Paeds · professional-practice-and-evidence
Breaking bad news and serious-illness communication
Also known as Breaking bad news in paediatrics · Serious-illness conversation · SPIKES protocol for children · Goals-of-care and advance care planning communication · Prognostic disclosure to children and families
Fellowship guide to breaking bad news and serious-illness communication in paediatrics: SPIKES, Ask-Tell-Ask and NURSE; goals-of-care and advance care planning; prognostic disclosure adapted to the child's development; managing hope, conflict and end-of-life transitions; clinician debrief; and ANZ/UK/US/Canada system and cultural differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
S.P.I.K.E.S. — six steps for delivering bad news
Overview & Definition
A six-year-old is admitted overnight with pallor and bruising. The morning blood film shows blasts. By midday both parents are in a side room with you. What you say next — and how you say it — will be remembered by this family for the rest of their lives. That is breaking bad news. [1] [3]
Breaking bad news means conveying information that adversely and materially alters a person's expectations about their present or future. In paediatrics the patient is a child embedded in a family, so the conversation is almost always held with parents and, developmentally, with the child or young person. The dominant teaching structure is the SPIKES six-step protocol, first described for adults with cancer and now adapted across paediatrics. [1]
Serious-illness communication is the larger, longitudinal craft this page also owns: values and goals, prognostic uncertainty, advance care planning, and the shift from cure-directed to comfort-focused care. Tools such as the Serious Illness Conversation Guide (and its paediatric adaptation) structure these talks. Breaking bad news is one event inside that longer conversation. [12] [13]
This page owns the process and skills. Cross-link dedicated leaves for consent and mature-minor frameworks, shared decision-making, communicating risk and uncertainty, open disclosure, conflict, trauma-informed care and working with interpreters — do not rebuild their content here. [3]
Classification
Sort the work by the type of conversation and the framework you reach for. [1] [12]
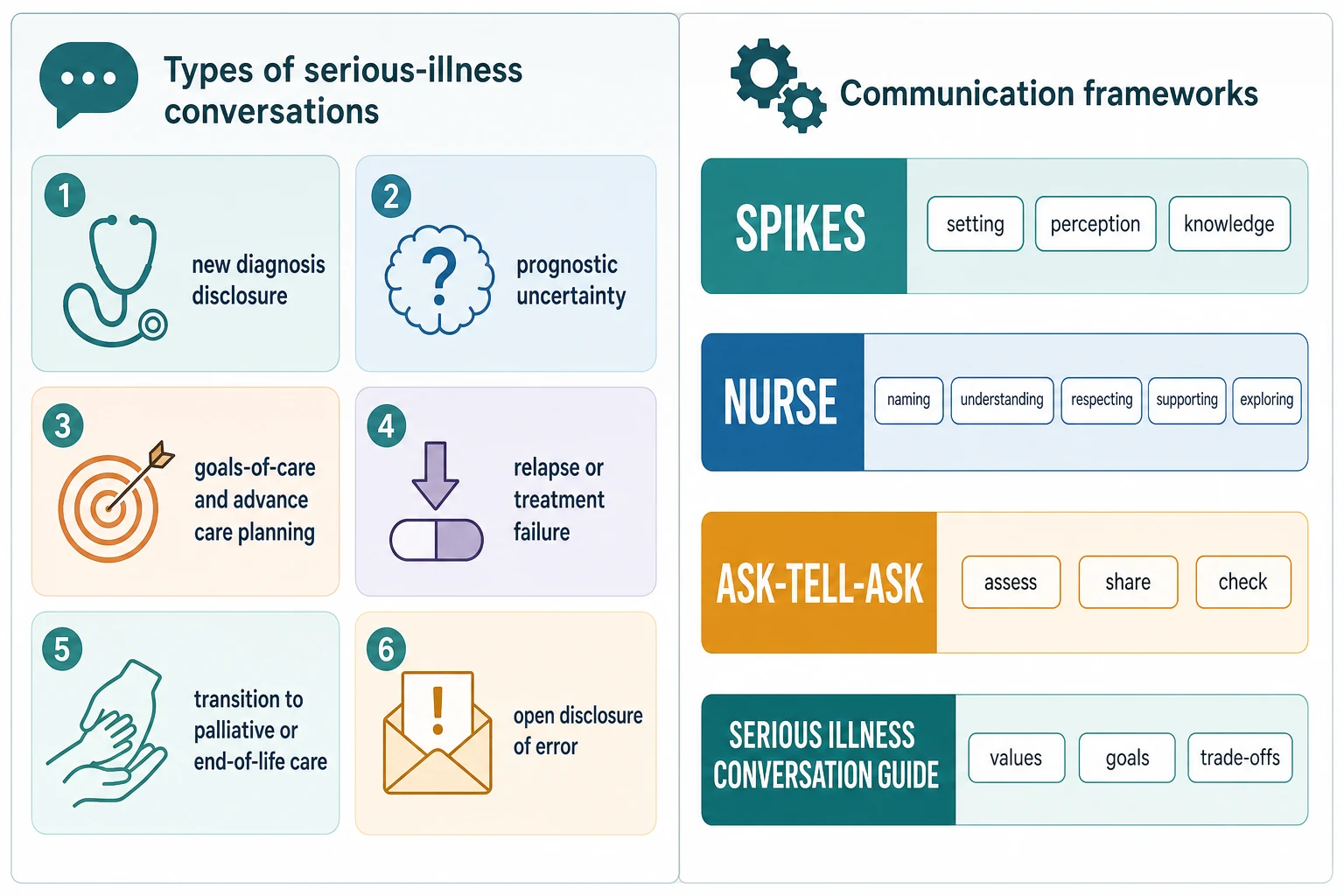
Types of serious-illness conversation. New diagnosis disclosure. Relapse or treatment failure. Prognostic uncertainty and answering "how long?". Goals-of-care and advance care planning. Transition from disease-directed to palliative or end-of-life care. Open disclosure of error or unexpected harm. Each has a different emotional weight, but the same core skills apply. [12] [13]
Frameworks. SPIKES for delivering the news itself. Ask-Tell-Ask for assessing and checking as you go. NURSE for responding to emotion. The Serious Illness Conversation Guide for values, goals and trade-offs. These are not rival religions; they compose into a single encounter. [1] [15]
