Paeds · preventive-and-community-paediatrics
Global child health and sustainable paediatric care
Also known as International child health · Global paediatrics · SDG 3.2 child survival · IMCI · Continuum of care maternal newborn child health · Sustainable healthcare paediatrics · Planetary health children · Under-5 mortality
Fellowship-level approach to global child health and sustainable paediatric care: under-5 and neonatal mortality metrics and SDG 3.2, major preventable causes, continuum-of-care packages including IMCI and essential newborn care, care of newly arrived children, and climate-smart low-carbon clinical practice.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a registrar in two rooms on the same day. In the first, a toddler from a refugee family presents with fever and incomplete records. In the second, a hospital meeting asks how to cut theatre waste without harming safety. Both rooms are global child health. The specialty is not diseases of faraway places. It is the science and practice of preventing avoidable child death and disability wherever the child lives — including inside high-income countries — and of designing care that does not borrow against the child's future climate. [5] [14] [16]
Global child health integrates clinical paediatrics, epidemiology, health systems and social determinants. Tropical paediatrics is a narrower pathogen and ecology lens. International health historically meant programmes run across borders. Use the broader frame: causes of death, coverage of proven interventions, quality of care, equity, and planetary boundaries of health-care delivery. [2] [8]
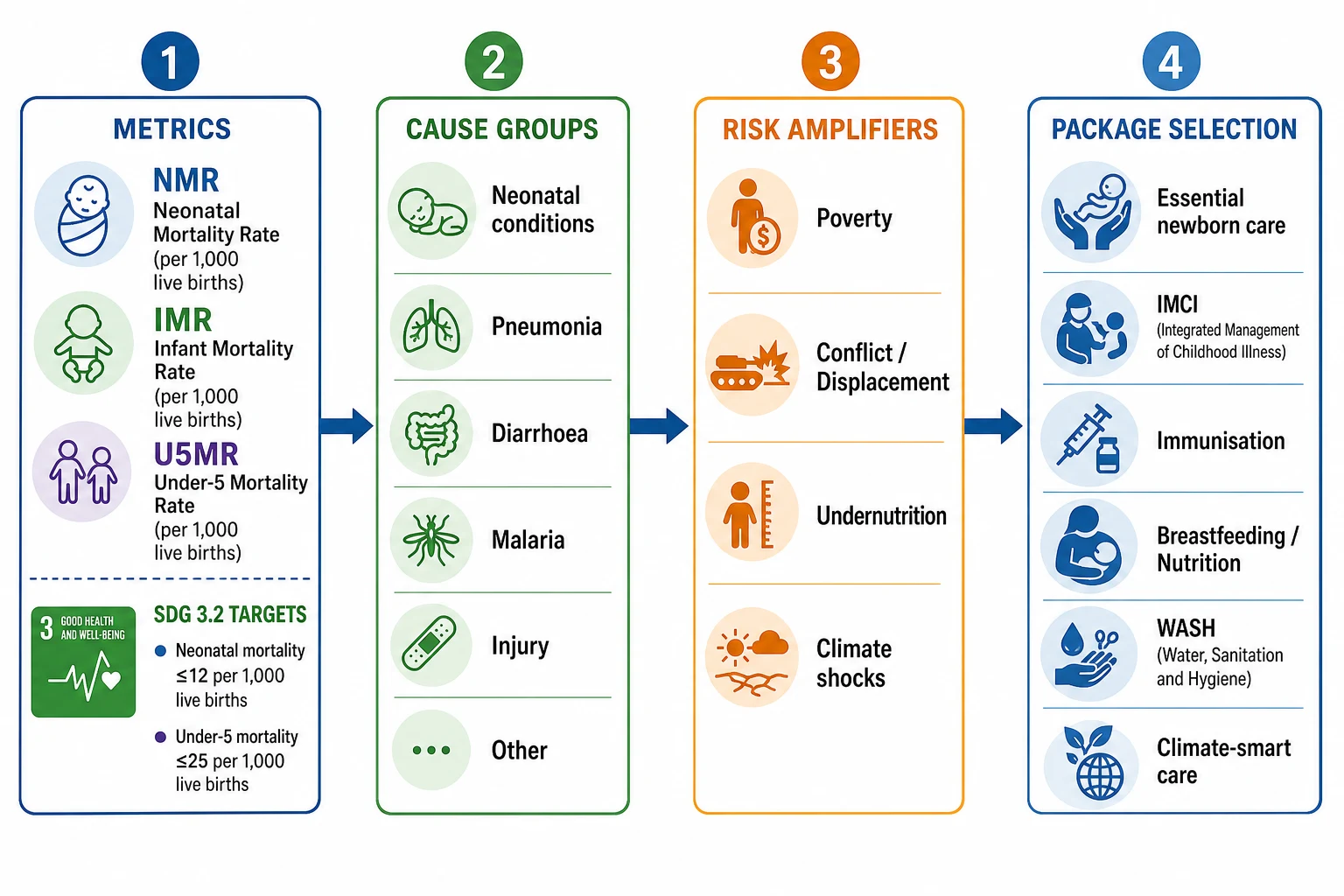
Mortality definitions you must say cleanly: [6]
| Metric | Definition (standard teaching) |
|---|---|
| Neonatal mortality rate (NMR) | Deaths in first 28 days per 1000 live births |
| Infant mortality rate (IMR) | Deaths under 1 year per 1000 live births |
| Under-5 mortality rate (U5MR) | Deaths under 5 years per 1000 live births |
Sources include vital registration where strong, and household surveys plus model-based estimates (for example UN IGME methods) where registration is incomplete. Always state uncertainty when using modelled numbers. [6]
SDG 3.2 asks countries to end preventable deaths of newborns and children under 5, with all countries aiming to reduce neonatal mortality to at least as low as 12 per 1000 live births and under-5 mortality to at least as low as 25 per 1000 live births. Those numbers are national target floors for exam language, not a claim that every district has already met them. [5] [6]
