Paeds · pain-palliative-and-end-of-life-care
Grief, bereavement and sibling support
Also known as Paediatric bereavement care · Sibling grief after child death · Complicated grief in parents · Anticipatory grief in life-limiting illness · Staff grief in paediatric death
Fellowship guide to grief, bereavement and sibling support after the death of a child. Covers anticipatory grief, developmental understanding of death by age, sibling support, parental complicated grief red flags, memory-making, cultural and religious variation, staff grief, and referral pathways. Built for RACP, RCPCH/MRCPCH, ABP/ACGME and RCPSC examination.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A twelve-year-old girl has just died at home from progressive neurodisability. Her parents are numb; her eight-year-old brother has become withdrawn and is refusing school. The community team asks how to structure bereavement care. The fellowship task is to move from this scene to a safe, ethical, documented plan that puts the child first while holding the family. [1] [2] [3]
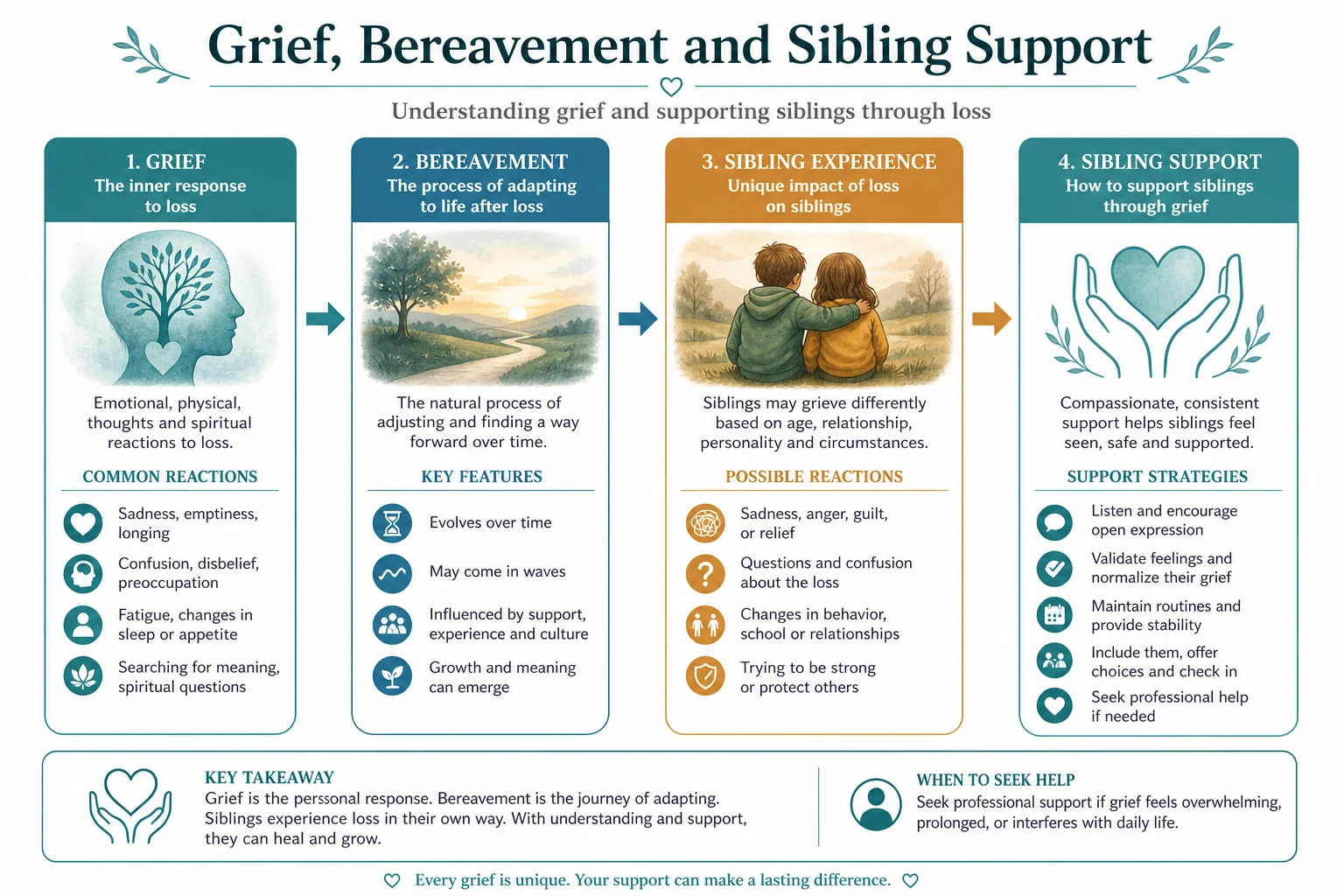
Grief and bereavement care after a child dies includes anticipatory support before death, developmental and sibling-aware follow-up, screening for complicated grief, culturally safe rituals and memory-making, school liaison, and structured support for staff who carried the child. [1] [2] [3]
This page is written so a candidate can answer examiner questions across definition, ethics, communication, documentation and escalation without reaching for another source. Regional frameworks differ in language, but the bedside sequence is stable: stabilise comfort, explore understanding, make a recommendation, share the decision, document, and escalate early when disagreement persists. [1] [2] [3] [4]
Classification
Classification is useful when it changes the conversation or the pathway. [1] [2] [3]
By who is grieving. Parents and carers; siblings; grandparents; peers; staff. [1] [2] [3]
