Paeds · preventive-and-community-paediatrics
Preschool health supervision
Also known as Preschool well-child visit · Pre-school health check · School readiness health supervision · 3 to 5 year preventive visit · Bright Futures preschool
Fellowship approach to preschool (about 3–5 years) health supervision: growth and BMI, school-readiness surveillance, vision and hearing gates, oral health and fluoride, immunisation review, behaviour sleep and media, injury prevention, equity and safeguarding, with regional schedule differences and safety-netting.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
P.R.E.S.C.H.O.O.L. visit
Overview & Definition
Picture a four-year-old on the examination table for a “school check.” The parent wants vaccines signed off. Your real job is broader. Preschool health supervision is structured preventive care for children roughly three to five years of age, before or around formal school entry. It combines measurement, developmental surveillance, sensory screening pathways, oral health, immunisation reconciliation, behaviour and lifestyle guidance, and social risk assessment. [1] [4]
AAP preventive periodicity recommendations organise these visits as a repeating package rather than a single birthday ritual. Local child health books in Australia and Aotearoa New Zealand, and the UK Healthy Child Programme, use different forms but the same idea: find problems early enough to change the school trajectory. [4]
This page owns the preschool package. Cross-link dedicated leaves for full immunisation schedules, detailed growth charting technique, and deep autism management rather than hiding whole second chapters here. [1] [4]
Classification
Sort the visit by purpose and by finding. [1] [4]
By purpose. Full well-child preschool visit. School-entry health assessment with incomplete records. Opportunistic preventive add-on during a mild illness review. Catch-up visit after missed care. [4]
By finding. Normal with anticipatory guidance only. Isolated speech or motor lag. Multi-domain delay. Social communication pattern concerning for autism. Sensory concern (vision or hearing). Rising BMI or faltering growth. Oral disease. Incomplete immunisation. Safeguarding concern. Medical complexity needing individualised goals. [1] [3] [10]
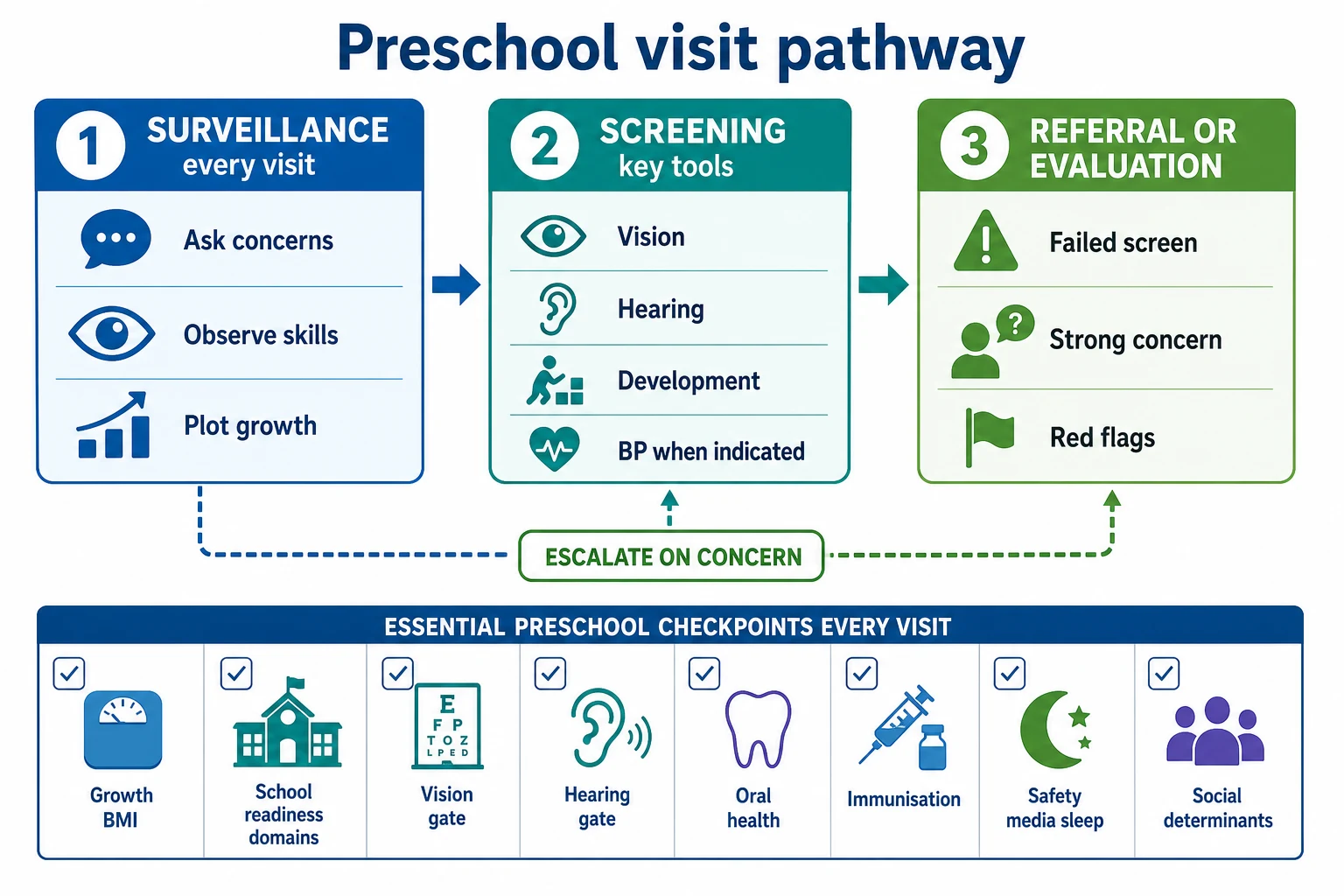
Surveillance versus screening versus evaluation. Surveillance is continuous: ask, watch, document. Screening uses a validated tool or structured sensory pathway at key ages or on concern. Evaluation is specialist or multidisciplinary work that can diagnose and open services. Autism-specific tools such as M-CHAT-R/F are validated for toddler risk stratification with follow-up; they are not a full preschool developmental diagnosis on their own. [1] [3]
Epidemiology & Risk Factors
Missed preschool preventive care clusters with poverty, transport barriers, housing instability, language discordance and fragmented out-of-home care. Those same children carry higher burdens of untreated caries, uncorrected vision problems, incomplete immunisation and delayed speech support. [10] [12]
