Paeds · professional-practice-and-evidence
Consent, parental responsibility and mature-minor frameworks
Also known as Informed consent in paediatrics · Parental permission and assent · Mature minor doctrine · Gillick competence and Fraser guidelines · Decision-making capacity in children · Adolescent consent and refusal · Emergency treatment of children without consent
Fellowship-level approach to consent in paediatrics: parental responsibility, child assent and dissent, decision-making capacity via Appelbaum domains, Gillick/Fraser and mature-minor frameworks, emergency necessity, refusal of life-saving care, and defensible documentation across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old needing a lumbar puncture. The mother agrees, the child is terrified, and the father is on the phone refusing. Your job is not to pick the loudest voice. It is to work out who holds authority for this decision and how the child's voice fits in. [1]
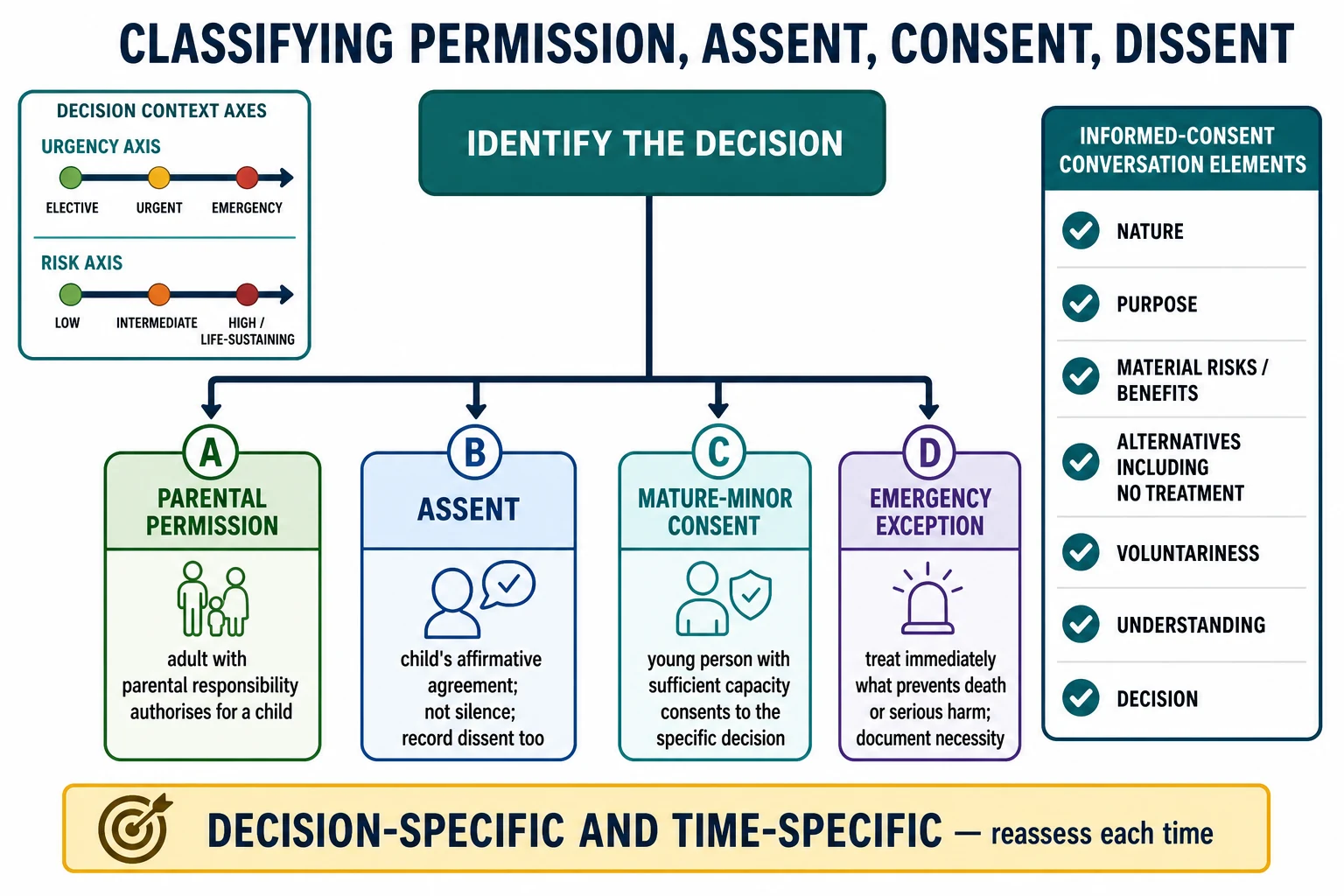
Four terms do most of the work. Informed consent is a voluntary, understanding agreement to a specific intervention after disclosure of its nature, purpose, material risks and benefits, alternatives including no treatment, and the option to decline. Parental permission is the equivalent authority given by someone holding parental responsibility for a child who cannot yet consent for themselves. Assent is the child's affirmative agreement to participate; mere silence or failure to resist is never assent. Dissent is the child's expressed objection, which deserves weight even when the child lacks legal authority to decide. [1] [2]
Two legal concepts sit underneath all of this. Decision-making capacity is a functional, clinical judgement about whether this person can make this decision now; it is distinct from legal competence, which is what the law assigns by status or age. Parental responsibility is the bundle of rights and duties that lets an adult authorise treatment for a child — and it does not automatically belong to whoever brought the child in today. [1] [3]
[1] [3]Classification
Start from the bedside, not from a statute book. The pathway you follow depends on the urgency of the decision, its risk, and whether the child can understand it. [1]
Parental permission is the default for infants and young children. An adult with parental responsibility authorises the intervention, and you layer in developmentally appropriate assent. For most neonates and infants there is no meaningful assent to obtain, so parental permission carries the decision. [1]
Parental permission plus assent is the model for school-age children. The parent remains the legal decision-maker, but the child's affirmative agreement is sought and their dissent is documented and weighed. Assent is not a tick-box; it changes how you prepare, pace and explain. [2] [12]
Mature-minor consent applies when a young person has sufficient understanding of the specific decision to consent for themselves. This is a functional assessment, not an automatic birthday. The same young person may be capable for a low-risk decision and not for an irreversible one. [3] [4]