By timing. Anticipatory grief; acute grief; longer-term bereavement; anniversary reactions. [1] [2] [3]
By risk. Normative grief; complicated or prolonged grief disorder risk; traumatic grief after sudden death. [1] [2] [3]
These axes are complementary. A single child may sit in more than one cell, and the classification should be restated whenever the clinical trajectory changes. [1] [2] [3]
Epidemiology & Risk Factors
Life-limiting illness and end-of-life decisions are concentrated in intensive care, oncology, neurodisability and neonatal services, but general paediatricians meet the same decisions on the ward and in the community. [1] [2] [3]
Risk of conflict rises when prognostic communication has been delayed, when multiple teams give inconsistent messages, when trust has been damaged by prior care, and when cultural or spiritual needs have not been elicited. [1] [2] [3] [4]
Children with medical complexity and technology dependence account for a growing share of deaths in PICU cohorts, which increases the importance of advance care planning before crisis. [1] [2] [3]
Pathophysiology
The pathophysiology that matters for this topic is not only disease biology; it is the pathway from prognostic uncertainty to a best-interests judgement under emotional load. [1] [2] [3]
Children's understanding of death evolves with age: irreversibility, universality and non-functionality are grasped at different developmental stages. [1] [2] [3]
Sibling grief is often invisible because adults protect siblings from information or focus solely on parents. [1] [2] [3]
Complicated grief red flags include persistent yearning with functional collapse, suicidal ideation, and inability to care for remaining children beyond the early months. [1] [2] [3]
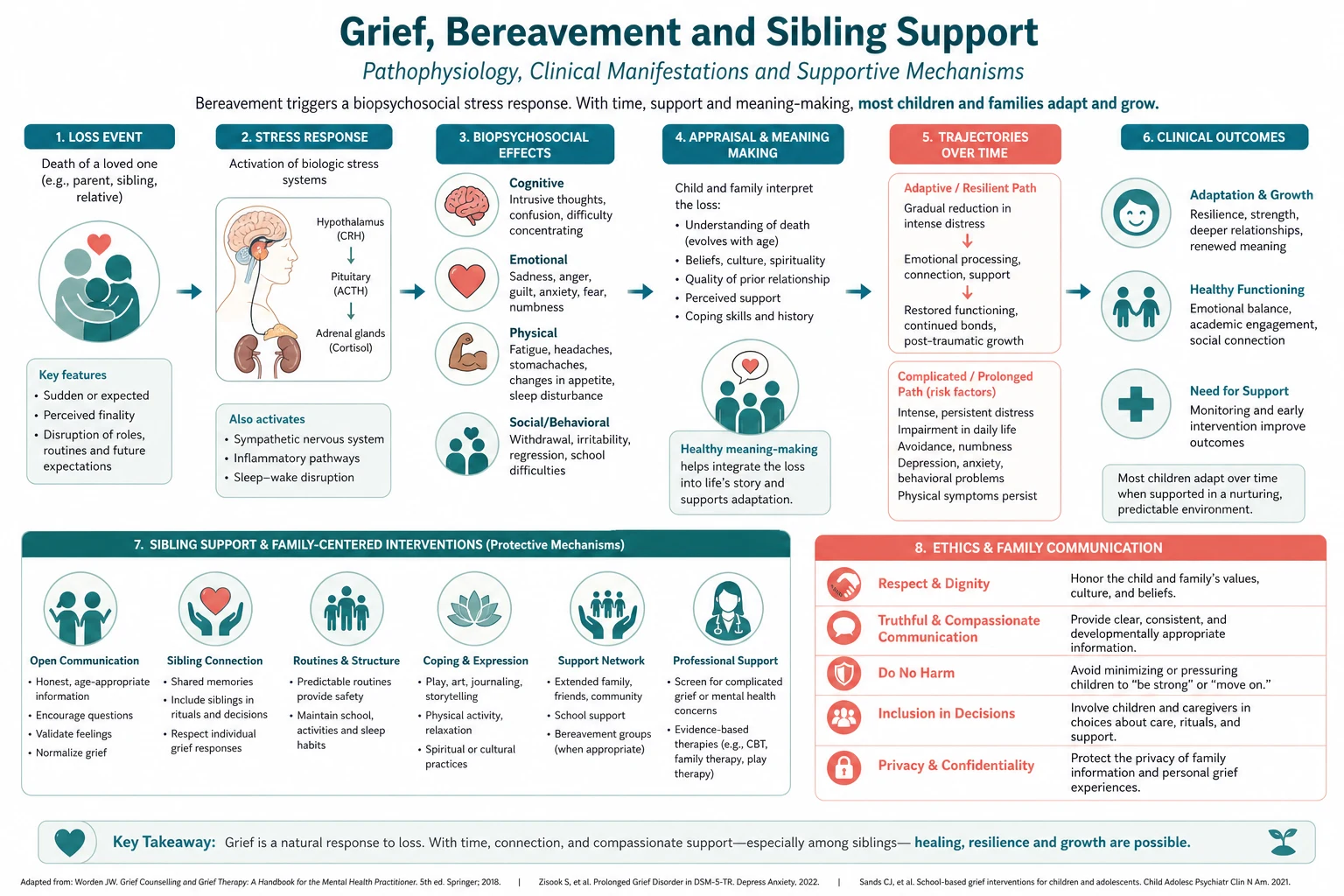
