Paeds · preventive-and-community-paediatrics
Housing insecurity, food insecurity and child health
Also known as Food insecurity children · Housing insecurity children · Hunger Vital Sign · Material hardship paediatrics · Homelessness child health · Social determinants food housing · Household food security
Fellowship-level approach to childhood food and housing insecurity: definitions and USDA severity, Hunger Vital Sign screening, multi-domain housing risk, medical sequelae, clinic-to-community management, safeguarding boundaries, and regional programme differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
You will meet these families in every setting: well-child clinic, ED, ward discharge, school health. The child may look well. The story is in the rent arrears, the empty fridge, the third address this year, or the parent who skips meals so the children can eat. Material hardship is a core paediatric social determinant. It drives infection, growth problems, developmental risk, mental health burden and avoidable hospital use. [2] [3] [11]
Food security means reliable access to enough safe, nutritionally adequate food for an active, healthy life. Food insecurity means that access is limited or uncertain. The US Department of Agriculture (USDA) Household Food Security Survey Module (HFSSM) ranks households as high, marginal, low or very low food security. Low and very low map to food insecurity; marginal is not a free pass — it still associates with adverse outcomes. [1] [8]
Housing insecurity is broader than street homelessness. Useful clinical domains are affordability (rent/mortgage stress), stability (moves, eviction threat), quality and safety (cold, damp, mould, pests, lead hazards), crowding, and homelessness (shelter, cars, couch-surfing, no fixed abode). Name the domain you are acting on. [4] [11]
Classification
Organise every case on three axes: food-security severity, housing-insecurity domain, and medical urgency tonight. Those axes decide whether you need emergency food, same-day shelter, growth work-up, or scheduled navigation. [1] [4]
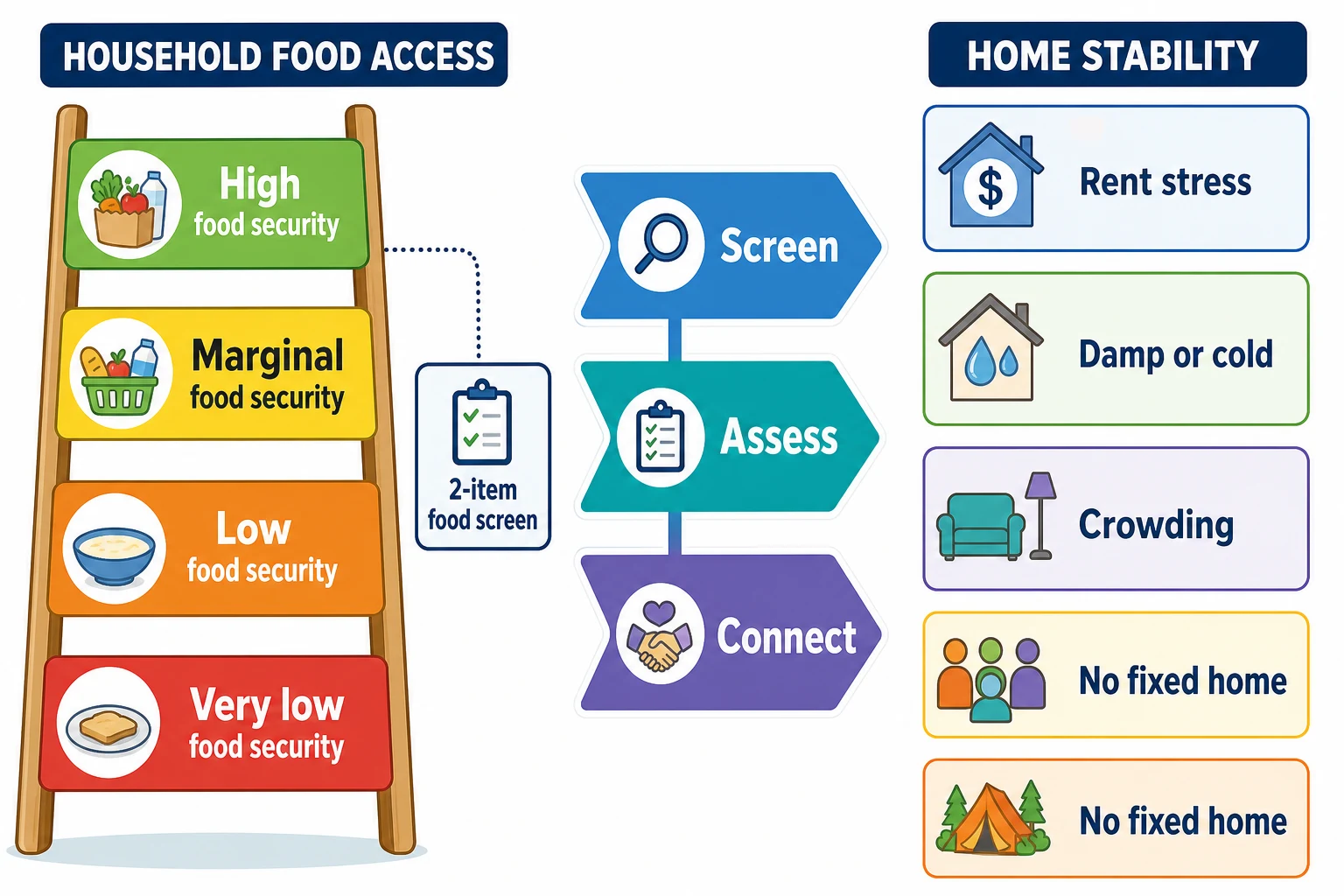
Hunger Vital Sign (Hager 2-item screen). Two questions, adapted from HFSSM, identify households at risk for food insecurity with good sensitivity for clinical use. An affirmative response to either item is a positive screen and should trigger assessment and help, not a lecture. Exact local wording may be adapted, but the construct is: worry that food would run out, and food that did not last with no money to buy more. [5]
