Paeds · preventive-and-community-paediatrics
Aboriginal and Torres Strait Islander child health
Also known as Indigenous Australian child health · First Nations Australian paediatric care · ATSI child health · Aboriginal child health · Torres Strait Islander child health · Culturally safe Aboriginal paediatric care
Fellowship-level culturally safe care for Aboriginal and Torres Strait Islander children: structural inequities, ACCHO partnership, ear lung skin and post-strep pathways, developmental vulnerability, racism as a health exposure, and regional distinctions from other Indigenous health systems.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar presents an Aboriginal toddler with chronic wet cough and school hearing concerns. The family left a previous clinic after feeling judged. This is core general paediatrics in Australia, not an optional special interest. [2] [12]
Aboriginal and Torres Strait Islander peoples are the First Nations peoples of Australia. They hold diverse languages, cultures, Countries and community structures. Never treat “Indigenous” as one culture or one postcode. [1]
Health, in many Aboriginal and Torres Strait Islander frameworks, is holistic. It includes physical health, social and emotional wellbeing, cultural identity, kinship and connection to Country. A problem list that only lists diagnoses misses the family’s goals. [1]
Cultural safety is not a badge you award yourself. It is defined by whether the Aboriginal or Torres Strait Islander person experiences care free of racism and power misuse. Cultural awareness is a starting step. Cultural safety is the outcome families feel. [2] [3]
Classification
Structure the consultation in three layers that you keep distinct. [1] [2]
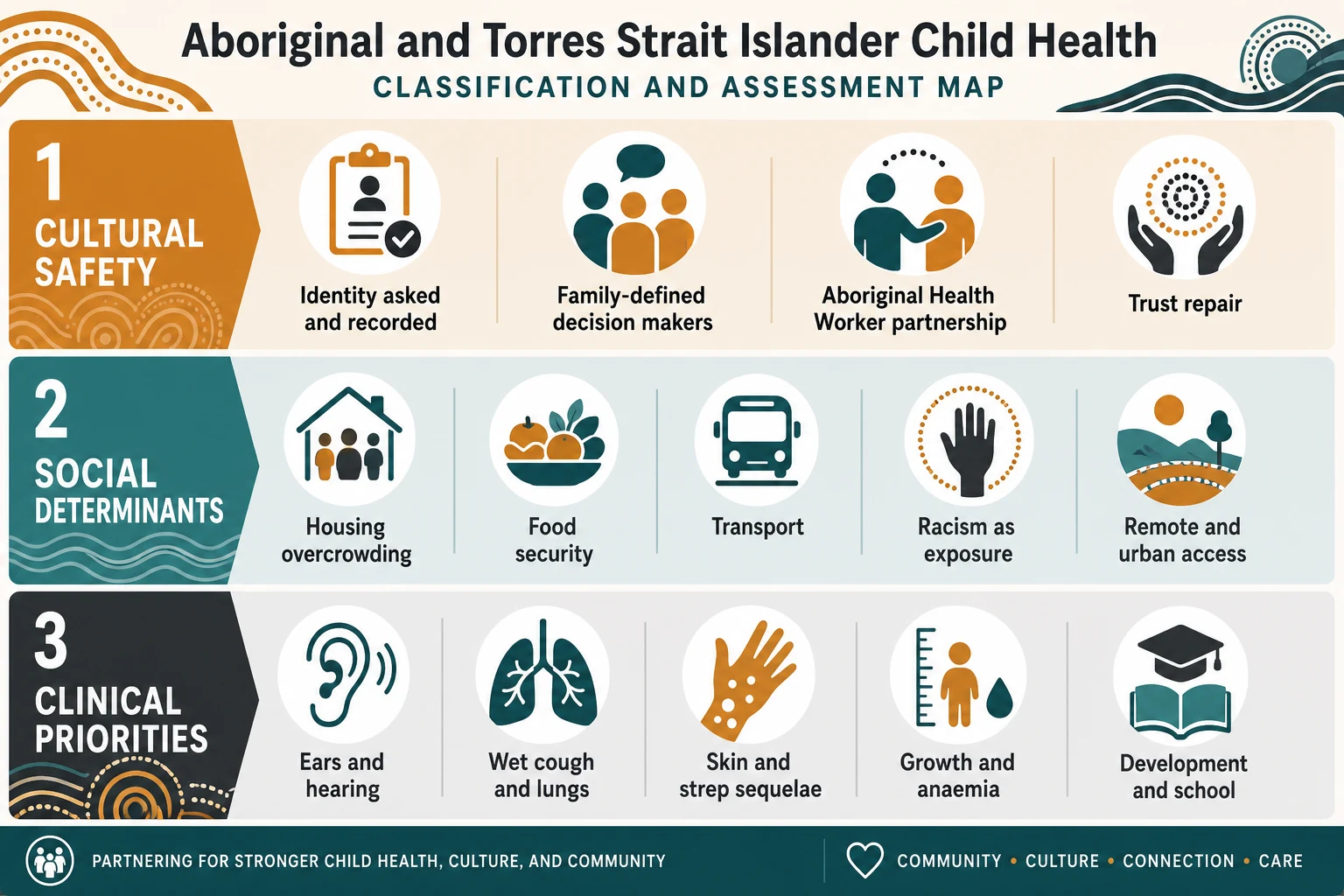
Frames you must not blur
- Recipient-defined experience of care
- Power, trust, communication, anti-racism
- Aboriginal Health Worker and ACCHO partnership
- Housing, overcrowding, food, transport, income
- Remote and urban access barriers
- Racism as a measured health exposure
- Ear disease and hearing
- Wet cough and chronic lung disease risk
- Skin infection and post-strep sequelae
- Growth, anaemia, development
Also classify care setting: Aboriginal Community Controlled Health Organisation (ACCHO/ACCHS), mainstream primary care, hospital, outreach/remote clinic, and telehealth with a local worker present. Community control is a model of care, not a courtesy referral. [2]
Epidemiology & Risk Factors
Inequities in ear disease, chronic respiratory disease, rheumatic fever risk, developmental vulnerability and some mental-health outcomes are well described. Explain them as the product of colonisation’s ongoing effects, socioeconomic disadvantage, environmental conditions and racism — not as inherent biological destiny. [1] [5] [8]
Risk amplifiers include overcrowding, poor housing, smoke exposure, interrupted primary care, transport barriers, food insecurity, and experiences of discrimination in health services. Longitudinal and scoping evidence links racial discrimination with worse child and adolescent health outcomes. Timing of first exposure can matter for wellbeing trajectories. [5] [6] [7] [8]
Protective factors include strong cultural identity, kinship networks, community-controlled services, continuous trusted primary care, immunisation access, and early childhood supports. Strengths belong in the history, not only problems. [1] [2]