Caregiver concern is not soft data. In acute care it associates with serious illness; the same habit applies in preventive clinic: “I am worried about speech” or “teachers cannot understand her” should change your plan the same day you hear it. [11]
Lead exposure risk varies by housing, migration pathway and local environment. USPSTF evidence for universal elevated blood lead screening is limited for asymptomatic children, so high-risk local policy and clinical judgement matter more than a single global rule. [9] Obesity risk rises with sugar-sweetened drinks, short sleep and high recreational screen time. [5] Road traffic injury remains a leading cause of severe paediatric trauma; child passenger restraint errors are common and fixable in anticipatory guidance. [8]
Pathophysiology
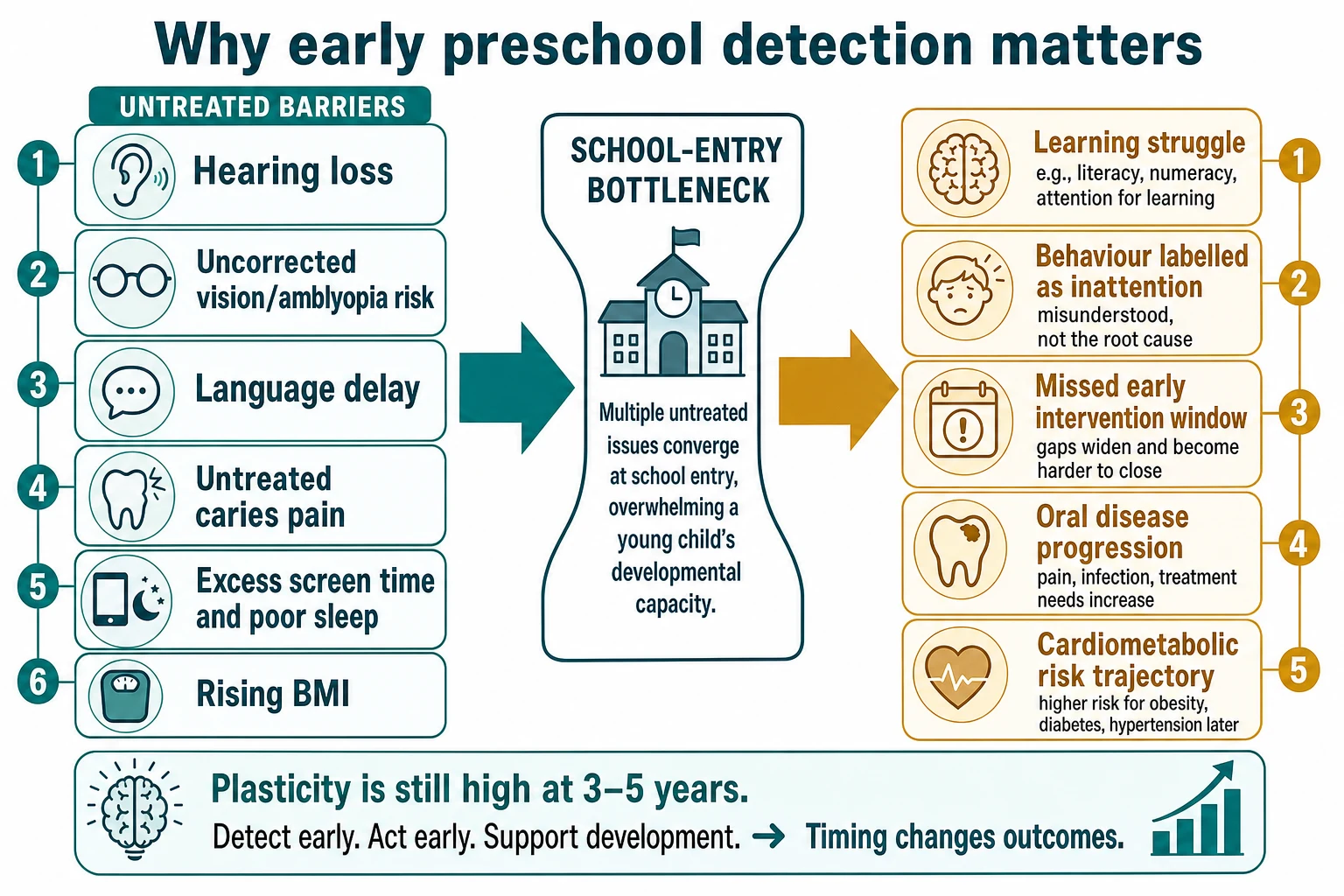
Between three and five years, language, executive attention and social reciprocity expand quickly. Skills stack. If hearing input is degraded, refractive error blurs near work, chronic dental pain steals sleep, or the home cannot support practice of words and play, the visible school-readiness pattern falls behind. Early detection does not “create IQ,” but it opens therapy, glasses, audiology, dental care and family support while catch-up is still realistic. [1] [2]
Dental caries is a biofilm disease driven by frequent sugar exposure and inadequate fluoride. Primary-care fluoride toothpaste counselling and, where programmes allow, fluoride varnish reduce caries risk; the mechanism is remineralisation and inhibition of demineralisation, not “hardening teeth overnight.” [6]
Energy imbalance, short sleep and passive media displace active play and family talk. That pathway links behaviour complaints to weight trajectory without blaming the child. [5] Trauma and toxic stress alter arousal, attention and trust. Trauma-informed care changes how you examine and counsel; it does not replace a careful developmental assessment. [15]
Blood pressure tracking becomes more relevant as children grow. Incorrect cuff size and single elevated readings mislead; confirmed hypertension needs a proper pathway, not a casual “high in clinic” label. [7]
Clinical Presentation
Many children look well. The visit may be framed as “forms for kindergarten.” Listen for quieter presentations: a child who sits too close to screens, ignores name in a noisy room, uses few word combinations, has nightly tantrums from toothache, or wets daily after a dry spell. Teachers may report inattention that is actually blurred vision or sleep debt. [1] [2]
Parents may minimise: “Boys talk late in our family.” Your job is to check the evidence-informed milestone picture, not family folklore. [2] Regression of language or social skills is never a routine preschool delay story — it is a prompt for urgent evaluation. [1] [3]
Differential Diagnosis