Understanding this pathway prevents two opposite errors: rushing a limitation decision before the family has understood the prognosis, and indefinitely postponing a decision that is already clear because the conversation feels hard. [1] [2] [3]
Clinical Presentation
The presentation is often a slow accumulation of burdens rather than a single dramatic moment: repeated admissions, escalating technology, loss of interactive ability, or a catastrophic event with no recovery trajectory. [1] [2] [3]
Families may present with hope for miracle recovery, fear of abandonment, guilt about giving up, or exhaustion after months of vigilance. Staff may present with moral distress when they judge ongoing treatment to be harmful. [1] [2] [3] [4]
Red-flag presentations include intractable disagreement, requests for potentially inappropriate treatment, adolescent refusal, and sudden collapse of parental coping. [1] [2] [3]
Differential Diagnosis
Not every request to do everything is a fixed demand for non-beneficial treatment. Differential considerations include misunderstood prognosis, incomplete symptom control, distrust, spiritual waiting for a ritual or relative, and decisional paralysis from grief. [1] [2] [3]
Likewise, not every staff wish to stop treatment is a completed best-interests analysis; countertransference, resource pressure and incomplete information must be examined. [1] [2] [3]
[1] [2] [3]Clinical & Bedside Assessment
Assessment has two parallel tracks: the child's clinical trajectory and the family's understanding and values. [1] [2] [3]
For the child, document current treatments, burdens, residual awareness or comfort behaviours, trajectory over days to weeks, and whether a time-limited trial is still informative. For the family, explore what they have been told, what they understand, what they hope for, what they fear most, and who else must be in the room. [1] [2] [3] [4]
In the adolescent, assess decision-making capacity specifically rather than assuming absence of capacity from age alone. [1] [2] [3]
[1] [2] [3]Investigations