Classification
Organise the field the way a programme planner and a clinician both can use it: metrics → causes → amplifiers → packages → system level. [4] [8]
Continuum of care is the service-delivery spine. Kerber and colleagues moved it from slogan to design: link preconception and antenatal care, skilled birth attendance, postnatal care, infancy and childhood services so mothers and children do not fall through gaps between vertical programmes. [8]
Intervention packages (exam clusters): [8]
- Essential newborn care and small or ill newborn care — warmth, hygiene, early breastfeeding initiation, resuscitation readiness, infection prevention, kangaroo mother care concepts where indicated. [7] [9]
- IMCI and primary care case management for the sick under-5 — classify severity, treat what first-level care can treat, refer with pre-referral treatment when needed, counsel caregivers, follow up. [10]
- Prevention platform — immunisation, exclusive breastfeeding, complementary feeding, micronutrients, malaria prevention where endemic, water/sanitation/hygiene (WASH). [1] [11] [13]
- Sustainable clinical practice — reduce low-value diagnostics, waste and high-carbon processes while protecting outcomes. [15] [16]
Epidemiology & Risk Factors
Under-5 mortality fell substantially from 1990 to 2015, yet progress was uneven. You and colleagues showed large absolute declines with scenario-based projections that still left many countries off-track for ambitious 2030 goals without accelerated action. Residual deaths concentrate in sub-Saharan Africa and Southern Asia, and within countries among poorer, rural, conflict-affected and less educated households. [6] [12]
Cause-of-death series by Black, Liu and colleagues remain the fellowship backbone: neonatal causes (preterm complications, intrapartum-related events or asphyxia, neonatal sepsis/meningitis/tetanus, congenital conditions) plus pneumonia, diarrhoea and malaria where transmission continues, with injury and other causes completing the picture. As overall mortality falls, the neonatal share of under-5 deaths rises — which is why Every Newborn priorities matter for SDG-era exams. [2] [3] [4] [5] [7]
Risk amplifiers you must name without euphemism: poverty and food insecurity; maternal undernutrition and limited education; delayed care-seeking and transport failure; commodity stock-outs; workforce shortages; urban slum crowding; displacement and conflict; climate shocks that destroy food systems and health infrastructure. [12] [13]
