Paeds · preventive-and-community-paediatrics
Preventive paediatrics and the well-child visit
Also known as Well-child care · Health supervision visit · Bright Futures visit · Preventive pediatric health care · Child health check
Fellowship hub on preventive paediatrics and the well-child visit: visit architecture, Bright Futures/periodicity principles, growth and development, screening, immunisation integration, anticipatory guidance, social determinants, safety, equity redesign, and when to convert a well visit to acute or safeguarding care.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother books a “nine-month check.” She wants sleep advice. The nurse notes the baby is not yet sitting with support. The growth chart is incomplete. Vaccines may be due. That single slot is the well-child visit: a planned health-supervision encounter that tries to prevent harm, find problems early, and strengthen the family’s plan for the months ahead. [1] [9]
Preventive paediatrics is the part of child health that acts before crises. Primary prevention stops problems starting (immunisation, safe sleep counselling, car-seat guidance). Secondary prevention finds problems early (vision screen, developmental screen, lead testing when indicated). Tertiary prevention limits harm from known disease (care coordination for a child with medical complexity attending for routine surveillance). The well-child visit is where those layers meet the child. [1] [14] [21]
The US Bright Futures / periodicity framework is a widely used map of recommended preventive content by age. It is not a global statute. In Australia and Aotearoa New Zealand you still use local child-health books, immunisation schedules and screening programmes. In the UK, the Healthy Child Programme frames universal contacts. In Canada, tools such as Rourke Baby Record guide many primary-care visits. The exam skill is the same everywhere: know the components, prioritise under time pressure, and name your local operational source. [1] [2]
Core well-child visit spine
Is the child well and safe?
If no, convert to acute or safeguarding pathway.
Shared agenda
Ask what the family wants from today before your checklist.
Growth and examination
Measure carefully; examine with age-adapted focus.
Development and behaviour
Surveillance every visit; standardised screens at key ages.
Screening and immunisation
Do indicated screens; review and give vaccines with consent.
Guidance, social context, plan
Safety, oral health, mood, social needs; document and close loops.
Classification
Start with what you are trying to do for this child today. Then classify the visit content so nothing important is left to chance. [1] [16]
Prevention levels
Primary prevention reduces incidence. Examples: vaccines, injury-prevention counselling, fluoride where indicated, supporting responsive parenting and play. [13] [14] [26]
