Paeds · neurology-neurodisability-and-neuromuscular
Antiseizure medicines: selection, adverse effects and monitoring
Also known as antiseizure medication · antiepileptic drug · ASM selection · antiepileptic drug monitoring · anticonvulsant adverse effects · antiepileptic pharmacology · valproate pregnancy prevention programme
A fellowship approach to antiseizure medicines in children: selecting the syndrome-matched first-choice drug, anticipating and monitoring the adverse effects that determine whether a child stays on treatment, and applying the valproate pregnancy prevention programme, the lamotrigine slow-titration rule, and the carbamazepine-worsens-absence contraindication.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A ten-year-old boy with newly diagnosed focal epilepsy is started on levetiracetam and develops irritability and aggression within two weeks; the task is to recognise the behavioural adverse effect, weigh it against seizure control, and decide whether to reduce, switch, or add a second agent. A fourteen-year-old girl with juvenile myoclonic epilepsy needs valproate for optimal seizure control, but the valproate pregnancy prevention programme applies, and the choice of an alternative such as levetiracetam or lamotrigine must be framed around her reproductive future. A seven-year-old on lamotrigine develops a rash six weeks into treatment, and the decision to stop or push through is the one that separates Stevens-Johnson syndrome from a benign morbilliform eruption. [5] [7] [11]
Select, start slow, survey, switch, stop — the five ASM moves
Overview & Definition
Antiseizure medicines are the drugs that suppress epileptic seizures by modulating the electrical activity of neurons, and their use in children is governed by the principle that the drug is chosen for the epilepsy syndrome, not for the seizure alone. The older term antiepileptic drug is being replaced by antiseizure medicine because these drugs suppress seizures without curing the underlying epilepsy, and the newer term is the one used in the ILAE and NICE guidelines. [1] [9]
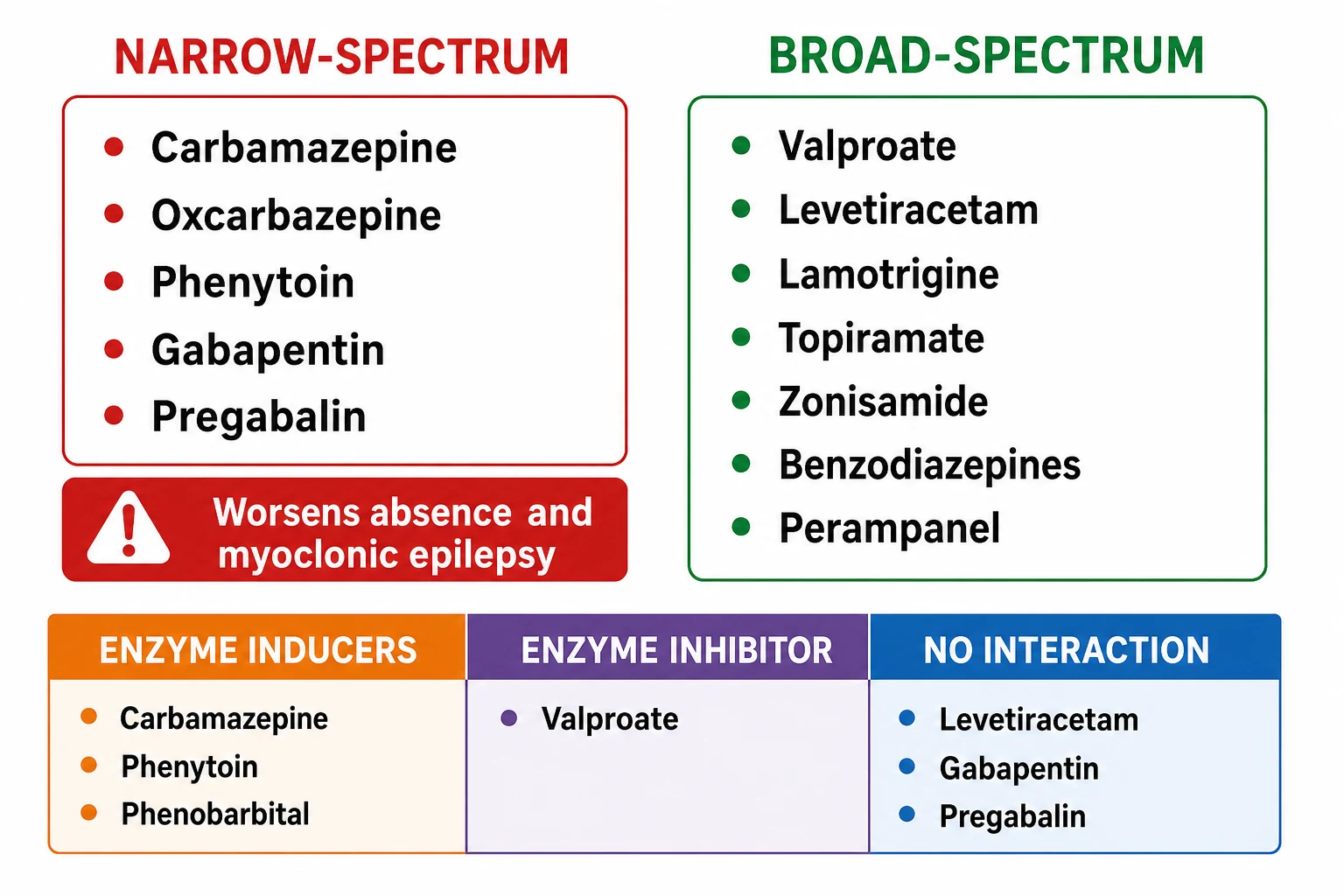
The fellowship framing rests on one distinction that governs selection. A narrow-spectrum drug controls focal seizures but worsens generalised seizures such as absence and myoclonus, while a broad-spectrum drug controls both. Carbamazepine, oxcarbazepine, phenytoin, gabapentin and pregabalin are narrow-spectrum, and they are the drugs that worsen absence and myoclonic epilepsy. Valproate, levetiracetam, lamotrigine, topiramate, zonisamide and the benzodiazepines are broad-spectrum. The selection move is to classify the syndrome from the EEG before the prescription, because the wrong spectrum drug does not merely fail but actively worsens the epilepsy. [1] [5]
The clinical importance of this topic is that adverse effects, not lack of efficacy, are the commonest reason children stop an antiseizure medicine. Roughly one in three children discontinues a drug because of an adverse effect, and the quality of life of a child with well-controlled seizures is driven more by the cognitive, behavioural and systemic effects of the medicine than by the seizure count. The fellowship skill is to anticipate these effects, to monitor for them, and to adjust the treatment so that the child is both seizure-free and functioning at their best. [5] [6]
Classification
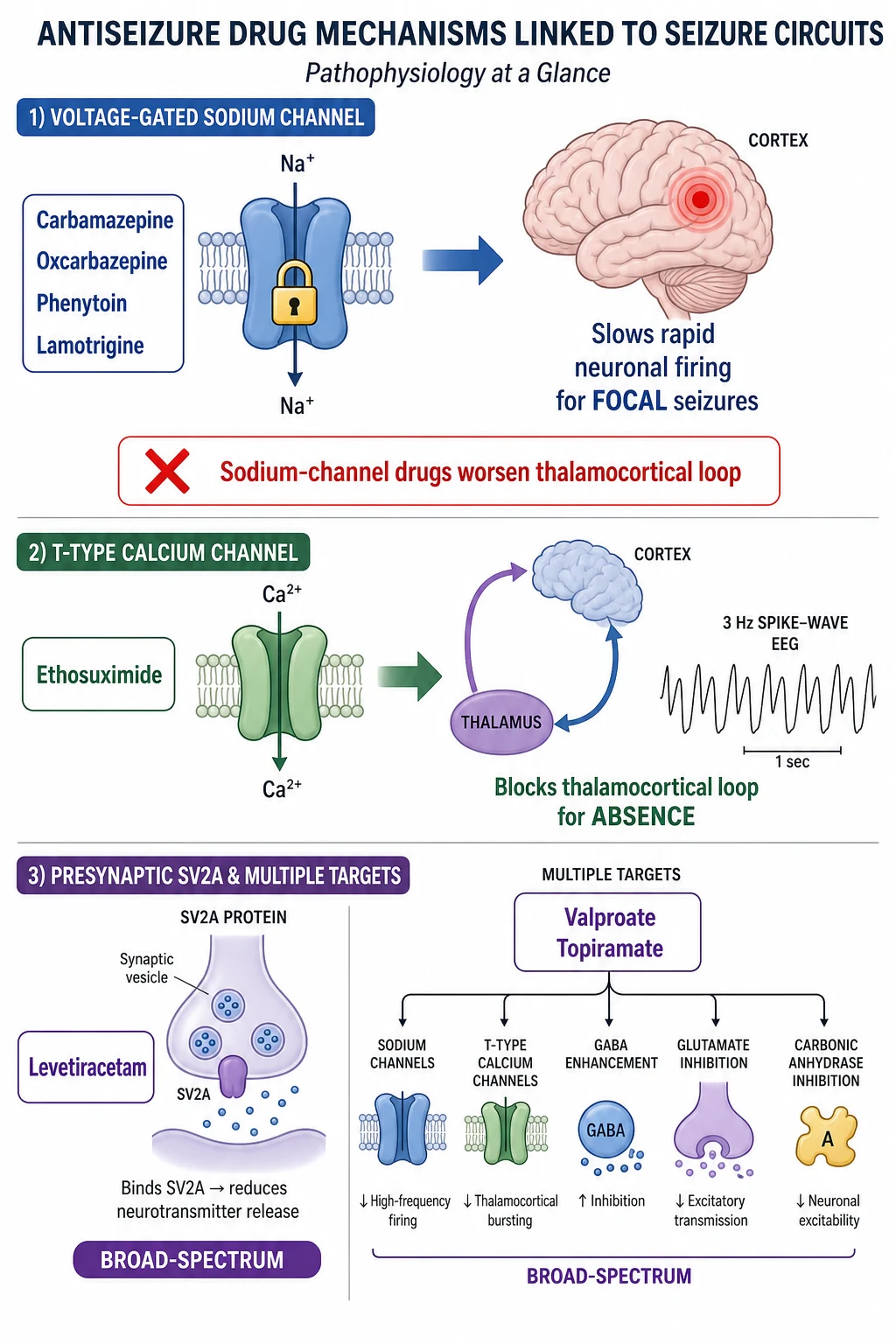
Antiseizure medicines are classified by their molecular mechanism of action, and each mechanism points to the seizure type it reaches. The sodium-channel blockers — carbamazepine, oxcarbazepine, phenytoin, lamotrigine, lacosamide and rufinamide — stabilise the inactive state of the voltage-gated sodium channel, slowing the rapid neuronal firing that drives a focal seizure. The calcium-channel blockers — ethosuximide and the gabapentinoids — block the T-type calcium channel of the thalamocortical loop in the case of ethosuximide, which is why it is specific for absence seizures. [5]
The synaptic-targeting drugs act on neurotransmitter release or receptors. Levetiracetam and brivaracetam bind the synaptic vesicle protein SV2A, modulating glutamate release, and they are broad-spectrum with no enzyme-inducing interactions. Valproate has multiple mechanisms — it blocks sodium channels, enhances GABA, and inhibits histone deacetylase — which explains both its broad spectrum and its unique adverse-effect profile. The benzodiazepines enhance GABA-A receptor function, and vigabatrin irreversibly inhibits GABA-transaminase. Perampanel is a selective AMPA-receptor antagonist, and topiramate and zonisamide act on multiple channels and carbonic anhydrase. [5]
