Paeds · preventive-and-community-paediatrics
Newborn preventive care and screening
Also known as Newborn screening · Neonatal screening · Bloodspot screening · Newborn hearing screening · CCHD pulse oximetry screening · NIPE
Fellowship guide to the newborn preventive package: physical examination, dried bloodspot screening, universal hearing screening, critical congenital heart disease pulse-oximetry, vitamin K, jaundice and DDH risk pathways, incomplete screens, family communication and regional programme differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Newborn preventive care is the set of actions that protect a baby who usually looks well at birth. It is not the same as delivery-room resuscitation. It is also not the same as the later infant health-supervision schedule. The work sits in the first hours to first weeks of life, when several serious conditions are still silent. [1] [8]
Screening means testing a whole population of newborns to find disease early, before symptoms declare. Diagnostic testing confirms or excludes disease in those who screen abnormal. Surveillance means planned review over time when risk remains after a first test. Case-finding means looking harder in a high-risk infant. Keep these words separate in viva answers. [1]
Modern screening still rests on Wilson and Jungner principles, refreshed for genomic and point-of-care tests. There must be an important health problem, an accepted treatment, a suitable test, an agreed policy on whom to treat, and a system that can deliver confirmation and care. A laboratory result alone is not a programme. [1] [8]
What you actually do from birth to first community review
Stabilise first
Resuscitation and transition come before elective screens. Do not delay life support for a bloodspot card.
Prevent immediate harm
Give vitamin K per local pathway. Start eye prophylaxis only where jurisdiction still requires it. Support feeding and temperature.
Examine systematically
Eyes, heart, hips, genitalia, spine, neurology, dysmorphology and growth. Document red-reflex and hip findings clearly.
Complete core screens
Bloodspot at the correct age window, hearing screen, and timed CCHD pulse-oximetry with pre- and post-ductal readings as per local algorithm.
Close the loop
Interpret pass, refer, fail, pending and incomplete states. Book confirmation. Hand over to community care with a named owner and safety-net.
Classification
Think in result states, not only disease names. Pass or clear means continue routine care and still counsel residual risk. Refer or fail means a defined next test or clinical pathway. Pending means the sample or result is not yet available. Incomplete means the test was never done, was invalid, or the family left without a plan. Each state needs a different action and a different urgency. [8] [13]
Critical congenital heart disease in screening language means duct-dependent or otherwise hypoxaemic lesions that pulse oximetry can help detect before collapse. It is not a synonym for every murmur or every structural heart defect. Coarctation and some other lesions can still be missed. [3] [4] [13]
Hearing programmes usually use otoacoustic emissions, automated auditory brainstem response, or a two-step combination. A refer is not a diagnosis of deafness. It is a ticket to diagnostic audiology within a time standard such as the widely taught 1-3-6 framework: screen by 1 month, diagnose by 3 months, intervene by 6 months, with local programmes sometimes aiming earlier. Always check the service standard you work under. [10] [11]