Secondary prevention detects disease or delay early. Examples: developmental and autism screening pathways, vision assessment, risk-based lead testing, perinatal mood screening in the paediatric setting. [3] [5] [6] [12]
Tertiary prevention reduces complications when a condition already exists. Examples: structured surveillance for a preterm graduate, care coordination for special health care needs, school supports for a child with known developmental disorder. [10] [21] [22]
Visit component domains
| Domain | What you actually do | Common trap |
|---|---|---|
| Relationship and agenda | Greet, ask parent/child goals, use interpreter when needed | Launching into your list first |
| Growth and physical exam | Measure, plot, examine age-focused systems | One-off numbers without trajectory |
| Development and behaviour | Surveillance every visit; screens at key ages | “Wait and see” after clear concern |
| Screening tests | Vision, hearing, labs only when indicated | Shotgun bloods in a well child |
| Immunisation | Review record, catch up, consent, observe | Assuming the record is complete |
| Anticipatory guidance and social care | Safety, sleep, feeding, oral health, SDOH, mood | Talking at families without asking needs |
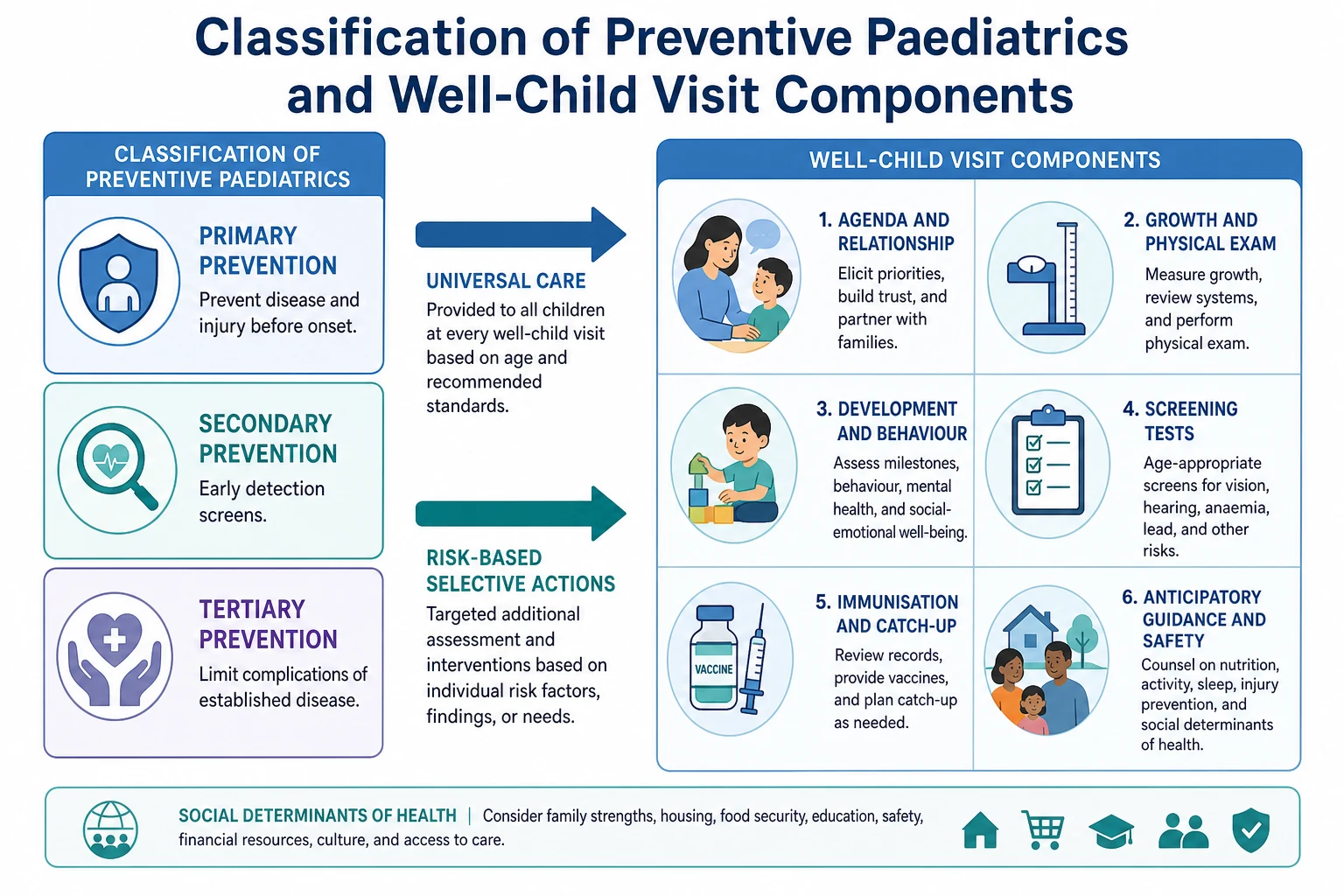
Read the figure like this: if time is short, you still need a safety net across domains. Dropping development “because vaccines took the slot” is how delay is missed. [3] [9]
Universal versus selective actions
Some actions are intended for almost every child at a given age band (for example, developmental surveillance at every visit). Others are risk-based (lead testing strategy, some laboratory tests, intensified social support). Exams love this distinction. Do not invent a universal blood panel for every asymptomatic child. [1] [12] [24]
Epidemiology & Risk Factors
Missed well-child care is not random. Children in poverty, with unstable housing, transport barriers, racism in care systems, language discordance or fragmented insurance/access patterns receive less complete preventive content. That gap is clinical, not only political. [8] [23] [24]
Parents often leave visits without the guidance they wanted. Schuster’s classic work showed a mismatch between information received and information desired. If you only recite your preferred topics, you may miss the family’s real risk. [7]
High-content ages (including around 9 and 24 months in Bright Futures workflows) are easy to under-deliver. Quality-improvement work shows that deliberate redesign can improve delivery of recommended preventive services. [9]
Children in foster or kinship care frequently present with incomplete immunisation and medical history. They need rapid medical-home assignment and catch-up, not a polite deferral until “things settle.” [20]