The practical classification for the fellowship candidate is the spectrum: narrow versus broad. A narrow-spectrum drug is appropriate for focal epilepsy and will worsen absence and myoclonic epilepsy. A broad-spectrum drug is appropriate for both focal and generalised epilepsies and is the safer default when the syndrome is uncertain. The second practical axis is the enzyme effect: the enzyme inducers — carbamazepine, phenytoin, phenobarbital — accelerate the metabolism of oral contraceptives, warfarin and other antiseizure medicines, and they deplete vitamin D and calcium over years. The enzyme inhibitor valproate slows the metabolism of lamotrigine, which is the pharmacological basis of the lamotrigine slow-titration rule. [5] [12]
Epidemiology & Risk Factors
Roughly sixty to seventy per cent of children with epilepsy achieve seizure freedom on the first or second antiseizure medicine, and the proportion is higher when the drug is correctly matched to the syndrome. The SANAD trial established that lamotrigine and oxcarbazepine are effective for focal epilepsy, and the SANAD II trial confirmed levetiracetam as non-inferior to lamotrigine for focal epilepsy with a more favourable adverse-effect profile. Valproate remains the most effective single drug for generalised epilepsies in males, but its restriction in females of childbearing potential has shifted first-line selection toward levetiracetam and lamotrigine in that group. [2] [3]
The risk factors for severe adverse effects are the ones that guide monitoring. Polytherapy carries a higher adverse-effect burden than monotherapy, and the goal is always monotherapy wherever the syndrome allows. Underlying hepatic disease raises the risk of valproate hepatotoxicity, and renal impairment requires dose adjustment for renally cleared drugs such as levetiracetam and gabapentin. Genetic susceptibility plays a specific role: the HLA-B star 1502 allele, prevalent in Han Chinese and South-east Asian populations, confers a high risk of carbamazepine-induced Stevens-Johnson syndrome, and genetic testing before carbamazepine is recommended in these populations. [5] [8]
Age is a key risk modifier. Valproate hepatotoxicity is highest in children under two years, particularly those with developmental delay and polytherapy, and the mitochondrial disorders are the metabolic substrate that converts a mild transaminase rise into fulminant hepatic failure. The cognitive and behavioural effects of antiseizure medicines are more pronounced in the developing brain, which is why phenobarbital impairs cognition in young children and why levetiracetam behavioural effects are closely watched in the school-age group. [6] [8]
Pathophysiology
The molecular mechanism of each antiseizure medicine determines which seizure type it reaches, and the mechanism is the link between the drug and the syndrome it treats. A focal seizure is driven by the rapid, hypersynchronous firing of a localised cortical focus, and the sodium-channel blockers reach it by prolonging the inactive state of the voltage-gated sodium channel, which slows the firing rate and raises the seizure threshold. Carbamazepine, oxcarbazepine, phenytoin and lamotrigine all act through this mechanism, which is why they are effective for focal epilepsy. [5]
The thalamocortical loop is the circuit that the sodium-channel drugs cannot reach, and it is the reason they worsen absence and myoclonic epilepsy. A typical absence seizure arises from an oscillation between the thalamic reticular nucleus and the cortical pyramidal cells, sustained by T-type calcium channels, and ethosuximide blocks these channels directly, which is why it is the first-line drug for childhood absence epilepsy. The paradox is that sodium-channel blockers such as carbamazepine and phenytoin can enhance the thalamocortical oscillation, increasing the frequency of absence and myoclonic seizures rather than suppressing them. This is the pharmacological basis of the contraindication. [5] [6]
Valproate and the broad-spectrum drugs reach both the focal and the thalamocortical circuits through multiple mechanisms, which is why they are effective across the seizure types. Levetiracetam binds SV2A and modulates neurotransmitter release without interacting with the sodium channel or the enzyme systems, giving it a clean interaction profile and a broad spectrum. Topiramate and zonisamide act on multiple channels and on carbonic anhydrase, which explains both their broad efficacy and their shared adverse effects of weight loss, nephrolithiasis and metabolic acidosis. The GABA-enhancing drugs — the benzodiazepines and vigabatrin — potentiate inhibition, and vigabatrin irreversibly inhibits GABA-transaminase in the retina as well as the brain, which is the mechanism of its irreversible visual field loss. [5]
Clinical Presentation