Who is the conversation for? Parents only, parents plus young child, or the adolescent as a primary participant. Developmental stage, not chronological age alone, decides the child's role. [3] [10]
Epidemiology & Risk Factors
Serious-illness conversations happen across paediatric oncology, chronic illness, PICU, neonatology and neurodisability — not only in cancer. Far more children now live with life-limiting chronic conditions than die from acute illness, so these talks are recurrent, not once-in-a-career events. [6] [14]
The burden these conversations address is real. Wolfe's landmark study of children dying of cancer found many suffered from fatigue, pain, dyspnoea and other symptoms that were often undertreated, and that suffering was associated with where care was delivered and how goals were set. [4] That data underpins why early palliative integration and honest communication matter. [6]
Communication quality is uneven. Race and ethnicity influence prognostic communication: parents from some minority groups are less likely to receive clear prognostic information about their child's cancer, a disparity that shapes later decision-making and trust. [9]
Clinician factors are part of the epidemiology too. Many paediatric trainees feel underprepared for these conversations, and prognostic avoidance is common. Targeted communication training has measurable effects. [2] [7]
Pathophysiology
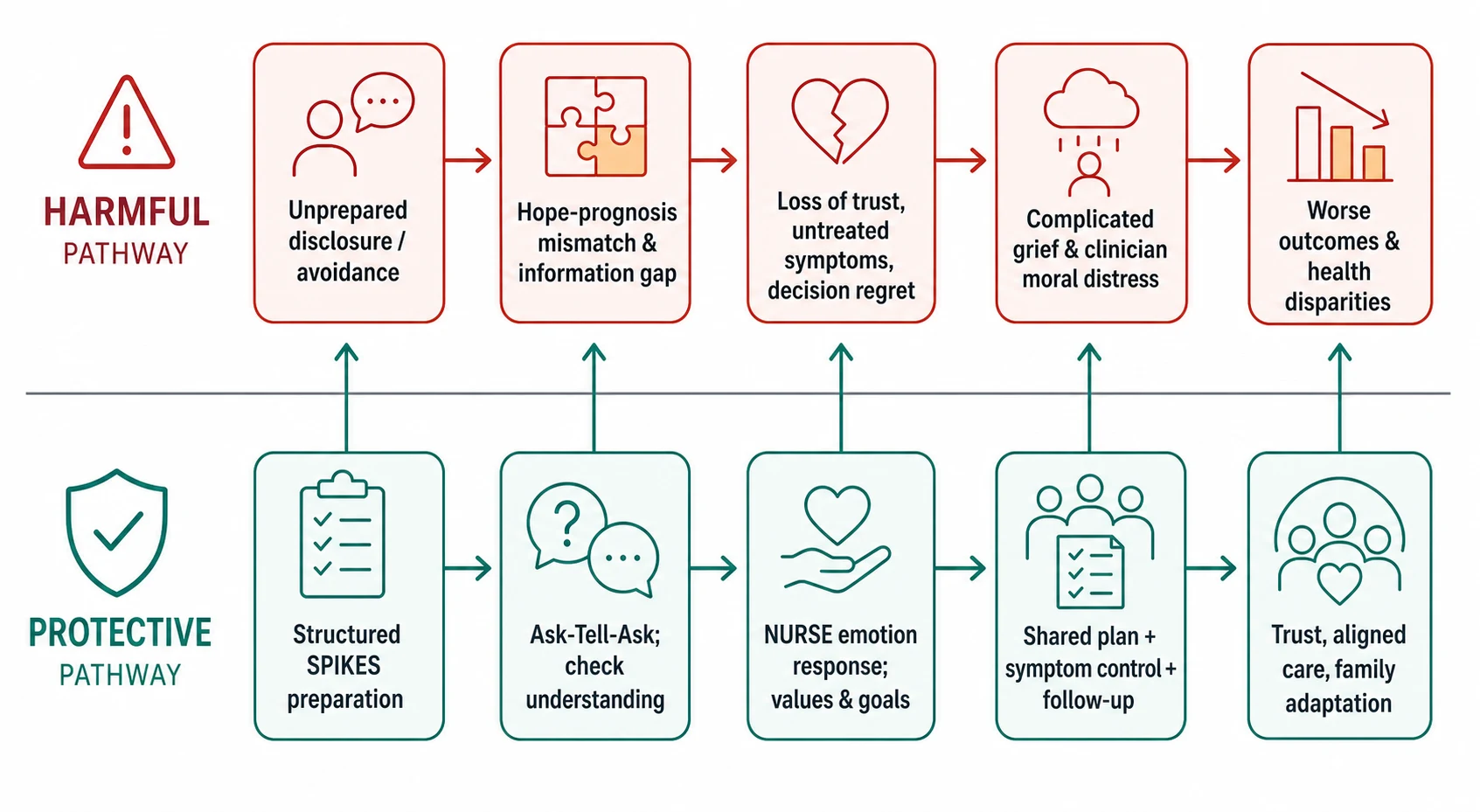
Think about the mechanisms that turn a piece of information into either harm or trust. [1] [5]
Shock and cognitive overload. Hearing serious news temporarily narrows a person's capacity to process new information. Information dumped into an unprepared mind is not retained, which is why a warning shot and small chunks matter more than completeness. [1]
Hope and prognostic mismatch. Parents hold hope powerfully, and that hope can be realistic, sustaining, or falsely optimistic. When clinicians collude with false hope — by avoiding prognosis or over-stating benefit — disease-directed treatment can continue against the family's deeper goals, and symptoms and suffering go unaddressed. [8] [11]
The family as the unit of care. A child's serious illness reshapes the whole family. Parental coping, sibling confusion, grandparents' grief and cultural expectations all meet in the room. Communication aimed only at one parent misses the system that will carry the child home. [5] [14]
Clinician emotion as a barrier. Fear of causing harm, distress at a poor outcome, and prognostic avoidance all push clinicians toward vagueness or delay. Unrecognised, these produce moral distress and burnout — which in turn degrade the next conversation. [7] [13]
Clinical Presentation
