Paeds · preventive-and-community-paediatrics
Infant health supervision: 3 to 6 months
Also known as 4-month well-child visit · 6-month well-infant review · Infant health check 3–6 months · Bright Futures 4 and 6 months · Child health nurse 4-month check
Fellowship guide to the 3–6 month health-supervision window: growth and feeding, evidence-informed milestones, safe sleep and tummy time, head shape, maternal mood screening, injury prevention, immunisation-ready visits, red flags and regional schedule differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Visit length and content matter. Rushed visits lose family-centred content and leave families less satisfied; protect time for concerns, not only for needles. [9]
G.R.O.W. 3–6
Overview & Definition
Picture a four-month-old on the examination mat. The mother says sleep is broken and the head looks flat on one side. The father asks when solids start. The infant smiles, holds the head up prone, and has doubled birth weight. That is the 3–6 month health-supervision window: still fully milk-fed for most infants, gaining head control and social engagement, still at peak risk for sleep-related death if the sleep environment is wrong, and still tightly bound to caregiver mental health. [1] [3] [4]
Infant health supervision in this band means planned preventive care that covers growth, development, physical examination, anticipatory guidance, immunisations and family context. It is not the same as a brief “jabs only” encounter. Bright Futures and equivalent child health programmes organise age-specific priorities so you do not invent a personal checklist each time. [9]
This page owns the 3–6 month leaf. Birth-to-3 months, 6–12 months, safe-sleep deep-dive, immunisation schedules and general developmental screening tools are adjacent topics — cross-link them rather than rewriting those chapters here. [5]
Classification
Classify the visit before you classify the infant. [9]
Scheduled 4-month-type visit. Focus on feeding volume and technique, vitamin D, social smile and head control, safe sleep reinforcement, maternal mood, and immunisations due on the local schedule. [1] [3] [5]
Scheduled 6-month-type visit. Reassess growth velocity, early rolling and hand transfer, readiness talk for complementary feeding, injury risks as mobility rises, continued maternal mood screening, and the next immunisation set. [4] [6]
Opportunistic preventive content inside an acute visit. If the infant is stable after a minor complaint, you may reinforce sleep or plot growth — but you do not delay treatment of illness to complete a full well-visit script. [13]
Surveillance versus screening versus evaluation. At this age you mainly run developmental surveillance: ask, watch, document domains, act on red flags. Standardised general developmental screening tools appear more often from later infancy/toddler ages in many schedules; do not wait for a birthday screen if concern is already high. [4] [5]