The double burden of malnutrition — undernutrition coexisting with rising overweight and obesity in many low- and middle-income settings — is now part of the global child-health map, not a high-income-only story. [13]
Pathophysiology
Start with the newborn. Transition from intrauterine life demands breathing, circulatory reorganisation, thermal control and infection defence in hours. Preterm lungs and brain, birth asphyxia, and early-onset infection explain why the first days carry outsized mortality. Evidence-based neonatal packages save lives because they target those mechanisms with warmth, resuscitation readiness, feeding support and infection control rather than exotic technology alone. [7] [9]
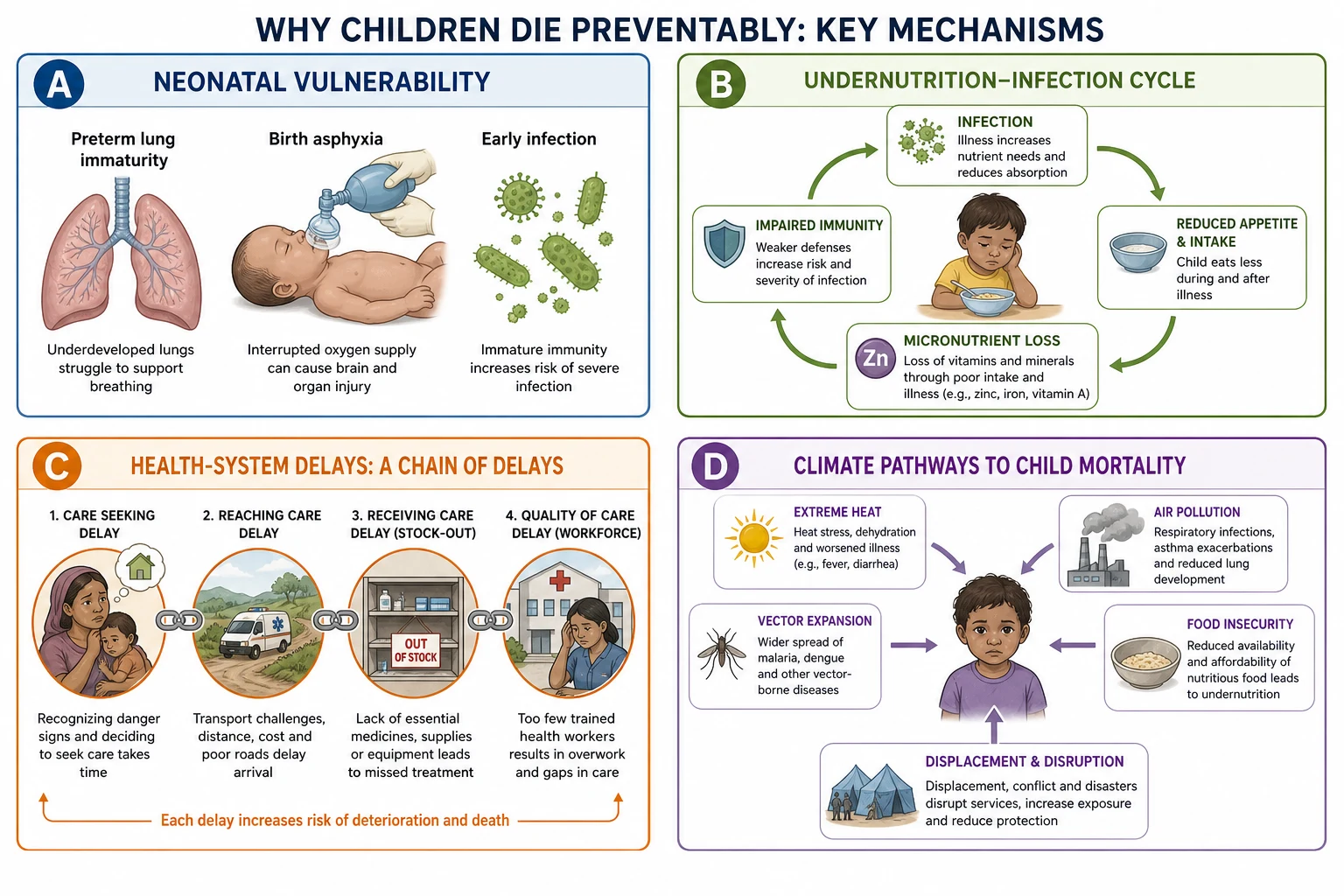
Next, the infection–undernutrition cycle. Infection raises metabolic demand and reduces intake. Undernutrition impairs barrier and immune function, prolongs illness and multiplies case fatality from pneumonia and diarrhoea. That is why nutrition interventions and infection case management are not competing priorities. [13]
Then the system pathway. A child can die from a treatable pneumonia because the caregiver did not recognise danger signs, transport failed, oxygen was unavailable, or antibiotics were stocked out. Population physiology includes supply chains and trust. Countdown tracking made coverage and equity visible as clinical variables. [12]
Finally, climate and environment. Children have higher minute ventilation per kilogram, more outdoor time, developing immune and thermoregulatory systems, and long latency for harm. Heat, air pollution, changing vector ecology, crop failure and displacement are paediatric pathways. Health systems themselves emit carbon; operating theatres are a documented hotspot, and national health services such as NHS England have quantified sector footprints — so sustainable paediatric care is mechanism-aware practice, not aesthetics. [15] [16]
Clinical Presentation
In first-level care using an IMCI logic, presentations cluster: cough or difficult breathing; diarrhoea; fever; ear problems; malnutrition or anaemia risk; and in young infants, a separate danger-sign set (poor feeding, convulsions, severe chest indrawing, fever or hypothermia, movement only when stimulated). The art is rapid severity classification, not encyclopaedic differentials on day one. [10]