Emergency exception lets you treat immediately what is needed to prevent death or serious harm when a decision-maker is absent or refuses and delay would be dangerous. You document the necessity and revisit full consent once the child is stable. [1]
Consent pathway by who can decide
Epidemiology & Risk Factors
Consent fails most often at the seams. The common drivers are language discordance without a professional interpreter, low health literacy, separated or conflicted parents, unclear guardianship, and the cognitive load of medical complexity with many surrogate decision-makers. [1] [12]
Adolescent presentations raise mature-minor questions every day. Sexual health, contraception, sexually transmitted infection care, mental health, substance use and gender-affirming care are the recurring triggers. A young person may request care without a parent present, which forces you to assess capacity and confidentiality in real time. [7]
The base rate of implied or emergency consent shifts sharply by setting. Emergency departments and retrieval services see far more necessity-based treatment than elective clinics, where there is usually time for a proper conversation. [1]
Social determinants change both willingness and ability to engage. Racism, prior trauma, mistrust of institutions, disability, and involvement with youth justice all alter how a family enters a consent encounter, and a rushed process can look like refusal when the real problem is fear or access. [7] [12]
The evidence on fixed age cut-offs is thin. Chronological age is a poor proxy for capacity, which is why most modern frameworks move toward functional, decision-specific assessment rather than a single bright line. [4] [6]
Pathophysiology
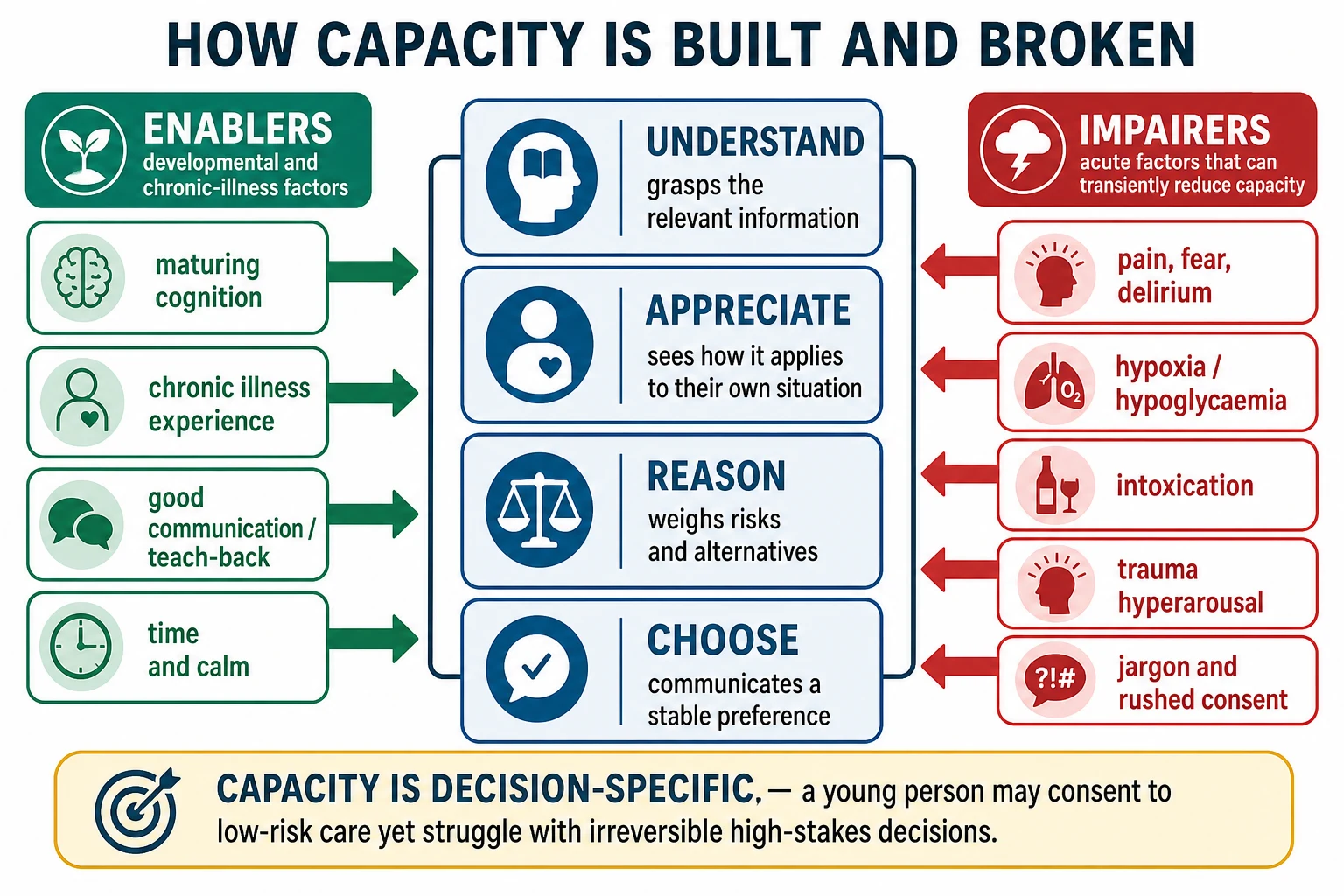
There is no enzyme for capacity, but there is a mechanism. Neurocognitive development reshapes how a child understands information, appreciates its personal relevance, reasons through trade-offs, and expresses a stable choice. [6]
Capacity is decision-specific, and the stakes matter. A young person may understand a low-risk, reversible decision thoroughly yet struggle with a high-stakes, irreversible one. The same brain that consents to a dressing change may not be ready to weigh a life-altering refusal. [3] [6]
Acute states impair capacity transiently. Pain, fear, hypoxia, hypoglycaemia, delirium, intoxication and severe mental illness can all erode the four domains, and the impairment often lifts once you treat the reversible cause. This is why you check glucose, oxygenation and pain before concluding a patient lacks capacity. [3]
Trauma physiology changes apparent agreement. Hyperarousal, freeze and dissociation can make a child or adolescent seem to consent when they are in fact frozen or trying to escape the encounter. A flat "yes" under threat is not a voluntary decision. [12]
The assent-versus-consent asymmetry is real and awkward. For some adolescents it is psychologically easier to accept care than to refuse it, especially life-saving care, because refusing carries a heavier cognitive and emotional load. Leading questions can manufacture false assent in preschool children, which is why you ask open questions and watch behaviour. [4] [12]
Clinical Presentation
From the doorway, a valid multi-party consent encounter looks calm, slow and explicit. Roles are named, the purpose of the decision is stated, and it is clear who is in the room and why. [12]