| Construct | Clinical meaning | Immediate action cue |
|---|---|---|
| High food security | Reliable access | Routine prevention education |
| Marginal food security | Anxiety or occasional limits | Still screen positive for risk; do not dismiss |
| Low / very low food security | Reduced quality, quantity or disrupted eating | Food access + medical review |
| Affordability stress | Rent/mortgage consuming income | Benefit and housing advice |
| Stability threat | Moves, eviction, doubled-up | Housing advocacy; safety plan |
| Quality hazard | Damp, cold, pests, unsafe sleep space | Environmental fix + health review |
| Homelessness | No safe fixed residence | Urgent shelter pathway |
Epidemiology & Risk Factors
Poverty is the common soil. Risk concentrates where income is low, work is unstable, benefits are hard to access, and discrimination shapes housing and wages. Single caregivers, racial and ethnic minority families, migrant and refugee households, and families of children with disability or medical complexity carry higher burdens. [2] [3] [13]
Housing instability is common among families of young children with special health care needs. Trajectories of housing insecurity from infancy through adolescence associate with poorer adolescent health outcomes. Eviction is not only a legal event — it clusters with other household hardships in families with very young children. [10] [12] [13]
Programme exposure matters. Participation in nutrition assistance (for example SNAP in the US) associates with better food security and health-care access markers. Loss of SNAP associates with food insecurity and poorer health in working families with young children. In exams, name the local programme, not only the US acronym. [14] [15]
Pathophysiology
Material hardship harms children through several linked pathways. Inadequate or irregular intake reduces energy and micronutrients needed for growth, iron status, immunity and cognitive work. Caregivers under chronic threat show higher rates of depression and anxiety; that stress environment shapes parenting capacity, sleep and child mental health. [3] [6] [9]
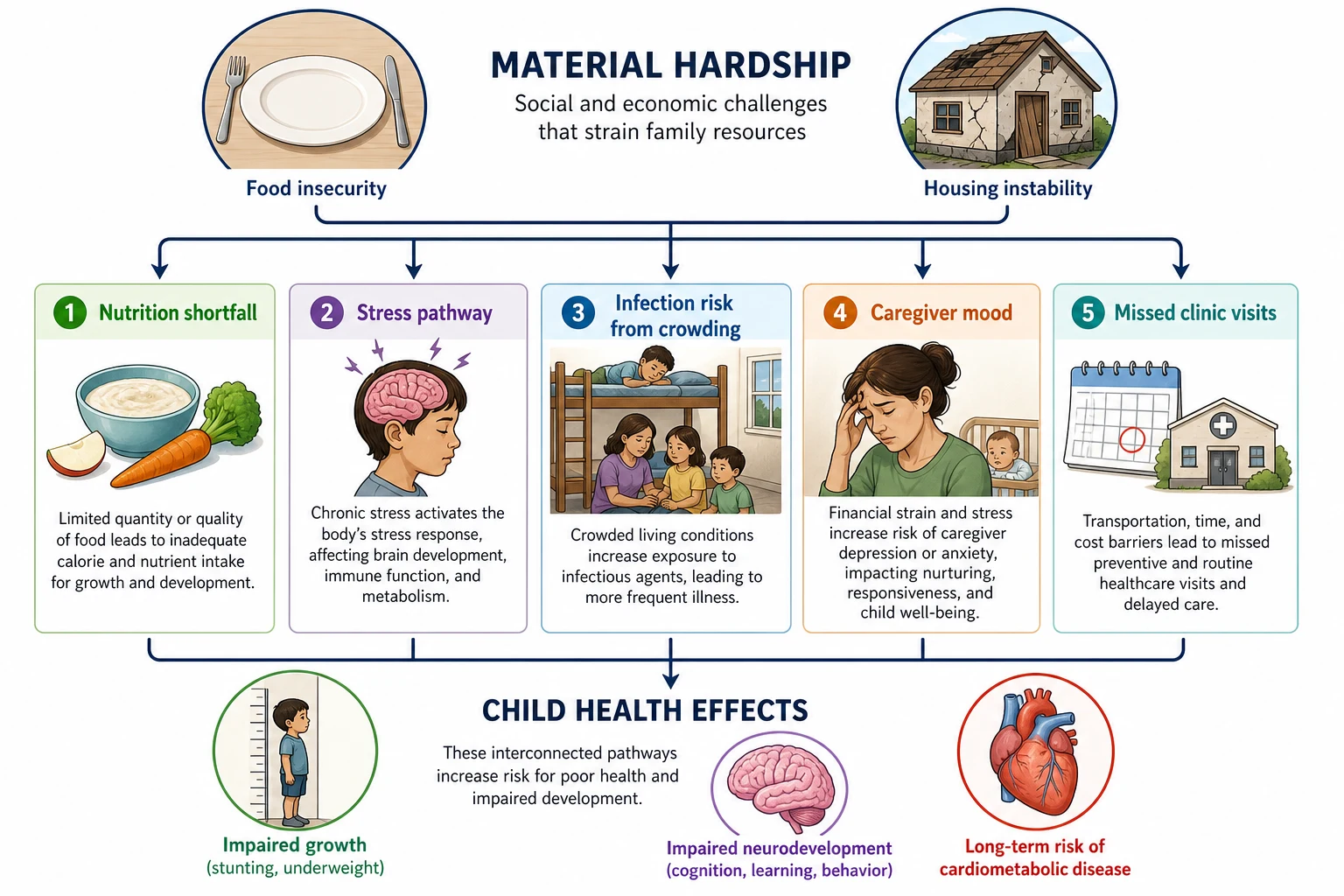
