Paeds · mental-behavioural-and-psychosomatic
Mental state examination in children and adolescents
Also known as Paediatric mental state examination · Child and adolescent MSE · Mental status examination · Psychiatric assessment of the child · Observation-based mental state assessment
A fellowship approach to performing and documenting a mental state examination on a child or adolescent: setting the conditions, observing each of the seven domains, adapting the method to preschool, school-age and adolescent patients, integrating validated brief screens, weighing findings against the developmental norm and against medical mimics, and acting on suicide and safety risk in the room.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 14-year-old sits in your clinic while a parent describes a year of declining marks, withdrawn behaviour, and a recent episode of self-harm. The parent has given you the history. What you do not yet have is a structured picture of how this young person's mind is working right now, today, in front of you. The mental state examination is the tool that produces that picture. [9] [8]
The MSE is a cross-sectional assessment. It records mental functioning at the moment of the encounter, which is why it complements but never replaces the longitudinal psychiatric history. The history tells you the story over time; the mental state examination tells you what is present now. A young person can describe years of low mood (history) while appearing bright and reactive in your room (current mental state), and both observations matter. [9]
Two ideas make the paediatric MSE different from the adult version, and both matter at every step. First, you must observe before you interview, because young children often cannot or will not report their inner state in words. Second, you must match the method to the developmental stage: a preschooler is assessed through play and behaviour, an adolescent through a private conversation. Apply an adult MSE unchanged to a five-year-old and you will record almost nothing of value. [10]
The reason this skill sits in general paediatrics, not only in child psychiatry, is simple. Mental disorder is common, help is scarce, and most young people who need mental-health care never reach a specialist. The general paediatrician who can perform and interpret a reliable MSE is the narrowing point of that gap. A well-conducted examination can recognise a depressive or anxious state, weigh it against a medical mimic, assess the risk of suicide, and decide the disposition — all in the same visit. [5] [9]
Classification
The MSE is recorded through seven domains, each capturing a different window on mental functioning. They are walked in a consistent order so that none is missed and so a colleague reading your note can follow. The order is appearance and behaviour, speech, mood and affect, thought (form and content), perception, cognition, and insight and judgment. [9]
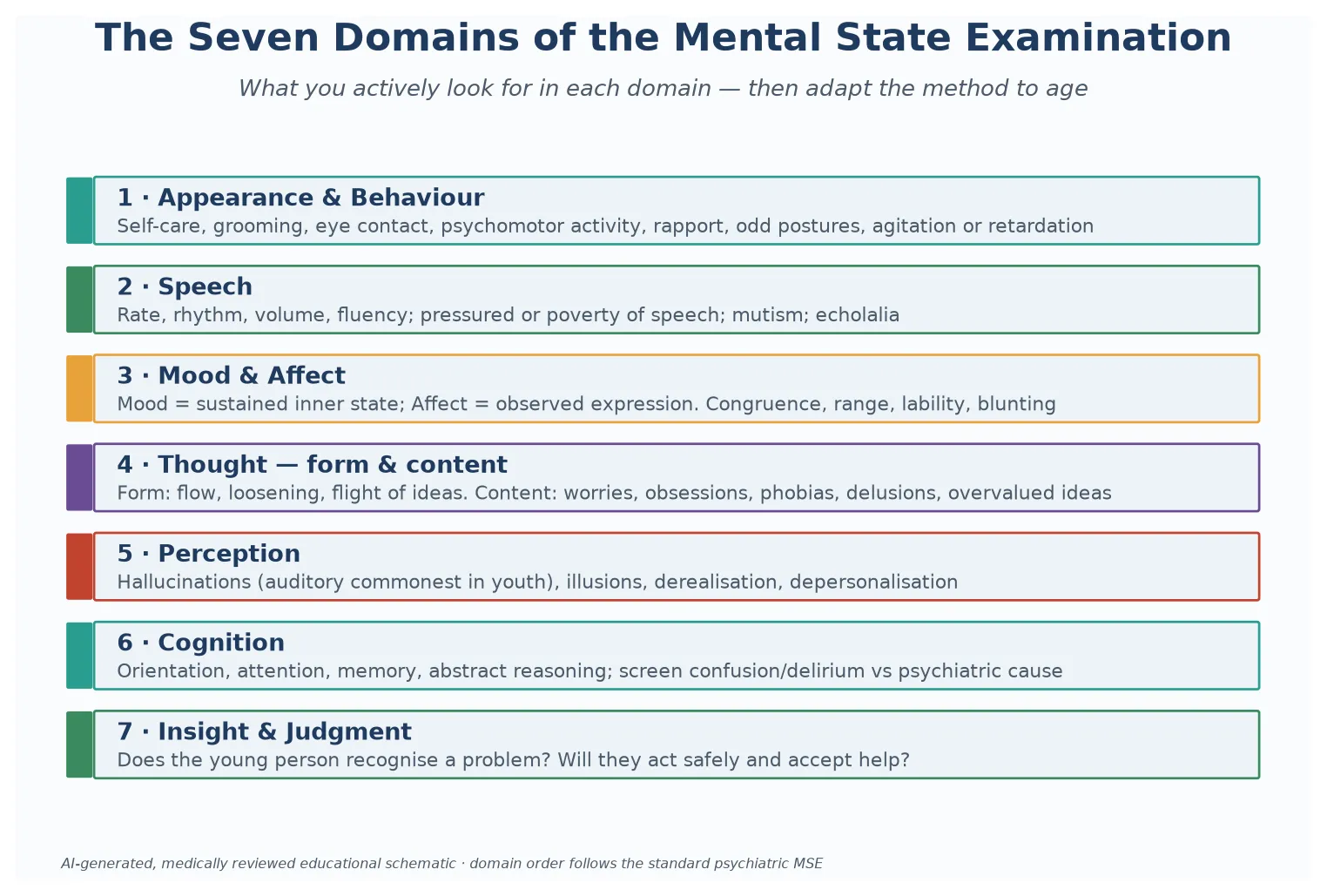
Read the figure like this: each domain is a separate window on the same mind. A young person can look well in one domain and unwell in another, which is why you cannot substitute a single impression for the full set. [9]
Appearance & behaviour
Observe first
- Self-care, grooming, eye contact
- Psychomotor activity: agitated or slowed
- Rapport, cooperation, odd postures
- Read from the moment they enter
Speech & mood
Listen
- Rate, rhythm, volume, fluency
- Mood = sustained inner state (subjective)
- Affect = observed expression (objective)
- Congruence, range, lability, blunting
Thought & perception
Probe gently
- Form: flow, flight of ideas, loosening
- Content: worries, obsessions, delusions
- Perception: hallucinations, illusions
- Auditory hallucinations commonest in youth
Cognition & insight
Weigh
- Orientation, attention, memory
- Always screen delirium vs psychiatric
- Insight: do they recognise a problem?