You will meet serious-illness communication in several recognisable shapes. [3] [12]
The new diagnosis. Results confirm a life-threatening or life-altering illness — leukaemia, a metabolic disorder, a severe congenital anomaly, a degenerative condition. The family needs the diagnosis, the immediate plan, and honest uncertainty about what comes next. [1]
Relapse or treatment failure. Scans or counts show progression despite treatment. The emotional ground shifts from hope-in-treatment toward re-evaluation of goals. [8]
The direct prognostic question. A parent — or an adolescent — asks plainly: "Is she going to die?" or "How long does he have?". This is the hardest and most important moment to answer honestly and with care. [9] [11]
Approaching end of life. The focus moves from cure to comfort. Introducing palliative goals, limitation of treatment, and where the child will be cared for is a distinct, sensitive conversation. [4] [6]
Error or unexpected harm. Something went wrong. Open disclosure — honestly explaining what happened, the consequences, and the response — is its own skill, owned on the dedicated leaf but sharing SPIKES foundations. [2]
Differential Diagnosis
Name the true problem before you reach for more words. [8] [11]
| You see | Prefer this framing | Trap |
|---|---|---|
| Family seems "in denial" about prognosis | Information gap, protective buffering, or grief | Label them difficult and stop engaging |
| Parent insists on continuing treatment | Goals-prognosis mismatch; explore values first | Assume demands are unreasonable |
| Child withdrawn and silent | Developmental processing, fear, depression | Exclude the child from all conversations |
| Adolescent asks to stop treatment | Emerging autonomy, values, symptom burden | Override assent without exploration |
| Family angry at the team | Trust breakdown, prior poor communication | Escalate to conflict without repair |
Realistic hope versus false hope. Both are present in most serious illness. Your job is not to destroy hope but to move it toward what is achievable — comfort, presence, meaning — while being honest about what is not. [11]
Clinical & Bedside Assessment
Assess before you share. What does the family already know? What do they think is happening? How much do they want to hear today? These perception and invitation questions are the spine of SPIKES and stop you from over- or under-sharing. [1]
Read the child developmentally. A preschooler thinks magically and blames themselves; a school-age child wants concrete, truthful detail and will fill gaps with worse fears if you do not; an adolescent wants honesty, privacy, and a say. Match language to stage, and invite the child in rather than defaulting to exclusion. [3] [10]
