Paeds · preventive-and-community-paediatrics
Indigenous child health and culturally safe care
Also known as Cultural safety in paediatrics · Indigenous paediatric health equity · First Nations child health framework · Anti-racism in child health · Community-controlled child health
Fellowship-level framework for Indigenous child health equity and culturally safe paediatric care: definitions, colonisation and racism as structural drivers, clinical patterns without stereotyping, partnership with community-controlled services, bedside practice, and regional frames across ANZ, Canada, the US and the UK.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A family sits down. The child has had many ear infections. School says hearing is a problem. The last clinic letter called the family “poorly compliant.” Your job is not a cultural lecture. Your job is excellent paediatrics that does not reproduce harm. [8] [12]
Indigenous peoples are not one clinical stereotype. They are distinct nations and communities with shared experiences of colonisation, dispossession and racism, and with deep strengths in culture, kinship and survival. In health systems, identity is usually based on self-identification and community recognition. Never force a label. Never assume one disease profile. [5] [7]
Cultural safety is the standard. It means the person receiving care feels safe — free from racism and from the power abuses that make people avoid services. Cultural awareness (knowing difference exists) and cultural competence (skills and knowledge) can help, but they are not enough if the patient still experiences racism. Cultural humility is the lifelong stance of self-reflection. Safety is the outcome the family defines. [1] [2]
This page is the global framework leaf. Nation-specific depth lives in sibling topics (for example Aboriginal and Torres Strait Islander child health; Māori child health and Te Tiriti). Use this page for definitions, structural drivers, bedside method and multi-region comparison. [1] [7]
Classification
Sort three ideas that examiners mix up: who the child is, what the service standard is, and what racism looks like. [1] [3]
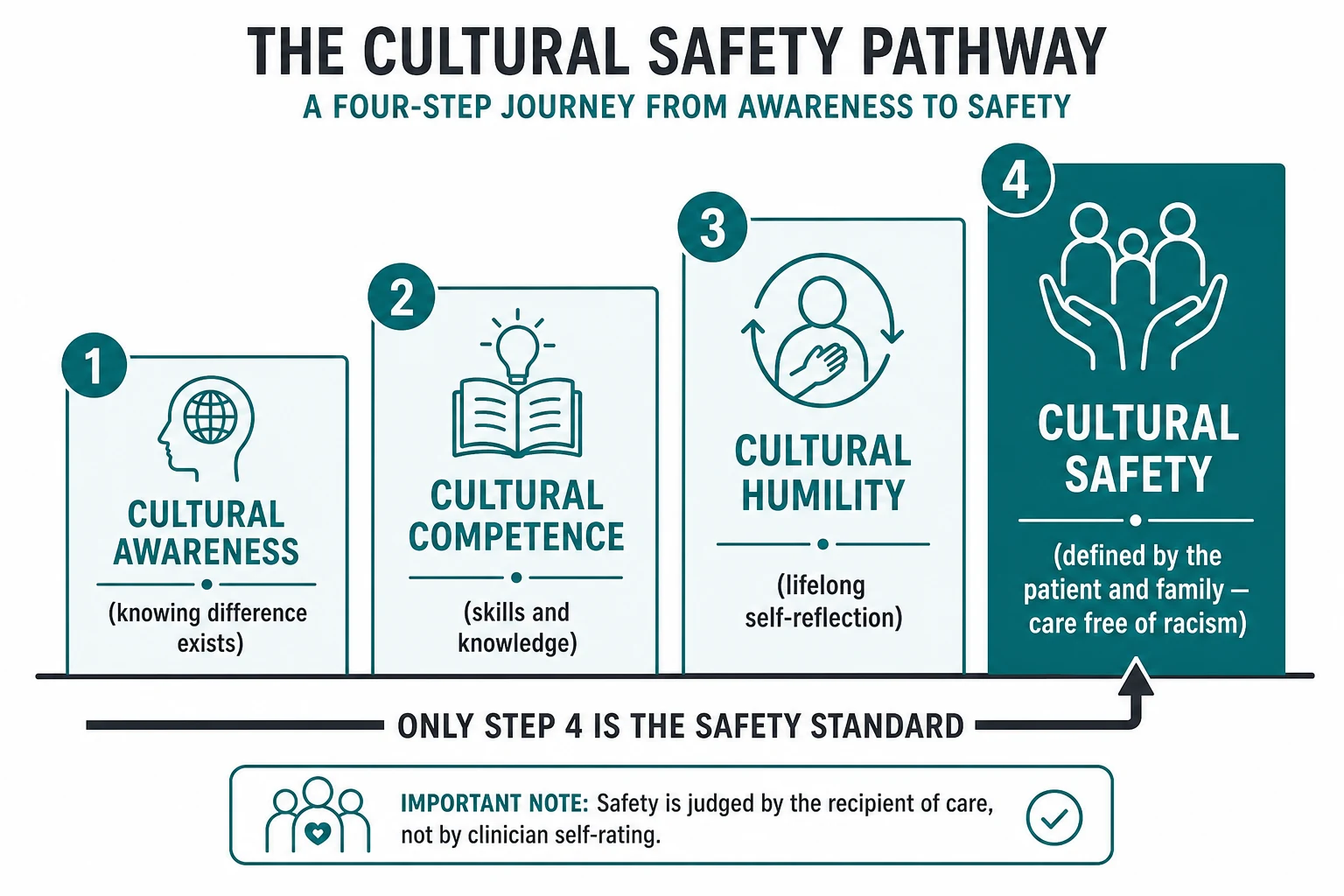
Terms you must keep separate
- Knows that cultures differ
- Can stay tourist-level
- Does not guarantee safe care
- Skills, knowledge, training checklists
- Useful but incomplete
- Risk: clinician self-certifies safety
- Defined by the recipient of care
- Addresses power and racism
- Curtis recommended definition for equity work
Jones’s framework classifies racism as institutional (differential access to goods and power), personally mediated (prejudice and discrimination), and internalised. In clinic you meet all three: a service that is hard to reach, a staff remark that shames, and a young person who has absorbed the message that “the hospital is not for us.” [3]