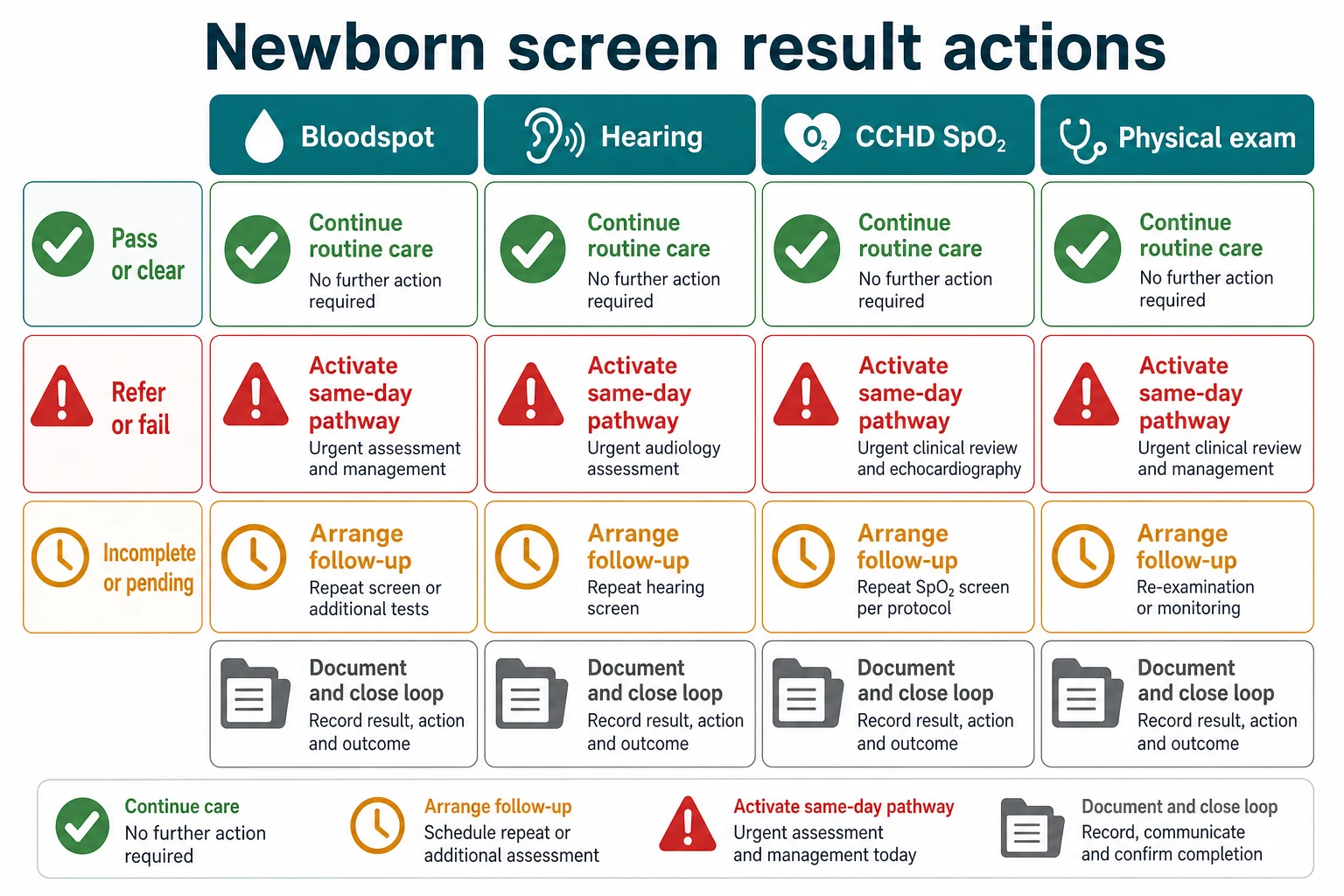
Read the figure like this: do not leave the ward with a grey incomplete cell and no name next to it. The common exam trap is treating “probably done” as done. [8] [13]
Bloodspot
Laboratory programme
- Dried blood on filter paper
- Panel content is jurisdiction-specific
- Timing and quality of the spot matter
- Critical results need same-day clinical response
Hearing
Point-of-care then audiology
- OAE and/or AABR
- Refer is not a final diagnosis
- Risk factors for late-onset loss remain
- Early intervention protects language
CCHD SpO2
Point-of-care hypoxaemia screen
- Pre- and post-ductal readings
- Algorithm-based pass, fail or repeat
- Non-cardiac causes of fail exist
- Pass does not exclude all heart disease
Examination
Hands-on case finding
- Red reflex, heart, hips, spine, genitalia
- Risk-factor guided DDH imaging
- Jaundice and feeding assessment
- Documents what screens cannot see
Epidemiology & Risk Factors
The purpose of each screen is different. Bloodspot programmes reduce disability and death from conditions such as congenital hypothyroidism and other treatable metabolic or endocrine diseases that are asymptomatic at birth. Hearing programmes reduce the language cost of permanent childhood hearing loss when detection is early. CCHD pulse-oximetry programmes reduce late presentation of duct-dependent heart disease after the duct closes. Vitamin K prophylaxis reduces vitamin K deficiency bleeding, including catastrophic late intracranial bleeding. [2] [9] [17] [18]
Missed or delayed screening clusters where systems are fragile. Early discharge, home birth, interhospital transfer, weekend staffing, incomplete contact details and rural distance all raise the chance that a test is never completed or a result never reaches a clinician who can act. [8] [22]
Infant factors change timing and interpretation. Prematurity, NICU care, transfusion, total parenteral nutrition and critical illness can invalidate or delay bloodspot sampling. Persistent transitional circulation and lung disease can produce false-positive CCHD screens. Family history, craniofacial anomalies, congenital infection and NICU stays raise concern for late-onset or progressive hearing loss even after a newborn pass. [10] [13]
Maternal factors matter. Maternal thyroid disease and antithyroid drugs change how you think about a borderline newborn TSH. Maternal medications, diabetes and substance use change examination and follow-up intensity. Language barriers, out-of-home care and prior healthcare distrust change whether follow-up appointments happen. [18]
DDH risk factors commonly taught at the bedside include breech presentation, family history of DDH and unstable or asymmetric hip findings. Exact imaging thresholds are local and age-dependent; examination alone misses some cases and over-calls others. [19] [20]
Jaundice risk rises with lower gestational age, exclusive breastfeeding with feeding difficulty, isoimmune haemolytic disease, bruising, East Asian ethnicity in some datasets, previous sibling with phototherapy and visible jaundice in the first 24 hours. The 2022 AAP hyperbilirubinemia guideline revises predischarge risk assessment for infants 35 or more weeks of gestation; use the current local implementation of that guidance rather than memorised older hour-specific cut-offs alone. [14] [15]
Pathophysiology
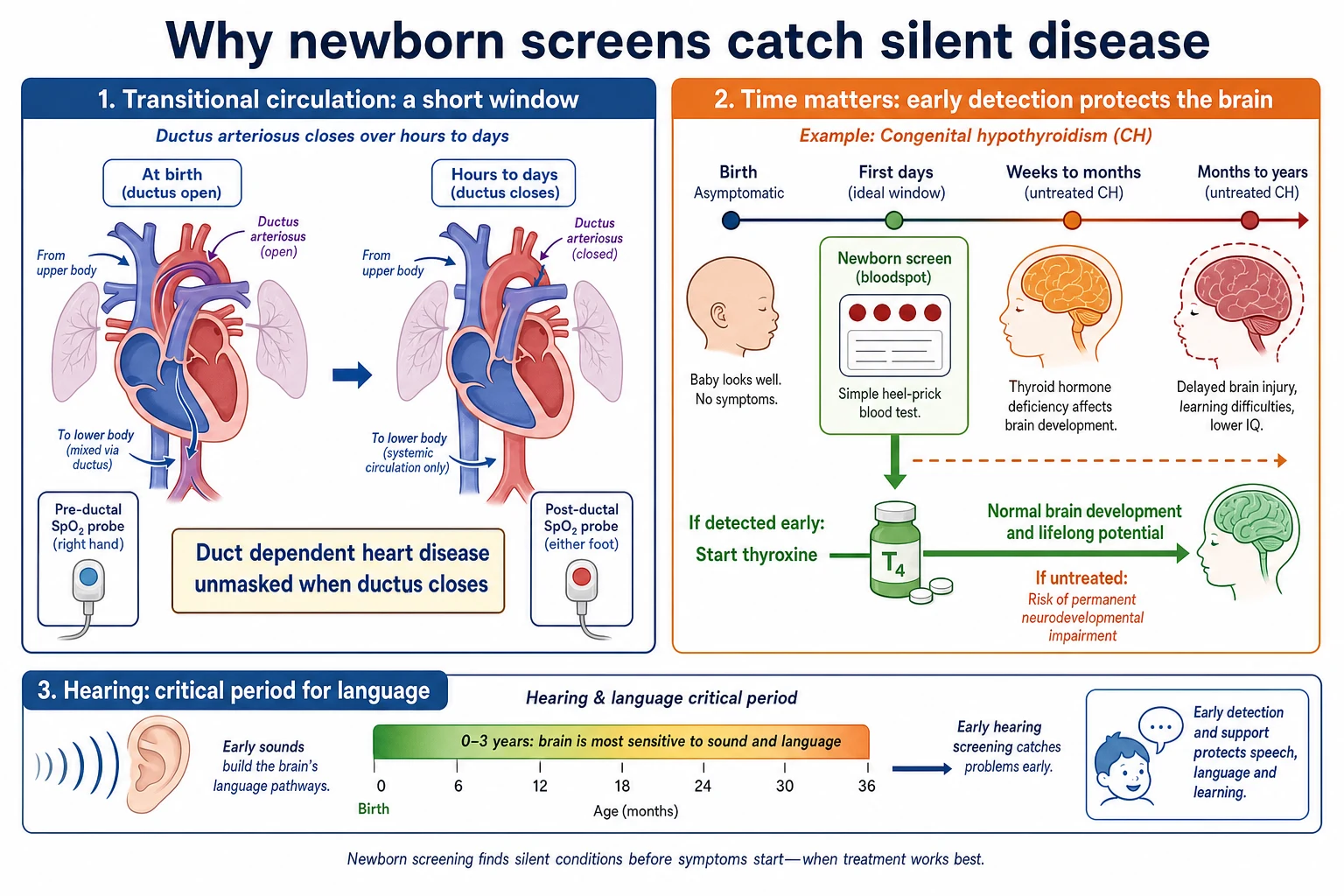