Read emotion in real time. Tears, anger, dissociation, sudden questions, silence — each is information. Respond with NURSE statements (naming, understanding, respecting, supporting, exploring) and tolerate silence rather than filling it. [1] [2]
Map the family and context before the meeting. Who should be present? Is an interpreter needed? Are there cultural or spiritual practices that shape how news is received and by whom? Are siblings or grandparents to be considered? [5] [14]
Check understanding with teach-back. Ask the family to say back what they heard, in their own words. Invite questions. Do not assume comprehension from a nod. [3]
Investigations
The "investigations" here are preparations, not blood tests. [1] [3]
Know the facts cold. Confirm the diagnosis, the prognosis and the immediate plan before the meeting. Vague hedging because you are unsure of the result erodes trust instantly. If a result is genuinely uncertain, say so honestly. [1]
Gather collateral. What have other clinicians already said? What records has the family seen? What conversations happened on the ward overnight? Avoid contradicting a colleague in front of the family; align the team first. [14]
Use structured conversation guides as assessment tools. The Serious Illness Conversation Guide elicits values, goals and what the family would and would not want to endure — information you cannot get from a scan. [12] [13]
Document the conversation. Who was present, what was disclosed, the family's understanding, the agreed plan, and the next contact. This is both a clinical and a medicolegal product. [3]
Management — Resuscitation
Some moments in these conversations are emergencies of a different kind. [2] [7]
Acute psychological collapse. A parent may dissociate, become acutely agitated, or disclose suicidal thoughts during or after the conversation. Pause the information, stay, offer support, and escalate to mental-health or social-work colleagues. Do not abandon the family to finish your list. [11]
Safeguarding surfaced. A family meeting can reveal domestic violence, neglect or coercion. Follow your mandatory safeguarding pathway exactly as you would anywhere else. [3]
Medical deterioration during the meeting. If the child becomes acutely unstable, stabilise first. Return to the conversation later; families cannot absorb news beside a resuscitation. [14]
Clinician acute distress. A registrar may be shaken after delivering terrible news alone. Offer immediate peer support, relieve them of further difficult tasks that day, and ensure a debrief. [7] [13]
Management — Definitive & Stepwise
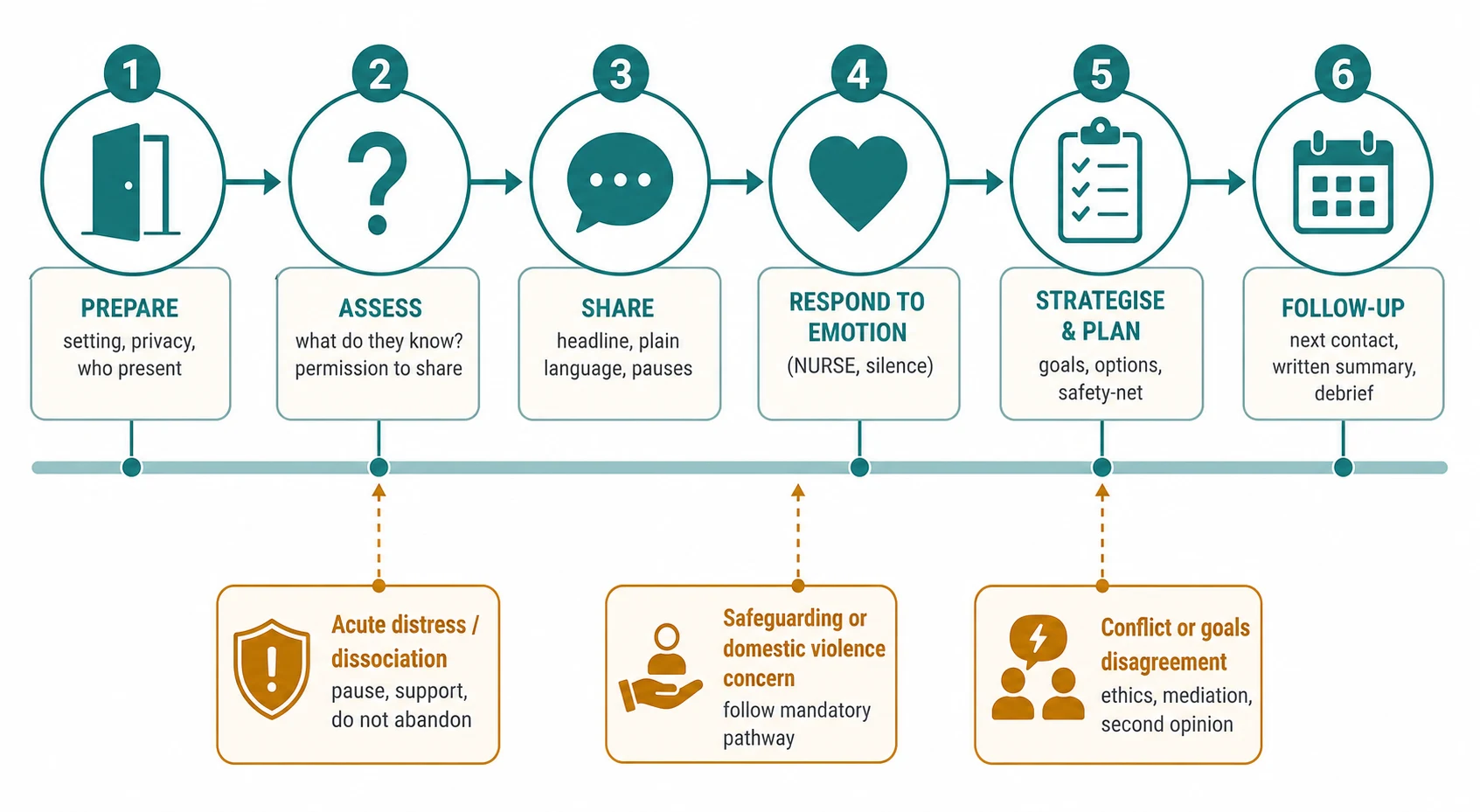
Use SPIKES as the backbone, layered with NURSE and Ask-Tell-Ask. [1] [2]
- Setting. Private room, enough time, the right people, phones away, tissues and water, a trained interpreter if needed. Sit at the family's eye level. [1]
- Perception. Ask what they understand so far: "Tell me what you think is happening with [child]." This reveals their starting point and their language. [1]