- Judgment: will they act safely?
A useful working distinction runs through the domains: some you observe (appearance, behaviour, affect, speech), others you elicit (mood, thought content, perception, insight). For a young child, the observed domains carry most of the weight, because elicited answers may be unreliable. For an adolescent, the elicited domains come into their own once rapport and privacy are established. [10]
The MSE is also distinct from three neighbours it is often confused with. It is not a developmental assessment, which measures milestones against age norms. It is not a cognitive or IQ assessment, which quantifies intellect with standardised tests. And it is not a structured diagnostic interview, which maps symptoms onto diagnostic criteria. The MSE is the bedside, cross-sectional observation that feeds all three. [9]
Epidemiology & Risk Factors
Roughly one in eight children and adolescents meets criteria for a mental disorder at any time. The leading contributors to illness and death in adolescence — suicide, injury, and the consequences of risk behaviour — are behaviour-driven and mental-health-linked. This is why a reliable MSE is a core general-paediatric skill, not a sub-specialty task held in reserve for the child psychiatrist. [5] [8]
The young people most likely to need a careful MSE are not evenly distributed. Rates of mental-ill health run higher in adolescents, in those with chronic illness or disability and neurodiversity, in young people in out-of-home care and youth justice, and in refugee and migrant families. Recognising these groups lets you make the MSE opportunistic — built into a diabetes review, a foster-care health check, or an emergency attendance. [9]
Who is missed
- Adolescents screened for a medical complaint only
- Children with disability assumed 'always like this'
- Somatic complaints taken at face value
- Boys and younger children under-screened
High-risk groups
- Chronic illness and neurodiversity
- Out-of-home care, youth justice
- Refugee, migrant and Indigenous youth
- Family violence and adverse childhood experiences
Hidden doorways
- Recurrent somatic complaints
- School refusal or declining marks
- Behavioural change and family conflict
- Repeated emergency attendance
System gaps
- No time alone built into the visit
- Few local CAMHS pathways
- Portal and billing confidentiality risks
- No interpreter or cultural broker
Suicide is among the leading causes of adolescent death in high-income countries, and this single fact sets a floor on what every adolescent MSE must contain. Any mood-related finding obliges a direct, same-visit enquiry about suicidal ideation, plan, intent, and access to means. A mental state examination that records "low mood" and stops there is incomplete and, in the worst case, dangerous. [8] [5]
Adverse childhood experiences and ongoing family violence raise both the prevalence of mental disorder and the difficulty of detecting it. They alter trust, affect, and the way a young person presents to authority, so the highest-risk young person may also be the hardest to engage. A steady, non-judgemental, predictable approach is the precondition for a reliable examination in this group. [9]
Pathophysiology
Two forces of normal development shape the paediatric MSE, and both push the same way: toward presentations that differ from the adult and toward methods that must change with age. [10]
The first force is brain maturation. In adolescence the reward and affect systems mature before the prefrontal systems that govern impulse control. This biological gap shows up at the bedside as sensation-seeking, stronger emotional reactivity, and decisions that an adult would not make. It is also why a calm, non-judgemental interview style works and a lecture does not — you are meeting a brain wired to feel the pull before it can apply the brakes. [10]
The second force is the developmental march of cognition and language. A preschooler cannot reliably report an inner state in words, so the examination rests on behaviour, play, and what you observe. A school-age child thinks concretely and can answer structured questions, given the right language. An adolescent can reason abstractly, hold insight, and describe internal experience — but only once they trust you and are private enough to speak. [10]
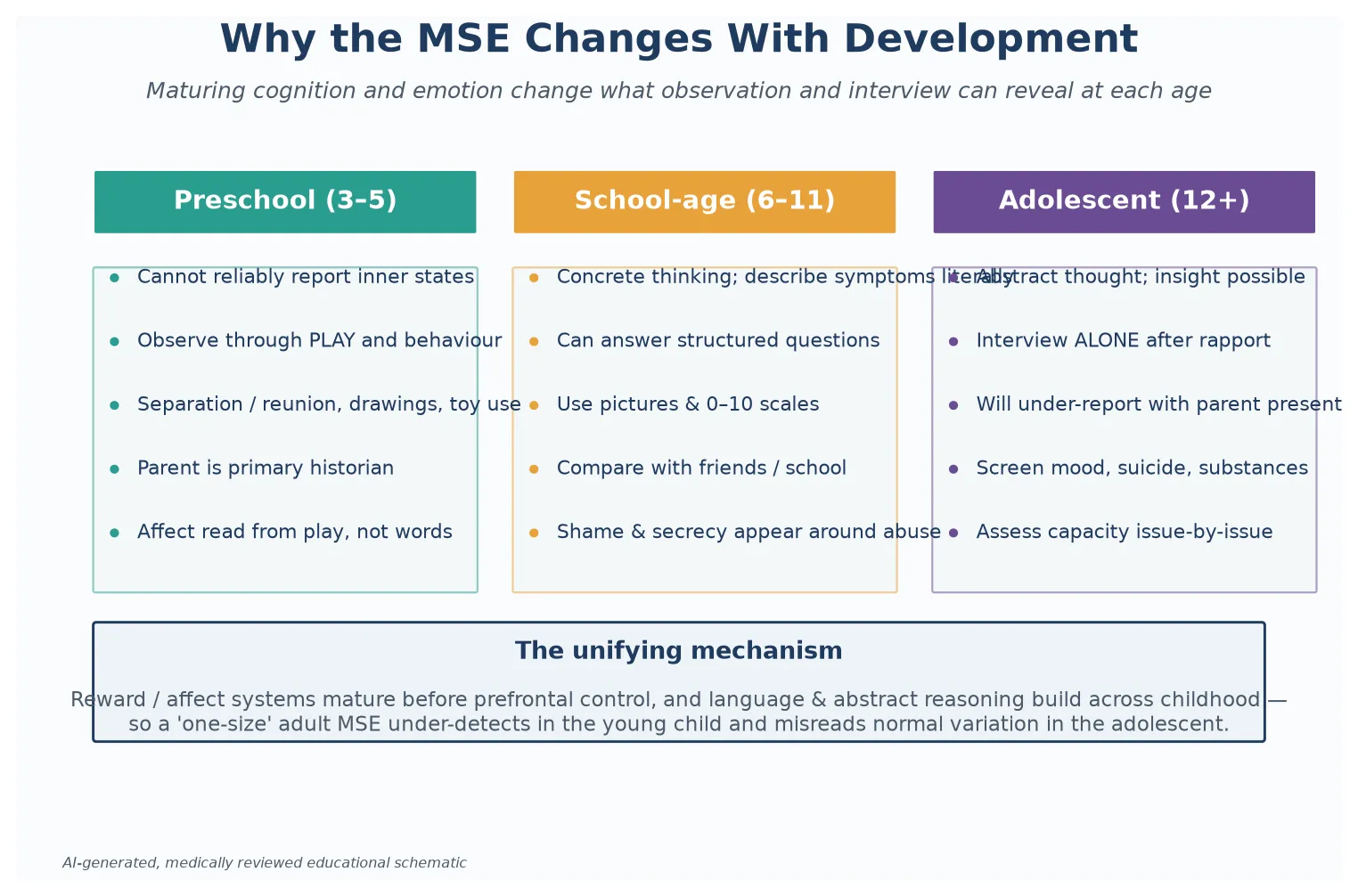
Read the figure like this: the method is not a preference, it is a consequence of development. The same seven domains are examined at every age, but the route into them shifts from play to conversation. [10]
Acute medical states distort the examination in a way you must always weigh. Delirium, intoxication, metabolic disturbance, infection, or a neurological event can each produce agitation, altered affect, disorientation, or apparently disorganised thought. The rule that protects you is simple: an acute change in cognition, especially with fluctuating consciousness, is delirium or an organic cause until proven otherwise. [9]