Speech concern. Isolated speech-language delay versus hearing impairment versus autism-related social communication difference versus global developmental delay versus extreme psychosocial deprivation. Always keep hearing on the list. [1]
“Inattentive in preschool.” Sensory deficit, sleep insufficiency, iron deficiency in selected contexts, developmental delay, emerging ADHD pattern (usually needs careful school-age assessment rather than instant diagnosis at three), anxiety, or chaotic environment. [1] [5]
Growth concern. Measurement error, familial short stature pattern, constitutional delay, chronic disease, endocrine disease, neglect. Plot BMI-for-age for excess weight; do not use adult BMI cut-offs. [4]
Injury. Developmental stage-appropriate accident versus supervision gap versus maltreatment. Pattern, delay in presentation and story consistency matter. [15]
Clinical & Bedside Assessment
Start with the child and caregiver together. Open with: “What questions do you have before school?” and “Do you have any concerns about talking, playing, hearing, seeing, behaviour or toileting?” Then watch the child: joint attention, conversation attempts, following two-step directions, pencil or crayon grasp, gait, and how they use the caregiver. [1] [2]
Growth. Measure height and weight with correct technique. Plot on the chart your service uses. Calculate and plot BMI-for-age. Comment on trend, not a single point. [4]
Blood pressure. When your periodicity schedule or clinical context calls for BP, use an appropriately sized cuff and interpret with paediatric tables; confirm elevations before labelling disease. [7]
Development and school readiness. Cover speech intelligibility to strangers, conversation, pretend play, peer interest, toileting progress, dressing help needed, and separation at preschool. Use evidence-informed milestone content rather than memorised folklore ages. [2] Deploy validated general developmental screens per local programme. For autism risk in the toddler window supported by evidence, M-CHAT-R/F with follow-up interview risk-stratifies; older preschoolers with social communication concern need local autism pathway referral rather than false reassurance from an age-mismatched tool. [1] [3]
Vision and hearing. Follow local office screening capability. If the child cannot complete a screen, or caregivers report concerns, refer rather than document “unable” and stop. [4]
Mouth. Look for obvious caries, pain, abscess or severe enamel problems. Ask about brushing twice daily with fluoride toothpaste of age-appropriate smear/pea amount per local advice, bottle or sippy cup with sweet drinks, and dental home. [6]
Safety and lifestyle. Car restraint type and position, water safety, smoke alarms, firearm storage where relevant, bike helmets, sleep duration, and recreational screen time. Media guidance for young children emphasises limited high-quality co-viewed content rather than unrestricted solo screen time. [5] [8]
Social determinants and safeguarding. Food security, housing, caregiver mental health, family violence, and who else cares for the child. Use professional interpreters when language is discordant — never the preschooler. [12] [15]