The clinical presentation of antiseizure medicine adverse effects spans every system, and the fellowship skill is to recognise the signature of each drug. The central nervous system effects are the commonest: sedation and ataxia with carbamazepine and phenytoin, cognitive blunting and word-finding difficulty with topiramate, and behavioural changes — irritability, aggression, depression — with levetiracetam. These effects are dose-dependent and often resolve with dose reduction, but the levetiracetam behavioural effects can persist and may require a switch. [5] [6]
The cutaneous adverse effects are the ones that demand immediate action. A rash within the first eight weeks of lamotrigine, carbamazepine, phenytoin or oxcarbazepine is Stevens-Johnson syndrome or toxic epidermal necrolysis until proven otherwise, and the drug must be stopped immediately. Lamotrigine rash risk is higher with rapid titration and with concurrent valproate, which inhibits lamotrigine metabolism and raises the plasma level, and the safeguard is the slow-titration schedule. The rash of carbamazepine is strongly associated with the HLA-B star 1502 allele in Asian populations, and pre-prescription genetic testing is recommended. [5] [11]
The systemic adverse effects define the monitoring requirements for each drug. Valproate causes weight gain, thrombocytopenia, hyperammonaemia and hepatotoxicity, the last being highest in children under two years on polytherapy with a metabolic substrate. Carbamazepine and oxcarbazepine cause hyponatraemia through drug-induced inappropriate antidiuretic hormone secretion, and the child may present with headache, lethargy or a seizure. Topiramate and zonisamide cause weight loss, metabolic acidosis and nephrolithiasis. Vigabatrin causes irreversible visual field constriction that may be asymptomatic until advanced. Phenytoin causes gingival hyperplasia, hirsutism and coarse facial features with chronic use, and its zero-order kinetics mean small dose increments produce large plasma-level rises. [5] [8]
Which reassuring-sounding stories must never close the search for a serious adverse effect? A child on levetiracetam who becomes irritable may have a treatable behavioural effect that resolves on dose reduction or switching, but the same symptom in a child on valproate may signal hyperammonaemic encephalopathy. A headache in a child on carbamazepine may be tension or may be hyponatraemia from the drug. A weight loss in a child on topiramate may be welcome or may signal metabolic acidosis and nephrolithiasis. The fellowship skill is to attribute the symptom to the drug first and prove otherwise, not to dismiss it. [5] [8]
Differential Diagnosis
The differential diagnosis when a child on an antiseizure medicine presents with a new symptom is between a drug adverse effect, a disease progression, and an unrelated intercurrent illness. A worsening of seizures on carbamazepine may be drug-induced exacerbation from a wrong-spectrum choice, non-adherence, an intercurrent illness, or disease progression, and the safeguard is to check the drug level, review the EEG, and reconsider the syndrome before increasing the dose. [1] [4]
The rash differential is the one with the highest stakes. A morbilliform eruption that spares the mucosae and improves with antihistamine may be a benign drug rash that can be managed conservatively. A rash with mucosal involvement, skin blistering, target lesions, or skin pain is Stevens-Johnson syndrome or toxic epidermal necrolysis, and the drug must be stopped immediately, the child admitted, and dermatology consulted. The pitfall is pushing through a rash to avoid losing seizure control, because a severe cutaneous reaction can be fatal. [5] [11]
The cognitive and behavioural change differential is between the drug effect, a comorbid condition, and a new encephalopathy. A child with epilepsy has higher baseline rates of attention-deficit hyperactivity disorder, anxiety and depression than their peers, and a new behavioural change may be the comorbidity declaring itself rather than a drug effect. The safeguard is to take a careful baseline before starting the drug and to reassess at each visit, attributing the change to the drug only when the temporal relationship and the known drug profile support it. A developmental regression on valproate demands an ammonia level to exclude hyperammonaemic encephalopathy. [6] [8]
Clinical & Bedside Assessment
The assessment before starting an antiseizure medicine establishes the baseline against which adverse effects are judged. The history captures the seizure type and syndrome from the EEG, the developmental and cognitive baseline, the psychiatric history, the family history of drug reactions, and the concurrent medications that may interact. In a child of Asian ancestry, the family history of carbamazepine reaction prompts HLA-B star 1502 testing before that drug is prescribed. [5] [9]