Medical-home attributes and developmental monitoring associate with earlier autism identification pathways in population analyses. The practical message is simple: a named home that actually screens and refers beats episodic care. [10] [16] [22]
Pathophysiology
Why does a quiet clinic visit matter years later? Early childhood is a period of rapid brain wiring. Skills build on earlier skills. If a baby cannot hear well, language maps form on a weaker signal. If severe, unbuffered stress is repeated, stress-response systems stay on high alert. Garner and colleagues framed this as toxic stress: prolonged activation of stress systems without adequate adult buffering. Adversity is not destiny, but it is not neutral biology either. [11]
Missed detection creates cascade harm. Untreated vision problems make reading harder. Unrecognised developmental delay delays early intervention during higher plasticity. Untreated dental caries causes pain, sleep loss and infection risk. Lead exposure can impair cognition; prevention and risk-based testing exist because the damage is easier to avoid than reverse. [6] [12] [13] [15]
Caregiver depression changes the child’s environment. A mother with major perinatal depression may struggle with feeding, sleep routines and help-seeking. Screening inside paediatric visits is justified because the infant’s medical home often sees the dyad most often. [5] [28]
Relational trust is a mechanism, not soft talk. Families disclose food insecurity, violence or adolescent risk more readily when they are known. Fragmented care lowers that disclosure and raises duplicated tests and conflicting advice. [16] [21] [23]
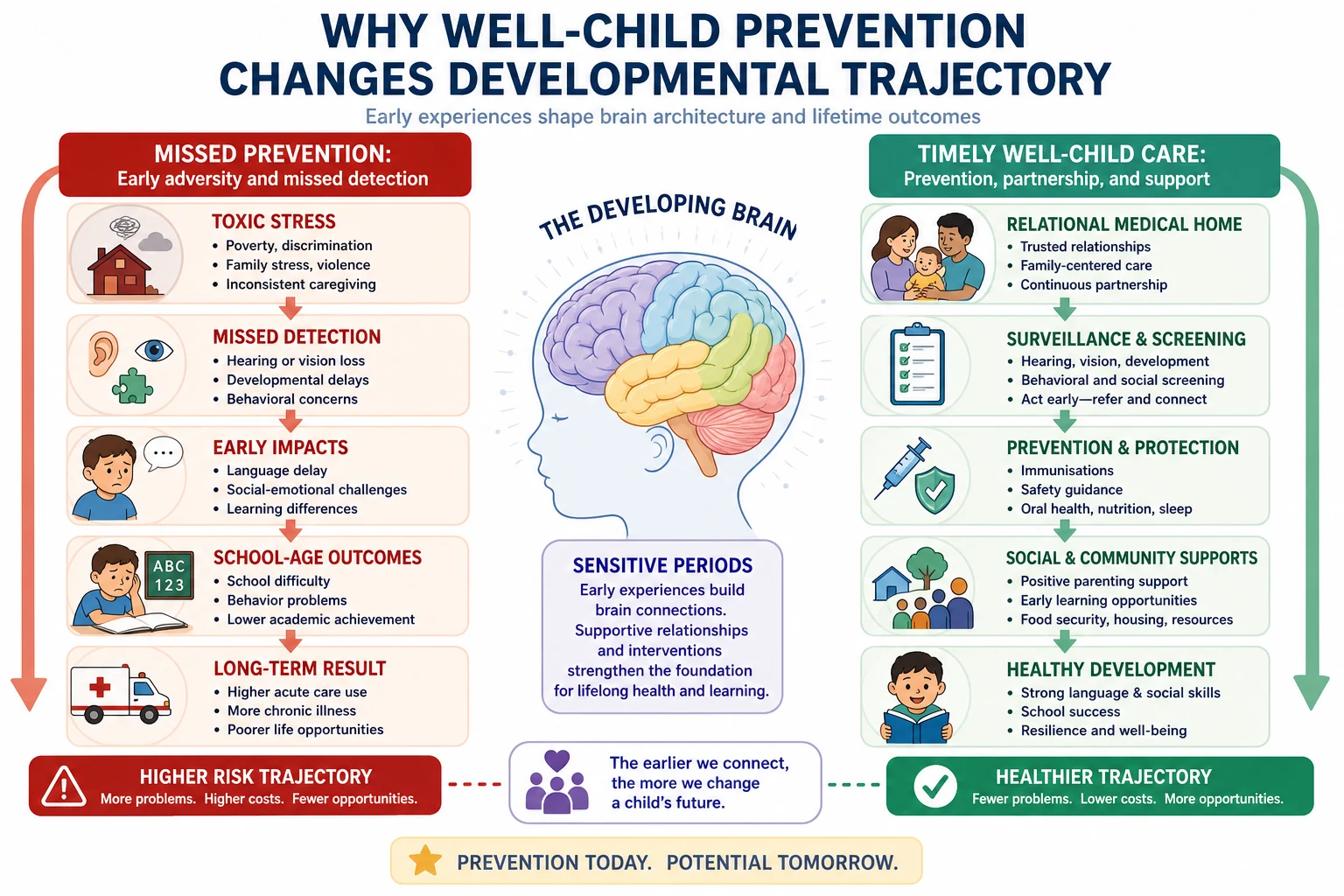
Read the figure like this: your job is not to promise a perfect life course. Your job is to remove remediable barriers early and strengthen buffers around the child. [11] [3]
Clinical Presentation
A good well-child visit looks calm but is cognitively busy. You hear what the family fears. You watch how the infant settles, how the toddler explores, how the adolescent makes eye contact when a parent leaves. You plot growth. You notice the car seat left in the corridor or the empty formula tin used as a toy. [1] [26]
Common “entry tickets”
- “Just immunisations.”
- “School form / childcare form.”
- “She is fine, but I worry about speech.”
- “He will not sleep.”
- “We moved / new foster placement / no records.”
Each ticket still needs the full preventive spine, adapted to time and risk. [9] [20]
Subtle presentations
Perinatal depression may present as an infant who is not gaining, a mother who does not smile at the baby, or repeated minor concerns. Food insecurity may present as stretching feeds, recurrent requests for formula samples, or obesity with poor diet quality. Developmental problems may present as “behaviour” or “stubbornness.” Adolescent depression or substance use may present only in confidential time. [5] [18] [23] [24]
When “well” is the wrong label
