Paeds · preventive-and-community-paediatrics
Drowning prevention and water safety
Also known as Water safety · Pool safety · Childhood drowning prevention · Submersion injury prevention · Life jacket counselling · Bath drowning prevention
Fellowship-level drowning prevention and water safety: WHO definition, age-specific hazards, layered prevention (supervision, barriers, flotation, swim skills, CPR readiness), bath and pool counselling, open-water and boating risk, immediate response after submersion, and regional practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
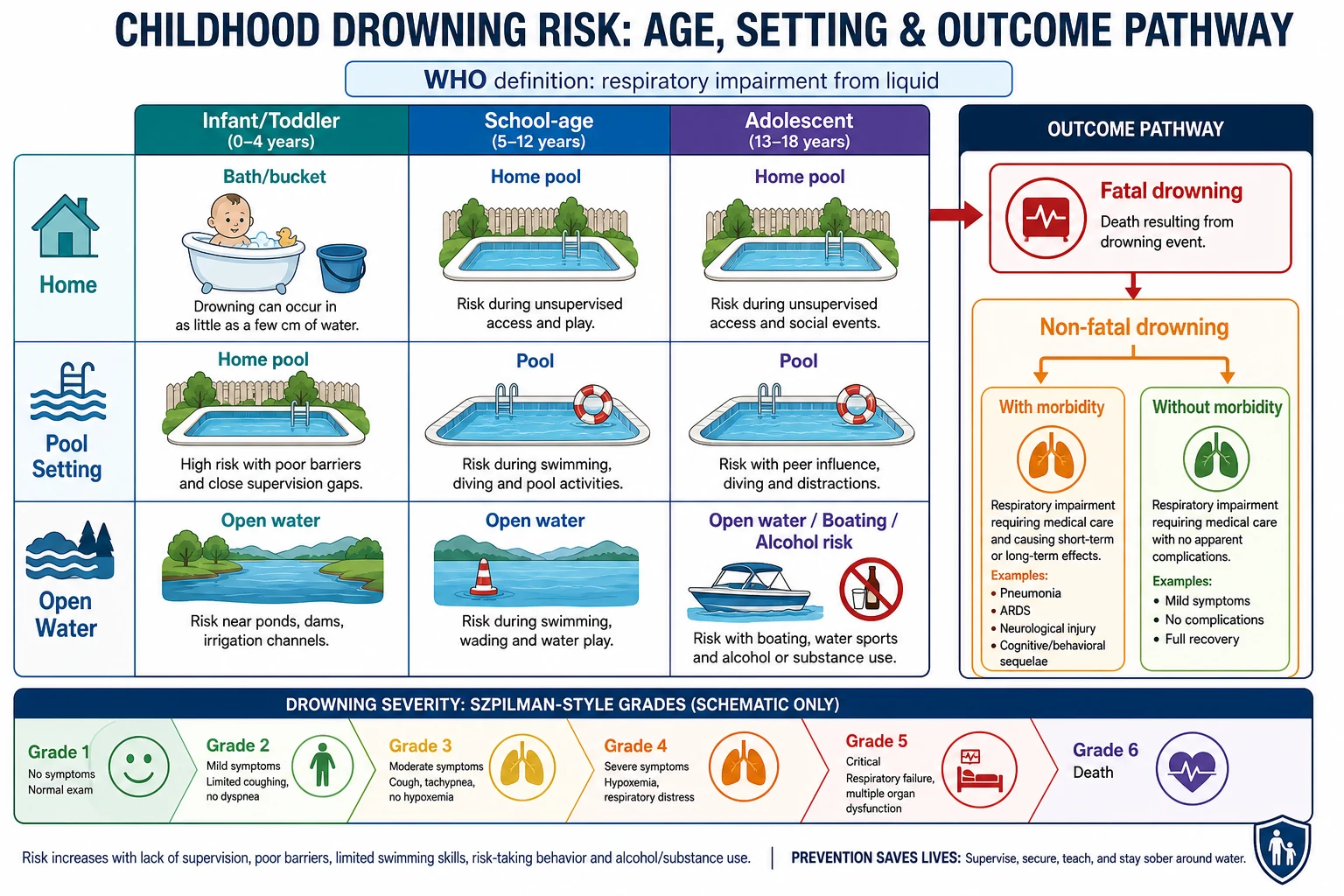
A parent asks, “Is the pool safe if we have a fence?” That question is the heart of this topic. Drowning means respiratory impairment from submersion or immersion in liquid. The child may die, survive with injury, or survive without lasting morbidity. The same word covers all of those outcomes, so drop older terms such as “near-drowning” in clinical speech and counselling. [3] [4]
Your job in general paediatrics is mostly prevention before any water event. You also need a clear emergency script if a child is found in water. Prevention works because drowning is a chain: access to water, inadequate protection, submersion, aspiration, hypoxaemia, then cardiac arrest. Break the early links and the later physiology never starts. [5] [15]
Classification
Sort the problem in three practical ways: who is at risk by age, where the water is, and what outcome followed a submersion. Those axes drive counselling and public health more usefully than a single severity number in clinic. [1] [20]
Terms you must keep clean
- Respiratory impairment from liquid submersion or immersion