The examination before starting captures the weight, the height, the skin, the neurological system, and the developmental and cognitive state. The weight is the baseline for the drugs that cause weight gain — valproate — or weight loss — topiramate and zonisamide. The skin is examined for any pre-existing eruption that might later be confused with a drug rash. The neurological examination establishes the baseline against which ataxia, sedation or a new focal deficit is later judged. [9]
The assessment at each follow-up visit is the monitoring that keeps the child on treatment. Ask about seizure frequency and any new seizures, and ask specifically about the adverse-effect signature of the drug: behaviour on levetiracetam, weight and cognition on topiramate, headache and lethargy on carbamazepine, gum hypertrophy on phenytoin, and visual symptoms on vigabatrin. Weigh the child, examine the skin for rash, and check the developmental and cognitive trajectory. A child who is seizure-free but failing at school may need a drug change rather than a dose increase. [5] [6]
Which findings must never be dismissed? A rash in the first eight weeks of any new antiseizure medicine demands immediate drug cessation and assessment for Stevens-Johnson syndrome. A child on valproate with vomiting and lethargy demands a liver function test and an ammonia level. A child on carbamazepine with a new headache or seizure demands a serum sodium. And a child on vigabatrin who develops visual symptoms demands urgent ophthalmology review, because the visual field loss is irreversible. [8] [5]
Investigations
The baseline investigations before starting an antiseizure medicine include a full blood count, liver function tests, and a renal function panel for most drugs. These establish the baseline against which later changes are judged, and they are particularly important for the drugs with haematological and hepatic toxicity — valproate, carbamazepine, and felbamate. A vitamin D level is checked for children starting an enzyme-inducing drug, because long-term use depletes vitamin D and impairs bone mineralisation. [8] [12]
Therapeutic drug monitoring is not routinely required for most modern antiseizure medicines. The exceptions are phenytoin, whose zero-order kinetics and narrow therapeutic window make the plasma level essential, and carbamazepine and valproate, whose levels are useful when seizure control is inadequate, toxicity is suspected, or adherence is in question. Levetiracetam, lamotrigine and topiramate have less well-defined therapeutic ranges, and their levels are used mainly to confirm adherence or to guide dose optimisation in the setting of concurrent interacting drugs. [5] [9]
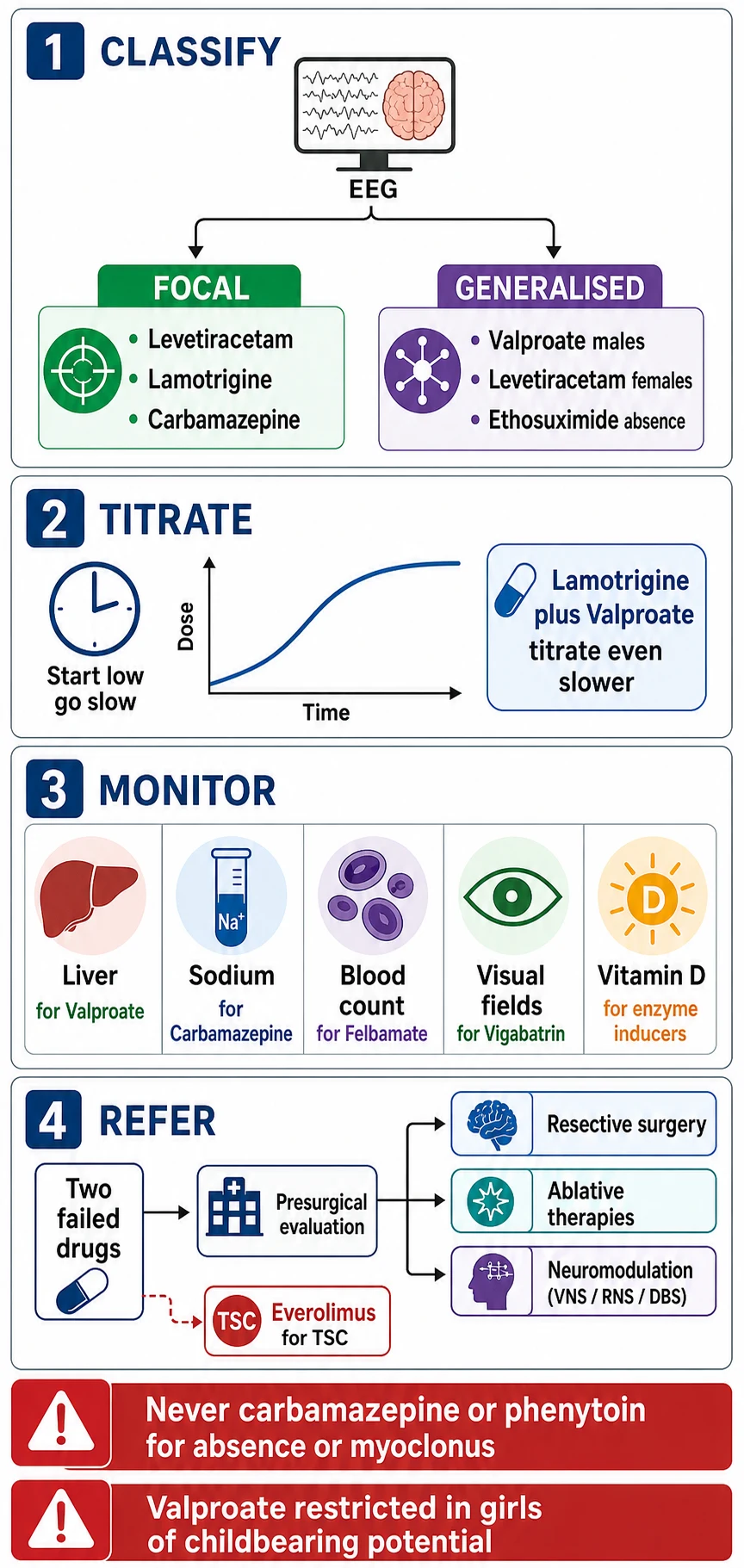
The drug-specific monitoring defines the follow-up schedule. Valproate demands liver function tests and a full blood count, particularly in the first six months and in children under two years. Carbamazepine and oxcarbazepine demand a full blood count and a serum sodium, with the sodium checked within the first three months and after any dose increase. Vigabatrin demands baseline and periodic visual field testing by perimetry, and the family is counselled about the irreversible risk. Felbamate, reserved for severe refractory epilepsy, demands fortnightly full blood counts for the first year because of the risk of aplastic anaemia. The enzyme-inducing drugs demand vitamin D and bone density surveillance over years. [5] [12]
Management — Resuscitation
Resuscitation in the context of antiseizure medicines is the management of the acute severe adverse effect, not of the seizure itself, which is owned by the sibling topic on status epilepticus. The cutaneous emergency is Stevens-Johnson syndrome or toxic epidermal necrolysis, and the first action is to stop the causative drug immediately, to admit the child, and to involve dermatology and intensive care. Fluid management, wound care, nutritional support, and infection surveillance are the pillars, and the child must never be rechallenged with the causative drug or a cross-reactive agent. [5] [11]
The hepatic emergency is valproate-induced fulminant hepatic failure, and the first action is to stop the valproate, to check liver function and coagulation, and to involve hepatology. The child under two years on polytherapy with a developmental delay is the highest-risk group, and the family is counselled about the warning signs of vomiting, lethargy, increased seizures and jaundice before starting. Carnitine supplementation is used in valproate hepatotoxicity and hyperammonaemia on the rationale that it supports mitochondrial beta-oxidation, though the evidence is limited. [8]
