the child is managed in a paediatric intensive care unit with targeted temperature management where indicated, careful ventilation to normocapnia, haemodynamic support, and the search for and treatment of the underlying arrhythmogenic cause. Every child who has been defibrillated or paced needs urgent cardiology involvement — for an electrocardiogram, echocardiography, inherited cardiac screening, and a plan for definitive rhythm control, which may include antiarrhythmic drugs, catheter ablation of an accessory pathway, or an implantable cardioverter defibrillator. [4] [6]
For the paced child, transcutaneous pacing is transitioned to transvenous pacing as soon as feasible, and the conduction disease is investigated and treated definitively — which may mean a permanent pacemaker for congenital or postsurgical complete heart block. Disposition from the emergency department or ward is always to a monitored bed with continuous electrocardiography and a clear escalation plan. [5]
Special Populations
The infant under one year deserves a separate line. The chest is small, the energy must be weight-based, and the pads may need to sit anteroposterior. A manual defibrillator is preferred so that 4 joules per kilogram can be delivered exactly, but an automated external defibrillator with paediatric pads is acceptable when no manual machine is available, and the data on automated rhythm analysis in infants support its use when it is the only option. [8] [10]
The child with congenital or acquired heart disease is the group most likely to meet a shockable rhythm. Post-operative cardiac patients, children with cardiomyopathy, myocarditis, and inherited channelopathies, and those with implanted devices all need a team that anticipates arrhythmia and has the pads, the energy doses, and the escalation plan ready. Know where the child's device sits, place pads away from it, and involve cardiology early. [4] [6]
The child with a tricyclic antidepressant or sodium-channel-blocker overdose can present with a broad-complex tachycardia that degenerates into ventricular fibrillation, and the treatment is sodium bicarbonate to narrow the QRS alongside resuscitation. The child in the magnetic resonance imaging scanner presents a specific hazard, because ferromagnetic defibrillator components and the scanner's radiofrequency field interact; MRI-conditional equipment and a clear extraction plan to a safe resuscitation area are required. [1]
For Aboriginal, Torres Strait Islander, Māori, and migrant and refugee children, and for children living in poverty or in remote communities, the arrhythmia may present late and the nearest defibrillator may be an automated external device in a rural clinic. Training rural and retrieval clinicians, and families of high-risk children, in automated external defibrillator use, and ensuring that paediatric attenuated pads are stocked in remote settings, is an equity issue as much as a clinical one. [8] [11]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions. The American Heart Association Pediatric Advanced Life Support guidance, the European Resuscitation Council Paediatric Life Support guidelines, and the Advanced Paediatric Life Support course used across Australia and New Zealand all agree on the core: defibrillate ventricular fibrillation and pulseless ventricular tachycardia early, use a weight-based dose, and resume compressions immediately. The remaining debates are narrow and sit on the dose. [1] [2]
The energy dose is the principal transatlantic difference. The European Resuscitation Council and APLS teach 4 joules per kilogram from the first shock. The American Heart Association accepts an initial dose of 2 to 4 joules per kilogram and allows escalation to higher doses (up to 10 joules per kilogram, not exceeding the adult dose) for refractory rhythms. A systematic review of human and animal evidence found no convincing survival difference between dose strategies, which is why the guidance permits a range while the taught standard in Australasia and Europe is 4 joules per kilogram. [1] [3]