At birth the ductus arteriosus is still closing. Some infants with critical congenital heart disease maintain systemic or pulmonary blood flow through that duct. As the duct constricts over hours to days, hypoxaemia or shock can appear suddenly in a baby who looked pink on the first postnatal check. Timed pulse-oximetry screening aims to detect hypoxaemia before that collapse. [2] [5] [21]
Pre-ductal and post-ductal saturations compare right-hand oxygenation with foot oxygenation. A low absolute saturation or a meaningful pre–post difference can flag right-to-left ductal shunting or mixing lesions. The exact fail thresholds belong to the current algorithm you use, such as the updated AAP clinical report pathway. [4] [6]
Many bloodspot-target conditions cause no early signs because the fetus was supported by placental function or residual maternal hormone. Congenital hypothyroidism is the classic teaching example. Thyroid hormone is essential for brain development. Delayed treatment allows preventable neurodevelopmental injury even while the infant still feeds and grows. That is why a well baby with a critical TSH result is an emergency of systems, not of appearance. [18]
Vitamin K is required for clotting factors II, VII, IX and X. Newborn stores are low. Without prophylaxis, bleeding can occur early, in the classical first week, or late in infancy with high risk of intracranial haemorrhage when oral regimens are incomplete or malabsorption is present. [16] [17]
Unconjugated bilirubin can cross into the brain when levels are high relative to binding capacity and clinical context. Acute bilirubin encephalopathy can progress to kernicterus. Predischarge measurement and timed follow-up exist because visual inspection alone is unsafe. [14]
Permanent hearing loss disrupts the early auditory map that language needs. Neural plasticity is highest early. That is why a refer must become a diagnosis and intervention on a clock, not when the family next happens to attend. Auditory neuropathy spectrum disorder can pass an OAE-based screen and still impair hearing; risk-based AABR strategies matter in NICU populations. [10] [11]
Clinical Presentation
Most screen-positive newborns look well. That is the whole point of screening. Teach yourself to fear the calm baby with a critical result more than the slightly unsettled baby with a complete normal package. [8] [18]
CCHD may present as failed pulse oximetry, mild tachypnoea, poor feeding, grey colour, weak pulses, or sudden collapse as the duct closes. Some infants pass screening and still present later, especially with coarctation or lesions that do not produce early hypoxaemia. [3] [13]
Hearing loss has no reliable parent-visible sign in the first weeks. Parents may say the baby startles to bangs yet still have a significant loss for speech frequencies. Do not use bedside clap tests to cancel a refer. [10]
Vitamin K deficiency bleeding may show as oozing from the cord or puncture sites, gastrointestinal bleeding, or late catastrophic intracranial bleeding with vomiting, seizures or a bulging fontanelle. [17]
Severe hyperbilirubinemia shows as progressive jaundice, lethargy, poor feeding, high-pitched cry, tone change or arching when encephalopathy develops. Any jaundice in the first 24 hours is pathological until proved otherwise. [14]
After early discharge, caregiver observations that demand urgent review include poor feeding, fewer wet nappies, increasing jaundice, breathing difficulty, colour change, floppiness, fever or a parent who says the baby is different. Incomplete screens are themselves a presentation: the “problem” is system failure, not a symptom. [8] [14]
Differential Diagnosis