A neonate or infant presents a parental-permission decision with little or no meaningful assent. You obtain permission from the parental-responsibility holder, include both parents when available, and rely on the emergency exception when delay would harm the baby. [1]
A preschool child shows assent or dissent through behaviour rather than words. Cooperation with distraction is assent; rigid pulling away, crying and clutching are dissent. You read behaviour and adjust preparation, not push through. [2] [12]
A school-age child can voice preferences while the parent remains the default decision-maker. Their assent is sought in age-appropriate language, and their dissent is documented even when the parent authorises the procedure. [2]
An adolescent often brings mixed agendas. Delayed help-seeking, a request for confidential care, or a refusal on religious or personal grounds all trigger a mature-minor analysis rather than an automatic deferral to the parent. [7] [4]
Parental disagreement can present as one parent consenting while another refuses, sometimes surfaced only at the bedside. A reassuring social presentation can still hide invalid consent — coercion, a language barrier, or incomplete risk disclosure are invisible unless you look for them. [1]
Differential Diagnosis
When a child or parent refuses, your first task is to work out what kind of refusal it is. The label changes everything downstream. [3]
| Surface presentation | What it might actually be | Must-not-miss alternative |
|---|---|---|
| "The child refuses" | Developmental fear, not true dissent | Pain, delirium or hypoxia impairing assent |
| "The parent refuses" | Misunderstanding of risks or prognosis | Coercion or undue influence by a third party |
| "The teen says no to transfusion" | Capable informed refusal | Transient incapacity from fear or intoxication |
| "They don't want it" | Health-literacy or language gap | Safeguarding concern changing who can consent |
Discriminate true informed refusal from misunderstanding, untreated pain, coercion or transient incapacity. Treat the reversible cause first, then re-assess. A refusal given in delirium is not an informed refusal. [3]
Distinguish a capable young person from one who merely looks old enough. Age is a cue to assess, not a substitute for assessment. Distinguish the parental-responsibility holder from a de facto carer who has no legal authority for the decision. [1]
When a parent refuses critical care for a non-capable child, weigh the harm threshold. Where refusal risks serious, foreseeable and imminent harm, the state may override the parent under the harm principle — usually via senior escalation, ethics and the courts, not a solo registrar decision. [8] [9]
Clinical & Bedside Assessment
Open by naming roles and the purpose of the decision. State who is in the room, what decision is on the table, and how urgent it is. Then assess the four capacity domains adapted for age and development. [3]