- Invitation. Ask how much they want to hear now: "Are you the sort of family who wants all the detail, or the headlines first?" Respect the answer. [1]
- Knowledge. Give a warning shot ("I'm afraid I have difficult news"), then a clear headline in plain language. Pause. Give small chunks. Avoid jargon. Check in. [1]
- Empathy. Respond to emotion with NURSE: name it ("This is overwhelming"), show understanding ("I can see how frightening this is"), respect it ("Your questions show how much you love her"), support ("We will face this with you"), and explore ("Tell me more about what worries you most"). Tolerate silence. [1] [2]
- Strategy and summary. Align with values and goals, agree concrete next steps, offer a written summary, and set the next contact. Do not end on information alone. [1] [3]
What training achieves. Randomised evidence shows that structured communication skills training improves clinicians' ability to give bad news and discuss transitions to palliative care. Critical-care communication curricula show similar gains. These skills are learnable and decay without practice. [2] [7]
What the evidence supports overall. A Cochrane review found that interventions to improve end-of-life interpersonal communication can change clinician behaviour, though effects on patient and family outcomes are more uncertain — train the skill, and measure it. [15]
Specific Subtypes & Scenarios
New cancer diagnosis in a young child. Talk with parents first and at length. Then speak with the child in concrete, truthful terms — what their body is doing, what treatment will feel like — correcting magical thinking and inviting questions. Parents and child usually do best hearing consistent messages from a coordinated team. [1] [3]
Adolescent with relapsed disease. Offer confidential time, respect emerging autonomy and assent, and discuss prognosis and goals directly when the young person wants them. Prognostic disclosures to children and adolescents have shifted historically toward greater honesty; default to inclusion, calibrated to the individual. [9] [10]
Non-cancer life-altering diagnosis. A neurodisability or metabolic diagnosis may not shorten life but reshapes it. Families grieve the future they expected. Pace the information, link to supports early, and avoid overloading a single visit. [3] [6]
Neonate in NICU. Antenatal or postnatal news lands on exhausted, often postpartum parents. Short, repeatable conversations beat one long meeting. Use lactation, social work and peer supports. [14]
PICU goals-of-care meeting. After prolonged critical illness, lead a structured discussion of what recovery would look like, what the family values, and whether continued disease-directed treatment serves those goals. Family-centred-care guidelines frame the meeting. [7] [14]