Failed CCHD pulse oximetry is not automatically heart disease. Consider lung disease, sepsis, persistent pulmonary hypertension, haemoglobinopathy, probe error, cold extremities and transitional delay. The differential still must include critical heart disease until a competent pathway says otherwise. [5] [13]
Hearing refer may reflect vernix or middle-ear fluid, noisy testing conditions, temporary conductive issues, permanent sensorineural loss or neural hearing loss. Your job is not to guess which one on the ward. Your job is to secure diagnostic audiology. [10] [11]
Abnormal bloodspot markers can reflect true disease, early or late sampling, transfusion, prematurity, total parenteral nutrition, maternal factors or laboratory artefact. Treat the clinical urgency of the reported condition while you sort pre-analytical causes with the laboratory. [8] [18]
Jaundice differentials include physiological jaundice, breastfeeding-associated jaundice, haemolysis, bruising, infection, metabolic disease and biliary obstruction. Conjugated hyperbilirubinemia is a different pathway from unconjugated disease and needs prompt cholestasis work-up. [14]
Hip clicks may be normal soft-tissue sounds, immature hips or true instability. Risk factors and repeated examination guide ultrasound or orthopaedic review according to local DDH pathways. [19] [20]
When parents decline screens or vitamin K, differentials include values-based refusal, misinformation, previous trauma in healthcare, access barriers and, rarely, safeguarding concern if critical follow-up is repeatedly avoided. Start with respectful curiosity, not confrontation. [16]
Clinical & Bedside Assessment
Start with the story that changes screens: gestation, birth events, maternal thyroid disease, family history of metabolic disease, hearing loss or DDH, consanguinity, early discharge plan, and who will actually bring the baby back. [8] [20]
Perform a calm, complete newborn examination. Check the red reflex in a dim room; an absent or white reflex needs urgent ophthalmology. Listen to the heart in a quiet infant and feel femoral pulses. Examine the hips with Ortolani and Barlow only if you are trained; force and repeated rough testing help no one. Inspect the spine and sacral region. Examine the genitalia and groin hernial orifices. Assess tone, alertness and feeding at the breast or bottle. [20]
For CCHD screening, use a motion-tolerant pulse oximeter designed for neonates when available. Measure after the transitional period defined by your algorithm, commonly after 24 hours when feasible, because earlier screening raises false positives. Record right-hand and foot saturations and follow the pass, repeat or fail branches exactly. [4] [7] [21]
For hearing screening, reduce noise, settle the infant, and document pass or refer language carefully. Do not invent a “borderline pass.” If the screen cannot be completed, label it incomplete and book completion. [11]
Assess feeding effectiveness, percentage weight change, stooling, voiding and visible jaundice before discharge. Use a predischarge bilirubin strategy consistent with the 2022 AAP guideline or your national equivalent, and give a timed follow-up that matches risk. [14] [15]
Assess parental capacity to complete the package: phone number that works, transport, language needs, understanding of why a well baby still needs a blood test, and who holds parental responsibility. [8]
Investigations