Ongoing stress and trauma change the picture further. They alter the trust, affect, and arousal a young person brings to the room, so a traumatised child may appear withdrawn, hypervigilant, or uncooperative for reasons that are not primarily psychiatric. A heavy-handed approach closes the door; a steady, trauma-informed frame is what reopens it. [9]
Clinical Presentation
A normal, developmentally appropriate presentation is the baseline against which every abnormality is read, and examiners test this deliberately. A preschooler's brief imaginary companion, an adolescent's mood swings, and a school-age child's situational tears are all normal if they do not impair function. The MSE finds disorder by measuring deviation from the right baseline, not from an adult norm. [9]
A depressive mental state in an adolescent shows psychomotor slowing, a sad or blunted affect, poverty of speech, and hopelessness. In a younger child the same illness often wears a different face — irritability, somatic complaints, and behavioural change rather than verbal sadness. Read the domain against the age, or you will miss it. [9] [2]
An anxious presentation shows restlessness, trembling, avoidance, and a fearful or strained affect. Speech may be impoverished not because thought is disordered, but because worry crowds it out. The affect is the clue, and it often brightens when the source of fear is removed or named. [3]
A psychotic process shows thought disorder, a young person responding to unseen stimuli, a blunted or incongruous affect, or a fixed false belief held against evidence. An important caveat follows the perception domain: isolated perceptual experiences, especially auditory, are common in childhood and usually transient and non-pathological. What raises concern is persistence, complexity, distress, and association with declining function. [11]
Looks like depression
- Slowing, sad or blunted affect
- Poverty of speech, hopelessness
- Irritability and somatic complaints in children
- Screen with PHQ-A; assess suicide risk
Looks like anxiety
- Restlessness, avoidance, fearful affect
- Speech crowded out by worry
- Brightens when the fear is named
- Screen with GAD-7
Looks like psychosis
- Responding to unseen stimuli
- Thought disorder, incongruous affect
- Fixed false belief against evidence
- Isolated perceptual experiences often transient
Looks like delirium
- Fluctuating consciousness
- Disorientation, attentional failure
- Acute onset — organic until proven
- Exclude infection, metabolic, neurological cause
An acute medical or delirious state shows fluctuating consciousness, disorientation, and attentional failure, and it must be distinguished from a primary psychiatric presentation before any psychiatric label is applied. The safest habit is to treat any acute cognitive change as organic until you have excluded a physical cause. [9]
Acute suicide risk has its own behavioural and affective signature, and a trap hides inside it. A young person at high risk can look deceptively calm once they have decided on a plan, because the agonising indecision has resolved. A calm presentation after a period of distress is therefore a reason to enquire more, not less. [8]
When the child is neurodivergent or has an intellectual disability, the baseline is different, and the only way to read it safely is against what is normal for that child, informed by a carer. A flat affect or avoiding eye contact may be the child's usual state, not a new finding — and a change from that baseline is what matters. [9]
Differential Diagnosis
When the MSE shows something concerning, your first job is to decide whether it is normal for age and context, or a problem that needs action. The MSE does not by itself diagnose; it raises findings that you then interpret against development, context, and the medical differential. [9]
Separate normal developmental variation from disorder. Mood swings in a teenager, an imaginary companion in a young child, and situational distress after a loss are all common. The discriminator is persistence, pervasiveness, and functional impairment — does it last, does it cross settings, and does it stop the young person doing what they usually do. [9]
The most important differential in any acutely disturbed presentation is organic versus psychiatric. Agitation, altered affect, or disorganised thought can be produced by delirium, intoxication, metabolic disturbance, infection, or a neurological event. An acute onset with fluctuating consciousness points to an organic cause, and you exclude it before attributing the picture to a primary psychiatric disorder. [9]
Normal variant
Watch + revisit
- Mood swings without impairment
- Imaginary companion in a young child
- Situational distress after a loss
- Single, transient perceptual experience
Likely disorder
Screen + assess
- Persistent, pervasive low mood
- Hazardous or recurrent substance use
- Disordered eating behaviours
- Declining function across settings
Organic mimic
Exclude first
- Acute cognitive change
- Fluctuating consciousness
- Metabolic or infectious cause
- Intoxication or neurological event
Urgent / safety
Act now
- Suicidal intent or plan
- Acute psychosis