Understand: can the child or young person restate, in their own words, what the intervention is, why it is proposed, and what it involves? Use teach-back rather than a yes-or-no check. Appreciate: do they grasp how it applies to their own situation, not in the abstract? Reason: can they weigh the risks and alternatives and give reasons for a choice? Choose: can they communicate a stable, voluntary preference? [3]
Structured tools such as the MacArthur Competence Assessment Tool were developed for adults and are adapted carefully in paediatrics. They support, but do not replace, clinical judgement, and there are no validated paediatric cut-scores to quote. [5]
Assess who holds parental responsibility and document identity and relationship. Do not assume the adult present has authority. Assess voluntariness directly — look for coercion, undue influence, time pressure and institutional power. [1]
Assess whether a professional interpreter is needed, and whether accessible information is required before seeking agreement. Using a family member as interpreter for a high-stakes decision is a recognised consent error. Assess developmental communication needs for assent — play, visual aids, simple language and time. [12]
Assess emergency-exception criteria when delay would cause significant harm. If the criteria are met, treat and document. Document the capacity findings, the information you gave, the questions answered, the decision, and any dissent. [1]
Investigations
There is no consent blood test, but there are reversible causes of apparent incapacity you must check before concluding a patient cannot decide. Bedpoint glucose, oxygenation, pain control and delirium screening all matter, because treating them can restore capacity within minutes. [3]
An adolescent sexual or substance-use history can change testing and consent pathways. Pregnancy testing, sexually transmitted infection screening and safeguarding-relevant history may shift who can authorise examination or photography. [7]
Certain records function as consent adjuncts. Court orders, guardianship papers, advance care plans and documented parental-responsibility arrangements carry authority you must verify and record. Read them before you proceed, not after. [1]
When a decision is genuinely contested, the "investigation" becomes the consultation itself. A second opinion, an ethics consultation or legal advice is the right next step rather than a further scan. Specialist psychiatry or psychology input helps for complex capacity assessments; most routine paediatric capacity is assessed at the bedside. [3] [9]
Prior documented refusals or advance wishes must be interpreted in light of current capacity. A refusal recorded weeks ago may no longer apply, and a now-capable young person may change their mind. Revisit rather than assume. [1]
Management — Resuscitation
When a child needs immediate life-saving treatment and a decision-maker is absent or refuses, treat first what prevents death or serious harm. Document the necessity and revisit full consent once the child is stable. [1]
State the emergency principle plainly: delay that risks death or serious harm overrides the ordinary consent sequence. This is necessity, not convenience, and you write down exactly what threat you were preventing. [1]