Dried bloodspot collection needs a warm heel, correct fill of circles, air drying and labelling that links the card to the right infant. Sampling too early can miss some conditions; sampling after transfusion can mask others. Follow your programme’s hour window and special-situation rules rather than improvising. [8]
After a failed CCHD screen, urgent clinical review comes first. Useful adjuncts may include four-limb blood pressures, blood gas, glucose, chest radiograph and echocardiography arranged without delay. Do not let a queue for non-urgent imaging replace senior review of a hypoxaemic neonate. [4] [21]
After hearing refer, the investigation is diagnostic audiology, not repeated casual ward screens used to cancel the pathway. Infants with NICU histories may need AABR-based strategies because OAE alone can miss neural loss. [10] [11]
For DDH, selective ultrasound is common in many systems when examination is abnormal or risk factors are present. Universal ultrasound remains debated because of cost, overtreatment and resource use; know the controversy and your local pathway. Radiographs are more useful later in infancy when ossification allows. [19] [20]
Bilirubin measurement should be interpreted with postnatal age in hours, gestation and neurotoxicity risk factors using current guidance, not with a single universal number remembered from an old textbook. [14]
Management — Resuscitation
If a newborn fails CCHD screening and becomes cyanosed, mottled or shocked, treat as a critically ill neonate. Call for senior and neonatal help. Support airway and breathing. Give oxygen according to neonatal guidance while you think about duct-dependent circulation. Obtain access, check glucose and prepare for prostaglandin discussion with cardiology when duct-dependent disease is likely. Pulse-oximetry screening is not a reason to delay resuscitation. [4] [5]
Suspected acute bilirubin encephalopathy needs immediate senior review, intensive phototherapy pathways and preparation for escalation according to local neonatal intensive care practice. [14]
Suspected vitamin K deficiency bleeding needs urgent vitamin K administration, blood product support as indicated and investigation of intracranial bleeding when neurological signs are present. Prevention is far better than rescue. [17]
A neonate who presents acidotic, encephalopathic or collapsing with a missed metabolic screen needs ABCDE care, glucose management, stopping feeds when indicated, and urgent metabolic specialist involvement. Exact metabolic cocktails are condition-specific and must come from current specialist advice. [8]
Management — Definitive & Stepwise
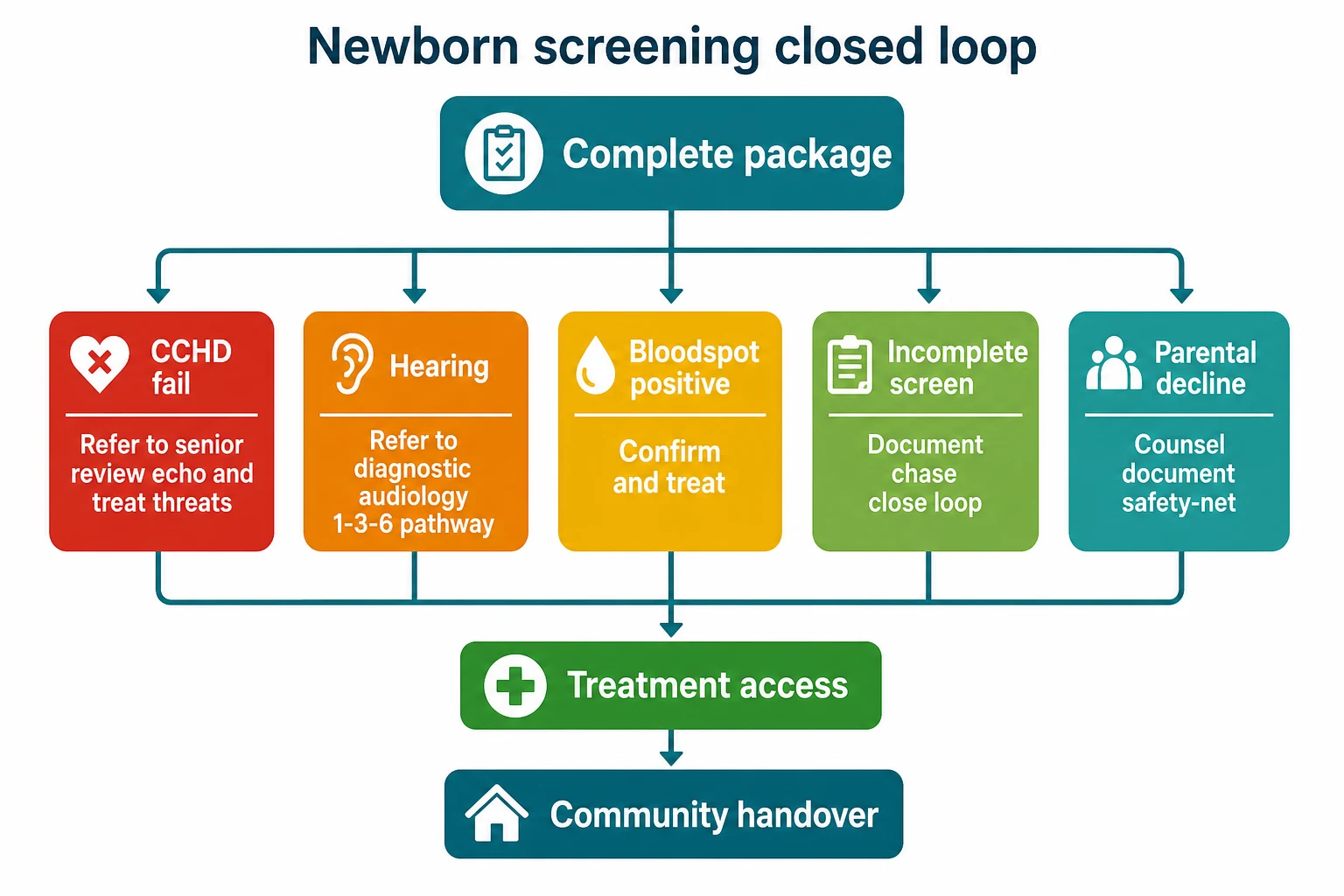
Complete the package
Before discharge, document examination, vitamin K, bloodspot status, hearing status, CCHD oximetry status, jaundice plan and hip plan. Incomplete items get a named clinician, a date and a communication path to the family. [8] [13]
CCHD fail pathway
Follow the current algorithm for immediate fail versus repeat windows. A confirmed fail needs prompt senior review and echocardiography access. While awaiting imaging, monitor, support physiology and avoid false reassurance because the baby is feeding. Implementation studies show programmes work only when the fail pathway is resourced. [2] [4] [12]
Hearing refer pathway
Explain that refer means more testing, not proven deafness. Book diagnostic audiology against the local time standard. Identify risk factors for progressive loss and ensure ongoing surveillance even after a later pass when risk remains. Early intervention services start when permanent loss is confirmed. [9] [11]
Bloodspot positive pathway