- Includes fatal and non-fatal events
- Preferred modern clinical term
- Near-drowning confuses outcomes
- Dry drowning and secondary drowning are often misused in media
- Use clear time-course language instead of scare labels
- Szpilman grades help rescue-to-hospital thinking
- Utstein-style elements support consistent reporting
- Clinic counselling still starts with age and setting, not grade numbers
Infants and toddlers mainly drown in domestic water: baths, buckets, spas and backyard pools. School-age children still drown in pools and open water when supervision thins. Adolescents more often drown in open water, while boating, after alcohol, or during high-risk recreation. That shift must change your anticipatory guidance at each visit. [1] [19]
Epidemiology & Risk Factors
Drowning remains a leading cause of unintentional injury death in children worldwide. The exact rate varies by country, but the pattern is stable enough for fellowship teaching: young children in everyday water, older youth in open water, and large inequities by place and social risk. [1] [13] [20]
Australian work long ago showed how domestic pools dominate toddler drowning in urban settings. Bath drowning reviews continue to show infants and young children left alone, even briefly. Child-death reviews also show that the story is often a few minutes of distraction near familiar water, not a dramatic storm at sea. [9] [17] [18] [19]
Risk rises when layers fail together. An unfenced pool plus a phone distraction is worse than either alone. A child who can dog-paddle still needs a fence and a watcher. Rural dams, farm troughs, holiday rentals, and unfamiliar beaches add risk that families may not name unless you ask. Indigenous and socioeconomically disadvantaged communities may face higher exposure and fewer engineered protections; that is a systems problem, not a character judgement. [1] [7] [13]