Poor housing quality adds biological load: crowding aids infection transmission; cold and damp aggravate respiratory illness; unsafe sleep spaces raise injury and sudden unexpected death risk in infants; frequent moves fracture continuity of care and school. Trade-offs — heat-or-eat, medicine-or-food, rent-or-food — are rational family decisions under scarcity, not moral failure. [4] [11]
Cook and colleagues showed that marginal food security already predicts adverse health outcomes in young children and mothers. That finding stops the exam answer “only very low food security matters.” [8]
Clinical Presentation
Most presentations are subtle. Think material hardship when you see recurrent ED visits for minor illness, missed immunisations, school absences, delayed development concerns, iron deficiency, dental disease, or a growth chart that wobbles without a clear organic story. Food insecurity associates with behavioural, emotional and academic problems in systematic review. Under-fours show health and developmental associations in large samples. [6] [7]
Parents may disclose only if you ask safely. Suburban families still experience food insecurity and may feel more stigma in affluent clinics. Housing stories include couch-surfing, frequent school changes, “we are staying with relatives,” or an eviction notice in a bag. Adolescents may hide hunger or work informal jobs to buy food. [4] [16]
Differential Diagnosis
Material hardship is both a diagnosis to act on and a confounder of other diagnoses. Your job is to hold both. [2]
| Presentation | Material-hardship pattern | Organic or safeguarding alternative | Discriminators |
|---|---|---|---|
| Faltering growth | Skipped meals, diluted formula, low food access | Coeliac, IBD, chronic disease, endocrine | Diet history + screen + targeted labs |
| Behaviour change | Hunger, chaotic housing, sleep disruption | ADHD, autism, trauma, mood disorder | Time course with food/housing stress |
| Recurrent infection | Crowding, damp, incomplete immunisation | Primary immunodeficiency | Severity, organisms, family history |
| Missed care | Transport, no fixed address, work hours | Caregiver avoidance of services | Outreach response when barriers removed |
| Empty cupboards | Poverty with engaged caregiver | Neglect / intentional withholding | Use of offered help; child safety |
Clinical & Bedside Assessment
Start with partnership language: “Many families worry about food or rent. We ask everyone so we can help.” Privacy matters — not in a crowded corridor, not with an unrelated adult translating sensitive immigration fears. [1] [16]