- Disclosure of abuse
- Medical instability
Separate an anxious or traumatised child from one with an underlying neurodevelopmental condition such as autism or ADHD. The two can look similar — avoidance, social difficulty, restlessness — but they need different frameworks and different help. Collateral from parents and teachers, and the developmental history, are what tell them apart, which is why the MSE is never the whole assessment. [9]
In the perception domain, distinguish transient perceptual experiences from an emerging psychotic disorder. Brief, simple, non-distressing experiences are common in childhood and usually resolve. Persistence, complexity (such as beliefs about the experiences), associated distress, and declining function are the features that raise concern and warrant specialist assessment. [11]
A single MSE is a snapshot, and several conditions fluctuate. A young person who looks well in your room may be profoundly unwell at home or at school. When the history or collateral suggests fluctuation, repeat the examination, and weigh the worst point rather than only the moment in front of you. [9]
Clinical & Bedside Assessment
This is the heart of the topic. The MSE is a skill you perform, not a list you memorise, and the conditions you set decide what you will find. [9]
Begin observing before you speak. Watch from the moment the young person enters the room — their gait, how they separate from their parent, whether they make eye contact, how they take a seat, and what they do with their hands. Much of the appearance and behaviour domain is captured in these first seconds, before any question shapes the encounter. [9]
Set the conditions. Use a quiet space, free of interruption. Build rapport before you approach sensitive ground. For an adolescent, create time alone as a normal part of the visit and state your confidentiality line up front, because a parent's presence suppresses disclosure of mood, self-harm, substances, and abuse. For a younger child, let the parent stay close and use play to build trust. [10]
Walk the seven domains in order. For appearance and behaviour, record self-care, grooming, eye contact, psychomotor activity, and rapport. For speech, note rate, rhythm, volume, and fluency. For mood and affect, ask how the young person's mood has been (the subjective, sustained state) and describe what you observe in their expression (the moment-to-moment affect), noting whether the two are congruent. [9]
For thought, separate form from content. Form is the flow and logic of thinking — is it slowed, racing, or loosely connected. Content is what is thought about — worries, obsessions, phobias, or delusional beliefs. For perception, ask gently about hallucinations and other perceptual disturbances; remember that isolated experiences in children are common and usually benign. [9] [11]
For cognition, screen orientation, attention, and memory, and treat any acute impairment as a possible organic cause. For insight and judgment, ask whether the young person recognises there is a problem and whether they will act safely and accept help. Insight and judgment become meaningfully assessable as abstract reasoning develops, so they carry more weight in the adolescent. [9]
The seven domains in order
Adapt for the preschool child. Use play, drawings, and structured toys, and read behaviour and affect from what the child does rather than what they say. Observe separation and reunion with the parent, the quality of play, and the child's response to a simple request. The parent is the primary historian, but the child's behaviour is your evidence. [10]
Adapt for the school-age child. Use concrete language, pictures, and simple 0-to-10 scales for mood and pain. Children at this age can describe symptoms literally once they trust you, but they may hide what shames them, so approach abuse and self-harm with gentleness and a clear reason for asking. [10]
Adapt for the adolescent. Secure time alone, state the confidentiality line, then use open, non-judgemental questions and the brief validated screens described below. Ask directly about mood, self-harm, and suicidal ideation — direct questions reduce risk, they do not increase it. [8] [5]
Record the examination descriptively, writing what you saw and heard rather than the label you suspect. "Avoids eye contact, speech sparse, flat affect, describes a voice commenting on her actions" is useful to a colleague; "psychotic" alone is not. Keep the descriptive MSE and the interpretive formulation as separate things. [9]
Investigations
The "investigations" of the MSE are the validated brief screens and the targeted medical tests that follow the history, not a blanket panel. A screen is a prompt for deeper assessment, never a diagnosis. [9]
The Strengths and Difficulties Questionnaire (SDQ) is a brief behavioural screen for children and adolescents covering emotional, conduct, hyperactivity, peer-relationship, and prosocial domains. It can be completed by a parent, a teacher, and (from about eleven years) the young person, and the value of multi-informant data is that the same child can look different across settings. [1]