The metabolic emergency is severe hyponatraemia from carbamazepine or oxcarbazepine, presenting with headache, vomiting, seizure or altered consciousness, and the first action is to stop the drug and to manage the sodium correction slowly to avoid central pontine myelinolysis. The haematological emergency is felbamate-induced aplastic anaemia or carbamazepine-induced agranulocytosis, and the first action is to stop the drug, to check the full blood count, and to involve haematology. The behavioural emergency is severe psychiatric decompensation on levetiracetam or perampanel, and the first action is to reduce or stop the drug and to involve mental health services. [5] [8]
Management — Definitive & Stepwise
The definitive management is the stepwise selection and titration of the syndrome-matched antiseizure medicine, and the first step is always the syndrome classification. For focal epilepsy, the SANAD and SANAD II trials support levetiracetam, lamotrigine, carbamazepine and oxcarbazepine as first-line monotherapy, with levetiracetam preferred for its favourable adverse-effect profile and lack of enzyme interactions. For generalised epilepsy in a male, valproate is the most effective single drug. For absence epilepsy, ethosuximide is first-line when absence occurs alone, with valproate added if generalised tonic-clonic seizures coexist. For myoclonic epilepsy, valproate in males and levetiracetam or lamotrigine in females. [1] [2]
The titration principle is to start low and go slow. Lamotrigine is titrated over at least eight weeks, and even more slowly when valproate is concurrent, because valproate inhibits lamotrigine metabolism via uridine diphosphate glucuronosyltransferase and raises the plasma level, multiplying the rash risk. Topiramate is titrated slowly to minimise cognitive blunting. Levetiracetam can be started at a therapeutic dose in some situations because of its rapid onset and clean profile, but behavioural tolerance is built by starting low. The goal of titration is seizure freedom with the lowest effective dose, and the dose is increased only when seizures persist and the adverse-effect burden is tolerable. [11] [5]
The switch principle governs the move from the first to the second drug. When the first appropriately chosen and tolerated drug fails to control seizures, the second drug is introduced as monotherapy — not added — wherever possible, because polytherapy increases the adverse-effect burden. When two appropriately chosen and tolerated drugs fail, the epilepsy is drug-resistant by the ILAE definition, and the child is referred to a specialist epilepsy centre for presurgical evaluation, because the chance of a third drug achieving seizure freedom falls sharply. The everolimus trial in tuberous sclerosis complex demonstrated that a mechanism-targeted drug can reduce seizures in a specific genetic epilepsy, and it illustrates the principle that the aetiology guides the treatment. [4] [10]
Selected by epilepsy syndrome, not by habit
Specific Subtypes & Scenarios
The valproate scenario is the highest-yield fellowship case, because it sits at the intersection of efficacy, teratogenicity and regulation. Valproate is the most effective single drug for the genetic generalised epilepsies — juvenile myoclonic epilepsy, juvenile absence epilepsy, and generalised tonic-clonic seizures — but it is teratogenic, raising the major congenital malformation risk, and it carries a dose-dependent neurodevelopmental risk including autism and lower cognitive scores in exposed offspring. The AAN, AES and SMFM practice guideline states that valproate is avoided in pregnancy wherever possible and that women of childbearing potential are counselled before starting and at every visit. [7] [5]
The lamotrigine scenario is the rash case. Lamotrigine is an effective broad-spectrum drug for both focal and generalised epilepsies, and it is the preferred first-line in females of childbearing potential because it has the most favourable pregnancy safety data among the antiseizure medicines. The challenge is the rash risk, which is roughly one in ten in adults and lower in children, and which is multiplied by rapid titration and by concurrent valproate. The safeguard is the slow-titration schedule — over at least eight weeks, and longer when valproate is concurrent — and the instruction to stop the drug immediately if any rash appears. [11] [7]
The carbamazepine scenario is the interaction case. Carbamazepine is an effective narrow-spectrum drug for focal epilepsy, but it is a potent enzyme inducer that accelerates the metabolism of the oral contraceptive pill, warfarin, and other antiseizure medicines, and it causes hyponatraemia, leukopenia and Stevens-Johnson syndrome. The HLA-B star 1502 allele, prevalent in Han Chinese and South-east Asian populations, confers a very high risk of carbamazepine-induced Stevens-Johnson syndrome, and genetic testing is recommended before prescribing in these populations. Oxcarbazepine shares the sodium-channel mechanism and the hyponatraemia risk but is a weaker enzyme inducer. [5] [9]