Protective layers are continuous supervision appropriate to age, isolation barriers, personal flotation devices (PFDs) for boating and weak swimmers, swim competence as an adjunct, alcohol-free water recreation, and adults who can start CPR. No single layer is enough. [1] [2] [7]
Pathophysiology
Think of drowning as a hypoxaemia emergency that starts in liquid. After immersion, the child holds breath, then aspirates liquid or has laryngospasm. Aspirated fluid damages surfactant and floods alveoli. Gas exchange collapses. Hypoxaemia drives bradycardia and arrest more often than a primary cardiac event. [4] [15]
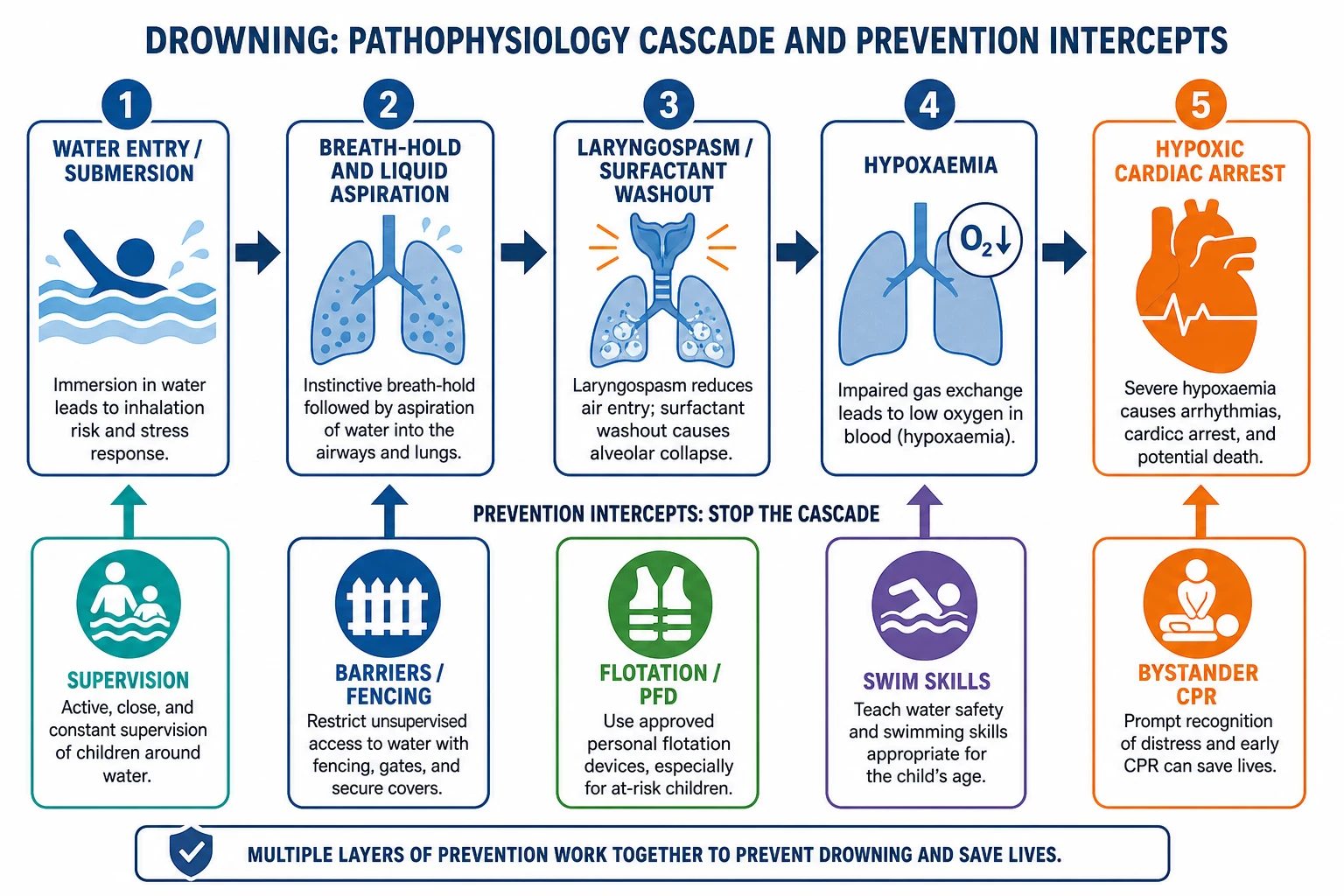
Only a modest volume of aspirated fluid can wreck oxygenation. That is why “the child only went under for a second” can still matter if breathing was impaired. Cold water adds hypothermia, which can protect the brain in rare prolonged submersions but also complicates resuscitation and must not create false hope or delay oxygen delivery. [4] [14] [15]
For prevention teaching, the physiology lesson is simple: stop access and stop unprotected immersion. Once liquid reaches the airway, the clock is about oxygen, not about draining mythical litres of water from the lungs. [5] [14]
Clinical Presentation
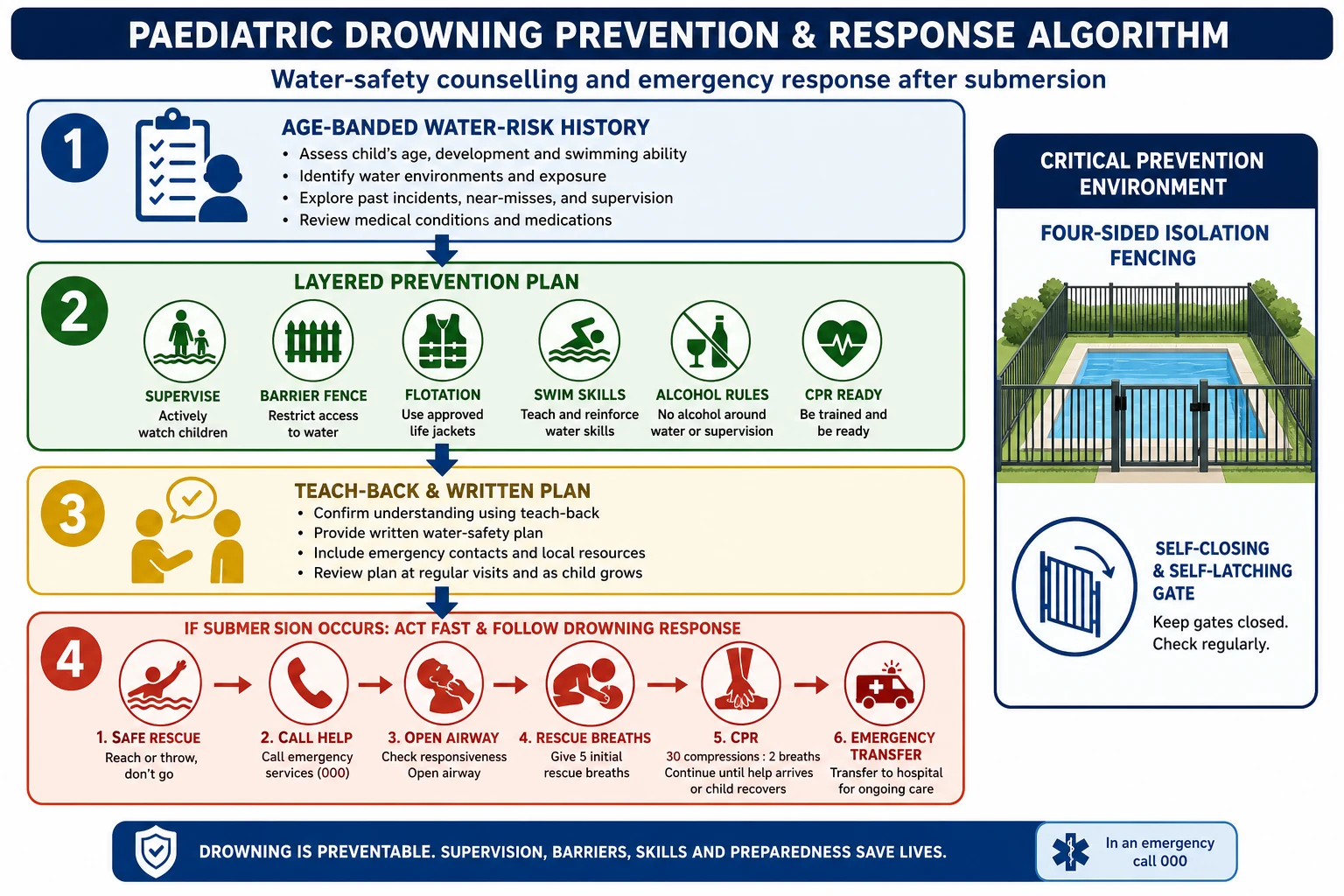
Most of the time this topic presents as a well child and a tired parent. You are not waiting for a drowning to teach water safety. Ask concrete questions: Is there a pool, spa, dam or pond at home or at grandparents? Is the fence four-sided with a working gate? Who watches bath time? Are there buckets or inflatable pools? Any boats, beaches or river trips planned? Can every adult caregiver start CPR? [1] [12]