Urban care is not low risk. Urban Aboriginal children still carry substantial ear-health and access needs. Remoteness is one risk pattern, not the definition of Indigeneity. [11]
Immunisation coverage surveillance remains a core equity metric. Coverage gaps should trigger catch-up planning with trusted providers, not blame. [17]
Pathophysiology
Structural conditions change infection ecology and care continuity. That is the mechanism examiners want. [8] [12]
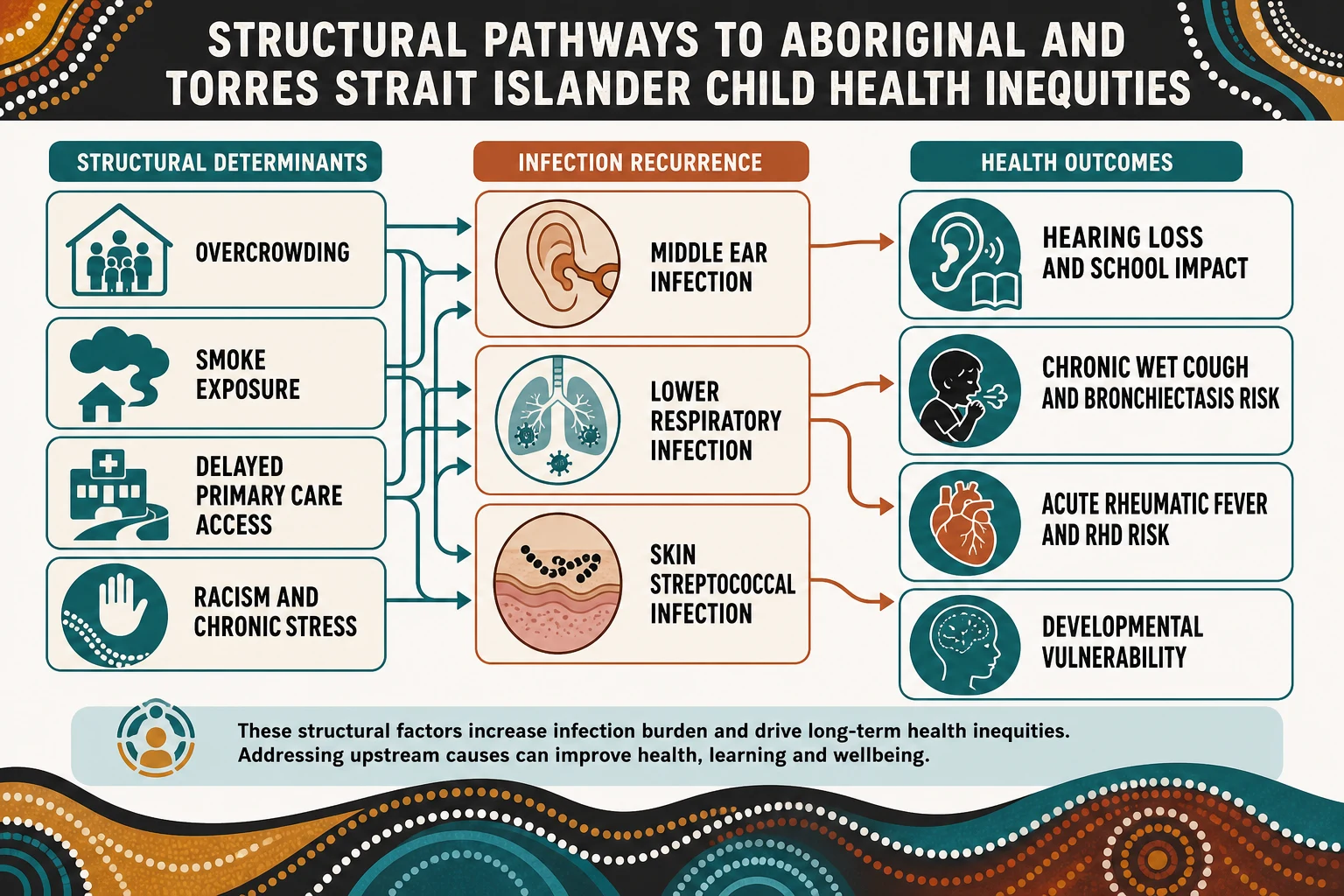
Ears. Recurrent acute otitis media and otitis media with effusion are linked to social determinants such as overcrowding and health-service access. Persistent middle-ear disease impairs hearing during language acquisition and school entry. Behaviour and learning concerns may be hearing until proven otherwise. [8] [9] [11]
Lungs. Indigenous children experience a high burden of acute and chronic respiratory disease. Recurrent infection and protracted bacterial bronchitis sit on a pathway toward bronchiectasis in high-burden populations. Whole-population and Northern Territory cohort work shows substantial chronic respiratory disease and distinct First Nations bronchiectasis profiles. [12] [13] [14]
Skin and post-streptococcal sequelae. Repeated group A streptococcal exposure in crowded living conditions raises population risk of acute rheumatic fever (ARF), rheumatic heart disease (RHD) and acute post-streptococcal glomerulonephritis. ARF remains a critical inequity marker for Indigenous Australian children. [15] [16]
Development. Early childhood anaemia more than doubled developmental vulnerability at school age in a remote Far North Queensland Aboriginal and Torres Strait Islander cohort. Nutrition, infection and hearing interact. [18]
Racism and stress. Discrimination is not only an ethical failure. It is associated with physical and mental health harm across Aboriginal and Torres Strait Islander populations, and longitudinal child-health literature supports racism as a developmental risk exposure. [5] [6] [7]
Clinical Presentation
Families may present late after prior racism, or may prefer an ACCHO and only attend hospital in crisis. Some bring a community worker or senior family member as decision partner. That is appropriate engagement, not interference. [2] [5]
Common high-yield clusters: [9] [12]
- chronic or recurrent ear discharge, hearing difficulty, or “not listening” at school [9] [11]
- wet cough lasting weeks, recurrent chest infections, exercise limitation [12] [14]
- skin sores, scabies in household clusters, and secondary bacterial infection [15]
- faltering growth, iron deficiency risk, developmental concerns at preschool/school entry [18]
- incomplete immunisation with access and trust barriers [17]
Red-flag presentations include respiratory distress, suspected sepsis, severe dehydration, possible ARF (fever with migratory arthritis, chorea, carditis features, or strongly suggestive context), severe malnutrition, acute mental-health crisis, and safeguarding concerns. Treat these as emergency pathways first. [12] [15]
Silence, short answers, or a family spokesperson can reflect communication norms, shame from past care, or waiting for the right person to speak. Do not label this non-compliance. [2]
Differential Diagnosis
Keep ordinary paediatric differentials open. Race does not replace clinical reasoning. [12]
| Pattern | High-burden considerations | Do not miss |
|---|---|---|