Epidemiology & Risk Factors
Missed 4- and 6-month visits cluster with transport barriers, insecure work, housing stress and fragmented care. Those same families often carry higher sleep-related death risk if smoke exposure, soft bedding or shared soft surfaces continue. [1] [11]
Sleep-related infant death risk remains clinically important well after the newborn period. Supine sleep on a firm flat surface, free of soft objects, remains the core environmental protection. [1]
Positional plagiocephaly rose as back-to-sleep campaigns succeeded. That is not a reason to abandon supine sleep. It is a reason to teach awake, supervised tummy time and position variation. [7]
Perinatal depression is common and under-treated. Untreated maternal depression links to feeding problems, inappropriate infant care patterns, and later developmental risk. AAP guidance asks paediatric settings to screen at the 1-, 2-, 4- and 6-month well-child visits. [3]
Language discordance without a professional interpreter degrades history, mood screening and safety counselling. [10] Children with medical complexity need the same preventive skeleton with individualised targets, not a skipped well visit. [12]
Pathophysiology
Why does this age feel different from the newborn review? [4]
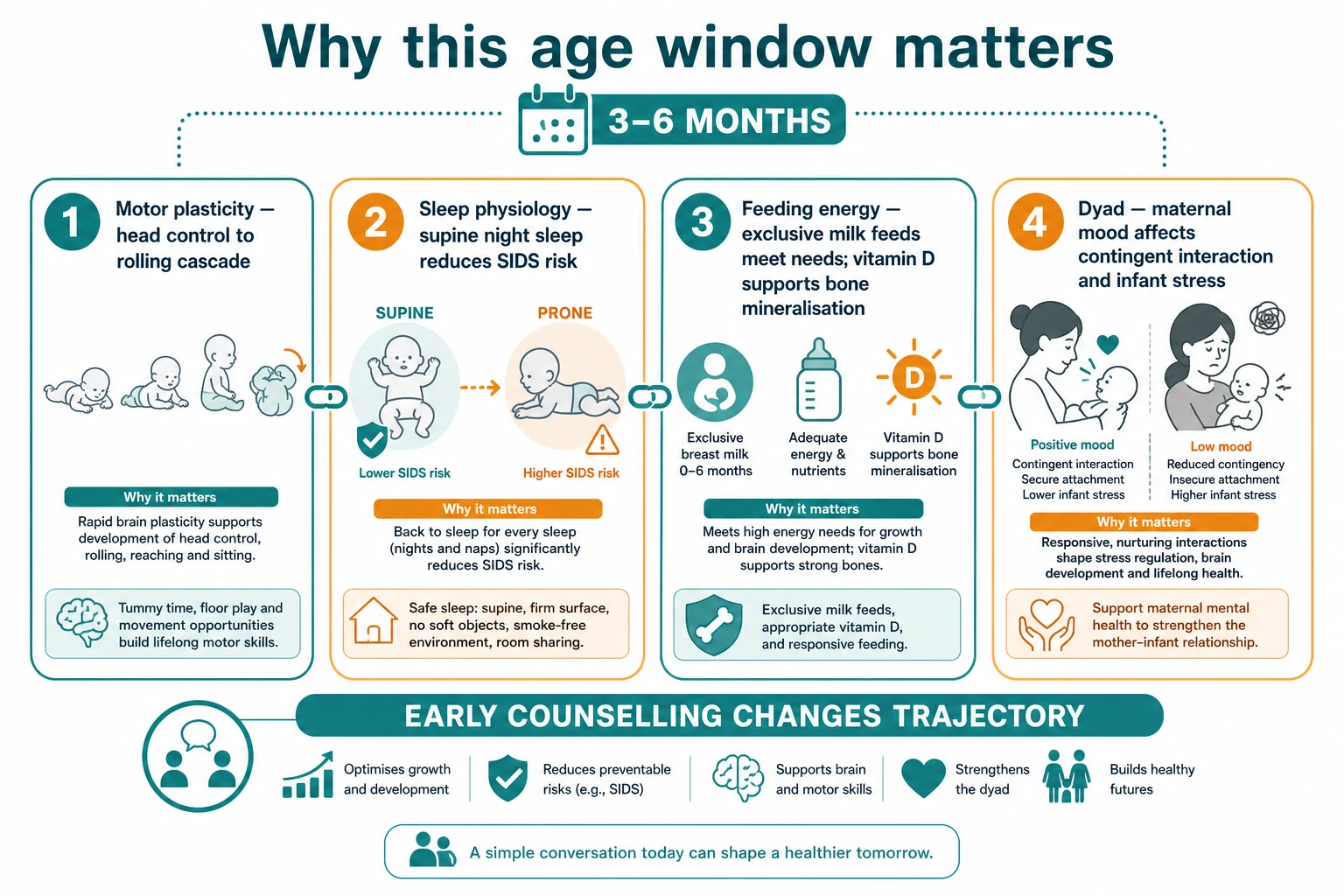
Motor cascade. Neck and trunk control improve so the infant can hold the head steady, push up when prone, and begin rolling. Skills stack: delayed head control changes what you expect next and how you examine tone. [4]
Sleep physiology and environment. Prone and side sleep increase risk of sleep-related death compared with supine sleep on a firm surface. Soft bedding and overheating add risk. The teaching point is environmental, not “make the baby sleep through.” [1]
Nutrition and bone mineral. Exclusive milk feeding can meet energy needs in this window for many infants. Vitamin D status depends on diet, sun and supplementation policy; AAP guidance supports vitamin D to prevent rickets and deficiency in at-risk milk-fed infants. [2] Iron stores gradually decline; prevention and testing strategy is risk- and age-dependent rather than a universal 4-month blood panel for every well infant. [8]
Dyadic stress biology. Caregiver depression changes contingent responses. The infant may show flatter engagement or unsettled behaviour. Trauma-informed care treats the dyad without blaming the parent for having an illness. [3] [11]
Clinical Presentation
Typical thriving visit. Caregivers describe frequent milk feeds, settling patterns that still fragment at night, increasing social smile and cooing, and curiosity about solids near six months. Growth tracks. Exam is reassuring. [4] [6]
Common concerns that still fit preventive care. “Head is flat.” “Cries every evening.” “Spits up a lot but is gaining.” “When can we start food?” “I am exhausted and tearful.” Each needs a structured answer, not dismissal. [3] [7]