Families also present after a near miss: a toddler found face-down in a bath, a child who slipped under at a party pool, an adolescent pulled from a river. Treat those stories as clinical events and as counselling triggers. The child in front of you may look well while the family is still in shock. [12] [20]
After true submersion, presentation ranges from asymptomatic to cough, tachypnoea, hypoxia, altered consciousness, hypothermia or cardiac arrest. Associated trauma, intoxication and seizure history matter. Silent drowning is the teaching point for parents: children often do not scream or splash dramatically. [4] [12]
Differential Diagnosis
After an immersion event, ask what started the cascade. Primary drowning with hypoxaemic arrest is commonest in children. Alternatives include a seizure that led to immersion, a cardiac event with secondary immersion, trauma, intoxication in adolescents, and non-accidental immersion. You keep safeguarding on the list without accusing every devastated parent. [4] [19]
In living children after brief events, distinguish true submersion impairment from simple water fright with no respiratory involvement. The history of underwater time, coughing, colour change and breathing effort matters more than labels. [12] [16]
Clinical & Bedside Assessment
Use an age-banded water audit, not a vague “be careful near water.” [1]
Five-minute water-safety assessment
Map the water
Bath, buckets, spa, home pool, neighbour pool, farm dam, beach, river, boat and holiday rentals.