Minimum food screen: Hunger Vital Sign (two items). Positive = either item affirmative. Then ask what the household needs this week. [5]
Minimum housing screen (domain checklist): [4] [11]
- Are you worried about paying rent or mortgage this month?
- Have you moved more than once in the past year, or are you at risk of eviction?
- Is the home overcrowded, cold, damp, or infested?
- Do you have a safe place for the child to sleep tonight?
- Any recent shelter stay or couch-surfing?
Examine growth (weight, length/height, BMI trajectory), development, oral health, skin for infestation or neglect signs, and respiratory findings if housing quality is poor. Assess caregiver mood briefly and ask about domestic violence when safe to do so — material hardship and violence often co-travel. [3] [9]
Investigations
No blood test diagnoses food or housing insecurity. Investigations serve two jobs: find medical sequelae and exclude important organic differentials when the growth or illness pattern demands it. [1] [7]
- Often useful: full blood count and iron studies when diet is poor or growth is off; consider vitamin D in high-risk settings; developmental screening tools already in your well-child kit.
- When growth falters without a clear social story: coeliac serology, urine, and other age-appropriate failure-to-thrive work-up — do not let “social” become a diagnostic dead end.
- Housing quality clues: think lead risk in old housing renovation contexts (cross-link your lead topic); mould/damp history for chronic respiratory symptoms.
- Document social needs in the medical record with consent and local privacy rules so the team can act.
Management — Resuscitation
Treat physiology first if the child is medically unstable: ABCDE for dehydration, severe malnutrition, hypothermia, or respiratory failure. Parallel to that, fix tonight’s material crisis. [4]
- Food today: on-site food if available, emergency food parcel, same-day referral to food bank or community meal programme, formula access for infants.
- Shelter tonight: if no safe sleep space, activate housing/shelter social work immediately; do not discharge a vulnerable infant into confirmed homelessness without a plan.
- Caregiver crisis: suicidal ideation, psychosis or inability to supervise → emergency mental-health and child-protection pathways.
- Medical fragility + eviction: same-day multidisciplinary escalation; letters supporting priority housing when clinically justified.