Feverish infants, children with work of breathing, unexplained bruising, severe faltering growth, or a child who is quiet because they are tired from respiratory failure are not well-child cases. Name the conversion early. [1]
Differential Diagnosis
In preventive care the differential is often what kind of problem is this system showing me? [1] [3]
| Finding | Prefer | Also consider | Do not assume |
|---|---|---|---|
| Parental speech concern | Hearing loss, language delay, autism spectrum pathways | Normal bilingual tempo with true concern still needs follow-up | “They will grow out of it” without a plan |
| Poor weight gain | Intake problem, illness, neglect, medical disease | Normal shifting centiles with thriving child | Single point equals failure to thrive |
| Behaviour change | Sleep debt, hearing, trauma, developmental disorder | Primary parenting conflict alone | Punishment advice as first line |
| Incomplete vaccines | Access barrier, record gap, hesitancy, true delay | Medical contraindication (rare) | Automatic refusal without exploring reason |
| Recurrent missed visits | Transport, poverty, distrust, chaos | Caregiver illness | “Non-compliance” as a moral label |
| The table is a reasoning aid, not a scored tool. [3] [12] [23] [28] |
Prioritise competing positives. A failed autism screen plus food insecurity plus overdue vaccines cannot all be “fully solved” in twelve minutes. You still must not ignore any of them. Make owners, times and interim safety plans. [8] [21]
Clinical & Bedside Assessment
Opening
Introduce yourself. Confirm decision-makers. Offer an interpreter before you need one. Ask: “What do you most want from today’s visit?” Then share your must-do items. Negotiation beats monologue. [7] [8]
Growth and physical examination
Measure weight, length/height and head circumference with correct technique for age. Plot on the appropriate chart. Look at trajectory, not a single elegant number. Examine with an age lens: hips and red reflex issues early; gait and skin findings in toddlers; spine, puberty staging and mental state in older children as indicated. This is not a fishing expedition for rare signs at the expense of listening. [1]
Developmental surveillance and screening
Surveillance is the skilled longitudinal process: elicit concerns, observe, review history and milestones, document domains. Do it every visit. Screening uses a standardised tool at key ages or when concern appears. Evaluation is the specialist diagnostic assessment after a failed screen or strong clinical worry. Lipkin’s AAP report is the modern anchor for this algorithm. Zubler’s evidence-informed milestones support surveillance tools; they are not a party-trick pass/fail list for viva theatre. [3] [4] [17]
If the caregiver is worried, do not let a “pass” screen end the story. Concern itself is data. Refer or recheck with a clear timeline. [3] [28]
Vision, hearing, oral health