Transition to palliative care. Reframe, do not abandon: "We are changing our goal from cure to your child's comfort and your time together." Early palliative integration alongside disease-directed therapy is increasingly the standard, not an either/or. [6] [13]
Complications & Pitfalls
- Information dumping without assessing perception or invitation. [1]
- Colluding with false hope so treatment continues against the family's real goals. [8] [11]
- Excluding the child or adolescent from conversations about their own illness. [10]
- No interpreter for a family with limited English proficiency. [3]
- Giving information without teach-back, a written summary, or follow-up. [3]
- Vagueness about prognosis to the family's detriment; prognostic disparities by race. [9]
- Continuing disease-directed treatment because prognosis was never discussed. [6] [8]
- No team debrief; clinician moral distress and burnout unaddressed. [7] [13]
Prognosis & Disposition
A good conversation is not measured by how smoothly it ran but by what it leaves behind. [5] [15]
Markers of success. The family can describe what they were told. Trust between family and team is intact or strengthened. Symptoms are being addressed. Goals are aligned with prognosis. A follow-up contact is named. The team has debriefed. [3] [14]
When to defer. If the family is acutely distressed, the medical facts are not yet clear, or a key person is missing, it is legitimate to share the headline, support, and return for the full conversation later. Deferral is a deliberate choice, not avoidance. [1]
When to escalate. Persistent goals conflict, a request the team cannot meet, or a breakdown of trust warrants ethics consultation, mediation or a second opinion. Use these early rather than as a last resort. [2] [13]
Sustain the clinician. Build debrief and peer support into the routine. The ability to hold these conversations across a career depends on it. [7] [13]
Special Populations
Non-speaking and cognitively diverse children. Communicate to function and relationship, not age alone. Use the child's usual communication system and the people who know them best; assume the child understands more than they can express. [3] [10]
Adolescents. Offer confidential time, respect privacy and assent, and address prognosis and goals directly when wanted. Avoid the dual failure of either excluding them or burdening them with decisions beyond their role. [9] [10]
Culturally and linguistically diverse families. Always use a trained interpreter — never a family member or child — and consider a cultural broker. Ask how the family wishes news to be shared and with whom. [3] [14]
Indigenous families. Culturally safe, family- and community-centred communication is central. Follow locally endorsed pathways and trusted workers; do not impose a generic model. [5]