Subtle worry. Poor social engagement, stiff or floppy tone, slow weight gain with long feeds, or a caregiver who says “something is not right.” Caregiver concern is a signal worth weight. [13] [5]
Wrong room presentation. An infant booked for immunisations who is mottled, working hard to breathe, or not feeding is an acute patient. Start with severity assessment, not the growth chart. [13]
You will also meet the overwhelmed but coping family. Feeds are frequent. Sleep is fragmented. The infant is growing. Your job is to validate the hard work, check that the sleep surface is still safe when everyone is exhausted, and offer practical supports rather than empty praise. Exhaustion plus an unsafe sleep shortcut is a classic trap. [1] [3]
Near six months, parents often push for a single “magic” solid food start date. Developmental readiness (sitting with support, good head control, interest in food, loss of pure tongue thrust) matters more than the calendar alone, and milk remains the main energy source early in complementary feeding. [6]
Differential Diagnosis
Evening crying. Normal developmental crying peaks and self-limited colic patterns versus gastro-oesophageal reflux disease with warning signs, cow’s milk protein allergy with other features, corneal abrasion, hair tourniquet, or infection. Weight gain and exam narrow the list. [13]
Flat head. Positional plagiocephaly (parallelogram head, ear position shift, no ridge) versus craniosynostosis red flags (bony ridge, progressive restricted skull growth, raised pressure signs). Positional deformity management must never include prone night sleep. [7] [1]
Slow weight gain. Inadequate intake, ineffective latch, incorrect formula preparation, increased losses, chronic illness, or neglect. Plot velocity before you order a panel. [8]
Low tone or delayed head control. Normal late variant after prematurity (use corrected age early) versus neuromuscular disease, central hypotonia, or severe illness. Persistent delay needs more than “review next time.” [4] [5]
Unsettled sleep. Normal night waking on milk feeds versus unsafe sleep practices, maternal depression amplifying distress, or occult pain. Fix the sleep surface first if it is unsafe. [1] [3]
Clinical & Bedside Assessment
Open the visit. “What worries you most today?” Then ask specifically about feeding type and volumes, vitamin D, sleep surface and position, smoke exposure, falls and car seat use, and maternal mood. [1] [3]
Growth. Undress appropriately. Measure weight, length and occipitofrontal circumference with correct technique. Plot on the chart your service uses (often WHO-based early childhood charts in ANZ/UK; confirm local policy). Interpret trend, not a single point. [8]