Paediatricians assess the visual system over childhood; formal vision screening recommendations for young children are supported by USPSTF synthesis in the 6-month to 5-year band, with practical assessment guidance from AAP ophthalmology policy. Hearing concerns need early audiology pathways. Oral health includes caries risk, fluoride principles and a dental home, not only “brush your teeth” slogans. [6] [13] [15]
Psychosocial, mood and social determinants
Ask about housing, food, transport, safety and caregiver mood in plain language. Poverty-related screening is a clinical act when you have a response pathway. Screen for perinatal depression in the paediatric medical home and know your local urgent mental-health route. [5] [23] [24]
Adolescent confidentiality
Create time alone. Explain confidentiality and its safety limits before sensitive questions. Privacy failures block disclosure. [18]
Red flags that stop the checklist
Investigations
Think of investigations as questions with an action attached. [1]
Usually verify rather than re-order: newborn bloodspot completion, newborn hearing screen result, immunisation registry data, prior growth points, previous developmental screen scores. [1] [3]
Indicated screens (examples of principle, not a universal lab panel):
- Vision screening pathway for young children. [6] [15]
- Developmental/autism screening tools at key ages or on concern. [3]
- Risk-based lead testing according to local epidemiology and policy. [12]
- Haemoglobin/iron studies when risk factors or findings warrant, not as unthinking ritual. [1]
- Perinatal depression instrument in the paediatric setting with follow-up capacity. [5]
Often low value in an asymptomatic well child: random broad metabolic panels without indication, imaging “for reassurance,” or repeating a normal test because the letter is missing—first retrieve the result. [1] [21]
When a screen is positive, the investigation is incomplete until referral and follow-up are owned. A ticked box without a loop is theatre. [3] [10]
Management — Resuscitation
Preventive clinics still see emergencies. [1] [5]
- Threat to airway, breathing, circulation or consciousness: call for help, start ABCDE, activate emergency response, do not finish anticipatory guidance.
- Safeguarding emergency: ensure immediate safety, follow mandatory reporting law, involve senior/child-protection pathways, document facts.
- Severe caregiver mental-health crisis: do not discharge a suicidal parent with only a leaflet; use urgent mental-health and safety planning routes while protecting the child.
- Immunisation-room anaphylaxis readiness: vaccines are given where adrenaline and trained staff are available per local protocol (product-specific detail lives in immunisation topics).
- Hand-off if transferring to ED: problem list, allergies, guardianship, what was found today, pending results.