Bereaved or previously bereaved families. Use grief-aware language, acknowledge prior loss, and offer additional support. A new serious conversation lands differently on a family that has already buried a child. [5] [11]
Evidence, Guidelines & Regional Differences
Core anchors are the Baile SPIKES protocol, the Back randomised trial of communication skills training, the Levetown AAP clinical report on communicating with children and families, Wolfe's NEJM data on symptoms and suffering, prognostic-communication evidence from Kaye, Sisk and Ilowite, the Serious Illness Conversation case-review and programme literature, the Davidson family-centred-care guidelines, and the Ryan Cochrane review of interpersonal end-of-life communication. [1] [2] [3] [4] [8] [9] [10] [12] [14] [15]
Paediatric palliative care networks (for example, state-based services and Quacknix/Hummingbird House-style hospices in Australia, and Te Tai Tokerau/Skylight-aligned services in Aotearoa) support these conversations. RACP and RCPCH-aligned communication curricula frame training. Use local advance-care-planning documents (for example, My Health Record and ACCT/PeDiE-style plans) and culturally safe pathways for Aboriginal and Torres Strait Islander and Māori whānau. Do not invent local statutory wording. [6] [14]
NICE and RCPCH guidance emphasises honest, developmentally appropriate communication and advance care planning (for example, the CYPACP framework). RCPCH Progress+ names communication as a core professional skill. Local palliative care networks (for example, Martin House, Helen and Douglas House-style children's hospices) provide support. [3] [6]
Ariadne Labs's Serious Illness Conversation Guide (and its paediatric adaptation) and AAP clinical reports shape practice. Trainees increasingly learn via Oncotalk- and C3-style structured curricula. Family-centred-care guidelines apply across the ICU. [1] [7] [12] [14]
CanMEDS roles (Communicator, Collaborator, Professional, Health Advocate) map directly onto leading difficult conversations. Provincial advance-care-planning frameworks and paediatric palliative services vary; use local documents and interpreters. [6] [14]
Controversies: full versus incremental disclosure; whether and how much to tell children about prognosis directly; how to preserve hope without false hope; and how to weigh family request for non-disclosure against the child's right to know. Exam answers show structured skill, honest uncertainty, and local humility. [1] [10] [13]
Exam Pearls
- Prepare the setting before you prepare the words. [1]
- SPIKES = Setting, Perception, Invitation, Knowledge, Empathy, Strategy. [1]
- NURSE = Naming, Understanding, Respecting, Supporting, Exploring. [1] [2]
- Ask-Tell-Ask: assess, share, check. [3]
- Tolerate silence; respond to emotion before more information. [2]