Contact the family the same day for critical results. Bring the infant back for confirmatory tests and, when indicated, start treatment before permanent harm. Congenital hypothyroidism pathways typically combine urgent free T4/TSH confirmation with early levothyroxine once the clinical laboratory pathway supports treatment, under specialist or protocolised guidance. Do not invent microgram-per-kilogram figures from memory in an exam if you cannot source them; state that you would use the current national dosing protocol. [18]
Vitamin K
Intramuscular vitamin K at birth is the most reliable route for preventing late vitamin K deficiency bleeding in standard teaching and narrative reviews. Oral regimens can be offered in some jurisdictions when intramuscular injection is declined, but they require complete multi-dose adherence and still leave residual risk, especially with malabsorption. Document the discussion, the regimen and follow-up. [16] [17]
Jaundice and DDH
Use predischarge bilirubin risk assessment and timed community measurement. For DDH, re-examine, arrange selective imaging when indicated, and refer unstable hips promptly. [14] [20]
Specific Subtypes & Scenarios
Early discharge within 24 hours. Compresses CCHD timing, bloodspot windows and jaundice surveillance. If discharge proceeds, every deferred test needs an appointment, not a vague instruction. [4] [14]
Home birth or freebirth with delayed presentation. Treat the first clinical contact as day zero for the package. Do not assume community services already completed screening. [8]
NICU graduate. Screens may have been modified, delayed or repeated. Verify what was actually completed before transfer to the ward or home. AABR-based hearing strategies often apply. [11] [13]
Rural maternity unit without on-site echocardiography. A CCHD fail needs early retrieval or transfer planning, not overnight observation without a destination. [22]
Parental decline of vitamin K or bloodspot. Explore reasons, correct specific misconceptions, offer lawful alternatives where they exist, document residual risk, and ensure the infant is not lost to follow-up. Escalation to safeguarding is for clear risk of significant harm with avoidance of critical care, not for every values-based refusal. [16]
Complications & Pitfalls
False positives create parental anxiety, extra tests and possible overtreatment. Mitigate with clear language: “This is a screen, not a diagnosis.” False negatives create false confidence. A CCHD pass does not exclude all congenital heart disease. A hearing pass does not guarantee lifelong normal hearing. [3] [10] [13]
Early bloodspot sampling, poor card quality and mislabelling cause programme errors. Screening CCHD too early increases false positives; screening without a fail pathway increases harm. Incomplete documentation is a silent failure mode. [7] [8]
Delayed treatment of congenital hypothyroidism, late presentation of CCHD, late vitamin K deficiency bleeding and delayed hearing intervention are the outcomes that make this topic examinable. [9] [17] [18]
Prognosis & Disposition
Safe disposition after birth is not “feeding well.” It is “package complete or package owned.” A well infant with a failed CCHD screen does not go home before the pathway is complete. A well infant with a pending non-critical bloodspot result may go home only if contact details work and the family understands how results return. [4] [8]
Hearing refer disposition always includes a booked diagnostic visit. Jaundice disposition includes a timed bilirubin check matched to risk. DDH disposition includes imaging or orthopaedic timing that matches age and findings. [11] [14] [20]