| Wet cough | Protracted bacterial bronchitis; bronchiectasis risk | Foreign body; TB where relevant; immunodeficiency if atypical |
| “Behaviour / not listening” | Hearing loss from OM/OME | Autism, ADHD, trauma, vision, language disorder |
| Joint pain + fever | ARF in high-incidence context | Septic arthritis, osteomyelitis, JIA, SLE |
| Skin sores | Impetigo, scabies clusters | Invasive bacterial disease, nephritis risk |
| School difficulty | Hearing, anaemia, sleep, housing instability | Specific learning disorder, maltreatment, mental health |
Urban low-incidence ARF regions still see cases. Do not exclude ARF solely because the child lives in a southern city. Conversely, do not diagnose ARF on weak features without a proper work-up pathway. [15] [16]
Clinical & Bedside Assessment
Use a practical script you can say aloud in a viva. [2] [3]
Culturally safe bedside sequence
Identity and welcome
Introduce yourself and role. Ask Aboriginal and/or Torres Strait Islander status. Offer Aboriginal Health Worker or Liaison involvement.
Family decision map
Ask who should be part of decisions today. Kinship decision-makers may not match the hospital next-of-kin form.
Holistic history
Housing, overcrowding, food, transport, school, hearing, cough, skin, growth, immunisation, prior care experiences, strengths and goals.
Targeted exam
Ears and hearing behaviour, wet cough and work of breathing, skin, growth parameters, cardiac exam when ARF risk is plausible, developmental screens.
Shared plan
Plain language plan, ACCHO link, transport/appointment logistics, safety-net, written summary the family can use.
Examine with consent, privacy and trauma-informed technique. Explain each step. For ear checks in young children, national consensus work supports routine ear health and hearing checks for Aboriginal and Torres Strait Islander children under six years in primary care. [9] [10]
Ask about racism in prior care only if the family opens that door or trust-building requires it. When they describe it, believe them and change the plan. [5]
Investigations
Investigate for decisions, not for stereotypes. [9] [12]
Ears and hearing. Follow primary-care ear health and hearing check recommendations for children under six. Escalate to audiology and ENT pathways when indicated by examination or developmental concern. Urban children need the same seriousness as remote children. [9] [10] [11]
Lungs. For prolonged wet cough, assess severity, prior treatments, and red flags. Imaging and specialist referral are driven by chronicity, severity and failure of appropriate primary treatment — not by race alone. In high-burden settings, have a low threshold to treat wet cough as infection-driven and to seek bronchiectasis assessment when chronic. [12] [13] [14]
ARF/RHD concern. Use local RHDAustralia-aligned pathways for diagnosis, echocardiography and secondary prophylaxis decisions. Do not invent Jones criteria thresholds from memory in the exam if you are unsure — state the need for current criteria and urgent senior/public-health programme input. Screening literature exists for high-risk populations; programme design is jurisdiction-specific. [15] [16]
Growth and anaemia. Check iron studies/haemoglobin when growth, diet, or developmental risk suggests deficiency. Early anaemia has been linked to later developmental vulnerability in remote Aboriginal and Torres Strait Islander children. [18]
Avoid race-based laboratory “normal ranges.” Interpret results for the child in front of you. [2]
Management — Resuscitation