- Include the child developmentally; do not exclude by default. [3] [10]
- Move hope toward what is achievable; avoid colluding with false hope. [8] [11]
- Check understanding with teach-back; leave a written summary and follow-up. [3]
- Communication training works; these skills are learnable and need practice. [2] [7]
- Debrief the team; communication is a team sport, not a solo performance. [13]
SPIKES at the bedside
Prepare: private space, right people, interpreter, time
Ask perception: what do they already know?
Ask invitation: how much do they want now?
Give a warning shot, then the headline in plain language
Respond to emotion with NURSE; tolerate silence
Agree the plan; written summary; next contact
References
- [1]Baile WF SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. The oncologist, 2000.PMID 10964998
- [2]Back AL Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Archives of internal medicine, 2007.PMID 17353492
- [3]Levetown M Communicating with children and families: from everyday interactions to skill in conveying distressing information. Pediatrics, 2008.PMID 18450887
- [4]Wolfe J Symptoms and suffering at the end of life in children with cancer. The New England journal of medicine, 2000.PMID 10655532
- [5]Contro NA Hospital staff and family perspectives regarding quality of pediatric palliative care. Pediatrics, 2004.PMID 15520103
- [6]Mack JW Early integration of pediatric palliative care: for some children, palliative care starts at diagnosis. Current opinion in pediatrics, 2006.PMID 16470155
- [7]Arnold RM The Critical Care Communication project: improving fellows' communication skills. Journal of critical care, 2015.PMID 25535029
- [8]Kaye EC Prognostic Communication Between Oncologists and Parents of Children With Advanced Cancer. Pediatrics, 2021.PMID 33952691
- [9]Ilowite MF Disparities in prognosis communication among parents of children with cancer: The impact of race and ethnicity. Cancer, 2017.PMID 28873224
- [10]Sisk BA Prognostic Disclosures to Children: A Historical Perspective. Pediatrics, 2016.PMID 27561728
- [11]Kamihara J Parental hope for children with advanced cancer. Pediatrics, 2015.PMID 25847801
- [12]van Breemen C Serious Illness Conversations in Pediatrics: A Case Review. Children (Basel, Switzerland), 2020.PMID 32824811
- [13]Doherty M The Pediatric Serious Illness Conversation Program: Understanding challenges and experiences for clinicians after advance care planning training. Palliative & supportive care, 2024.PMID 37288722
- [14]Davidson JE Guidelines for Family-Centered Care in the Neonatal, Pediatric, and Adult ICU. Critical care medicine, 2017.PMID 27984278
- [15]Ryan RE Interventions for interpersonal communication about end of life care between health practitioners and affected people. The Cochrane database of systematic reviews, 2022.PMID 35802350