Long-term outcomes are excellent for many screened conditions when treatment starts early. Congenital hypothyroidism treated promptly has a far better neurodevelopmental outlook than historical late presentations. Permanent hearing loss managed early supports better language trajectories. Missed CCHD still carries mortality and morbidity risk. [9] [12] [18]
Special Populations
Preterm and unwell infants need individualised timing, sometimes repeated bloodspots, and careful interpretation of oximetry against lung disease. Indigenous, rural and remote families need discharge plans that match real travel times and culturally safe communication, not urban default assumptions. Migrant and refugee families may lack records and need interpreter-supported consent and result notification. Out-of-home care requires clarity on who can consent and who receives results. Technology-dependent or anomalied newborns need the same screens plus lesion-specific follow-up. [8] [22]
Evidence, Guidelines & Regional Differences
Cochrane synthesis supports pulse-oximetry screening for critical congenital heart defects as a test with high specificity and moderately high sensitivity, useful as an adjunct to examination. Large Swedish implementation work showed improved detection of duct-dependent disease. US policy and AAP clinical reports translated that evidence into algorithms, with a 2025 update refining practice. Nordic groups have published implementation lessons and calls for uniform standards. [2] [3] [4] [7]
Hearing evidence and quality standards centre on early detection and intervention; local EHDI or national programmes set operational clocks. Point-of-care newborn screening needs the governance framework Kemper and colleagues outlined. [8] [9] [11]
Hyperbilirubinemia care for infants ≥35 weeks should follow the 2022 AAP revision or the equivalent national guideline where you practise. Vitamin K evidence continues to favour reliable prophylaxis and attention to late VKDB when regimens fail. DDH policy remains mixed between selective and universal ultrasound strategies. [14] [16] [19]
Australia and Aotearoa New Zealand run state, territory or national bloodspot panels that are not identical; always quote the local panel. Newborn hearing screening is widespread. CCHD pulse-oximetry implementation varies by maternity service and should be confirmed locally. Culturally safe follow-up for Aboriginal, Torres Strait Islander, Māori and Pacific families includes realistic geography and whānau participation. [4] [12]
United Kingdom combines newborn blood spot screening, the NIPE examination, newborn hearing screening and local pulse-oximetry policies. NICE and national screening programme handbooks govern operational detail. [3] [8]
United States uses state-based dried bloodspot panels, EHDI hearing programmes and AAP CCHD algorithms. Condition lists differ by state. [4] [12]
Canada uses provincial programmes with panel and logistics variation; remote geography often dominates follow-up design. [22]
State only differences you have checked against current official programme pages. Do not invent a universal condition list. [1]
Exam Pearls
- A well baby can still be a time-critical patient after a critical screen. [18]
- CCHD pass ≠ normal heart. Hearing pass ≠ lifelong normal hearing. [10] [13]
- Give the algorithm you use for oximetry; do not invent saturation cut-offs if you cannot source them live. [4]