Neonates present with poor feeding, respiratory distress, temperature instability, lethargy, seizures or omphalitis after home or facility birth — treat these as emergencies until proven otherwise. [7]
Newly arrived migrant and refugee children often look well while carrying incomplete immunisation, interrupted chronic care, TB exposure risk, eosinophilia from geohelminths depending on origin, developmental catch-up needs, and trauma-related mental health symptoms. The presentation is frequently administrative — no records — until you take a structured migration history. [14]
Climate-linked presentations in ordinary practice include heat illness, asthma flares with air pollution or wildfire smoke, gastroenteritis after flood water contamination, and injury after extreme weather. Name the pathway in the problem list when it changes advice. [16]
Differential Diagnosis
| Problem representation | Global-health-favouring clues | Must-not-miss alternatives |
|---|---|---|
| Fever + cough + fast breathing | Peak under-5 pneumonia burden settings; hypoxia; incomplete immunisation | Foreign body, cardiac failure, TB, malaria with respiratory distress |
| Watery diarrhoea + sunken eyes | Epidemic season, unsafe water, delayed ORS | Surgical abdomen, DKA, adrenal crisis, toxin |
| Failure to thrive | Food insecurity, conflict, caregiver illness | Coeliac, IBD, congenital heart disease, neglect/safeguarding |
| Incomplete vaccines | Displacement, stock-out, access cost | True medical contraindication (rare), documented refusal with counselling needs |
| Chronic cough | High TB incidence origin, household contact | Asthma, protracted bacterial bronchitis, aspiration |
Do not let tropical framing steal the case. Worldwide, the common killers remain newborn complications, pneumonia and diarrhoea more often than rare parasites. Malaria matters enormously where endemic — geography and season belong in the differential, not as decoration. [3] [5]
Clinical & Bedside Assessment
Open with partnership. For a local sick under-5: "I will check for danger signs first, then we will decide treatment or referral together." For a newly arrived family: "I will not judge how you arrived. I need a clear timeline so we can protect your child's lungs, growth and vaccines." Shame blocks disclosure of illegal work, detention, traditional remedies or missed doses. [10] [14]
Bedside global-child-health assessment (any setting)
Emergency screen
Airway, breathing, circulation, disability, exposure; IMCI emergency and priority signs; glucose if altered.