For depression, the PHQ-9 (and its adolescent version, the PHQ-A) is a brief self-report measure of depression severity. The US Preventive Services Task Force recommends screening adolescents aged 12 to 18 years for depression, which is why a mood screen belongs inside the adolescent MSE. A positive result prompts a clinical assessment, including a suicide-risk assessment, not an automatic label. [2] [5]
For anxiety, the GAD-7 is a brief self-report measure of anxiety severity that performs well as a screen in adolescents. Use it as a prompt, then interpret it with the young person against the findings of the examination. [3]
SDQ
Broad behavioural
- Parent, teacher and self-report
- Emotional, conduct, hyperactivity, peer, prosocial
- Multi-informant across settings
- A screen, not a diagnosis
PHQ-A / PHQ-9
Mood
- Brief depression severity self-report
- USPSTF: screen 12–18 yr (grade B)
- Positive result prompts assessment
- Always pair with suicide-risk assessment
GAD-7
Anxiety
- Brief anxiety severity self-report
- Validated in adolescents
- A prompt for clinical assessment
- Interpret with the examination
C-SSRS / ASQ
Suicide risk
- Validated suicide-risk tools
- Assess ideation, plan, intent, means
- C-SSRS: severity across domains
- ASQ: brief paediatric emergency screen
For suicide risk, structured tools support but do not replace a direct clinical assessment. The Columbia-Suicide Severity Rating Scale maps ideation and behaviour across severity domains, and the Ask Suicide-Screening Questions tool is a brief screen validated for paediatric emergency settings. Either way, a positive screen triggers a same-visit, face-to-face risk assessment. [6] [7]
For substance use, the CRAFFT screen is validated for adolescents, and a positive result triggers further assessment and brief advice rather than a reflex urine drug screen. A urine drug screen has a narrow role, used only when the result will change management, and it carries real pitfalls of timing, consent, false results, and confidentiality. [4]
Targeted medical testing follows the history, never replaces it. Consider infection screens, electrolytes and glucose, a drug or toxin screen, or neuroimaging when the examination suggests an organic mimic — especially any acute cognitive change. A blanket panel ordered "to be sure" without a clinical question is low-value medicine. [9]
When the examination or collateral suggests an underlying neurodevelopmental condition, the right investigation is a formal cognitive or educational assessment, which sits downstream of the MSE and confirms what the bedside observation has flagged. [9]
Management — Resuscitation
Some findings cannot wait for follow-up. They demand action in the room, now, and recognising them is the pass-or-fail skill of this topic. [8]
A positive suicide-risk screen or any hint of intent. Do not file and forget. Perform a same-visit assessment of ideation, plan, intent, access to means, prior attempts, and protective factors. Decide between a crisis or emergency pathway for high risk and an early outpatient review with a written safety plan for lower risk. A psychology referral that takes three weeks is not a safe plan for a young person with active intent. [8] [5]
Active suicidal intent. If a young person discloses a plan and intent to act, override confidentiality as needed to keep them safe. Tell them plainly what must be shared and why. Secure immediate safety, do not leave them alone, and use your local child and adolescent mental-health crisis pathway. Share the minimum necessary with the people who can keep them safe, and preserve their dignity throughout. [8]
Acute psychosis or agitation. Maintain safety for the young person, the family, and the staff. Reduce stimulation, offer a low-stimulation space, bring enough support, and escalate to your local crisis or mental-health team. Avoid confrontation, and never attempt a solo physical restraint. [9]
Medical instability. If the examination reveals an unstable picture — bradycardia, postural drop, hypothermia, severe weight loss, or electrolyte disturbance from an eating disorder, or an acutely delirious state — this is a medical emergency that supersedes the rest of the visit. Stabilise, investigate, and escalate to a service that can manage the physical risk. [9]
Confidentiality override in practice. When you must break confidentiality, say so explicitly: "I am worried about your safety, so I need to share this with the team who can help you. I will tell you what I am doing and why." Share the minimum necessary. The goal is to keep the young person safe and still preserve enough trust that they will come back next time. [8] [10]
Same-visit response to a red-flag finding
Assess
Suicide risk, psychosis, abuse, instability — directly, now.
Decide
Crisis pathway versus early review with a safety plan.
Share
Override confidentiality only as needed; explain why.
Secure
Do not leave a high-risk young person alone or unsupported.
Hand over
Warm hand-off to crisis, safeguarding, or medical team.