Investigations at this stage exist only to answer a decision-relevant question. Non-contributory blood tests, imaging and monitoring that increase burden without changing the plan should be stopped as part of good care. [1] [2] [3]
When neurological prognosis is uncertain, targeted imaging or specialist review may support a time-limited trial framework. When death determination is required for donation pathways, only accepted paediatric testing protocols are used. [1] [2] [3] [4]
Management — Resuscitation
Resuscitation decisions are goals-of-care decisions made in advance when possible. [1] [2] [3]
If a child arrests without a prior plan, default emergency care proceeds while senior clinicians urgently clarify trajectory and family understanding. If a valid limitation plan exists, it is followed, and comfort measures are maximised. [1] [2] [3]
Never use a chaotic arrest as the first goals-of-care conversation if that conversation could have been held electively. [1] [2] [3]
Management — Definitive & Stepwise
-
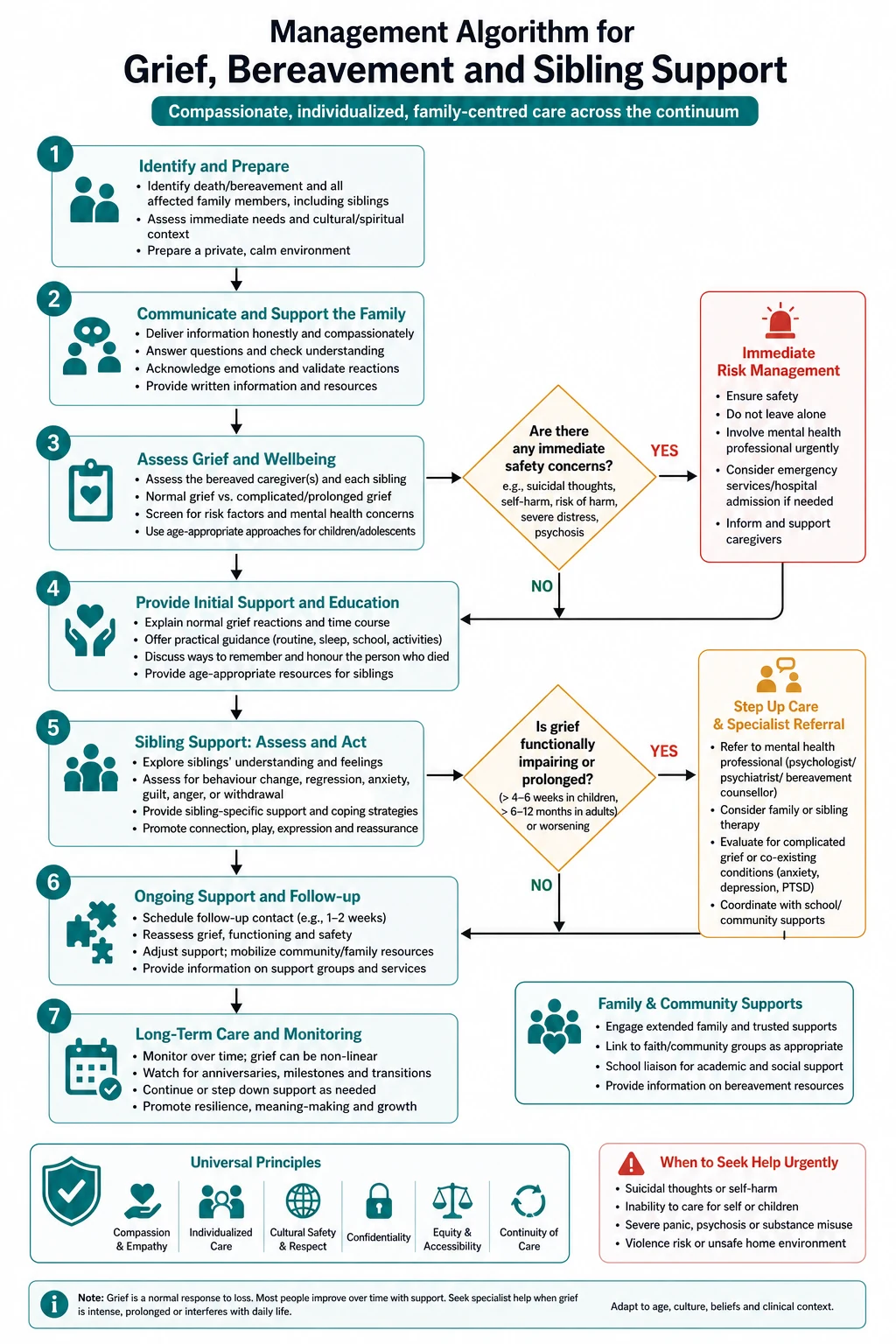
Begin bereavement care before death through honest communication, memory-making and sibling inclusion. [1] [2] [3]
-
After death, offer a structured follow-up contact, written information, and a named bereavement lead. [1] [2] [3]
-
Screen parents and siblings for complicated grief risk and refer early to specialist services when red flags appear. [1] [2] [3]
-
Support staff through debrief, peer support and access to employee assistance; do not rely on stoicism alone. [1] [2] [3]
Recognise
Recognise the decision point and stabilise comfort while the plan is formed.
Meet
Hold a senior-led goals-of-care meeting exploring understanding, hopes and worries.
Agree and document
Agree, document and communicate the plan across teams, naming treatments continued and limited.
Escalate if needed
Escalate ethics or court if disagreement persists, without abandoning comfort care.