Age-band history
Neonatal events, feeding, immunisation, growth, development, chronic disease, medications.
Context history
Housing, water and sanitation, food security, conflict or displacement, school, caregiver mental health, legal barriers.
Exam that changes action
Work of breathing and SpO2 if available, hydration, nutrition (WHZ/MUAC where used), fever focus, skin, ears, abdomen, neurology.
Records and catch-up
Vaccine card, TB contacts, prior admissions, developmental services, interpreter needs.
Plan with teach-back
Danger signs to return for, ORS use, follow-up date, referral logistics, social supports.
Use WHO growth standards language for international comparison. In acute malnutrition programmes, mid-upper arm circumference and weight-for-height z-scores guide classification — apply local programme thresholds rather than inventing numbers. Developmental and mental-health screening after forced migration is part of the examination, not an optional extra. [13] [14]
Investigations
IMCI was designed so first-level workers can save lives without waiting for laboratories. That is a feature. Investigations become essential when they change referral, antimicrobial choice, TB decisions, or malnutrition complication management. [10]
Useful in many settings when available: pulse oximetry for pneumonia severity; glucose in severe illness; haemoglobin; malaria rapid test or microscopy where endemic; HIV testing per local PMTCT and paediatric guidelines; molecular TB testing when indicated. [10] [14]
For newly arrived children in high-income clinics: prioritise history, growth, development, vision and hearing as indicated, immunisation catch-up planning, and risk-based infectious screening guided by origin and immigrant-child frameworks — not a shotgun panel on every child. Chest imaging and TB testing follow risk, symptoms and local public-health pathways. [14]
Population investigations clinicians should interpret: DTP3 and measles coverage, exclusive breastfeeding rates, skilled birth attendance, ORS use in diarrhoea, antenatal care attendance, and out-of-pocket spending that blocks care. These are the vital signs of a child-health system. [12]
Management — Resuscitation
Universal paediatric emergency care comes first. Oxygen for hypoxia, airway support, fluid resuscitation matched to shock physiology, seizure control, correction of hypoglycaemia, and urgent antibiotics for suspected sepsis are not global-health alternatives to good medicine — they are good medicine. [10]
IMCI emergency logic asks you to recognise the child who cannot wait: not breathing or gasping; severe respiratory distress; shock; coma or convulsions; severe dehydration. Give pre-referral treatment your system authorises, keep the child warm, prevent hypoglycaemia in the small infant, and move. Do not invent drug doses from memory when your local formulary or WHO pocket book is the operational source — state the principle and the source you will follow. [10]
Severe acute malnutrition with complications is a special resuscitation lane: hypothermia, hypoglycaemia, careful fluids, infection treatment and feeding protocols differ from routine gastroenteritis pathways. Escalate early. [13]
In disasters, use paediatric mass-casualty triage principles your hospital trains, protect caregivers when possible, and restore immunisation and feeding supports as soon as acute trauma care allows. [12]
Management — Definitive & Stepwise
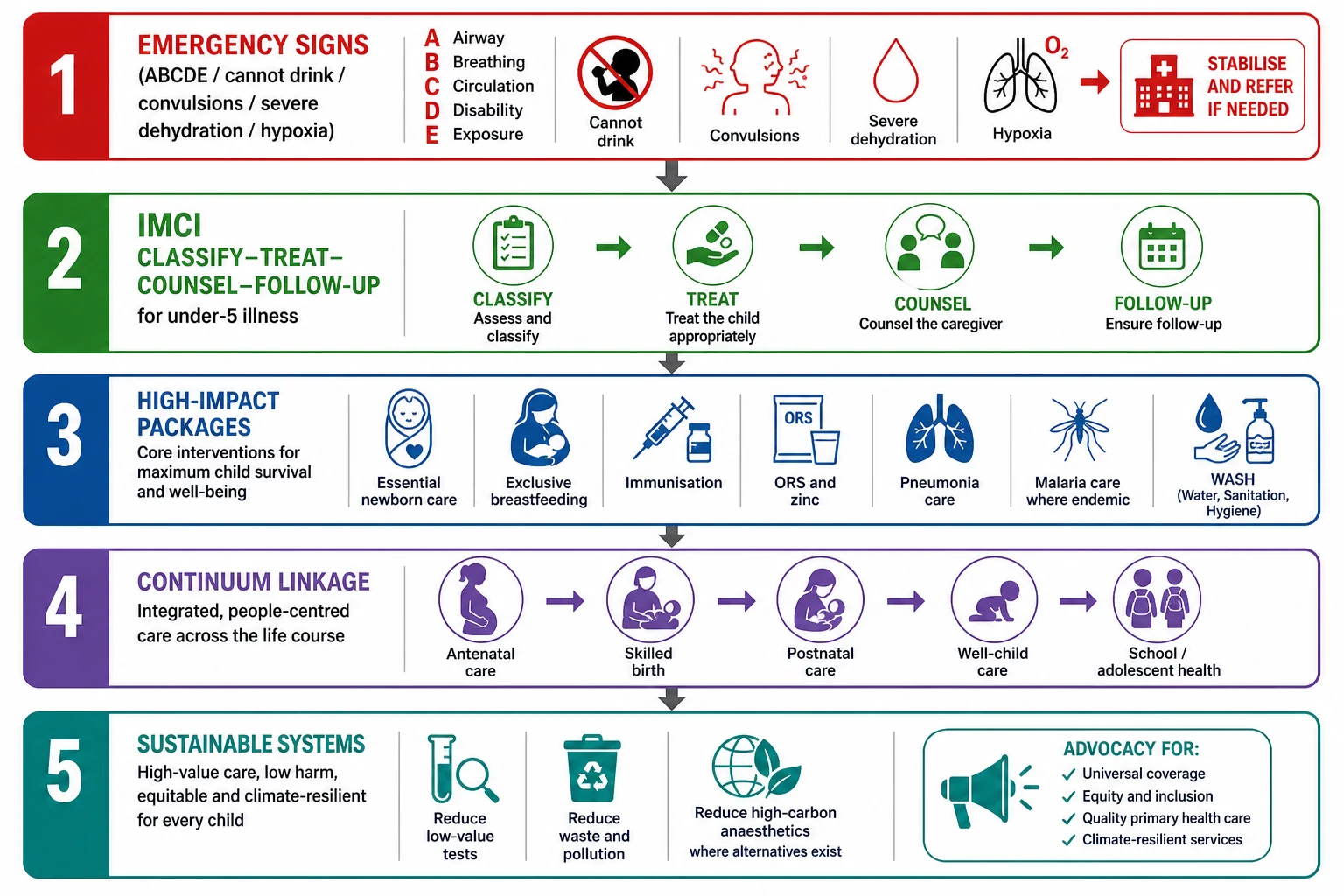