Epidemiology & Risk Factors
Across high-income settler states, Indigenous children carry a larger share of preventable morbidity and mortality than non-Indigenous peers. The Lancet–Lowitja collaboration and the Gracey/King series document a global pattern: higher infectious burden in early life, earlier onset of chronic disease, and gaps that track colonisation and social exclusion rather than “race biology.” [5] [6] [7]
In Australia, burden-of-disease work framed an Indigenous health gap driven largely by chronic disease, injury and social determinants — a teaching example of excess preventable burden, not a number to invent in an oral. [10] Dignity and social investment matter because health gaps shrink when material conditions and respect improve together. [9]
Risk factors that change paediatric work include housing crowding and inadequate housing (repeated respiratory and ear infection), food insecurity and poverty (growth and developmental risk), remote geography and fragmented services (delayed diagnosis), tobacco smoke and unsafe sleep environments (SUDI-environment inequity), and racism in care (delayed help-seeking). [5] [6] [7] [13] [4] [8]
Protective factors are clinical assets: connection to culture and kin, trusted Aboriginal Community Controlled Health Organisations (ACCHOs) or equivalent Indigenous-led services, secure housing, early childhood education, and continuity with a named clinician. [8]
Pathophysiology
Do not teach a racialised body. Teach how structural harm becomes biology. [6]
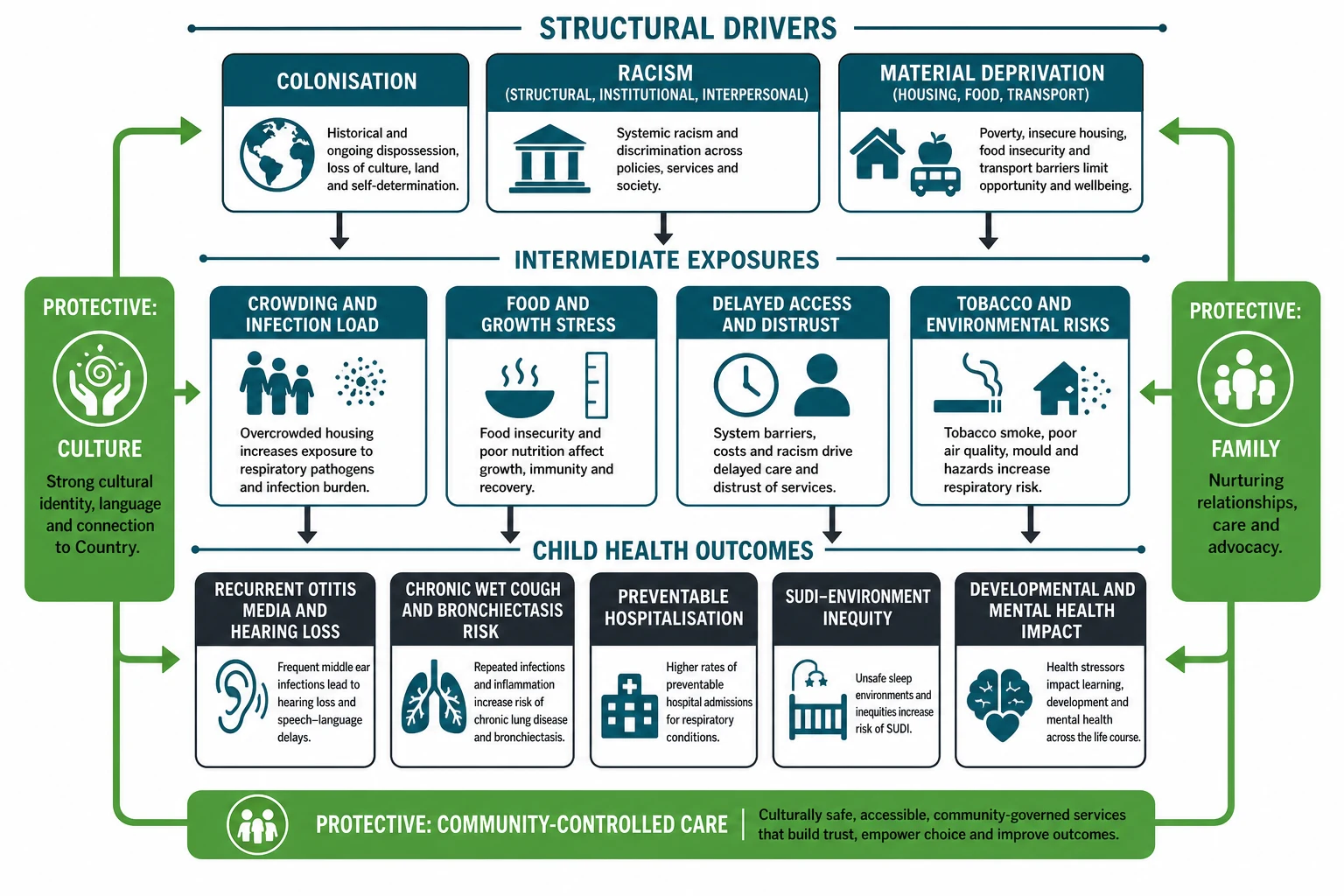
Early-life infection load rises when many people share small, poorly ventilated homes. Repeated otitis media damages middle ears and hearing. Repeated lower respiratory infection, especially with chronic wet cough, can progress toward bronchiectasis — a long-term structural lung problem that needs active follow-up, not resignation. [12] [15]
Racism adds a second pathway. Meta-analytic evidence links racism to poorer mental and physical health outcomes. In a child, that may look like anxiety, sleep disruption, school disengagement, or families who only present in crisis because prior visits felt unsafe. [4]
King’s “underlying causes” framing is the viva line: the gap is produced by social, political and historical forces, not by Indigenous culture as pathology. [6]
Clinical Presentation
What walks into your room can include a well-child visit where the real diagnosis is access; recurrent ear disease with school hearing impact; chronic wet cough needing active assessment rather than “just a cold”; infant sleep counselling with stacked environmental hazards; and an adolescent labelled “difficult” when prior racism or trauma sits underneath. [8] [12] [15] [13] [4] [11]