The drug-resistant epilepsy scenario opens the door to surgery and to the targeted therapies. A focal epilepsy that fails two appropriately chosen and tolerated drugs is drug-resistant by the ILAE definition, and the child is referred for presurgical evaluation with video-EEG, MRI and PET. In tuberous sclerosis complex, the EXIST-3 trial demonstrated that adjunctive everolimus, an mTOR inhibitor, reduces focal-onset seizures by targeting the molecular basis of the disease, and it illustrates the principle that the aetiology guides the treatment. In Dravet syndrome, stiripentol, fenfluramine and cannabidiol are syndrome-specific agents added to valproate and clobazam. [4] [10]
Complications & Pitfalls
The complications of antiseizure medicine treatment are the adverse effects that erode the quality of life and the adherence that keeps the child on treatment. The cognitive effects — sedation, memory impairment, slowed processing — are the commonest reason a child underperforms at school on treatment, and they are dose-dependent and often reversible. The behavioural effects — irritability, aggression, depression — on levetiracetam and perampanel are the ones that families struggle with most, and they are the ones most often missed because the family does not volunteer them. The fellowship skill is to ask actively at every visit. [5] [6]
The pitfall of the wrong-spectrum drug is the error that causes the most preventable seizure worsening. Carbamazepine or phenytoin prescribed for an unrecognised absence or myoclonic epilepsy worsens the seizures, may precipitate absence status, and delays the correct diagnosis. The safeguard is the EEG before the prescription, and a low threshold to reconsider the syndrome whenever a child worsens on an antiseizure medicine rather than simply increasing the dose. [1] [5]
The pitfall of ignoring drug interactions is the error that compromises concurrent treatment. An adolescent girl on carbamazepine who is prescribed the oral contraceptive pill may conceive because the enzyme induction accelerates the oestrogen metabolism, and a child on warfarin for a cardiac condition may become subtherapeutic when carbamazepine is added. The safeguard is to review the concurrent medications at every visit and to adjust the dose or choose a non-interacting drug such as levetiracetam or lamotrigine. [5] [12]
The pitfall of the missed vitamin D deficiency is the error with the longest reach on bone health. Children on long-term enzyme-inducing drugs — carbamazepine, phenytoin, phenobarbital — have lower vitamin D levels and lower bone mineral density than their peers, and they are at higher risk of fractures over years. The safeguard is the baseline and periodic vitamin D check, supplementation where indicated, and the consideration of a non-enzyme-inducing drug for long-term use. [12] [5]
Prognosis & Disposition
The prognosis of antiseizure medicine treatment is generally favourable when the drug is correctly matched to the syndrome. Roughly sixty to seventy per cent of children achieve seizure freedom on the first or second drug, and the proportion is higher when the syndrome is correctly classified and the adverse effects are managed proactively. The prognostic modifiers are the underlying cause — a structural brain abnormality or a genetic syndrome carries a harder course — and the presence of drug resistance, defined as the failure of two appropriately chosen and tolerated drugs. [1] [4]
The quality-of-life prognosis is driven by the adverse-effect burden as much as by the seizure control. A child who is seizure-free but sedated, cognitively blunted, or behaviourally dysregulated is not well, and the fellowship skill is to balance seizure freedom against function. The children who do best are those whose drug is right for the syndrome, whose adverse effects are caught early and managed, and whose developmental, educational and mental-health comorbidities are screened for and treated alongside the seizures. [5] [6]
The disposition is shared between the general paediatrician and the paediatric neurologist. The general paediatrician owns the initiation of the first-choice medicine in a straightforward syndrome, the adverse-effect surveillance at follow-up, the developmental and educational surveillance, and the long-term relationship with the family. The paediatric neurologist is consulted for the atypical or drug-resistant epilepsy, the presurgical evaluation, the developmental and epileptic encephalopathies, and the transition to adult care. The transition is a structured handover that includes reviewing the medicine choice — particularly valproate in young women — and introducing reproductive health counselling before the young person is sexually active. [9] [7]
Special Populations