Step 1 — Save the child in front of you. Treat dehydration with ORS when the child can drink; use IV or IO pathways for severe dehydration or shock per local protocol. Treat pneumonia severity tiers with oxygen and antibiotics per guideline. Treat malaria where confirmed or endemic. Feed and warm the neonate. [1] [10]
Step 2 — Deliver packages with known impact. Jones and colleagues framed how many deaths are preventable with existing interventions. Darmstadt quantified newborn lives saveable with cost-effective packages. Scale what works: exclusive breastfeeding, complementary feeding, immunisation, clean delivery, neonatal resuscitation readiness, antibiotics for sepsis and pneumonia, ORS and zinc for diarrhoea, insecticide-treated nets and effective antimalarials where relevant. [1] [9] [11]
Step 3 — Use IMCI as an operating system, not a poster. Gera's Cochrane review supports IMCI for some process and mortality-related outcomes while highlighting implementation quality as the limiting reagent. Train, supply, supervise, and link community practices (care-seeking, home ORS, feeding). [10]
Step 4 — Stitch the continuum. Antenatal iron and folate and infection screening, skilled birth attendance, postnatal checks, newborn care, well-child visits, school health and adolescent services must hand patients to each other. Vertical campaigns fail when the hand-offs fail. [8] [12]
Step 5 — Practise sustainable paediatric care. Health care contributes measurable greenhouse gas emissions. MacNeill mapped operating-theatre footprints across health systems; Tennison quantified NHS England's carbon profile and response levers. At clinician level: avoid low-value tests and admissions; prefer reusable systems where infection control allows; reduce anaesthetic gas waste with modern practice; deprescribe; choose telehealth when clinically equivalent; design clinics that do not require repeated high-carbon travel for low-acuity follow-up. Sustainability is quality improvement with a longer time horizon. [15] [16]
Step 6 — Advocate. Coverage, equity and quality need financing and political attention. Countdown taught that measurement drives accountability. Your clinic data on missed immunisations, interpreter gaps and housing instability are advocacy instruments. [12]
PACKAGES — high-yield global child survival memory hook
Specific Subtypes & Scenarios
Rural first-level clinic, febrile toddler with fast breathing. Classify pneumonia severity; give oxygen if available for severe disease; antibiotics per protocol; counsel danger signs; arrange referral transport if IMCI severe classification. Do not wait for a chest radiograph that does not exist. [10]
Home birth, day-3 neonate, poor feeding. Think sepsis and dehydration; urgent assessment; antibiotics and supportive care per neonatal pathway; review tetanus protection and clean cord practices for future births; plan facility delivery counselling. [7] [9]
Refugee child, age 4, no vaccine card, well today. Build a catch-up schedule using national rules for unknown history; screen growth and development; take TB exposure and symptom history; address dental, vision, hearing, mental health and school entry needs; use interpreters; avoid unnecessary separation of child and caregiver during visits. [14]
Urban LMIC clinic: stunted preschooler and overweight adolescent sibling. Address food quality, marketing, activity space and maternal health — the double burden lives in one household. [13]