Development. Use evidence-informed milestone expectations for age (and corrected age when appropriate). At a teaching level around four months many infants show steady head control when held, push up on forearms when prone, and engage socially; by around six months many roll, transfer objects and babble more richly — use the official list you are taught, not folklore averages. Document domains: gross motor, fine motor, language/communication, social-emotional. [4] [5]
Physical exam essentials. General appearance and work of breathing; fontanelle; red reflexes; heart sounds and femoral pulses; hip stability manoeuvres per local practice; abdomen; skin; genitalia; tone and primitive reflexes that should be evolving; head shape from above. [7]
Worked micro-sequence on the mat. Place the infant supine and watch spontaneous movement. Pull to sit and note head lag. Prone for a few seconds of supervised observation if the infant is settled — do you see forearm push and a lifting head? Offer a rattle and watch reach. Talk and smile; does the infant brighten and coo? None of these replace a validated tool later, but they make surveillance real. [4] [5]
Hip and heart traps. A soft murmur may be innocent or not — document timing and refer by local pathway rather than guessing. Absent or weak femorals with upper-limb blood pressure concern needs same-day senior review. Hip examination needs structured technique and local ultrasound pathways when indicated; do not invent imaging ages from memory. [12]
Dyad observation. Watch how the caregiver settles the infant. Flat affect or harsh handling is data, not a moral verdict. Use trauma-informed language. [11]
Maternal mood screen. AAP guidance supports structured recognition of perinatal depression in paediatric visits at 1, 2, 4 and 6 months, with a pathway for positive screens. Name the tool your service uses (for example EPDS) rather than inventing cut-offs here. [3]
Investigations
Most thriving infants need no blood tests at a routine 4- or 6-month visit. [8]
Order or arrange tests when the story demands them: growth failure evaluation, suspected anaemia risk groups per iron guidance, incomplete newborn screening, hearing concerns, or imaging when craniosynostosis is clinically suspected. Do not treat a single soft flat occiput as an imaging indication. [7] [8]
Maternal depression screening is a caregiver investigation with infant impact — have a referral path before you hand out a form. [3]
Management — Resuscitation
A well-child clinic can still meet an emergency. [13]
If the infant is cyanosed, apnoeic, convulsing, severely dehydrated or in shock, leave the preventive agenda and use paediatric emergency pathways. If you suspect serious inflicted injury or the infant cannot be safely cared for, activate safeguarding and protective services while treating medical needs. If a caregiver discloses active suicidal intent, escalate adult mental-health emergency care and ensure the infant is safe with a responsible adult. [3] [11] [13]
Management — Definitive & Stepwise