[1] [2]The evidence on pad position has matured. A 2024 JAMA Network Open study of out-of-hospital shockable arrest found no clear survival difference between anterolateral and anteroposterior positions in adults, supporting the pragmatic approach of using whichever position is achievable, with anteroposterior preferred for the small infant and for atrial arrhythmias. The automated external defibrillator in children evidence, built over two decades, confirms that attenuated paediatric pads deliver an appropriate lower energy to the under-eight-year-old and that automated rhythm analysis is reliable in children and acceptable in infants when no manual machine exists. [7] [8]
The genuine controversies are narrow. Whether to stack shocks or deliver single shocks with cycles of cardiopulmonary resuscitation between them has settled toward the single-shock strategy with two-minute cycles of compressions. Whether amiodarone or lidocaine is preferred after the third refractory shock remains open; both are acceptable, and amiodarone is the commoner choice. The role of double sequential defibrillation in children is unproven and not part of standard paediatric guidance. [1] [3]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [1] [2]
The single distinction is the pulse: pulseless ventricular fibrillation or pulseless ventricular tachycardia takes unsynchronised defibrillation at 4 joules per kilogram; a perfusing tachyarrhythmia takes synchronised cardioversion at 1 joule per kilogram, escalating to 2 joules per kilogram. State it first, and name the sync function, and you have the spine of the topic. [1]
The mode errors are the highest-yield traps. SYNC off for ventricular fibrillation (or the machine never fires); SYNC on for a perfusing tachyarrhythmia (or an R-on-T shock provokes ventricular fibrillation). For pacing, set the rate at 80 to 100 per minute, increase the output until you see electrical capture (a QRS after each spike) and mechanical capture (a palpable pulse), and give analgesia. [1] [5]
The pad positions are anterolateral or anteroposterior; use anteroposterior for the small infant, for atrial arrhythmias, and when anterolateral pads would touch. Resume compressions immediately after a defibrillation shock without a pulse check, reassess after two minutes, and give adrenaline 10 micrograms per kilogram after the second shock and amiodarone 5 milligrams per kilogram after the third. For the infant, a manual defibrillator is preferred but an automated external defibrillator with attenuated paediatric pads is acceptable. [1] [8]
References
- [1]Topjian AA, Raymond TT, Atkins D, et al Part 4: Pediatric Basic and Advanced Life Support 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Pediatrics, 2021.PMID 33087552
- [2]Van de Voorde P, Turner NM, Djakow J, et al European Resuscitation Council Guidelines 2021: Paediatric Life Support Resuscitation, 2021.PMID 33773830
- [3]Mercier E, Laroche E, Beck B, et al Defibrillation energy dose during pediatric cardiac arrest: Systematic review of human and animal model studies Resuscitation, 2019.PMID 31029714
- [4]Brugada J, Blom N, Sarquella-Brugada G, et al Pharmacological and non-pharmacological therapy for arrhythmias in the pediatric population: EHRA and AEPC-Arrhythmia Working Group joint consensus statement Europace, 2013.PMID 23851511
- [5]Neubrand TL, Topoz I, Mistry RD Updated Approaches to Cardiac Electrical Stimulation and Pacing in Pediatrics Pediatric Emergency Care, 2020.PMID 32868549
- [6]Samson RA, Atkins DL Tachyarrhythmias and defibrillation Pediatric Clinics of North America, 2008.PMID 18675025
- [7]Lupton JR, Newgard CD, Dennis D, et al Initial Defibrillator Pad Position and Outcomes for Shockable Out-of-Hospital Cardiac Arrest JAMA Network Open, 2024.PMID 39250154
- [8]Atkins DL, Jorgenson DB Attenuated pediatric electrode pads for automated external defibrillator use in children Resuscitation, 2005.PMID 15993727
- [9]Berg RA Attenuated adult biphasic shocks for prolonged pediatric ventricular fibrillation: support for pediatric automated defibrillators Critical Care Medicine, 2004.PMID 15508658
- [10]Atkinson E, Mikysa B, Conway JA, et al Specificity and sensitivity of automated external defibrillator rhythm analysis in infants and children Annals of Emergency Medicine, 2003.PMID 12883506
- [11]Morgan RW, Kirschen MP, Kilbaugh TJ, et al Pediatric In-Hospital Cardiac Arrest and Cardiopulmonary Resuscitation in the United States: A Review JAMA Pediatrics, 2021.PMID 33226408
- [12]Abbasi E, Vijayashankar SS, Goldman RD Management of acute supraventricular tachycardia in children Canadian Family Physician, 2023.PMID 38092445