Parental refusal of blood products or other critical interventions is handled differently depending on capacity. For a non-capable child, the refusal may be overridden under the harm principle via senior escalation and usually the courts. For a capable adolescent's informed refusal of life-saving care, you face a genuine legal-ethical crisis that needs senior clinician, ethics and often legal input — never a solo override. [8] [10]
If imminent self-harm, assault or abuse is disclosed during a confidential adolescent conversation, your safeguarding duties engage. Confidentiality has limits, and you explain those limits honestly rather than promising secrecy you cannot keep. [1]
Allocate roles when consent conflict and resuscitation compete. One person leads the resuscitation, another manages the family conversation, and the consent status is handed over explicitly: who consented, whether emergency exception was used, and whether a court order is pending. [1]
Management — Definitive & Stepwise
Use a sequence you can defend out loud in a viva, anchored on the four capacity domains. [1] [3]
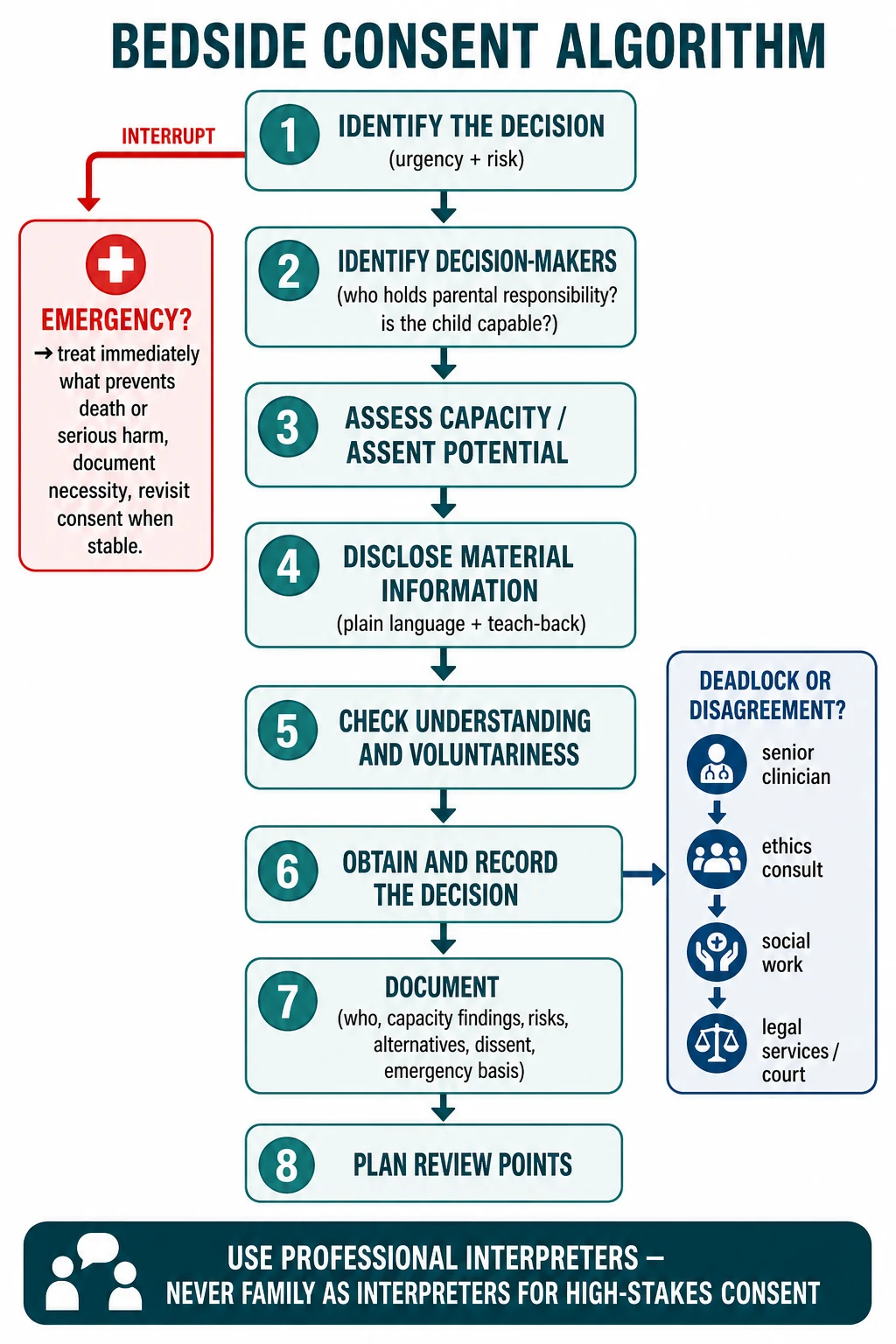
Bedside consent algorithm
Identify the decision — urgency and risk
Identify decision-makers — who holds parental responsibility, can the child decide?
Assess capacity and assent potential for this specific decision
Disclose material information in plain language with teach-back
Check understanding and voluntariness
Obtain and record the decision
Document who, capacity findings, risks, alternatives, dissent, emergency basis
Plan review points for staged or prolonged care
Structure parental permission for common procedures with age-appropriate assent. For an intravenous cannula, imaging with sedation, a lumbar puncture or surgery, name the procedure, its purpose, the material risks, the alternatives and what happens if you do nothing — in language the child and parent can both use. [1]
Open mature-minor analysis for a young person requesting confidential care. Assess the four domains for the specific decision, confirm voluntariness, and explore whether a trusted adult can be involved without forcing disclosure. Apply local statute and hospital policy for the operational thresholds. [4] [7]
Negotiate dual parental disagreement by setting. For elective care, defer, mediate and seek consensus or a second opinion. For urgent care where delay risks harm, escalate to senior clinician, ethics, social work or legal services rather than letting deadlock endanger the child. [9]
Shared decision-making tools help families reach a decision but do not replace legal consent requirements. Use them to structure the conversation, then confirm the authority basis separately. [11]
Document dissent by a child who lacks legal authority but still deserves a voice. Close in child-accessible language and confirm the plan with the caregiver. Arrange follow-up that reconfirms ongoing consent for staged treatment, sedation series or prolonged therapy. [1] [12]
Specific Subtypes & Scenarios
Neonate needing emergency surgery with one parent present. Treat under necessity, document, and involve the second parent and senior team as soon as possible. The emergency exception covers the window until full consent is possible. [1]
Preschool child refusing venepuncture with distressed parents. Read behaviour for dissent, build in play and topical anaesthesia, and do not equate a terrified freeze with assent. The parent authorises; the child's distress shapes preparation. [12]