If the child is critically unwell, open the emergency pathway immediately. Cultural safety does not pause resuscitation; it shapes communication during it. [2]
- Support airway, breathing and circulation using standard paediatric emergency care. [12]
- Keep family present when safe; explain actions in plain language. [2]
- Call for Aboriginal Liaison/Health Worker support early when available. [2]
- For remote retrieval, coordinate with the local clinic and family decision-makers while stabilising. [12]
- Suspected ARF with carditis, severe respiratory failure, sepsis, or severe malnutrition needs senior escalation without delay. [15]
Never delay oxygen, fluids, antibiotics or retrieval to complete cultural paperwork. Do the life-saving steps and the respectful communication together. [3]
Management — Definitive & Stepwise
Definitive care is continuous, partnered and prevention-heavy. [1] [2]

Step 1 — Partnership as standard care
Link care with the family’s ACCHO when they have one. Invite Aboriginal Health Workers into planning. Community-controlled services improve access and trust for many families. Mainstream services still carry full responsibility for cultural safety. [2] [3]
Step 2 — Condition pathways that examiners test
Ear health. Treat acute disease, arrange hearing assessment, and loop in education supports for classroom hearing. Prevention includes reducing overcrowding harms where possible, smoke-free homes, timely primary care, and immunisation per schedule. [8] [9] [11]
Wet cough / chronic lung disease risk. Treat protracted wet cough seriously. Prevent recurrent infection, address environmental drivers, and refer when chronicity suggests bronchiectasis evaluation. Do not relabel all cough as asthma without evidence. [12] [13] [14]
Skin and strep sequelae. Treat the child and consider household transmission context. In ARF-endemic settings, integrate sore throat/skin infection care with local ARF prevention programmes and secondary prophylaxis systems when RHD/ARF is established. Use current local guidance for regimens rather than recalled doses. [15] [16]
Immunisation. Offer catch-up through trusted providers. Coverage reports are a prompt for system action, not family shaming. [17]
Development and anaemia. Correct nutritional deficiencies, treat hearing contributors, and arrange developmental supports early. School-entry vulnerability is modifiable when drivers are addressed. [18]
Step 3 — Advocacy and logistics
Write plans families can use. Fix transport, appointment timing, and inter-service letters. Advocate on housing and school supports when those determine medical outcomes. [1] [8]
Step 4 — Clinician practice change
Cultural safety training helps when it changes behaviour and power, not only knowledge quizzes. Reflect on bias. Invite feedback. Repair trust after system failures. [3] [4]
Specific Subtypes & Scenarios
Scenario map examiners use
- Urban Aboriginal child with recurrent OM: do not minimise because the family is metropolitan; arrange ear checks, audiology and school supports. [11]
- Remote child with chronic wet cough: infection-first reasoning, environmental history, specialist pathway for possible bronchiectasis. [12] [13]
- Possible ARF: urgent structured assessment and programme-linked follow-up; do not wait for “classic textbook only” features if concern is high. [15] [16]
- Family avoiding hospital after racism: acknowledge harm, offer AHW support, shared care with ACCHO, and concrete changes in who is in the room. [2] [5]