Deliver support
Deliver the plan with intensified family and sibling support.
Symptom control is not paused while ethics is consulted. Pain, dyspnoea, secretions and agitation are treated actively throughout. [1] [2] [3]
Documentation should name the people present, the best-interests reasoning, the treatments to continue, the treatments to limit or withdraw, the review points, and the escalation plan if consensus fails. [1] [2] [3] [4]
Specific Subtypes & Scenarios
Death after long illness
Anticipatory grief may already be advanced; still expect acute intensification at death. [1] [2] [3]
Sudden unexpected death
Trauma features are common; prioritise clear information, viewing, and early mental-health pathways. [1] [2] [3]
Neonatal or stillbirth loss
Validate parenthood, offer memory-making, and support subsequent pregnancy anxiety. [1] [2] [3]
Staff grief after a difficult death
Structured debrief within days; watch for cumulative moral distress. [1] [2] [3]
Complications & Pitfalls
Common pitfalls include delayed honesty, inconsistent messaging across teams, asking parents to carry the whole decision alone, treating withdrawal as ethically worse than withholding, and abandoning families who disagree. [1] [2] [3]
High-yield examiner traps
Do not equate parental demand with best interests. Do not treat withdrawing as morally worse than withholding. Do not ask parents to decide alone. Do not stop comfort care when life support is limited. Do not delay ethics involvement until conflict is toxic.
Legal risk rises when documentation is absent, when unilateral withdrawal occurs without due process in a contested case, or when a capable adolescent is excluded. [1] [2] [3]
Prognosis & Disposition
Prognosis discussions should be honest about uncertainty ranges and should separate physiological survival from meaningful recovery. [1] [2] [3]
Disposition after a limitation decision may be continued PICU comfort care, ward-based end-of-life care, hospice, or home with community palliative support, depending on symptoms, family preference and service availability. [1] [2] [3] [4]
Special Populations
Neonates require perinatal palliative partnership and parental holding opportunities. Adolescents require capacity assessment and inclusion. Children with disability require careful avoidance of ableist assumptions about quality of life. Indigenous and culturally diverse families require culturally safe communication and room for extended kinship decision structures. [1] [2] [3]
Rural and remote families may face travel, accommodation and retrieval constraints that shape place-of-care options and must be named explicitly. [1] [2] [3]
Evidence, Guidelines & Regional Differences
[1] [2] [3] [4]The RCPCH framework remains a high-yield structure for classifying when treatment limitation may be appropriate, while ANZICS and local health-service guidance shape operational practice in Australia and New Zealand. North American institutions rely on ethics committees and professional society statements with similar best-interests logic. [1] [2] [3] [4] [5]
Evidence for communication interventions and early palliative partnership supports fewer conflicts and better family outcomes than late, crisis-only conversations. [1] [2] [3] [4]
Exam Pearls
- Ask about the sibling by name at every contact. [1] [2]
- Developmental truth-telling beats protective silence for most children. [1] [2]
- Complicated grief is a clinical diagnosis pathway, not a moral failure. [1] [2]
- Anniversary dates re-open grief — plan contact. [1] [2]
- Staff grief is patient-safety relevant. [1] [2]
BEDSIDE decision frame
References
- [1]Yuste Segarra M et al. Grieving in the shadows: A systematic review of invisible losses in siblings of pediatric cancer patients. Death Stud, 2026.PMID 42054273
- [2]Hussain H et al. Exploring challenges and opportunities in paediatric bereavement care: a qualitative study from a tertiary care hospital in Pakistan. BMC Palliat Care, 2026.PMID 41851707
- [3]Jolly A et al. Being broken: A qualitative study exploring unexpected death in the Paediatric Intensive Care Unit and the family experience of care. Aust Crit Care, 2026.PMID 41512802
- [4]Bylund-Grenklo T et al. Acute and long-term grief reactions and experiences in parentally cancer-bereaved teenagers. BMC Palliat Care, 2021.PMID 34044835
- [5]Eklund R et al. Talking about death when a parent with dependent children dies of cancer: A pilot study of the Family Talk Intervention in palliative care. Death Stud, 2022.PMID 34214023
- [6]Roberts M et al. A mixed methods analysis of songs written by bereaved preadolescents in individual music therapy. J Music Ther, 2013.PMID 23847863
- [7]Himelstein BP et al. Pediatric palliative care. N Engl J Med, 2004.PMID 15103002
- [8]Papadatou D et al. Home or hospital as the place of end-of-life care and death: A grounded theory study of parents' decision-making. Palliat Med, 2021.PMID 33307990