School-age child with cancer treatment decisions. Layer progressive assent onto parental permission. The child's voice grows across a treatment arc, and a child who assented at diagnosis should re-assent as the plan evolves. [2] [11]
Adolescent requesting contraception without parental knowledge. Run a Gillick- or Fraser-style capacity analysis for the specific decision — understanding, appreciation, reasoning and choice — and apply local statute and policy for the operational threshold. Confidentiality is upheld within its legal limits. [4] [7]
Adolescent refusing life-saving transfusion on religious grounds. Treat this as a high-stakes, capable-refusal scenario. Assess capacity for this irreversible decision, involve senior clinicians and ethics early, and expect legal input, because courts internationally have moved toward overriding refusal of life-saving treatment in minors under defined conditions. [8] [10]
Separated parents disagreeing about elective tonsillectomy. For elective care, defer and mediate; clarify who holds parental responsibility and what your local policy requires before proceeding. Do not assume one parent's consent is enough. [1]
Child in out-of-home care. Identify the statutory guardian and the policy for routine versus major decisions. Routine care may sit with the carer; major decisions usually require the statutory decision-maker. [1]
Young person with mild intellectual disability consenting to a low-risk procedure. Assess decision-specific capacity with supported decision-making. Do not equate disability with incapacity, and bring in a support person the young person trusts. [6]
Telehealth consent. Verify identity, disclose limits of remote assessment, and document who consented and from where. Telehealth raises real risks of mistaken identity and incomplete disclosure. [1]
Research offered during clinical care. Separate clinical consent from research consent. Research assent and permission have their own standards, and a family can accept clinical care while declining the trial. [4] [5]
Complications & Pitfalls
- Treating chronological age as capacity. [3]
- Using family members as interpreters for high-stakes consent. [12]
- Promising absolute confidentiality that safeguarding duties will override. [1]
- Equating quiet cooperation with assent. [2]
- Proceeding on one parent's consent when local law or policy requires both or a specific holder. [1]
- Overriding a capable young person without legal basis. [10]
- Failing to treat under emergency exception when delay is dangerous. [1]
- Incomplete disclosure of material risks or alternatives. [2]
- Poor documentation of who decided, capacity findings and emergency basis. [1]
- Letting conflict escalate without early senior, ethics or legal help. [9]
Prognosis & Disposition
Good consent process pays off in the short term. Trust, adherence and fewer complaints follow a conversation in which the family understood the decision and felt heard. [1] [12]
A child can be discharged after a refused investigation if safety-netting is robust and the capacity and permission basis is clear. Name the red flags that should bring them back, and confirm who to call. [1]