Families may not open with the word racism. They may say, “We don’t bother with that clinic,” or “They never listen.” That is clinical data. [8]
Differential Diagnosis
Culture is never a diagnosis. [1]
| Problem you face | Better framing | Trap |
|---|---|---|
| Missed follow-up | Access, cost, transport, trust | “Non-compliant family” |
| Recurrent OM | Infection ecology + incomplete treatment | “Normal for Indigenous kids” so no audiology |
| Wet cough months | Chronic endobronchial infection pathway | “Asthma” label without wet-cough logic |
| Thin child | Food insecurity, illness, safeguarding spectrum | Either ignoring poverty or leaping to blame |
| Bruising concern | Same safeguarding evidence standards | Over-calling or under-calling because of ethnicity |
Safeguarding uses evidence, not ethnicity. Cultural practices are not abuse. Abuse is not excused by culture. Hold both truths. [11]
Clinical & Bedside Assessment
Start with power. You hold institutional power. The family may have been hurt by people who looked like you. [3] [8]
Open well. Introduce your name and role. Ask what name and pronouns the child and caregivers use. Ask who should be in the room. Invite a support person or Aboriginal Liaison Officer when available. Sit down. Do not rush the first two minutes. [8]
History that earns trust. After the presenting problem, ask practical social questions as medical facts: housing stability and crowding; food this week; transport to clinic; smoke exposure and infant sleep space; school and hearing; prior hospital experiences that felt unsafe. [6] [8]
Examination. Use the same standards as for any child: growth chart, ears, throat, chest, skin, development. Explain each step. For ear disease, look carefully and think about hearing early. [12]
Synthesis. State the medical problem and the access problem in one plan. Example: “She has ongoing middle-ear disease that can affect hearing. We will treat today, arrange hearing testing, and fix the appointment system so you are not punished for transport barriers.” [8] [12]
Investigations
Order tests for clinical reasons, not for ethnicity labels. [1]
- Hearing assessment and audiology pathways after recurrent OM or speech/school concerns. [12]
- Wet-cough work-up as per respiratory standards; do not normalise chronic wet cough. [15]
- Standard bloods or imaging when indicated by illness severity — neither withhold nor over-order because of stereotype. [11]
- Document social determinants in the chart as clinical context, not moral commentary. [8]