Management — Definitive & Stepwise
Once the red flags are cleared, the MSE runs as a deliberate sequence. Treat it as a procedure with steps. [9]
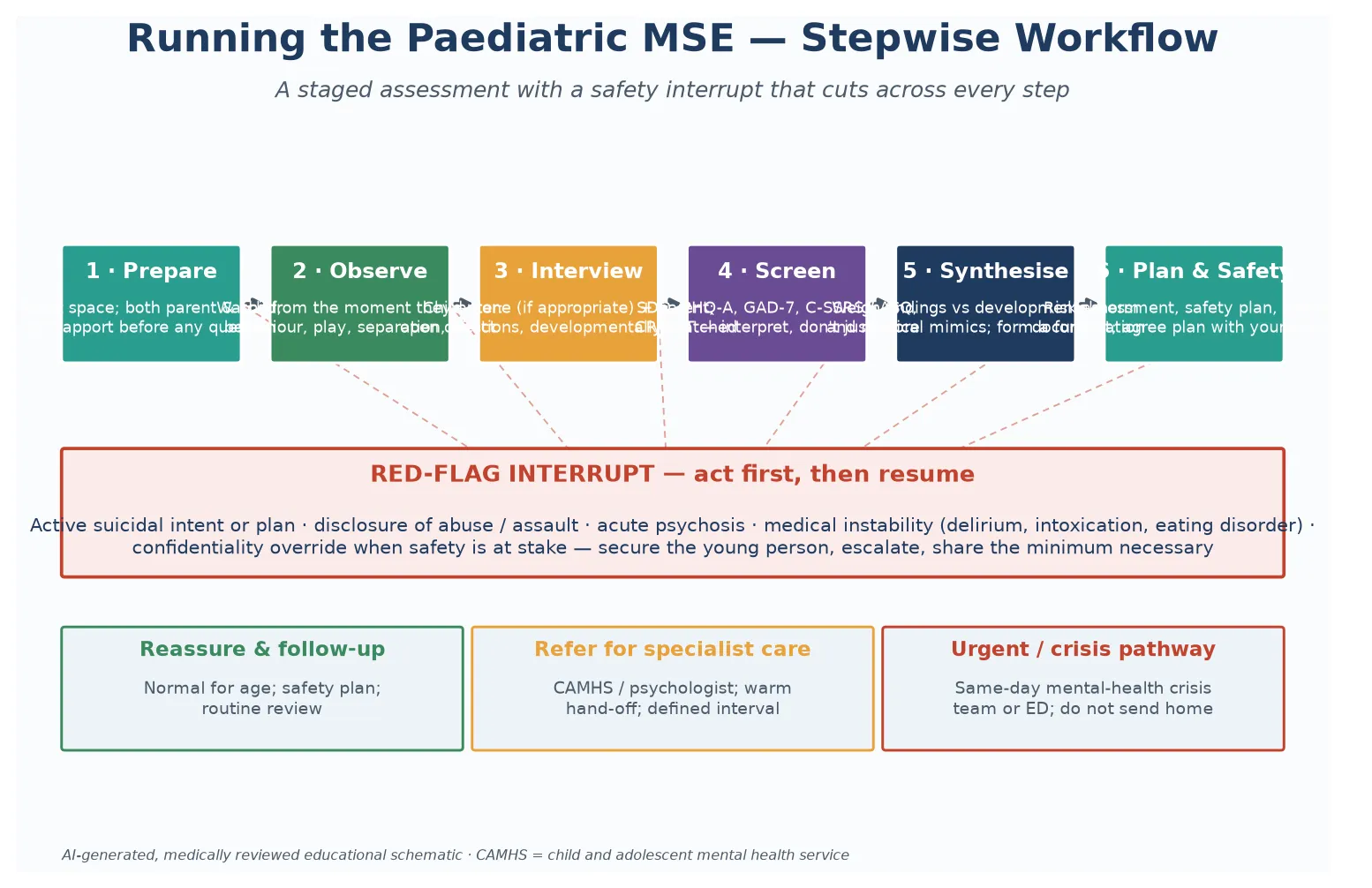
Prepare. Use a quiet, private space and plan where the parent will be. Preparation is not a courtesy; it is what makes a reliable examination possible, because noise, interruption, and an audience each suppress the findings you most need. [10]
Observe. Capture appearance and behaviour from the moment the young person enters, before any question. These first seconds are often the most honest data of the encounter, before the child has edited themselves for the interview. [9]
Interview. Take collateral from the parent and then, for an adolescent, secure time alone to take the young person's own account. Weigh the two together rather than letting either dominate, because each holds information the other cannot. [10]
Screen. Deploy the validated brief screens that match the findings — SDQ, PHQ-A, GAD-7, a suicide-risk tool, CRAFFT — and interpret them with the young person rather than scoring in silence. A screen is a doorway to a conversation, not the end of one. [1] [5]
Synthesise. Build a formulation that weighs the findings against developmental stage, context, and the medical differential. State what is most likely, what must be excluded, and what the key risks are. This is where the descriptive MSE becomes an interpretive, defensible plan. [9]
Plan and ensure safety. Agree the plan with the young person first, then the family, deciding together what stays confidential. Match the follow-up interval to the risk, give a written safety-net, and make a warm hand-off to the next service where needed. [8]
The full sequence
1. Prepare
Quiet space; plan the parent's role.
2. Observe
From entry — appearance, behaviour, affect.
3. Interview
Parent collateral, then child alone for adolescents.
4. Screen
SDQ, PHQ-A, GAD-7, suicide tool, CRAFFT as indicated.
5. Synthesise
Weigh against age, context, organic mimics.