Adolescent girls of childbearing potential are the special population that demands the most deliberate antiseizure medicine planning. The valproate pregnancy prevention programme applies from the onset of reproductive potential, and the first-choice drug for a generalised epilepsy in a female adolescent is levetiracetam or lamotrigine wherever the syndrome permits. When valproate is the only effective option, the conditions of the pregnancy prevention programme are met: specialist supervision, a pregnancy test before starting, highly effective contraception, an annual specialist review, and a signed risk acknowledgement form. The transition to adult care is the moment to review the choice, to introduce contraception and pregnancy planning, and to involve the general practitioner and the adult neurology service. [7] [5]
Children with developmental disability and neurodiversity are over-represented among the epilepsy population, and their adverse-effect profile is harder to elicit because the child may not communicate the symptom. The behavioural effects of levetiracetam may manifest as an escalation of self-injury or aggression in a non-verbal child, and the cognitive effects of topiramate may be masked by the baseline developmental delay. The assessment adapts — a caregiver who interprets the baseline, a longer consultation, a lower threshold to try a different drug — and the management balances seizure control against the cognitive and behavioural effects. [6] [5]
Indigenous, migrant, refugee and socioeconomically disadvantaged children face the additional burden of access and equity. The distance to a specialist and an electroencephalogram delays the diagnosis and the treatment, and the cost of the medicine and the follow-up tests may compromise adherence. The HLA-B star 1502 testing for carbamazepine is relevant in South-east Asian and Han Chinese populations, and a newly arrived migrant child may carry an undocumented past drug history that must be reconstructed. The fellowship answer builds the supports — a reliable medicine supply, a clear follow-up schedule, a seizure action plan, and a single named coordinator — that keep the child in care. [9] [5]
Socioeconomic disadvantage compounds all of these. Adherence to a daily medicine is harder when the family is under stress, the appointments are missed, and the epilepsy is uncontrolled, which deepens the educational and developmental disadvantage. The fellowship answer acknowledges the social determinants and builds the practical supports that keep the child safe and in care. [9] [5]
Evidence, Guidelines & Regional Differences
The evidence for antiseizure medicine selection rests on a small number of landmark trials and guidelines. The 2013 ILAE evidence review graded the monotherapy evidence by seizure type and syndrome, and it remains the reference for first-choice selection. The SANAD trial compared the standard and the newer drugs for focal and generalised epilepsy, supporting lamotrigine for focal and valproate for generalised. The SANAD II trial established levetiracetam as non-inferior to lamotrigine for focal epilepsy with a favourable adverse-effect profile, and it reflected the shift away from carbamazepine first-line in many centres. [1] [2] [3]
The 2024 practice guideline from the American Academy of Neurology, the American Epilepsy Society and the Society for Maternal-Fetal Medicine addressed the teratogenic, perinatal and neurodevelopmental outcomes of antiseizure medicines in pregnancy, and it reinforced the avoidance of valproate and the relative safety of levetiracetam and lamotrigine. The NICE guideline NG217 on the epilepsies in children, young people and adults provides the UK framework for selection and monitoring, and it is the reference for the fellowship answer in the ANZ context, supplemented by the local Therapeutic Goods Administration guidance. [7] [9]
The regional differences centre on the valproate pregnancy prevention programme. In the United Kingdom and Europe the Medicines and Healthcare products Regulatory Agency and the European Medicines Agency restrict valproate in girls and women of childbearing potential through a structured pregnancy prevention programme with annual specialist review. In Australia the Therapeutic Goods Administration advises caution without the same regulatory structure, and in North America the emphasis is on informed shared decision-making. The fellowship answer applies the most cautious standard, because the teratogenic and neurodevelopmental risk is the same in every region. [7] [9]
The controversies are the timing of medicine withdrawal after a sustained remission, the role of generics, and the place of the newer agents such as cannabidiol and fenfluramine in the treatment algorithm. The fellowship answer names these judgement calls without pretending that a single algorithm resolves them, and it anchors each decision in the syndrome, the evidence, and the individual child. [1] [9]