Avoid both poles of bias: under-investigation (“they always have ear problems”) and over-investigation that feels extractive and distrustful. [8] [12]
Management — Resuscitation
Life threats do not wait for a cultural checklist. [1]
Use the same paediatric emergency algorithms for airway, breathing, circulation, seizures and sepsis. While you resuscitate, keep communication open: plain language, a family member present if safe, early liaison support, and no shaming comments in the bay. Cultural practices that comfort a family can often run in parallel with critical care; they do not replace it. [1]
Retrieval and transfer decisions follow clinical need. Do not delay a necessary transfer because of assumptions about “where Indigenous families prefer to stay.” Ask, explain, and involve family in the plan as soon as physiology allows. [1] [11]
Safeguarding activation, when required, uses the same evidence thresholds as for any child. Ethnicity is not a risk score. [11]
Management — Definitive & Stepwise
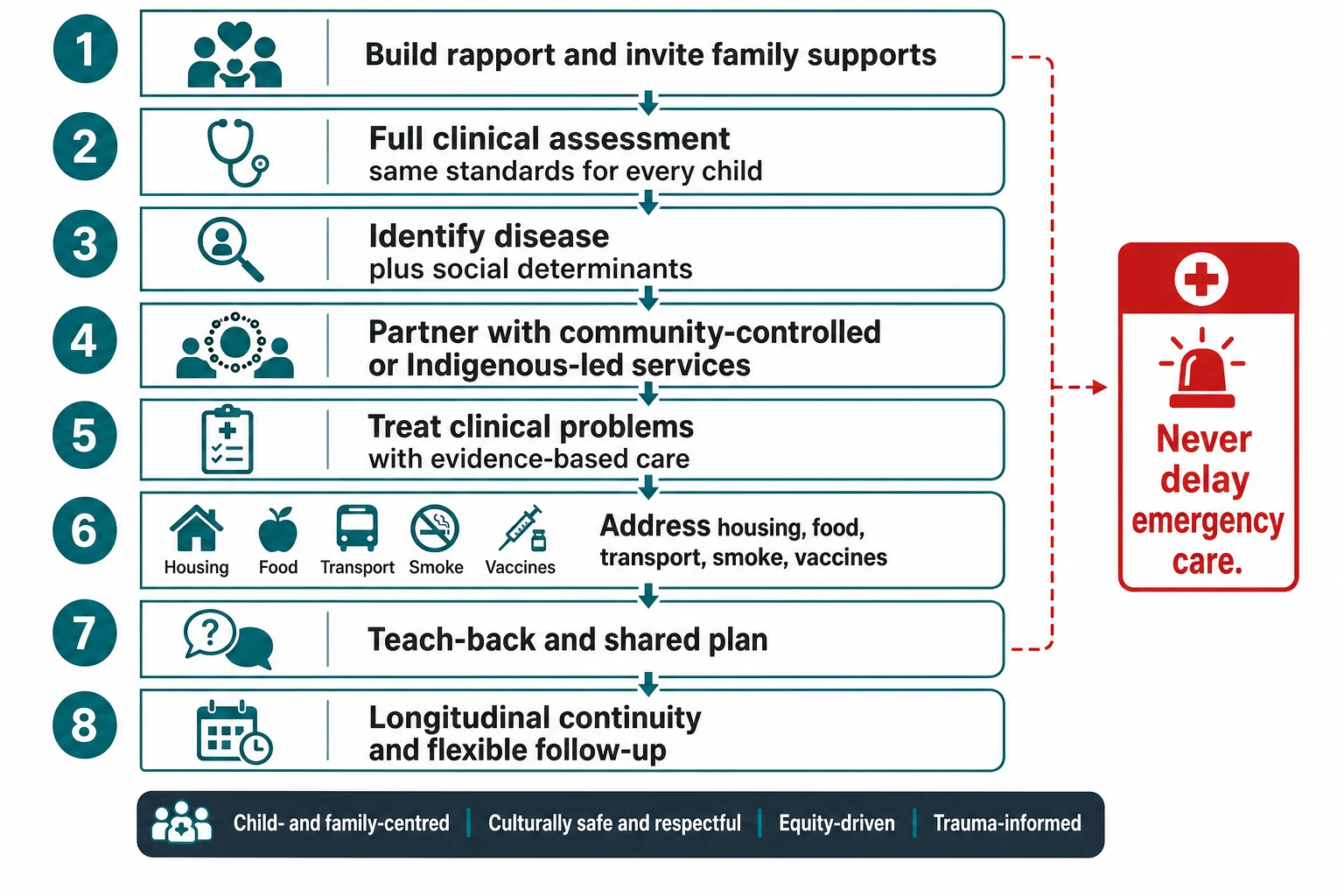
Clinic pathway you can defend in a viva
1
2
3
4
5
6
Browne’s equity strategies emphasise organisational change, not only polite clinicians: welcoming spaces, flexible systems, Indigenous staff, and accountability for racism. [8]
Disease-specific examples: use Indigenous-focused OM guidance where it applies; treat chronic wet cough seriously with long-term surveillance after bronchiectasis; apply safe-sleep rules while solving resource gaps without shame. [12] [15] [13]
Specific Subtypes & Scenarios
Urban Indigenous family in a mainstream clinic. Do not assume low risk because the postcode is metropolitan. Ask about identity only when relevant to care navigation, and offer liaison/ACCHO partnership. Continuity still matters. [8]
Remote community clinic. Prioritise what can be finished today. Arrange reliable follow-up before the wet season or before the family leaves town. Telehealth supports specialists but does not replace local trust. [7] [8]
Recurrent otitis media. Treat actively, prevent where possible, and protect hearing for school. Guidelines for Aboriginal and Torres Strait Islander children summarise intensified pathways. [12]
Chronic wet cough / bronchiectasis risk. Stop normalising months of wet cough. Treat, review, and plan long-term lung care. [15]
US AI/AN children. AAP clinical guidance stresses historical trauma, sovereignty, Indian Health Service/tribal systems, mental health burden and the need for culturally grounded care without lowering clinical standards. [11]
Canadian First Nations, Inuit and Métis children. History includes systemic failure to provide equitable medical care; Jordan’s Principle is a policy response to service disputes for First Nations children. Know the equity frame; apply local pathways. [14]