A contested decision may require keeping the child in hospital pending senior or legal resolution. Do not discharge a safeguarding or high-stakes deadlock to an unsafe environment. [9]
After emergency treatment under necessity, disposition includes re-engaging the family once the child is stable. Re-open the consent conversation without framing the family as the enemy, and document the ongoing basis for continued care. [1]
Court or guardianship processes change who must be notified. Hand over incomplete consent status at every shift change — who consented, what is pending, and what escalation is live. Long-term relationship repair follows conflicted encounters, and a structured debrief helps the team and the family. [1] [9]
Special Populations
Neonates and infants. Parental permission only; include both parents when available; the emergency exception is common and should be used when delay would harm the baby. [1]
Children with disability or neurodiversity. Provide accessible information and supported decision-making. Never equate disability with incapacity; assess the specific decision with the supports the child usually uses. [6]
Intellectual disability. Assess decision-specific capacity, involve trusted support persons, and recognise that legal guardianship may apply for some decisions and not others. [6]
Indigenous families. Use a culturally safe process, identify kinship decision-makers, and avoid assuming a Western nuclear-parent model — while still verifying who holds legal authority for the decision. [12]
Migrant and refugee families. Use professional interpreters, pace the conversation for trauma, and explain the health-system norms that the family may not share. [12]
Out-of-home care and youth justice. Identify the statutory decision-maker and the local policy split between routine and major decisions. [1]
Gender and sexual diversity adolescents. Use confidential-care pathways and apply local law for mature-minor sexual and gender-affirming health care; capacity is assessed for the specific decision. [7]
Maltreatment contexts. Consent for examination may shift, and safeguarding duties override ordinary parental control where statute requires. [1]
Socioeconomic disadvantage and low health literacy. Use teach-back, plain language, time and written materials. A plan a family cannot afford or understand is not a valid consent. [12]
Palliative and life-limiting illness. Layer consent across goals-of-care conversations, link it to the care plan, and seek the child's voice even when it is not legally decisive. [2] [11]
Evidence, Guidelines & Regional Differences
The AAP 2016 informed consent policy and clinical report frame permission, assent and consent for US paediatric practice and remain the core anchor for the language examiners expect. [1] [2]
Appelbaum and Grisso defined the four capacity domains — understanding, appreciation, reasoning and expressing a choice — as adult-derived constructs adapted carefully to children. The MacArthur tools operationalise these domains but carry no validated paediatric cut-score. [3] [5]