These steps protect life and safety before any preventive paperwork. [1] [5] [21]
Rural and telehealth preventive contacts need a pre-agreed escalation path when red flags appear on video. [8]
Management — Definitive & Stepwise
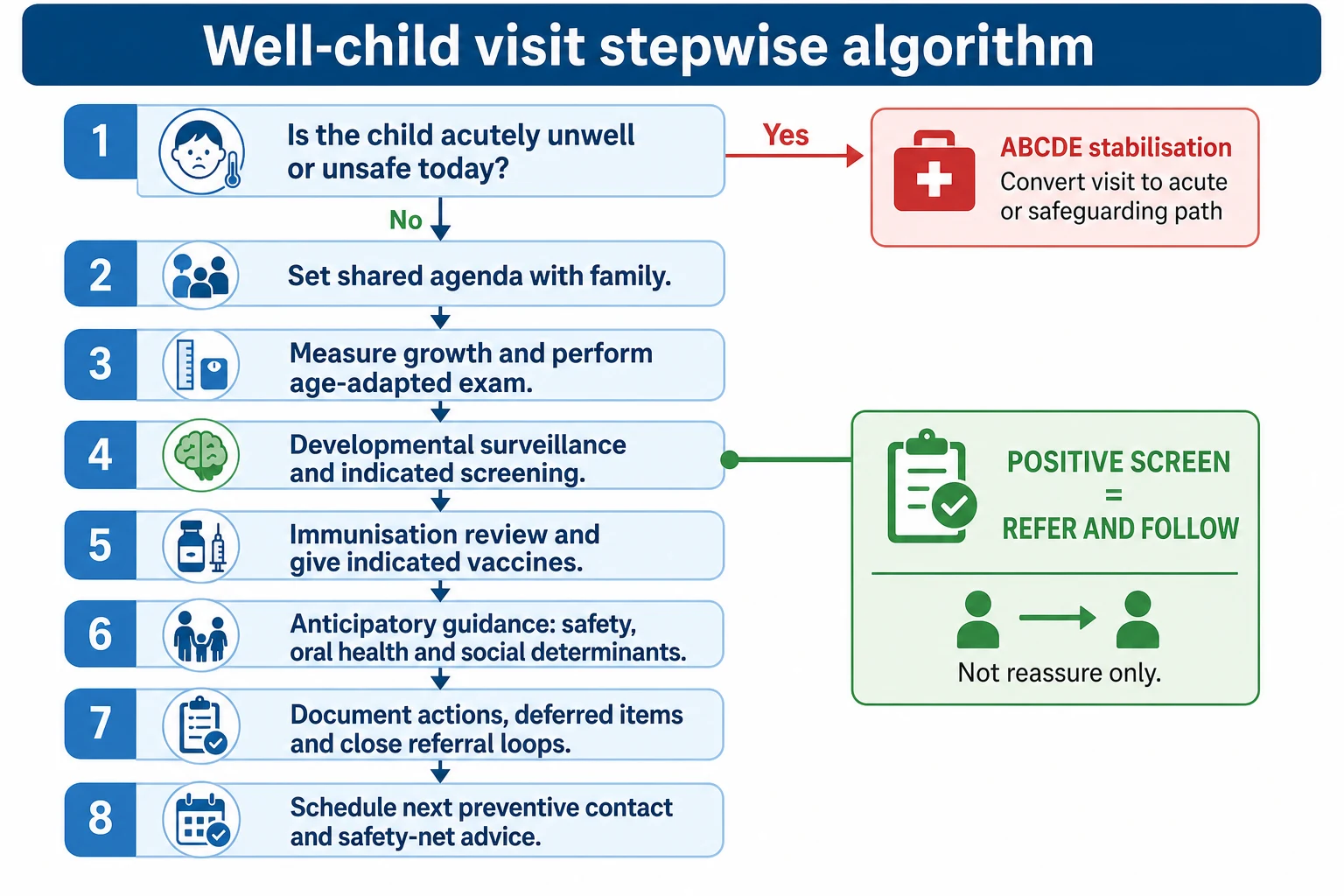
Stepwise visit algorithm
- Triage wellness and safety. Convert if needed.