Out-of-home care. Protect cultural connection as a health need, not an optional extra. Coordinate with child protection and Indigenous family organisations. [11]
Adolescent mental health. Screen and treat as for any young person, and ask about racism, grief, identity and safety. Do not pathologise culture. [4] [11]
Complications & Pitfalls
Other pitfalls include deficit discourse that erases strengths, token workshops without system change, data and research harm without community benefit, and false dichotomies that pit clinical standards against anti-racist practice. [6] [1] [8] [7]
Prognosis & Disposition
Inequities are modifiable. Population gaps move when housing, income, education, anti-racism and Indigenous-led care improve. [7] [9]
After an acute episode, disposition includes named clinician follow-up, hearing or respiratory surveillance when indicated, linkage to community-controlled care if wanted, practical help with transport and scripts, and safety-net advice with teach-back. [8] [12]
Speak with honest hope. Fatalism is not professionalism. [9]
Special Populations
- Neonates and infants: SUDI-environment inequity and smoke exposure need non-shaming, resource-aware counselling. [13]
- School-age children: hearing loss and school engagement are paediatric outcomes, not only education issues. [12]
- Adolescents: mental health, substance use, youth justice and transition need youth-friendly, culturally safe spaces. [11]
- Disability: Indigenous children with disability face dual barriers; partner with family and specialist services. [8]
- Out-of-home care and youth justice: cultural continuity and trauma-informed care are part of the medical plan. [11]
- Urban and remote: geography changes logistics, not the right to excellent care. [7]
Evidence, Guidelines & Regional Differences
[1] [11] [14]Landmark evidence you can name includes Curtis on cultural safety, Papps on NZ cultural safety roots, Jones on levels of racism, Paradies on racism as a health determinant, Gracey/King and Anderson (Lancet–Lowitja) on global Indigenous health patterns, Browne on organisational equity strategies, Vos and Marmot on the health gap and dignity, plus Bell (AAP), Leach (OM), Shipstone (SUDI risks), Kamran (Canadian equity history) and McCallum (bronchiectasis follow-up). [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15]
Controversy to handle cleanly: equity-targeted programmes are not reverse discrimination; they correct structural disadvantage. Universal paediatric standards remain. What changes is system design and power, not the physiology textbook. [1] [9]
Exam Pearls