Document domain by domain and source of each report so the next clinician can continue the story. Structured handover reduces lost abnormal results. [13]
Investigations
Most preschool well visits need no blood test. Investigate when the story or examination demands it. [1] [4]
First-line when communication or school concerns dominate. Formal audiology and vision assessment pathways as indicated. [1]
Lead. Do not invent a universal capillary lead for every preschooler. USPSTF found insufficient evidence for routine screening of asymptomatic children; apply high-risk criteria and local public health policy. [9]
Blood pressure follow-up. Repeated measurements; ambulatory pathways per paediatric hypertension guidance when confirmed high. [7]
Growth or obesity labs. Directed, not shotgun. Chronic disease symptoms, severe faltering, or local obesity pathway triggers guide tests. [4]
Avoid genetic mega-panels from a single mild speech lag without evaluation context. [1]
Management — Resuscitation
A well-child clinic still finds emergencies. Collapse, severe respiratory distress, seizures, unexplained bruising with instability, or a child who cannot protect their airway needs acute paediatric pathways immediately — not a completed anticipatory guidance checklist. [11]
Safeguarding emergencies and mandatory reporting obligations run in parallel with medical care when injury patterns or disclosures demand them. [15] Acute severe visual symptoms or sudden hearing loss need urgent specialty access. [4]
Management — Definitive & Stepwise
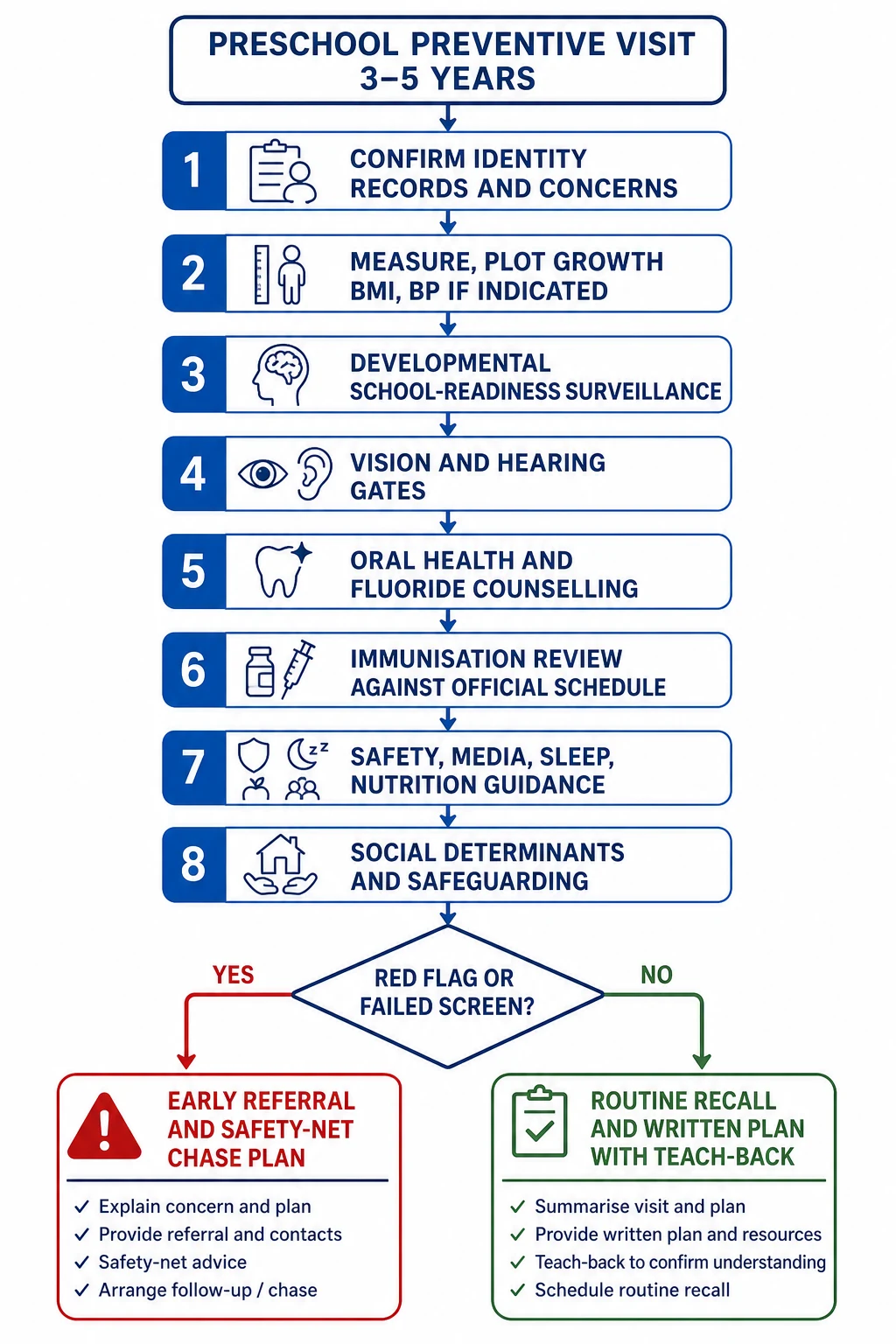
- Confirm identity, records and agenda. Ask caregiver priorities first. [14]
- Measure and plot growth, BMI-for-age, and BP when indicated. [4] [7]
- Run developmental and school-readiness surveillance; use validated screens per local schedule. [1] [2]
- Complete vision and hearing gates or refer if incomplete/abnormal. [4]
- Inspect the mouth; counsel fluoride toothpaste and dental home; apply varnish only within your trained local programme. [6]
- Reconcile immunisations against the official national or jurisdictional schedule; plan catch-up without inventing doses from memory. [4]
- Deliver anticipatory guidance: sleep, media co-viewing limits, nutrition, toilet readiness, car restraints and water safety. [5] [8]
- Address social risk and offer concrete supports; open safeguarding routes when required. [15]
- Explain the plan with teach-back, written points, and a chase plan for referrals. Consent and information-sharing rules still apply when you contact preschool or agencies. [14] [16]
Strong clinical concern can justify referral even if a family declines a paper screen or a tool is incomplete. [1]
Specific Subtypes & Scenarios
School-entry paperwork visit. Do not sign “normal” without growth, development and sensory review. Incomplete overseas records need a catch-up immunisation plan from the official handbook, not guesswork. [4]