Management — Definitive & Stepwise
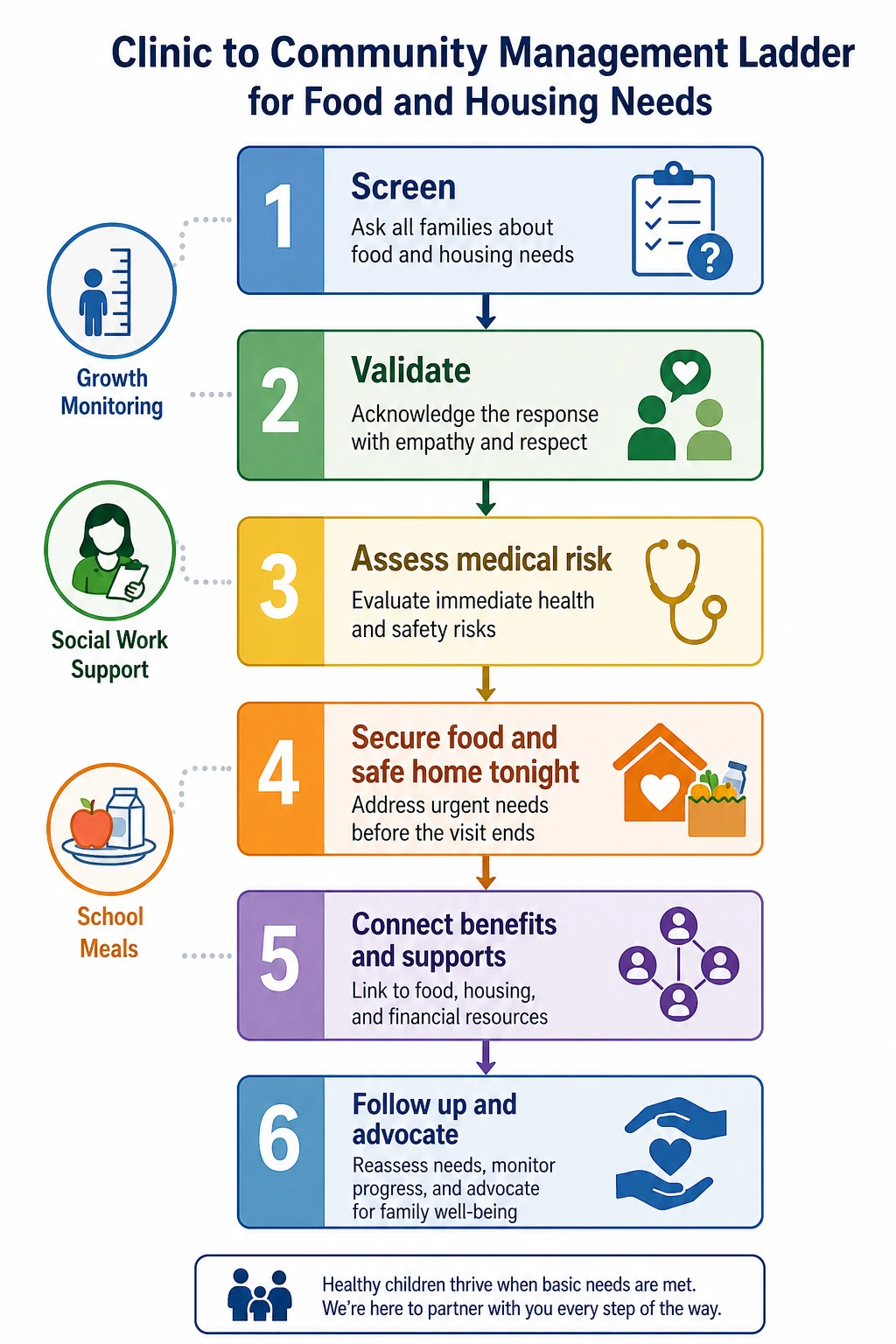
Use a ladder you can recite in viva: [1] [5]
- Screen (food + housing domains) with non-stigmatising language. [5]
- Validate and normalise: “This is common and treatable with the right supports.” [16]
- Assess medical sequelae (growth, iron, development, immunisations, mental health). [6] [7]
- Connect to resources with a named person and timeframe (closed loop). [1]
- Follow up the connection and the child’s health, not only the paperwork. [1]
- Advocate when systems fail (medical-legal partnership, priority housing letters, school meal access). [2] [4]
Nutrition and medical care. Treat iron deficiency when present; give practical food advice that respects budget (not a perfect plate lecture); support breastfeeding where chosen and feasible; ensure school-age children can access free or subsidised meals where programmes exist. Universal free school meals associate with favourable school and student outcomes in systematic review — know the evidence direction even if your jurisdiction is still means-tested. [1] [7]
Team. Social work, community health workers, dietitians, school nurses, housing officers and legal aid are part of the clinical plan. Your letter describing medical vulnerability can change housing priority. Continuity of the medical home after address changes prevents lost follow-up. [2] [4]
Closed-loop social needs response
Ask (HVS + housing domains)
Assess medical risk today
Offer concrete help this week
Name the referral owner
Recheck connection and growth
Specific Subtypes & Scenarios
Positive Hunger Vital Sign, well child. Validate, offer food resources, review growth and iron risk, book follow-up, ask about housing trade-offs. [5] [1]
Adolescent with obesity and food insecurity. Address both. Restrictive “diet only” advice fails if the household cannot buy consistent food. Use school meals, sports access and non-stigmatising counselling. [1] [6]
Eviction with infants. Treat as time-critical. Document medical vulnerability, activate housing advocacy, check safe sleep after any temporary placement, review immunisations and feeding supplies. [12] [4]
Child with special health care needs. Housing instability is enriched in this group. Equipment, power for devices, clean storage for feeds and proximity to hospital all matter in housing advocacy letters. [13]
Refugee / new-arrival family. Food knowledge, eligibility rules and language barriers stack. Use interpreters, culturally familiar food programmes and legal settlement services. [2]
Rural family. Transport and food deserts dominate. Telehealth follow-up, pharmacy and grocery delivery options, and school as a food hub may be more realistic than urban food-bank maps. [2]
Complications & Pitfalls
- Screening without help available or offered. [16]
- Judgemental language that stops disclosure. [16]
- Assuming thinness is required for food insecurity. [1]
- Missing organic disease by stopping at “social.” [7]
- Missing safeguarding by stopping at “poverty.” [2]
- Asking immigration status in a way that deters care. [4]
- One food parcel with no plan for rent crisis driving the hunger. [11]
- Losing the child after a move because no one updated contact details. [4]
Prognosis & Disposition