- Torres Strait Islander family: ask about specific cultural protocols; do not assume mainland Aboriginal protocols apply unchanged. [1]
- Adolescent access barriers: confidential, respectful care; address transport, shame, and service design barriers documented across Indigenous adolescent primary-care access literature. [2]
- Kinship/out-of-home care: cultural connection plans and clear medical handover across carers. [1]
- Telehealth outreach: local clinic nurse or AHW present with the family whenever possible. [2]
Complications & Pitfalls
- Treating non-attendance as family failure when transport, racism or clinic design is the barrier. [2]
- Over-investigating based on race, or under-investigating because “this is normal for the community.” [12]
- Excluding fathers, grandparents or kinship carers who hold decision authority. [1]
- Copying New Zealand Māori or North American Indigenous policy language without Australian community control context. [4]
- Inventing ARF prophylaxis doses under exam pressure instead of naming the local programme source. [15]
Prognosis & Disposition
Many infectious and developmental risks are modifiable with early continuous primary care, environmental improvement and trusted follow-up. Population gaps close only when clinical care joins structural reform and community control. [1] [8]
Disposition principles: [1] [2]
- Prefer shared care with the family’s ACCHO when available. [2]
- Give a written plan, safety-net advice, and named follow-up. [9]
- For chronic ear or lung disease, schedule longitudinal review and education supports. [11] [12]
- For ARF/RHD, link to the jurisdictional register/programme pathway and secondary prevention system. [15] [16]
- Document strengths, goals and cultural supports beside medical problems. [1]
Special Populations
Neonates and infants need continuity from maternal care, safe sleep counselling without shaming, early immunisation access, and skin/ear infection prevention in crowded households. [1] [17]
Remote communities need outreach logistics, environmental health partnership, and realistic appointment design. [8] [12]
Urban families may be invisible to services that only look for remoteness markers. Ask identity and offer the same quality pathways. [11]
Disability and neurodiversity assessments require culturally competent communication; families report that deficit framing damages trust. [2]
Out-of-home care and youth justice interfaces demand cultural connection planning and careful trauma-informed care. [1] [5]
Adolescents need privacy, respect, and services that remove access barriers rather than moralise non-attendance. [2]
Evidence, Guidelines & Regional Differences
Australian evidence spans cultural determinants, cultural safety reviews, racism and child health, ear-health consensus statements, indigenous lung disease cohorts, ARF/RHD literature, immunisation coverage reports, and nutrition-development links. Use these to defend practice, not to pathologise communities. [1] [2] [5] [9] [12] [15] [17] [18]
[2] [4] [9] [15]Cultural safety training interventions across Australia, Canada, New Zealand and the US show mixed design quality. Training is necessary but insufficient without service redesign and accountability. [4]
Exam Pearls
- Strengths-based history first: kinship, culture, community assets. [1]
- Hearing before labelling behaviour. [9] [11]
- Wet cough before default asthma labelling. [12]