- Safety is defined by the recipient of care. [1]
- Racism is a health determinant, not only a courtesy issue. [4]
- Equality of offer ≠ equity of outcome. [9]
- ACCHO/Indigenous-led care is partnership, not an optional referral of last resort. [8]
- Recurrent OM and chronic wet cough are high-yield clinical clusters — manage actively. [12] [15]
- This leaf is the framework; use ATSI and Māori leaves for nation-specific detail. [1] [7]
- Never delay resuscitation for cultural processes; integrate supports in parallel. [1]
References
- [1]Curtis, E Why cultural safety rather than cultural competency is required to achieve health equity: a literature review and recommended definition International journal for equity in health, 2019.PMID 31727076
- [2]Papps, E Cultural safety in nursing: the New Zealand experience International journal for quality in health care, 1996.PMID 9117203
- [3]Jones, CP Levels of racism: a theoretic framework and a gardener's tale American journal of public health, 2000.PMID 10936998
- [4]Paradies, Y Racism as a Determinant of Health: A Systematic Review and Meta-Analysis PloS one, 2015.PMID 26398658
- [5]Gracey, M Indigenous health part 1: determinants and disease patterns Lancet, 2009.PMID 19577695
- [6]King, M Indigenous health part 2: the underlying causes of the health gap Lancet, 2009.PMID 19577696
- [7]Anderson, I Indigenous and tribal peoples' health (The Lancet-Lowitja Institute Global Collaboration): a population study Lancet, 2016.PMID 27108232
- [8]Browne, AJ Enhancing health care equity with Indigenous populations: evidence-based strategies from an ethnographic study BMC health services research, 2016.PMID 27716261
- [9]Marmot, MG Dignity, social investment and the Indigenous health gap The Medical journal of Australia, 2017.PMID 28659108
- [10]Vos, T Burden of disease and injury in Aboriginal and Torres Strait Islander Peoples: the Indigenous health gap International journal of epidemiology, 2009.PMID 19047078
- [11]Bell, S Caring for American Indian and Alaska Native Children and Adolescents Pediatrics, 2021.PMID 33753539
- [12]Leach, AJ Otitis media guidelines for Australian Aboriginal and Torres Strait Islander children: summary of recommendations The Medical journal of Australia, 2021.PMID 33641192
- [13]Shipstone, RA Prevalence of risk factors for sudden infant death among Indigenous and non-Indigenous people in Australia Acta paediatrica, 2020.PMID 32239524
- [14]Kamran, R Canada's history of failing to provide medical care for Indigenous children Paediatrics & child health, 2021.PMID 34336055
- [15]McCallum, GB A decade on: Follow-up findings of indigenous children with bronchiectasis Pediatric pulmonology, 2020.PMID 32096916