Early and persistent material hardship tracks into developmental risk and later adolescent health. Housing-insecurity trajectories from infancy associate with adolescent outcomes — prevention and stability earlier are better than late rescue. Benefit programmes that improve food security are health interventions, not pure welfare trivia. [3] [10] [14] [15]
Disposition rules of thumb: [1] [4]
- Home with same-week resource connection and clinic review if medically stable.
- Social-work-led housing pathway the same day if unsafe tonight.
- ED/ward for medical instability; social needs work continues in parallel.
- School and community supports as ongoing protective factors.
Special Populations
Infants and toddlers are most sensitive to feeding disruption and unsafe sleep environments. School-age children may show learning and behaviour effects first. Adolescents may be both hungry and responsible for siblings. Out-of-home care transitions can break food routines and benefit eligibility. Indigenous and migrant families face structural barriers that require culturally safe navigation, not generic pamphlets. Technology-dependent children need housing that can support power, space and hygiene. [4] [6] [7] [13]
Evidence, Guidelines & Regional Differences
Landmark policy anchors for exams: AAP Promoting Food Security for All Children (2015); AAP Poverty and Child Health with the companion technical report on mediators (2016); AAP homelessness and housing insecurity care policy (2013). Screening science rests on Hager’s 2-item tool. Outcome science includes Cook (marginal food security), Shankar (behavioural/academic review), Drennen (under-fours), Cain (mental health), Pierce and Bess (housing trajectories/scoping), Cutts (eviction), Rose-Jacobs (CSHCN housing), and Ettinger de Cuba (SNAP gain/loss). [1] [2] [3] [4] [5] [8] [10] [12] [14]
Controversy you should own: universal versus risk-based social-needs screening; how to measure housing insecurity consistently; and whether clinic screening is ethical without funded navigation. The defensible fellowship position is: if you screen, you must be able to help; if help exists, you should ask. [1] [16]
Regional practice differences
In Australia and Aotearoa New Zealand, clinicians navigate Centrelink/Work and Income supports, social housing waitlists, community food relief, Aboriginal Community Controlled Health Services and Māori providers, and local child-protection thresholds. Programme names differ by jurisdiction; the clinical ladder (screen → safety → connect → follow up) does not. [2]
Exam Pearls
- Hunger Vital Sign: two items; either “often/sometimes true” style affirmative is positive. [5]
- Marginal food security still predicts harm. [8]
- Housing insecurity ≠ only street homelessness. [4] [11]
- Eviction is a paediatric health event. [12]
- Food insecurity can coexist with overweight. [1]
- Screen without a pathway is incomplete. [16]
- Poverty ≠ neglect, but neglect can hide behind poverty language. [2]
- SNAP loss associates with worse food security and health — programmes are clinical. [14]
- Children with special needs have higher housing instability. [13]
- Long-case gold: growth chart + social needs screen + closed-loop plan + safeguarding reasoning.