Hospital green team asks paediatrics to cut emissions. Start with low-value care reduction, anaesthetic gas stewardship in children's theatres, supply-chain waste audits, and asthma device choices where evidence-based alternatives exist — measure, do not performative-recycle. [15] [16]
Heatwave weekend. Prioritise infants, athletes, children on psychotropics or with chronic disease; counsel hydration, shade, never leaving children in cars; surge plan for ED heat illness. [16]
Complications & Pitfalls
- Treating global health as overseas elective tourism rather than equity science. [12]
- Chasing rare pathogens while under-treating pneumonia, diarrhoea and neonatal sepsis. [3]
- Running vertical programmes that ignore primary care and referral transport. [8]
- Declaring success by coverage percentages while quality (oxygen, correct antibiotic, respectful care) is poor. [12]
- Missing safeguarding and caregiver mental health inside malnutrition labels. [13]
- Over-investigating the newly arrived well child and delaying immunisation catch-up. [14]
- Expanding disposable-heavy, low-value pathways that raise carbon cost without outcome gain. [15] [16]
- Inventing local drug doses or national cut-offs under exam pressure — name the guideline you follow. [10]
Prognosis & Disposition
At population level, prognosis tracks coverage × quality × equity of known interventions more than discovery of new silver bullets. Countries that raised immunisation, skilled birth care, breastfeeding support and case management saw large mortality falls; stalled places share conflict, inequity and weak primary care. [6] [12]
For the individual child: home with clear danger-sign teaching and follow-up; same-day primary care review; referral hospital; or critical care. Disposition fails when the caregiver cannot afford transport or leave work — solve the barrier or the plan is fiction. [10]
Long-term, early undernutrition and recurrent infection link to stunting, poorer schooling and later NCD risk. Climate harms accumulate across childhood. Sustainable systems are therefore prognosis tools for the next cohort, not optional branding. [13] [16]
Special Populations
Small vulnerable newborns (preterm, small-for-gestational-age, low birth weight) drive a large share of neonatal deaths and stillbirths; they need the Every Newborn agenda, not only PICU technology narratives. [7]
Children with disability in low-resource settings face exclusion from school and rehabilitation; include function and participation in plans. [12]
Indigenous children within high-income countries experience health gaps that are structural, not cultural blame — coordinate with dedicated culturally safe care topics rather than token paragraphs. [12]
Migrant, refugee and asylum-seeking children need trauma-informed, language-accessible care, careful infectious and mental-health assessment, and protection from detention-related harm where relevant. Linton's AAP clinical report is a practical high-income-clinic anchor. [14]
Adolescents add sexual and reproductive health, injury, mental health, climate anxiety and transition of chronic disease — still under-measured in classic under-5 metrics. [12]
Evidence, Guidelines & Regional Differences
Evidence pillars. Jones (2003) estimated preventable child deaths with existing interventions. Black and Liu series defined cause structure over time and framed SDG priorities as neonatal and infectious burdens evolved. You quantified levels and trends toward 2030 scenarios. Darmstadt and Lawn shifted attention to newborn packages and the Every Newborn agenda. Kerber operationalised the continuum. Gera's Cochrane review tempers IMCI enthusiasm with implementation realism. Victora's breastfeeding and Countdown papers bind biology to accountability. Black 2013 frames undernutrition and the emerging double burden. [1] [2] [5] [6] [7] [8] [9] [10] [11] [12] [13]