- Intramuscular vitamin K is the most reliable standard prophylaxis route in most teaching reviews; oral alternatives need complete dosing. [16]
- First-24-hour jaundice is never “physiological” by default. [14]
- Ortolani and Barlow are adjuncts, not a complete DDH programme. [20]
- False positives are programme harms you must counsel through. [1]
- Rural CCHD fail means early destination planning. [22]
- Handover language should list each screen’s status in one sentence. [8]
- Boards test whether you can close the loop, not whether you can name every analyte. [1]
NEWBORN package
References
- [1]Andermann A Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Journal, 2008.PMID 18438522
- [2]de-Wahl Granelli A Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns. Journal, 2009.PMID 19131383
- [3]Plana MN Pulse oximetry screening for critical congenital heart defects. Journal, 2018.PMID 29494750
- [4]Oster ME Newborn Screening for Critical Congenital Heart Disease: A New Algorithm and Other Updated Recommendations: Clinical Report. Journal, 2025.PMID 39679594
- [5]Jullien S. Newborn pulse oximetry screening for critical congenital heart defects. Journal, 2021.PMID 34496777
- [6]Mahle WT Endorsement of Health and Human Services recommendation for pulse oximetry screening for critical congenital heart disease. Journal, 2012.PMID 22201143
- [7]de-Wahl Granelli A Nordic pulse oximetry screening--implementation status and proposal for uniform guidelines. Journal, 2014.PMID 25060211
- [8]Kemper AR A framework for key considerations regarding point-of-care screening of newborns. Journal, 2012.PMID 22899090
- [9]Kemper AR. Universal newborn hearing screening improves quality of life for children with permanent hearing impairment. Journal, 2011.PMID 21482247
- [10]Grindle CR. Pediatric hearing loss. Journal, 2014.PMID 25361905
- [11]Awad R Meeting the Joint Committee on Infant Hearing Standards in a Large Metropolitan Children's Hospital: Barriers and Next Steps. Journal, 2019.PMID 31084570
- [12]Kemper AR The Success of State Newborn Screening Policies for Critical Congenital Heart Disease. Journal, 2017.PMID 29209703
- [13]Oster ME Lessons Learned From Newborn Screening for Critical Congenital Heart Defects. Journal, 2016.PMID 27244826
- [14]Kemper AR Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Journal, 2022.PMID 35927462
- [15]Daggle L Management of Neonatal Hyperbilirubinemia: Shedding Light on the American Academy of Pediatrics 2022 Clinical Practice Guideline Revision. Journal, 2024.PMID 38852082
- [16]Mirone A Vitamin K Prophylaxis in Newborns: A Narrative Review of the Molecular Basis, Clinical Evidence, and Comparative Effectiveness of Intramuscular Versus Oral Administration and Parental Hesitation. Journal, 2026.PMID 41751806
- [17]Perrone S Late Vitamin K Deficiency Bleeding in Infancy: The Time to Ensure Effective Prevention. Journal, 2025.PMID 41241783
- [18]Cavarzere P Primary congenital hypothyroidism: a clinical review. Journal, 2025.PMID 40862110
- [19]Alassaf N. Universal ultrasound screening and early treatment of developmental dysplasia of the hip: a critical review. Journal, 2024.PMID 39539433
- [20]Alam AE Developmental Dysplasia of the Hip: Management from a Pediatrician Perspective. Journal, 2026.PMID 42131112
- [21]Frank LH Critical congenital heart disease screening using pulse oximetry. Journal, 2013.PMID 23266220
- [22]Hom LA Newborn Critical Congenital Heart Disease Screening Using Pulse Oximetry: Value and Unique Challenges in Developing Regions. Journal, 2020.PMID 33123641