Test supervision quality
Ask who watches, whether phones are put away, and whether infants/toddlers get touch supervision within arm’s reach.
Inspect barriers in words
Four-sided isolation fence, self-closing self-latching gate, no propped doors, pool-to-house access control.
Check flotation and skills
Fitted life jackets for boats; swim lessons as adjunct only; no reliance on arm bands as life-saving devices.
Plan the emergency
Phone access, who calls emergency services, and which adults can start paediatric CPR.
After a submersion, assess airway, breathing, circulation, consciousness, temperature and injuries. Listen for crackles, watch work of breathing, and check pulse oximetry. Document estimated underwater time, water type, rescue method and any CPR already given. If the story is inconsistent with the injuries, involve safeguarding pathways while still supporting the family. [12] [14] [19]
Investigations
Routine prevention visits need no tests. The investigation is the history and the home plan. Document advice and barriers that remain. [1]
After submersion, investigations follow physiology, not a fixed drowning panel. Use pulse oximetry for everyone with symptoms. Add blood gas when respiratory distress or altered consciousness is present. Chest radiograph helps when there are respiratory findings, but a normal early film does not prove the lungs are safe forever in a symptomatic child. Check glucose in altered consciousness. Consider ECG if arrhythmia or significant hypothermia is present. Toxicology may matter in adolescents. Trauma imaging follows trauma indications, not automatic whole-body scanning for every immersion. [12] [14] [20]
After fatal drowning, local death-investigation and multi-agency review pathways apply. Your role includes accurate history, family support and sibling safety planning. [16] [19]
Management — Resuscitation
If a child is unresponsive after water immersion, treat this as a hypoxaemic arrest until proven otherwise. Get the child to a safe surface. Open the airway. Start rescue breathing and CPR according to current paediatric basic and advanced life support. Call for emergency help early. Do not delay ventilation to perform unproven water-expulsion manoeuvres. [4] [14]
The drowning chain of survival is a useful teaching frame: prevent, recognise distress, provide flotation, remove from water, and give care as needed with an emphasis on ventilation and oxygenation. Bystander CPR quality often decides outcome before any hospital technology appears. In cold-water drowning, prolonged resuscitation may be appropriate under specialist guidance, but oxygen delivery still comes first. [5] [14]
Support caregivers during resuscitation. Avoid accusatory language at the scene. If later findings raise safeguarding concerns, activate the proper pathway without abandoning family care. [19]
Management — Definitive & Stepwise
Prevention is the definitive management for almost every outpatient encounter on this topic. Use a layered model and say so out loud so families do not pin everything on one intervention. [1] [2] [7]
1. Supervision matched to age. Infants and toddlers need continuous attention within arm’s reach in any water — baths included. “I was only gone a minute” is the classic fatal phrase. Designate a water watcher at gatherings. Phones and alcohol do not mix with watching. Older children still need eyes-on supervision that matches their real skill, not their confidence. [1] [9] [13]
2. Barriers that truly isolate water. For home pools, the high-yield design is four-sided isolation fencing that separates the pool from the house and play areas, with a self-closing, self-latching gate. Three-sided fencing that uses the house wall as the fourth side fails when a door is left open. Cochrane evidence supports pool fencing as a drowning-prevention intervention in children; legislation and compliance determine real-world effect. Spa covers, door alarms and pool alarms may add layers but do not replace isolation fencing and watching. [1] [6] [17]
3. Empty indoor water hazards. Empty baths, buckets and wading pools immediately after use. Toilet lids and bathroom doors matter for mobile toddlers. Never leave an infant in a bath seat or ring as if it were a safety device — these products have been linked to drowning when caregivers step away. [9] [10]
4. Flotation the right way. On boats and for weak swimmers in open water, use a correctly fitted life jacket or PFD appropriate to the child’s size and activity. Inflatable arm bands and toys are playthings, not life-saving devices. Observational work shows flotation use is often incomplete even in designated swim settings, so ask what the family actually wears, not what they own. [1] [11]