Hein and colleagues found that many children from around twelve can consent to clinical research, informing a move from age-based to functional assessment; the same group showed the MacArthur tool's accuracy in children is imperfect, supporting clinical judgement over rigid scoring. [4] [5] Grootens-Wiegers and colleagues laid out the developmental and neuroscientific basis for how children and adolescents actually make medical decisions. [6]
On refusal, Diekema articulated the harm principle as the threshold for state intervention over parental refusal, and revisited how the best-interests standard is used and misused. Freckelton and McGregor traced the emerging international judicial consensus on refusal of life-saving treatment for minors. [8] [9] [10]
Coyne and colleagues' Cochrane review found limited, low-certainty evidence on interventions to promote children's participation in shared decision-making in cancer care — a reminder that the participation evidence base is still maturing. [11]
Australia and Aotearoa New Zealand approach consent through a mix of statute and common law. Parental responsibility and the mature-minor concept are governed by local legislation and case law, so state the principle — a capable minor can consent to the specific decision — and direct examiners to local statute, hospital policy and legal advice for operational thresholds. Never invent a statutory age or section number. [1] [4]
Exam Pearls
DECIDE
References
- [1]COMMITTEE ON BIOETHICS Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456514
- [2]Katz AL, Webb SA, COMMITTEE ON BIOETHICS Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [3]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment. N Engl J Med, 1988.PMID 3200278
- [4]Hein IM, De Vries MC, Troost PW, Meynen G Informed consent instead of assent is appropriate in children from the age of twelve: Policy implications of new findings on children's competence to consent to clinical research. BMC Med Ethics, 2015.PMID 26553304
- [5]Hein IM, Troost PW, Lindeboom R, Benninga MA Accuracy of the MacArthur competence assessment tool for clinical research (MacCAT-CR) for measuring children's competence to consent to clinical research. JAMA Pediatr, 2014.PMID 25317644
- [6]Grootens-Wiegers P, Hein IM, van den Broek JM, de Vries MC Medical decision-making in children and adolescents: developmental and neuroscientific aspects. BMC Pediatr, 2017.PMID 28482854
- [7]Viner RM, Ozer EM, Denny S, Marmot M Adolescence and the social determinants of health. Lancet, 2012.PMID 22538179
- [8]Diekema DS Parental refusals of medical treatment: the harm principle as threshold for state intervention. Theor Med Bioeth, 2004.PMID 15637945
- [9]Diekema DS Revisiting the best interest standard: uses and misuses. J Clin Ethics, 2011.PMID 21837884
- [10]Freckelton I, McGregor S Refusal of potentially life-saving treatment for minors: The emerging international consensus by courts. J Law Med, 2016.PMID 30136557
- [11]Coyne I, O'Mathuna DP, Gibson F, Shields L Interventions for promoting participation in shared decision-making for children with cancer. Cochrane Database Syst Rev, 2016.PMID 27898175
- [12]Levetown M, American Academy of Pediatrics Committee on Bioethics Communicating with children and families: from everyday interactions to skill in conveying distressing information. Pediatrics, 2008.PMID 18450887