Speech concern at 3–4 years. Full surveillance, hearing pathway, consider autism features, early speech-language referral, and safety-net while waiting. [1] [2]
Rising BMI. Plot BMI-for-age, take a non-shaming diet and activity history, address sugar drinks and screens, screen for comorbidities per local pathway, and set family goals. [4] [5]
Refugee or migrant preschooler. Interpreter, trauma-informed history, catch-up vaccines, dental and sensory screens, and schooling support links. [12] [15]
Out-of-home care. Assume disrupted records and higher adversity burden; complete a full package and share plans with carers and agencies lawfully. [15]
Medical complexity. Ask what is new for this child. Prevent diagnostic overshadowing — known cerebral palsy does not explain new vision loss or untreated caries. [10]
Possible autism beyond the classic toddler screen window. Do not force an age-mismatched checklist as reassurance. Refer on clinical concern to local developmental-behavioural pathways. [1] [3]
Complications & Pitfalls
“Wait until school — teachers will sort it.” Skipping vision and hearing because conversation seems fine in a quiet room. Treating a screen score as a diagnosis. Using the child as interpreter. Shaming weight or parenting. Signing immunisation forms without checking the official schedule. Losing abnormal results between clinic and specialist. [1] [12] [13]
Promising “they will grow out of it” after regression is a serious error. [1]
Prognosis & Disposition
Earlier access to speech therapy, audiology, ophthalmology, dental care and early childhood education supports improves function for many children. Disposition is not binary. Options include routine recall, early nurse or GP review, allied health referral, paediatric developmental clinic, dental urgent care, or safeguarding pathways. Always leave a written safety-net: what to watch for, how to chase appointments, and when to return sooner. [1] [16]
Special Populations
Indigenous families. Culturally safe care, community-controlled service partnership where available, and respect for family structure without lowering clinical standards. [12]
Language-discordant families. Professional interpreters for history, screens and counselling. [12]
Disability and neurodiversity. Affirming language, sensory-aware examination, and goals defined with the family. [10]
Socioeconomic disadvantage. Food insecurity and transport shape adherence; write plans families can actually do. [10]
Trauma-exposed children. Predictable examination steps, choice where safe, and no forced “smile for the doctor” theatre. [15]
Evidence, Guidelines & Regional Differences