Red Flags (quick list)
- No safe sleep place tonight. [4]
- Medically fragile child facing eviction. [12] [13]
- Severe malnutrition or dehydration with empty household food access. [1]
- Caregiver unable to supervise or actively suicidal. [9]
- Clear neglect pattern after realistic help offered. [2]
- Positive screen with zero follow-through plan. [16]
One-page recovery
When the family is hungry or unstably housed, your job is concrete: ask safely, secure food and shelter, treat the medical effects, connect to named supports, follow the loop, and escalate safeguarding only when the child remains unsafe despite help. That is fellowship-level community paediatrics. [1] [2] [4] [5]
References
- [1]COUNCIL ON COMMUNITY PEDIATRICS, COMMITTEE ON NUTRITION Promoting Food Security for All Children. Pediatrics, 2015.PMID 26498462
- [2]COUNCIL ON COMMUNITY PEDIATRICS Poverty and Child Health in the United States. Pediatrics, 2016.PMID 26962238
- [3]Pascoe JM Mediators and Adverse Effects of Child Poverty in the United States. Pediatrics, 2016.PMID 26962239
- [4]Council on Community Pediatrics Providing care for children and adolescents facing homelessness and housing insecurity. Pediatrics, 2013.PMID 23713108
- [5]Hager ER Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics, 2010.PMID 20595453
- [6]Shankar P Association of Food Insecurity with Children's Behavioral, Emotional, and Academic Outcomes: A Systematic Review. Journal of developmental and behavioral pediatrics, 2017.PMID 28134627
- [7]Drennen CR Food Insecurity, Health, and Development in Children Under Age Four Years. Pediatrics, 2019.PMID 31501233
- [8]Cook JT Are food insecurity's health impacts underestimated in the U.S. population? Marginal food security also predicts adverse health outcomes in young U.S. children and mothers. Advances in nutrition, 2013.PMID 23319123
- [9]Cain KS Association of Food Insecurity with Mental Health Outcomes in Parents and Children. Academic pediatrics, 2022.PMID 35577282
- [10]Pierce KA Trajectories of Housing Insecurity From Infancy to Adolescence and Adolescent Health Outcomes. Pediatrics, 2024.PMID 38946454
- [11]Bess KD The effects of housing insecurity on children's health: a scoping review. Health promotion international, 2023.PMID 35134939
- [12]Cutts DB Eviction and Household Health and Hardships in Families With Very Young Children. Pediatrics, 2022.PMID 36120757
- [13]Rose-Jacobs R Housing Instability Among Families With Young Children With Special Health Care Needs. Pediatrics, 2019.PMID 31292218
- [14]Ettinger de Cuba S Loss Of SNAP Is Associated With Food Insecurity And Poor Health In Working Families With Young Children. Health affairs, 2019.PMID 31059367
- [15]Ettinger de Cuba SA SNAP, Young Children's Health, and Family Food Security and Healthcare Access. American journal of preventive medicine, 2019.PMID 31542130
- [16]Palakshappa D Suburban Families' Experience With Food Insecurity Screening in Primary Care Practices. Pediatrics, 2017.PMID 28634248