- Co-create agenda. Family priorities plus clinician must-dos. [7]
- Growth and exam. Technique, trajectory, focused examination. [1]
- Development. Surveillance always; standardised screen when due or concerned. [3] [4]
- Indicated screening. Vision/hearing/oral/psychosocial/labs as appropriate. [6] [13] [24]
- Immunisation. Reconcile history; give due vaccines; counsel; arrange catch-up rather than vague “next time.” (Schedule detail is jurisdiction-specific.) [1]
- Anticipatory guidance. Match age risks and parent questions: sleep, feeding, play, discipline without harm, passenger safety, media, school. [7] [14] [26]
- Social and caregiver health. Food, housing, mood, interpersonal safety. Offer concrete help pathways. [5] [23]
- Plan and close loops. Write what was done, what was deferred, who owns referrals, when to return, and how to access acute care. [9] [21]
Practice redesign for equity
Coker’s redesign work for low-income children supports team-based models, pre-visit data collection, and non-physician contributions so physicians are not the only delivery channel for every Bright Futures item. If your clinic relies on heroics alone, content will fail when the waiting room is full. [8] [9]
Documentation standard
Document trajectory, concerns, screen results, vaccines, guidance actually given, social actions, and safety-net advice. Do not document a fantasy visit. [9]
Specific Subtypes & Scenarios
Newborn community visit
Confirm feeding, weight trend, jaundice concerns, maternal mood, safe sleep, and that newborn screens are complete or followed. Strengthen the medical home early. [1] [5] [16]
Dense infancy visits (including 9- and 24-month patterns)
These visits pack development, feeding transitions, safety and vaccines. Use structured tools and team support or you will drop content. [9]
Developmental concern without “failed” tool
Believe the parent enough to make a plan. Recheck early or refer. Early emotional and behavioural problems also need pathways, not minimisation. [3] [25] [28]
School-age preventive visit
Growth, vision/hearing as indicated, learning and attention concerns, dental home, activity, injury prevention, and school functioning. [1] [15]
Adolescent visit
Confidential time, psychosocial risk assessment, sexual and mental health, vaccine catch-up, and transition planning as adulthood approaches. Age-limit and transition policies remind teams that adolescence is still paediatrics until a planned handover. [18] [19] [27]
Foster/kinship care
Assume incomplete data. Rebuild history, examine fully, catch up prevention, and identify a durable medical home. [20]
Medical complexity
Preventive tasks still matter: vaccines, nutrition, vision, dental, development, caregiver burnout, emergency plans. Care coordination is part of the well visit, not an optional extra. [21] [22]
Vaccine or screen hesitancy
Stay curious, correct specific misinformation, keep the relationship, and document informed refusal without humiliating the family. Detailed hesitancy communication is covered in its sibling topic; here the rule is: do not trade away all other preventive care because one discussion ran long. [1]
Complications & Pitfalls
Other high-yield traps (each is an examiner favourite): [3] [7]
- Treating screen pass as lifelong clearance.
- Treating screen fail as a final diagnosis.
- No confidential adolescent time.
- Ordering labs instead of addressing food or housing.
- Referral without follow-up ownership.
- Ignoring incomplete records in out-of-home care.
- Cultural stereotyping of risk.
- Inventing local schedule ages from memory in a viva—state principle and official source.
Each trap is common in clinics and exams. [1] [3] [18] [23]
Prognosis & Disposition
Earlier access to developmental services improves the chance of meaningful support during higher plasticity windows. That is why surveillance and referral speed matter more than elegant labels. [3] [17]
Disposition options after a well visit: [1] [3]
- Home with timed next preventive contact and clear acute-care access.
- Same-day acute workup if the child is not well.
- Fast-track referral with interim safety advice when screens fail.
- Social-work or mental-health urgent pathway when household safety is at risk.
Choose disposition by acuity and open loops, not by the original booking label. [5] [21]
Incomplete visits are allowed if honest: document what was deferred and why, then book the return. Silent omission is the danger. [9]
Longitudinal medical-home care is associated with better coordination experiences and supports earlier identification pathways; it is not a magic shield against all disease. [10] [16] [22]
Special Populations
Preterm / NICU graduates: intensified developmental and growth surveillance; do not use term-only expectations blindly. [3]
Disability and neurodiversity: adapt examination, communication and screening; avoid diagnostic overshadowing of treatable problems. [21]
Indigenous families: culturally safe care, community strengths, and honest access barrier repair. [23]
Refugee and migrant families: language access, uncertain vaccine history principles, interrupted screening, trauma-aware history. [23]
Out-of-home care: rapid comprehensive catch-up. [20]
Gender and sexually diverse youth: confidential, affirming preventive care. [18]