Lipkin and colleagues frame developmental surveillance plus screening for early identification. [1] Zubler and colleagues supply evidence-informed milestone content that reduces false reassurance from outdated lists. [2] Robins and colleagues validated M-CHAT-R/F with follow-up for toddler autism risk screening. [3] AAP periodicity recommendations structure preventive content across ages. [4] Media and Young Minds guides early childhood screen advice. [5] Clark and colleagues detail fluoride use in primary care caries prevention. [6] Flynn and colleagues provide the paediatric BP screening and management framework. [7] Durbin and colleagues summarise child passenger safety principles. [8] USPSTF states the evidence limits for universal lead screening in asymptomatic children. [9]
Use jurisdictional child health books, local vision and hearing programmes, and the Australian Immunisation Handbook or New Zealand schedule for vaccines. Cultural safety and interpreter access are part of valid supervision. Confirm fluoride varnish programmes before promising chairside application. [4] [6] [12]
Healthy Child Programme contacts, school-entry hearing and vision pathways, and NICE autism recognition guidance shape thresholds. Map local health visitor and community paediatric routes rather than importing US tool ages wholesale. [1]
Bright Futures and AAP periodicity tables drive many clinic checklists; Canadian provincial programmes vary. State the local tool and lead policy rather than inventing universal cut-offs. [4] [9]
Exam Pearls
- Preschool visit equals school readiness plus sensory gates, not vaccines alone. [4]
- Caregiver concern is data — write it and act. [11]
- Use evidence-informed milestones, not folklore. [2]
- A screen is not a diagnosis. [1] [3]
- BMI-for-age for preschool weight status. [4]
- Correct cuff size before trusting BP. [7]
- Fluoride toothpaste counselling is core primary care oral health. [6]
- Name the official immunisation schedule when planning catch-up. [4]
- Professional interpreter; never the child. [12]
- Safety-net every referral wait. [16]
References
- [1]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [2]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [3]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [4]COMMITTEE ON PRACTICE AND AMBULATORY MEDICINE 2023 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2023.PMID 36938620
- [5]COUNCIL ON COMMUNICATIONS AND MEDIA Media and Young Minds. Pediatrics, 2016.PMID 27940793
- [6]Clark MB Fluoride Use in Caries Prevention in the Primary Care Setting. Pediatrics, 2020.PMID 33257404
- [7]Flynn JT Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics, 2017.PMID 28827377
- [8]Durbin DR Child passenger safety. Pediatrics, 2011.PMID 21422094
- [9]US Preventive Services Task Force Screening for Elevated Blood Lead Levels in Children and Pregnant Women: US Preventive Services Task Force Recommendation Statement. JAMA, 2019.PMID 30990556
- [10]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [11]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [12]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [13]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [14]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [15]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [16]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428