5. Swim skills as adjunct, not vaccine. Formal swimming lessons are associated with lower drowning risk in some case-control data for young children, but lessons do not make a child drown-proof. Teach skills when the child is developmentally ready, keep supervision and barriers, and never use lessons as permission to leave a toddler at a pool edge. [1] [8]
6. Adolescent-specific rules. Address open-water hazards, rips, cold water, peer pressure, night swimming and alcohol. Alcohol and water recreation are a lethal pair. Encourage group safety plans and refusal skills, not only slogans. [1] [19]
7. CPR readiness. Urge caregivers to learn paediatric CPR. After an event, early rescue breathing and compressions are the bridge to advanced care. [5] [14]
8. Teach-back and written plans. Ask the parent to restate tonight’s bath plan or this weekend’s pool plan. For holidays, write the rental-pool and beach rules before travel. [1] [2]
WATCHED
Specific Subtypes & Scenarios
Infant bath. One adult stays within arm’s reach for the whole bath. Gather towels and clothes first. Never leave a sibling “in charge.” Bath seats are not safety devices. [9] [10]
Toddler backyard pool. Confirm four-sided fencing and a gate that closes every time. Remove furniture that helps climbing. Do not prop the gate for convenience at parties. Toys left in the water attract toddlers. [1] [6] [17]
Farm and rural water. Dams, troughs, tanks and rivers need explicit discussion. Barriers and routines may differ from suburban pool fencing, so build a site-specific plan. [1] [18]
Beach and open water. Swim between flags where lifeguards operate when available. Discuss rips, currents and cold shock in plain language. Adolescents need a separate conversation about alcohol and night swimming. [1] [20]
Boating. Every child wears a fitted life jacket before the boat moves. Know the local carriage rules, but counsel beyond minimum legalism. [1] [11]
Disability, autism or epilepsy. Water can be both therapeutic and high risk. Use closer supervision ratios, secure barriers, flotation when appropriate, and seizure-action plans near water. [1]
Holiday rental. Unfamiliar pools and open gates are classic traps. Inspect the fence and gate on arrival before children unpack. [1]
Well-appearing child after brief submersion. Assess thoroughly. Observe according to local ED protocols when there was underwater time, coughing or any respiratory symptom. Safety-net for delayed breathing difficulty and fix the prevention failure before discharge. [12] [14]
Complications & Pitfalls
Other pitfalls: assuming drowning is noisy; promising that lessons make a child safe; missing safeguarding when immersion stories do not fit; and forgetting that grandparents’ pools and neighbour access matter as much as the child’s own backyard. [7] [19]
Prognosis & Disposition
Outcome after drowning turns on submersion duration, hypoxia duration, and quality of early CPR. Some children recover fully after brief events. Prolonged underwater time with delayed ventilation predicts severe hypoxic-ischaemic injury or death. Early prognostic certainty is often unwise in the first hours. [4] [14] [20]
After prevention counselling, disposition is usually home with a concrete layered plan. After non-fatal drowning, disposition ranges from ED observation to ward oxygen therapy to PICU respiratory and neuroprotective care. After a death, disposition includes family support, multi-agency review and immediate safety planning for other children in the household. [12] [19]
Special Populations
Indigenous children in some regions face higher drowning rates driven by exposure, access to safe swimming environments, and structural inequity. Partner with community programmes and avoid deficit-only framing. [1]
Rural and remote families need dam, tank and river plans, not only suburban pool talk. [18]
Migrant and refugee families may be new to local beaches, rips or backyard pool culture. Use interpreters and pictures. Do not assume shared water knowledge. [1] [13]
Children with disability or neurodiversity need individualised supervision ratios and secure environments. [1]
Socioeconomic disadvantage may mean unfenced rental pools or no money for lessons or jackets. Prioritise free high-yield actions: empty baths, continuous watching, closing doors, and local life-jacket loan schemes where they exist. [7] [13]
Out-of-home care requires the same water rules for every adult who supervises the child. Written plans travel better than one verbal chat. [1]