6. Plan & safety
Risk, safety plan, referral, document, follow-up.
Record the examination clearly, domain by domain, so a colleague can rely on it tomorrow. A well-documented MSE lets the next clinician pick up where you left off, which matters most for the young people whose care will pass through many hands. [9]
Specific Subtypes & Scenarios
The preschool child. Rest the examination on structured play, behavioural observation, and parent collateral. Use toys, drawings, and simple tasks, and read affect from what the child does. Observe separation and reunion, the quality of play, and the response to a gentle request. The elicited domains are limited; the observed domains carry the weight. [10]
The school-age child. Use concrete language, pictures, and 0-to-10 scales. Children at this age can describe symptoms literally once they trust you, but they may conceal what shames them, so approach self-harm and abuse gently and with a clear reason for asking. A drawing or a feeling-faces chart can reach a child whom direct questions cannot. [10]
The adolescent. Secure time alone, state the confidentiality line, then use open questions and brief screens. Ask directly about mood, self-harm, and suicidal ideation, and perform a same-visit risk assessment whenever mood is low or any concern is raised. The adolescent MSE is where the elicited domains — thought content, perception, insight — come fully into play. [8] [5]
An opportunistic adolescent MSE in the emergency department
The child with intellectual disability or neurodiversity. Adapt to the young person's communication with concrete language and visual supports, and read findings against their baseline informed by a carer. The vital question is what has changed, because a flat affect or avoided eye contact may be this child's usual state rather than a new sign. Assess capacity issue-by-issue rather than as a global label. [9]
The telehealth examination. The same domains apply, with new safeguards. Confirm who else is in the room at each end, secure privacy at the young person's location, and agree how notes and results will reach them without breaching confidentiality through a shared portal. Observation is harder through a screen, so name what you can and cannot see. [10]
The young person in out-of-home care or youth justice. Confidentiality and consent lines are more complex because several adults may hold legal interests. Be explicit about who will be told what and why. These young people carry high rates of trauma and unmet need, so a steady, predictable, trauma-informed frame is the foundation of a reliable examination. [9]
Complications & Pitfalls
The most damaging pitfall is to treat a single snapshot as a fixed diagnosis. The MSE records a moment, and several conditions fluctuate, so a young person who looks well in your room may be profoundly unwell elsewhere. Weigh the worst point in the history, and repeat the examination when the picture is changeable. [9]
Reading the examination without a developmental baseline produces two opposite errors. You may over-diagnose normal variation — an adolescent's mood swings, a child's imaginary companion — or you may miss a real disorder because you compared the child to an adult norm instead of to children of the same age. State the baseline you are reading against. [9]
A failed rapport or a parent-dominated interview produces a falsely reassuring MSE. The boxes are ticked, the affect is described as "appropriate," and the dangerous findings stay hidden because the conditions for disclosure were never built. The fix is structural: secure time alone, state the confidentiality line, and approach the hard domains gently. [10]
Modern confidentiality breaches usually arrive through a screen, not a conversation. The patient portal, the itemised bill, the pharmacy text, and the open note can all surface a sensitive examination to a parent who holds the account. Know your local portal controls, use sensitive-note workflows, and keep confidential contact details current. [10]
Cultural and linguistic mismatch can mislabel a normal expression as a thought disorder. An idiom, a spiritual experience, or speech filtered through an interpreter may sound disorganised when it is not. Use a professional interpreter — never a family member for sensitive content — and ask openly when something is unclear, rather than coding uncertainty as pathology. [11]
Prognosis & Disposition
The MSE is not a one-off test; it is the opening of a relationship, and the quality of the encounter around it shapes future help-seeking. A young person who feels heard and respected is more likely to return, to disclose, and to accept care. A brisk, judgemental, or breached encounter can push them out of care for years. [10]
The disposition follows the risk. A normal examination with no positive screen may need only routine follow-up and a safety-net for the family. A positive screen that did not require the crisis pathway needs early review, often within one to two weeks, with a written safety plan and a clear escalation route. An acute safety concern needs same-day contact with a crisis service. [8] [5]
Safety-net every family after the visit, even when the examination was reassuring. Tell them what to watch for, what would warrant urgent help, and how to reach it. A good safety-net turns a single encounter into ongoing surveillance, which is how deterioration gets caught early. [8]
Because mental state can change, name when the examination should be repeated — after a change in treatment, after a crisis, or when collateral suggests the room encounter was not representative. The MSE you document today is one point on a line, and the disposition includes the next point. [9]
Special Populations
Children and adolescents with intellectual disability or neurodiversity need an examination adapted to their communication, with concrete language, visual supports, and a baseline drawn from a carer. Separate what is normal for this child from what is new, and screen for the same risks — including vulnerability to exploitation — that you would in any young person. [9]
Aboriginal, Torres Strait Islander, Māori and other Indigenous young people need a culturally safe examination that acknowledges the history and determinants shaping their health. Work in partnership with community-controlled services where possible, and recognise that culturally bound expressions of distress are not pathology. [10]
Migrant and refugee adolescents need a professional interpreter and, where available, a cultural broker — never a family member for sensitive content. Honour cultural meanings of family, distress, and confidentiality while still delivering the examination and its safety content. [10]