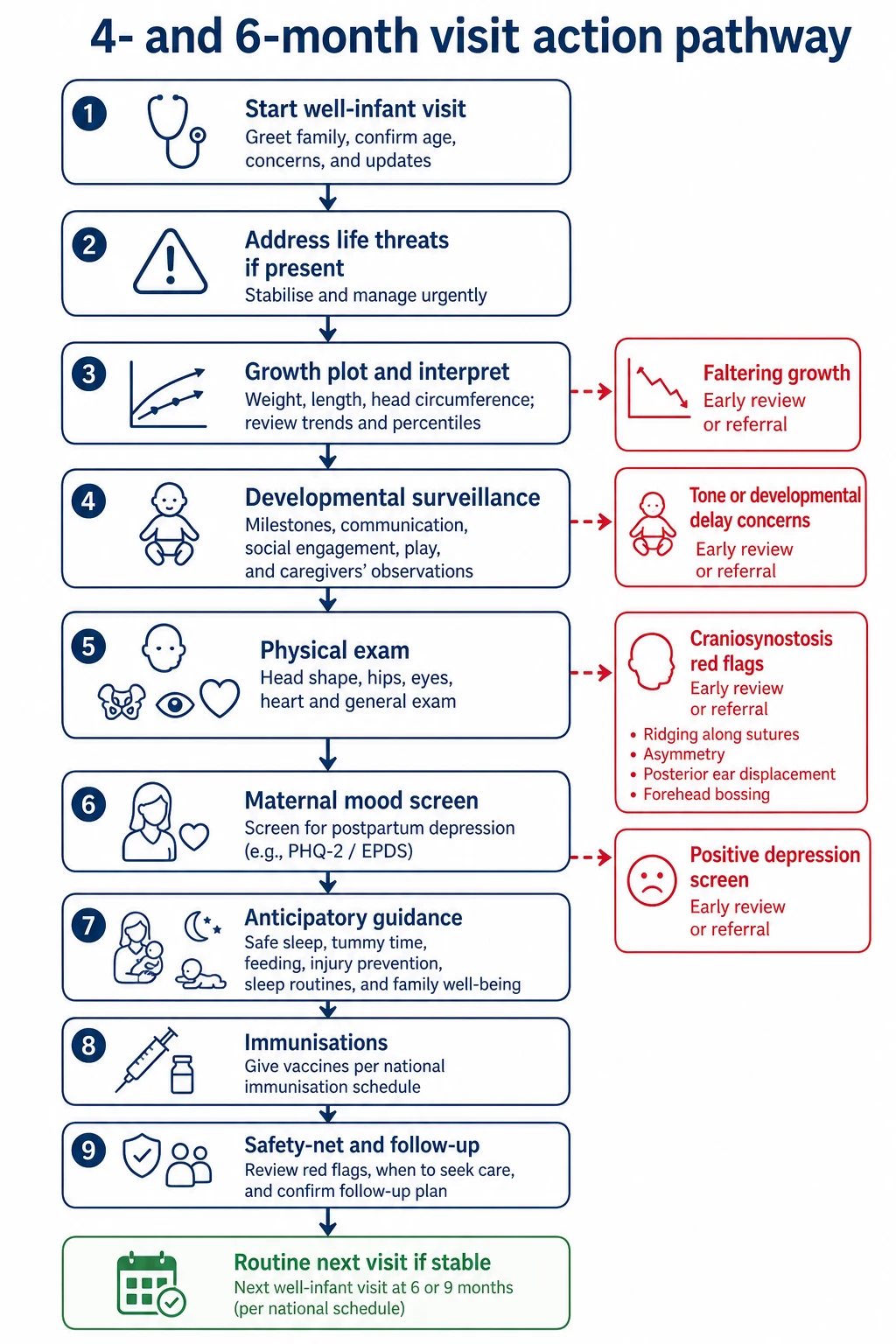
- Confirm stability and the visit purpose. [13]
- Elicit concerns and complete maternal mood screening per local tool and AAP timing framework. [3]
- Measure and plot weight, length and OFC; explain the curve in plain language. [8]
- Surveillance of development with evidence-informed milestones; act on red flags without “wait and see” fog. [4] [5]
- Targeted examination including head shape, hips, eyes, heart and femorals. [7]
- Anticipatory guidance
- Safe sleep: back to sleep for every sleep; firm flat surface; no soft bedding or soft shared sleep surfaces; avoid smoke exposure. [1]
- Tummy time: only when awake and supervised, to support motor development and reduce positional skull deformity risk. [7]
- Feeding: support breastfeeding or safe formula preparation; discuss vitamin D per national/AAP guidance for at-risk milk-fed infants. [2]
- Complementary feeding timing: ESPGHAN supports introduction of complementary foods when the infant is developmentally ready, not before about 4 months and not delayed long after 6 months for the general population — map exact public health wording to your jurisdiction. [6]
- Injury prevention: never leave on elevated surfaces; correct car restraint; water temperature; rising mouthing and choking awareness near six months. [15]
- Immunisations due on the national or state schedule — health supervision and immunisation are one visit, not rivals. Consent principles still apply. [14]
- Safety-net written and spoken: when to return for fever, poor feeding, breathing difficulty, colour change, seizures, or parental despair; how to chase results and referrals. [15]
- Handover outstanding issues clearly if another clinician will see the family next. [16]
How to talk about sleep without shame. Many families bed-share because of culture, housing or exhaustion. Lead with risk reduction: firm flat surface, supine position, no soft bedding or sofas, no smoke, and no shared sleep with a caregiver impaired by alcohol or drugs. If they will still share sleep, keep the conversation open so they hear the highest-risk practices to avoid. A slammed door ends disclosure. [1] [11]
How to talk about mood without pathologising culture. Say: “Looking after a young baby is hard on every parent. We ask every family about low mood and anxiety because help works better early.” Then use your local screen. If positive, treat the infant visit as an entry point to adult care and dyad support, not a diagnosis ceremony. [3]
Feeding troubleshoot in three questions. What is offered (breast, formula brand/preparation, water/other)? How often and how long? What comes out (wet nappies, stool pattern, vomiting character) and what does the growth chart say? Match advice to the chart, not to parental anxiety alone. [2] [8]
Four-minute closing script
Teach-back sleep
Ask the caregiver to show how the infant will be placed tonight.