- Shared written plans beat verbal-only advice when logistics are hard. [2]
- Emergency care and cultural safety run in parallel, not in sequence. [3]
References
- [1]Verbunt E Cultural determinants of health for Aboriginal and Torres Strait Islander people - a narrative overview of reviews. International journal for equity in health, 2021.PMID 34384447
- [2]De Zilva S Culturally safe health care practice for Indigenous Peoples in Australia: A systematic meta-ethnographic review. Journal of health services research & policy, 2022.PMID 34875923
- [3]McGough S There is no health without Cultural Safety: why Cultural Safety matters. Contemporary nurse, 2022.PMID 35014602
- [4]Hardy BJ Systematic review of Indigenous cultural safety training interventions for healthcare professionals in Australia, Canada, New Zealand and the United States. BMJ open, 2023.PMID 37793931
- [5]Kairuz CA Impact of racism and discrimination on physical and mental health among Aboriginal and Torres Strait islander peoples living in Australia: a systematic scoping review. BMC public health, 2021.PMID 34217243
- [6]Cave L Racial discrimination and child and adolescent health in longitudinal studies: A systematic review. Social science & medicine (1982), 2020.PMID 32143088
- [7]Cave L Racial discrimination and the health and wellbeing of Aboriginal and Torres Strait Islander children: Does the timing of first exposure matter? SSM - population health, 2019.PMID 31649999
- [8]DeLacy J The social determinants of otitis media in aboriginal children in Australia: are we addressing the primary causes? A systematic content review. BMC public health, 2020.PMID 32295570
- [9]Harkus S Routine ear health and hearing checks for Aboriginal and Torres Strait Islander children aged under 6 years attending primary care: a national consensus statement. The Medical journal of Australia, 2023.PMID 37716709
- [10]Harkus S Development of the national consensus statement on ear health and hearing check recommendations for Aboriginal and Torres Strait Islander children aged under 6 years attending primary care. BMC primary care, 2024.PMID 38486181
- [11]DeLacy J Ear health and hearing in urban Aboriginal children. Australian and New Zealand journal of public health, 2023.PMID 37517360
- [12]Chang AB Lung disease in indigenous children. Paediatric respiratory reviews, 2014.PMID 24958089
- [13]McCallum GB Comparison of Profiles of First Nations and Non-First Nations Children With Bronchiectasis Over Two 5-Year Periods in the Northern Territory, Australia. Chest, 2021.PMID 33964302
- [14]Laird P Prevalence of chronic respiratory diseases in Aboriginal children: A whole population study. Pediatric pulmonology, 2022.PMID 36098280
- [15]Parnaby MG Rheumatic fever in indigenous Australian children. Journal of paediatrics and child health, 2010.PMID 20854325
- [16]Rémond MG Screening for rheumatic heart disease in Aboriginal and Torres Strait Islander children. Journal of paediatrics and child health, 2013.PMID 23638751
- [17]Hull B Annual immunisation coverage report 2021. Communicable diseases intelligence (2018), 2023.PMID 37817316
- [18]Leonard D Early childhood anaemia more than doubles the risk of developmental vulnerability at school-age among Aboriginal and Torres Strait Islander children of remote Far North Queensland: Findings of a retrospective cohort study. Nutrition & dietetics : the journal of the Dietitians Association of Australia, 2020.PMID 31914484