Evidence, Guidelines & Regional Differences
The paediatric prevention spine is the AAP Prevention of Drowning policy and its 2021 update: layered protection, fencing, supervision, swim skills as adjunct, life jackets, and CPR readiness. Systematic reviews support multi-component approaches; pool fencing has specific Cochrane support. Swimming-lesson evidence is encouraging but not absolute. WHO definition work and global status reporting keep the epidemiology honest. Resuscitation detail follows the AHA/AAP 2024 drowning focused update and broader drowning physiology reviews. [1] [2] [3] [6] [7] [8] [14]
Australia and Aotearoa New Zealand emphasise home-pool fencing legislation, Royal Life Saving public messaging, bath-safety teaching, and beach/open-water programmes. Brisbane pool studies historically shaped understanding of domestic-pool risk. Always check current state or territorial fencing standards rather than inventing measurements in an exam answer. [9] [17] [18]
Controversies to handle cleanly. How early formal lessons should start, how much residual risk remains after fencing, and how strongly to mandate life jackets in designated swim areas all attract debate. Your exam-safe answer: layers beat single interventions; barriers and continuous watching are non-negotiable for toddlers; lessons and jackets add protection but never replace the basics. [1] [7] [8] [11]
Exam Pearls
If you remember only one chain: unprotected water access → silent submersion → hypoxaemia. Your counselling removes access and adds watchers, barriers, flotation and CPR skill before that chain starts. That is the fellowship answer in one sentence. [1] [5] [15]
References
- [1]Denny, SA Prevention of Drowning Pediatrics, 2019.PMID 30877146
- [2]Denny, SA Prevention of Drowning Pediatrics, 2021.PMID 34253571
- [3]van Beeck, EF A new definition of drowning: towards documentation and prevention of a global public health problem Bulletin of the World Health Organization, 2005.PMID 16302042
- [4]Szpilman, D Drowning New England Journal of Medicine, 2012.PMID 22646632
- [5]Szpilman, D Creating a drowning chain of survival Resuscitation, 2014.PMID 24911403
- [6]Thompson, DC Pool fencing for preventing drowning in children Cochrane Database of Systematic Reviews, 2000.PMID 10796742
- [7]Wallis, BA Interventions associated with drowning prevention in children and adolescents: systematic literature review Injury Prevention, 2015.PMID 25189166
- [8]Brenner, RA Association between swimming lessons and drowning in childhood: a case-control study Archives of Pediatrics & Adolescent Medicine, 2009.PMID 19255386
- [9]Peden, AE Unintentional fatal child drowning in the bath: A 12-year Australian review (2002-2014) Journal of Paediatrics and Child Health, 2018.PMID 29417672
- [10]Rauchschwalbe, R The role of bathtub seats and rings in infant drowning deaths Pediatrics, 1997.PMID 9310534
- [11]Quan, L Use of life jackets and other types of flotation for in-water recreation in designated swim areas in Washington State Injury Prevention, 2018.PMID 28424217
- [12]Mott, TF Prevention and Treatment of Drowning American Family Physician, 2016.PMID 27035042
- [13]Jullien, S Prevention of unintentional injuries in children under five years BMC Pediatrics, 2021.PMID 34496772
- [14]Dezfulian, C 2024 American Heart Association and American Academy of Pediatrics Focused Update on Special Circumstances: Resuscitation Following Drowning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation, 2024.PMID 39530204
- [15]Bierens, JJ Physiology Of Drowning: A Review Physiology (Bethesda), 2016.PMID 26889019
- [16]Idris, AH 2015 revised Utstein-style recommended guidelines for uniform reporting of data from drowning-related resuscitation: An ILCOR advisory statement Resuscitation, 2017.PMID 28728893
- [17]Pitt, WR Childhood drowning and near-drowning in Brisbane: the contribution of domestic pools Medical Journal of Australia, 1991.PMID 2034145
- [18]Nixon, J Fifteen years of child drowning--a 1967-1981 analysis of all fatal cases from the Brisbane Drowning Study and an 11 year study of consecutive near-drowning cases Accident Analysis & Prevention, 1986.PMID 3730093
- [19]Quan, L Analysis of paediatric drowning deaths in Washington State using the child death review (CDR) for surveillance: what CDR does and does not tell us about lethal drowning injury Injury Prevention, 2011.PMID 21278094
- [20]Abelairas-Gómez, C Drowning: epidemiology, prevention, pathophysiology, resuscitation, and hospital treatment Emergencias, 2019.PMID 31347808