Name the next visit
Give the month and purpose, including immunisations if due.
Write three return triggers
Breathing, feeding, colour or behaviour change — plus caregiver crisis contacts.
Close open loops
Referrals, vitamin D supply, lactation or mental-health follow-up with a named path.
Specific Subtypes & Scenarios
Ex-preterm infant. Use corrected age for early developmental expectations as your follow-up protocol advises, still plot growth carefully, and do not skip safe-sleep or mood content because the NICU course “explained everything.” [4] [12]
Exclusively breastfed infant. Support latch and supply; address vitamin D per guidance; avoid pressure to start solids before developmental readiness. [2] [6]
Formula-fed infant. Check preparation concentration, volumes and bottle practices; overfeeding can present as rapid weight gain and reflux-like symptoms. [8]
Positional plagiocephaly. Reassure when features are positional; increase supervised tummy time and position variation; refer when progressive deformity, neurological signs or craniosynostosis features appear. Never prescribe prone sleep at night. [7] [1]
Vaccine-hesitant family. Stay in relationship, address specific fears, avoid humiliation, and document informed decision-making. Detailed hesitancy counselling is an adjacent leaf — still offer the vaccines due today if consent is obtained. [14]
Language-discordant family. Book professional interpreters for mood screening and safety counselling; do not use older siblings. [10]
Out-of-home or kinship care. Confirm legal decision-makers, records of immunisations and prior growth, and a named medical home contact. [11] [12]
Twins and multiples. Feeding logistics and parental sleep debt multiply risk of unsafe sleep shortcuts. Counsel each infant’s sleep space and check that car restraints and feeding plans are workable at home, not only ideal on paper. [1] [3]
Rural and telehealth reviews. You can still open concerns, review plotted measurements if the family has clinic weights, watch development on video, and counsel sleep and feeding. You cannot replace hands-on hip, red reflex and full tone exam forever — schedule an in-person exam when distance delayed it. [9] [12]
Complications & Pitfalls
- Treating the visit as “needles only” and missing growth or mood. [9] [3]
- Reassuring delayed head control without a neurological exam. [5]
- Advising tummy time asleep to fix a flat head. [1] [7]
- Calling every flat occiput craniosynostosis — or missing true suture fusion. [7]
- Starting complementary foods far too early without readiness, or delaying without a plan. [6]
- Inventing universal iron labs at four months for every well infant. [8]
- Positive maternal screen with no referral pathway. [3]
- Incomplete handover of open growth or safeguarding concerns. [16]
Prognosis & Disposition
Most infants leave with a routine next scheduled visit. Early review is required for faltering growth, abnormal tone, failed social engagement, unsafe sleep that cannot be fixed today, or a positive maternal mood screen needing prompt support. [3] [5]
Disposition options include lactation support, dietetics, physiotherapy for motor delay or plagiocephaly pathways, developmental services, maternal mental health, and social work. Safety-netting improves when families leave with concrete triggers and contacts, not vague “come back if worried.” [15]
Special Populations
Medical complexity. Keep preventive anchors: growth with appropriate equipment, individualised developmental expectations, emergency care plans, and caregiver burnout checks. [12]
Indigenous families. Prioritise cultural safety, continuity, and community-controlled service links where available. [11]
Migrant and refugee families. Rebuild interrupted immunisation and screening histories; use interpreters; screen for housing and food insecurity. [10]
Socioeconomic disadvantage. Ask about formula cost, safe sleep space and transport to the next visit; link practical supports. [1] [11]