Poverty and housing instability: screen and respond; redesign visit flow. [8] [23] [24]
Complex chronic / technology-dependent children: integrate emergency plans and coordination into health supervision. [21] [22]
Evidence, Guidelines & Regional Differences
[1] [2]Key evidence anchors for exams: [1]
- Periodicity recommendations as living US preventive maps. [1] [2]
- Developmental surveillance/screening algorithm. [3] [17]
- Evidence-informed milestones for tools. [4]
- Perinatal depression in paediatric practice. [5]
- Vision screening synthesis. [6]
- Anticipatory guidance needs mismatch. [7]
- Redesign for low-income well-child care. [8]
- Improving content delivery at dense visits. [9]
- Toxic stress conceptual framework. [11]
- Lead, fluoride, passenger safety, medical home and poverty policies. [12] [13] [14] [16] [23]
Controversies to handle honestly: universal versus selective labs; how much content fits in a short visit; team-based delivery versus physician-only ideals; limits of evidence for some screening targets. When evidence is weak, say so and avoid inventing certainty. [1] [8]
Exam Pearls
WELL CHILD visit spine
How boards test this hub
Written papers test definitions (surveillance vs screening), prioritisation, and red-flag conversion. Long cases test a real health-supervision narrative with social complexity. Short cases/OSCE test growth technique talk-through, developmental enquiry, and counselling. Structured orals push Bright Futures principles versus local schedules and equity redesign. [1] [3] [8]
One-page recovery
If you remember nothing else: make sure the child is well, hear the family, measure growth, watch development, do the indicated screens, reconcile vaccines, give guidance that matches real life, and close every loop you open. [1] [3] [21]
References
- [1]Committee on Practice and Ambulatory Medicine 2023 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2023.PMID 36938620
- [2]Committee on Practice and Ambulatory Medicine 2021 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2021.PMID 33593848
- [3]Lipkin, Paul H Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [4]Zubler, Jennifer M Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [5]Earls, Marian F Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics, 2019.PMID 30559120
- [6]US Preventive Services Task Force Vision Screening in Children Aged 6 Months to 5 Years: US Preventive Services Task Force Recommendation Statement. JAMA, 2017.PMID 28873168
- [7]Schuster, Mark A Anticipatory guidance: what information do parents receive? What information do they want? Archives of pediatrics & adolescent medicine, 2000.PMID 11115301
- [8]Coker, Tumaini R Well-child care clinical practice redesign for serving low-income children. Pediatrics, 2014.PMID 24936004
- [9]Duncan, Paula M Improving delivery of Bright Futures preventive services at the 9- and 24-month well child visit. Pediatrics, 2015.PMID 25548322
- [10]Barger, Brian Medical Home, Developmental Monitoring/Screening, and Early Autism Identification. Journal of autism and developmental disorders, 2024.PMID 37477840
- [11]Garner, Andrew S Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [12]Council on Environmental Health Prevention of Childhood Lead Toxicity. Pediatrics, 2020.PMID 32471839
- [13]Clark, Melinda B Fluoride Use in Caries Prevention in the Primary Care Setting. Pediatrics, 2020.PMID 33257404
- [14]Durbin, Dennis R Child Passenger Safety. Pediatrics, 2018.PMID 30166368
- [15]Donahue, Sean P Visual System Assessment in Infants, Children, and Young Adults by Pediatricians. Pediatrics, 2016.PMID 29756730
- [16]Medical Home Initiatives for Children With Special Needs Project Advisory Committee The medical home. Pediatrics, 2002.PMID 12093969
- [17]Council on Children With Disabilities Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics, 2006.PMID 16818591
- [18]Agostino, Holly Considerations for privacy and confidentiality in adolescent health care service delivery. Paediatrics & child health, 2023.PMID 37205141
- [19]White, Patience H Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [20]Szilagyi, Moira A Health Care Issues for Children and Adolescents in Foster Care and Kinship Care. Pediatrics, 2015.PMID 26416941
- [21]Turchi, Renee M Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [22]Homer, Charles J A review of the evidence for the medical home for children with special health care needs. Pediatrics, 2008.PMID 18829788
- [23]Council on Community Pediatrics Poverty and Child Health in the United States. Pediatrics, 2016.PMID 26962238
- [24]Berman, Rebecca S Screening for Poverty and Poverty-Related Social Determinants of Health. Pediatrics in review, 2018.PMID 29716966
- [25]Gleason, Mary Margaret Addressing Early Childhood Emotional and Behavioral Problems. Pediatrics, 2016.PMID 27940734
- [26]Milteer, Regina M The importance of play in promoting healthy child development and maintaining strong parent-child bond: focus on children in poverty. Pediatrics, 2012.PMID 22201149
- [27]Hardin, Amy Peykoff Age Limit of Pediatrics. Pediatrics, 2017.PMID 28827380
- [28]Glascoe, Frances Page Parenting behaviors, perceptions, and psychosocial risk: impacts on young children's development. Pediatrics, 2010.PMID 20100743