Sustainability evidence. MacNeill's multi-system theatre footprint study and Tennison's NHS England carbon assessment give examiners concrete numbers that health care is not climate-neutral. Pair them with AAP climate and child health policy direction for advocacy language. [15] [16]
[14] [16]Controversies. How far IMCI alone moves mortality without health-system investment; vertical versus horizontal financing; whether high-income hospitals should prioritise carbon metrics alongside safety; and how aggressively to screen asymptomatic migrant children for infections — always balance benefit, stigma and cost. [10] [14] [15]
Exam Pearls
- Lead with preventable causes + packages + equity, not a travel diary. [1] [5]
- Quote SDG 3.2 targets: neonatal ≤12/1000 and under-5 ≤25/1000 live births as national aims. [5] [6]
- As U5MR falls, neonatal deaths become a larger share — say it. [5] [7]
- Continuum of care = linked service delivery across pregnancy to childhood. [8]
- IMCI = classify, treat, counsel, follow up + community + system supports. [10]
- Breastfeeding is clinical therapy and population survival policy. [11]
- Newly arrived child: vaccines, TB risk, growth, development, mental health, interpreter, legal stressors. [14]
- Sustainable care starts by cutting low-value activity; theatres and national health systems have measurable footprints. [15] [16]
- Never invent doses: state agent class and per WHO pocket book or local formulary. [10]
- Global health skills are local equity skills. [12]
References
- [1]Jones G How many child deaths can we prevent this year? Lancet, 2003.PMID 12853204
- [2]Black RE Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet, 2010.PMID 20466419
- [3]Liu L Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet, 2012.PMID 22579125
- [4]Liu L Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet, 2015.PMID 25280870
- [5]Liu L Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet, 2016.PMID 27839855
- [6]You D Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet, 2015.PMID 26361942
- [7]Lawn JE Every Newborn: progress, priorities, and potential beyond survival. Lancet, 2014.PMID 24853593
- [8]Kerber KJ Continuum of care for maternal, newborn, and child health: from slogan to service delivery. Lancet, 2007.PMID 17933651
- [9]Darmstadt GL Evidence-based, cost-effective interventions: how many newborn babies can we save? Lancet, 2005.PMID 15767001
- [10]Gera T Integrated management of childhood illness (IMCI) strategy for children under five. Cochrane Database of Systematic Reviews, 2016.PMID 27378094
- [11]Victora CG Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet, 2016.PMID 26869575
- [12]Victora CG Countdown to 2015: a decade of tracking progress for maternal, newborn, and child survival. Lancet, 2016.PMID 26477328
- [13]Black RE Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet, 2013.PMID 23746772
- [14]Linton JM Providing Care for Children in Immigrant Families. Pediatrics, 2019.PMID 31427460
- [15]MacNeill AJ The impact of surgery on global climate: a carbon footprinting study of operating theatres in three health systems. Lancet Planetary Health, 2017.PMID 29851650
- [16]Tennison I Health care's response to climate change: a carbon footprint assessment of the NHS in England. Lancet Planetary Health, 2021.PMID 33581070