Possible maltreatment. Unexplained injury, extreme neglect of basic care, or fabricated illness concerns need safeguarding processes in parallel with medical care. [11]
Evidence, Guidelines & Regional Differences
Moon and colleagues summarise the evidence base behind 2022 updated safe infant sleep recommendations. [1] Wagner and Greer provide AAP vitamin D and rickets prevention guidance still widely cited for milk-fed infants. [2] Earls and colleagues set the paediatric practice framework for perinatal depression recognition, including screening at 1-, 2-, 4- and 6-month visits. [3] Zubler and Lipkin guide modern milestone surveillance and the surveillance–screening–evaluation model. [4] [5] Fewtrell and ESPGHAN frame complementary feeding timing for European practice with global influence. [6] Laughlin addresses positional skull deformity prevention and management. [7] Baker addresses iron deficiency prevention and diagnosis in early childhood. [8]
Use the local child health book / Well Child Tamariki Ora schedule, jurisdictional nurse checks, and the current National Immunisation Program (or NZ schedule). WHO-based growth charts are common in early childhood — confirm your service chart. Cultural safety and interpreter access are part of valid supervision. [10]
Map to the Healthy Child Programme and local health-visitor contacts. Immunisation timing follows the UK schedule. Developmental surveillance language may differ from US Bright Futures ages — state the local tool. [5]
Bright Futures / AAP periodicity structures many 4- and 6-month visits. Safe sleep, vitamin D, iron and perinatal depression guidance above are frequently examined. Canadian provincial programmes vary — name the provincial schedule rather than inventing one. [1] [2] [3]
Exam Pearls
- Health supervision at 3–6 months is multi-domain, not weight-and-jab. [9]
- Back to sleep every sleep; tummy time only awake and watched. [1] [7]
- Plot weight, length and OFC and read the velocity. [8]
- Use evidence-informed milestones; caregiver concern is data. [4] [13]
- Screen maternal mood at 4- and 6-month visits in the AAP framework and have a path for positives. [3]
- Vitamin D for at-risk milk-fed infants — cite the guidance you follow. [2]
- Complementary feeding: not before ~4 months; aim around readiness near 6 months per ESPGHAN framing and local public health advice. [6]
- Positional plagiocephaly ≠ licence for prone night sleep. [7] [1]
- Unwell infant overrides the preventive script. [13]
- Safety-net with concrete triggers. [15]
References
- [1]Moon RY Evidence Base for 2022 Updated Recommendations for a Safe Infant Sleeping Environment to Reduce the Risk of Sleep-Related Infant Deaths. Pediatrics, 2022.PMID 35921639
- [2]Wagner CL Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics, 2008.PMID 18977996
- [3]Earls MF Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics, 2019.PMID 30559120
- [4]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [5]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [6]Fewtrell M Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. Journal of pediatric gastroenterology and nutrition, 2017.PMID 28027215
- [7]Laughlin J Prevention and management of positional skull deformities in infants. Pediatrics, 2011.PMID 22123884
- [8]Baker RD Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0-3 years of age). Pediatrics, 2010.PMID 20923825
- [9]Halfon N Duration of a well-child visit: association with content, family-centeredness, and satisfaction. Pediatrics, 2011.PMID 21930541
- [10]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [11]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [12]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [13]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [14]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [15]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [16]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088