Gender-diverse and sexual-minority youth need an affirming, non-judgemental frame that screens the elevated risks of depression and suicide without forcing disclosure. Use the young person's names and pronouns, and apply the same confidentiality protections as for any adolescent. [8]
Young people in out-of-home care and youth justice carry high rates of trauma and unmet need. Negotiate the consent and confidentiality lines explicitly, because several adults may hold legal interests, and deliver a steady, predictable examination that can be the start of trust. [9]
When maltreatment or family violence is suspected, the examination must safeguard both the young person and any disclosure. Follow your local safeguarding pathway, obtain enough to act, and hand over to the child-protection team without interrogating the child yourself. [9]
Evidence, Guidelines & Regional Differences
The evidence base is mature at the level of the instrument and the principle, and it continues to evolve at the level of service delivery and the electronic record. [9]
The seven-domain structure of the MSE is the standard psychiatric framework, taught consistently across AACAP, RACP, RCPCH, AAP and RCPSC training. AACAP's practice parameter for the assessment and treatment of children and adolescents with depressive disorders embeds structured assessment and suicide-risk evaluation within the clinical encounter, which is the model the general paediatrician adapts. [9]
On screening, the USPSTF 2022 statement recommends screening adolescents aged 12 to 18 years for depression and notes the co-occurrence of suicide risk, which is why a mood screen and a suicide-risk assessment travel together in the adolescent MSE. [5]
The brief validated screens each rest on their own evidence. The SDQ is a well-established behavioural screen with multi-informant versions. The PHQ-9/PHQ-A is a validated depression severity measure, the GAD-7 a validated anxiety screen, the C-SSRS and ASQ validated suicide-risk tools, and CRAFFT a validated adolescent substance-use screen. Each detects; none diagnoses alone. [1] [2] [3] [6] [7] [4]
C-SSRS — initial validity (Posner 2011)
Multisite validation, adolescents and adults
Key finding
The Columbia-Suicide Severity Rating Scale showed initial validity and internal consistency across three multisite studies, mapping suicidal ideation and behaviour onto severity domains rather than a single yes/no.
Practice change
Use the C-SSRS to structure a suicide-risk assessment that captures ideation, plan, intent, and behaviour — but treat any positive finding as a prompt for a same-visit clinical decision, not as a standalone verdict.
In the perception domain, a 2022 review of psychotic experiences in the general population underlines that isolated perceptual experiences in young people are common and usually transient, with persistence, complexity, distress, and declining function marking the minority that warrant specialist assessment. [11]
[9] [5] [11]A live controversy is the tension between open-notes transparency for families and the adolescent's right to confidential care. Mandated access to notes can inadvertently expose a sensitive examination through a parent-held account, which is why sensitive-note workflows and confidential contact details now matter operationally, not just ethically. [10]
Where the evidence is weakest is the paediatric MSE itself. Developmental adaptation rests on clinical judgement more than on randomised trials, because you cannot ethically randomise children to a better or worse assessment. The honest position for a candidate is to state the principle, name the screens, and defer the operational detail to local statute and service pathways. [9]
Exam Pearls
The communication station is where this topic is most often examined, and the trap is to recite the domains without demonstrating the conduct. Examiners want to see you observe before you question, secure time alone with an adolescent, approach thought and perception gently, ask directly about suicide, and then do something with a positive answer in the room. A candidate who ticks every box but files the positive screen for later fails. [8] [5]
In the long case, expect a young person with a chronic illness or complex social background whose mental state has been neglected because the medical agenda crowded it out. Your job is to show you would perform a developmentally appropriate MSE, integrate the screens, weigh the medical differential, and coordinate care across the medical home and mental-health services. [9]
In the structured oral, be ready for a branching scenario that moves from a routine review to a mood finding to a suicide disclosure in a few minutes. The skill is to hold the structure — observe, interview, screen, assess safety, act — while the stakes rise, and to state plainly when you would override confidentiality and why. [8] [5]
References
- [1]Goodman R Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child and Adolescent Psychiatry, 2001.PMID 11699809
- [2]Kroenke K, Spitzer RL The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine, 2001.PMID 11556941
- [3]Spitzer RL, Kroenke K, Williams JB, Lowe B A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine, 2006.PMID 16717171
- [4]Knight JR, Sherritt L, Shrier LA, Harris SK, Chang G Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Archives of Pediatrics & Adolescent Medicine, 2002.PMID 12038895
- [5]Mangione CM, US Preventive Services Task Force Screening for Depression and Suicide Risk in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2022.PMID 36219440
- [6]Posner K, Brown GK, Stanley B, Brent DA, Yershova KV, Oquendo MA, Currier GW, Melvin GA, Greenhill L, Shen S, Mann JJ The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. American Journal of Psychiatry, 2011.PMID 22193671
- [7]Horowitz LM, Bridge JA, Teach SJ, Ballard E, Klima J, Rosenstein DL, Wharff EA, Geng X, Pao M, Koplewicz HS Ask Suicide-Screening Questions (ASQ): a brief instrument for the pediatric emergency department. Archives of Pediatrics & Adolescent Medicine, 2012.PMID 23027429
- [8]Shain B, American Academy of Pediatrics Committee on Adolescence Suicide and Suicide Attempts in Adolescents. Pediatrics, 2016.PMID 27354459
- [9]Birmaher B, Brent D, AACAP Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 2007.PMID 18049300
- [10]Cohen E, MacKenzie RG, Yates GL HEADSS, a psychosocial risk assessment instrument: implications for designing effective intervention programs for runaway youth. Journal of Adolescent Health, 1991.PMID 1772892
- [11]Staines L, Healy C, Coughlan H, Murphy J, Lane A, Kelleher I, Cannon M Psychotic experiences in the general population, a review; definition, risk factors, outcomes and interventions. Psychological Medicine, 2022.PMID 36004805