Exam Pearls
The fellowship answer turns on six facts. Antiseizure medicines are selected by the syndrome, not by habit, and the spectrum — narrow versus broad — is the selection axis. Carbamazepine, oxcarbazepine, phenytoin and gabapentin are narrow-spectrum and worsen absence and myoclonic epilepsy. Valproate, levetiracetam, lamotrigine, topiramate and zonisamide are broad-spectrum. Valproate is restricted in girls and women of childbearing potential under the pregnancy prevention programme. Two failed appropriately chosen drugs define drug-resistant epilepsy and trigger a presurgical referral. The adverse-effect signature of each drug — lamotrigine rash, levetiracetam behaviour, carbamazepine hyponatraemia, vigabatrin visual fields — is the monitoring skill. [1] [5]
The examiner probes three traps. The first is the child with absence or myoclonic epilepsy given carbamazepine — the syndrome comes before the prescription. The second is the adolescent girl on valproate without a pregnancy prevention plan — the valproate rule applies from the onset of reproductive potential. The third is the rash in the first eight weeks of lamotrigine that is pushed through rather than stopped — a severe cutaneous reaction can be fatal, and the drug is stopped immediately. [1] [11]
The examiner rewards the candidate who frames the adverse effects as part of the treatment, not as incidental. The cognitive, behavioural and systemic effects of antiseizure medicines are surveyed at every visit, the drug is adjusted when the effect erodes the quality of life, and the monitoring for the severe effects — liver, blood, sodium, visual fields, vitamin D — is built into the follow-up schedule. A candidate who shows this breadth demonstrates the pharmacological reasoning that the fellowship demands. [5] [6]
References
- [1]Glauser T, Ben-Menachem E, Bourgeois B, Cnaan A, Guerreiro C, Kalviainen R, Mattson R, French JA, Perucca E, Tomson T, ILAE Subcommission on AED Guidelines. Updated ILAE evidence review of antiepileptic drug efficacy and effectiveness as initial monotherapy for epileptic seizures and syndromes. Epilepsia, 2013.PMID 23350722
- [2]Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, Gamble C, Jacoby A, Shackley P, Smith DF, Tudur-Smith C, Vanoli A, Williamson PR. A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial. Health Technol Assess, 2007.PMID 17903391
- [3]Marson A, Burnside G, Appleton R, Smith D, Leach JP, Sills G, Tudur-Smith C, Plumpton C, Hughes DA, Williamson P, Baker GA, Balabanova S, Taylor C, Brown R, Hindley D, Howell S, Maguire M, Mohanraj R, Smith PE, SANAD II collaborators. The SANAD II study of the effectiveness and cost-effectiveness of levetiracetam, zonisamide, or lamotrigine for newly diagnosed focal epilepsy: an open-label, non-inferiority, multicentre, phase 4, randomised controlled trial. Lancet, 2021.PMID 33838757
- [4]Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen Hauser W, Mathern G, Moshe SL, Perucca E, Wiebe S, French J. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia, 2010.PMID 19889013
- [5]Perucca P, Gilliam FG. Adverse effects of antiepileptic drugs. Lancet Neurol, 2012.PMID 22832500
- [6]Loring DW, Meador KJ. Cognitive side effects of antiepileptic drugs in children. Neurology, 2004.PMID 15037684
- [7]Pack AM, Oskoui M, Williams Roberson S, Donley DK, French J, Gerard EE, Gloss D, Miller WR, Munger Clary HM, Osmundson SS, McFadden B, Parratt K, Pennell PB, Saade G, Smith DB, Sullivan K, Thomas SV, Tomson T, Dolan O'Brien M, Botchway-Doe K, Silsbee HM, Keezer MR. Teratogenesis, Perinatal, and Neurodevelopmental Outcomes After In Utero Exposure to Antiseizure Medication: Practice Guideline From the AAN, AES, and SMFM. Neurology, 2024.PMID 38748979
- [8]Vidaurre J, Gedela S, Yarosz S. Antiepileptic Drugs and Liver Disease. Pediatr Neurol, 2017.PMID 29097018
- [9]Jones KEA, Howells R, Mallick AA, Paul SP, Dey I. NICE guideline review: Epilepsies in children, young people and adults NG217. Arch Dis Child Educ Pract Ed, 2023.PMID 37339862
- [10]French JA, Lawson JA, Yapici Z, Ikeda H, Polster T, Nabbout R, Curatolo P, de Vries PJ, Dlugos DJ, Berkowitz N, Voi M, Peyrard S, Pelov D, Franz DN. Adjunctive everolimus therapy for treatment-resistant focal-onset seizures associated with tuberous sclerosis (EXIST-3): a phase 3, randomised, double-blind, placebo-controlled study. Lancet, 2016.PMID 27613521
- [11]Guberman AH, Besag FM, Brodie MJ, Dooley JM, Duchowny MS, Pellock JM, Richens A, Stern RS, Trevathan E. Lamotrigine-associated rash: risk/benefit considerations in adults and children. Epilepsia, 1999.PMID 10403224
- [12]Shellhaas RA, Joshi SM. Vitamin D and bone health among children with epilepsy. Pediatr Neurol, 2010.PMID 20472188