Paeds · professional-practice-and-evidence
Goals-of-care conversations and advance care planning for children
Also known as Advance care planning children · Goals of care paediatrics · Serious illness conversation paediatric · Resuscitation planning children · Paediatric palliative care communication · Voicing My CHOiCES · Family-centred advance care planning
Fellowship-level approach to goals-of-care conversations and advance care planning (ACP) for children with serious or life-limiting illness: goals-of-care frames, the ACP document ladder, the Serious Illness Conversation Guide, age-appropriate tools (family-centred ACP, Voicing My CHOiCES), prognostic disclosure, documentation, dissemination, disagreement, and the evidence base.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a 12-year-old with relapsed leukaemia whose third admission in two months is for a febrile neutropenia that will not respond the way the first two did. Somewhere between the antibiotic order and the PICU referral, the team and the family need to answer a different question: what is the medical plan actually trying to achieve, and does it still match what this child and family most want? That is a goals-of-care conversation. It is not a single document and not a death sentence — it is the structured alignment of treatments with values, hoped-for outcomes and an honest sense of the trajectory. [1]
Advance care planning (ACP) is the broader, proactive process that surrounds that conversation for a child with a serious or life-limiting illness. It anticipates the decisions that are coming, captures what matters to the child and family, records it, and shares it so that when a crisis arrives the decision is already half-made. Done well, it moves the hardest choices out of a resuscitation bay and into a quiet room with the people who should be making them. [7] [9]
The common mistake is to treat goals of care as the thing you do when the child is dying. In children, most of the value sits upstream — in the oncology clinic, the complex-chronic medical home, and the PICU step-down — long before a terminal admission. The paediatric evidence is now strong enough that you can defend the practice at viva with randomised trials, not just expert opinion. [1] [2]
Classification
Sort the frames before you sort the documents, because the frame decides what the documents should say. [1]
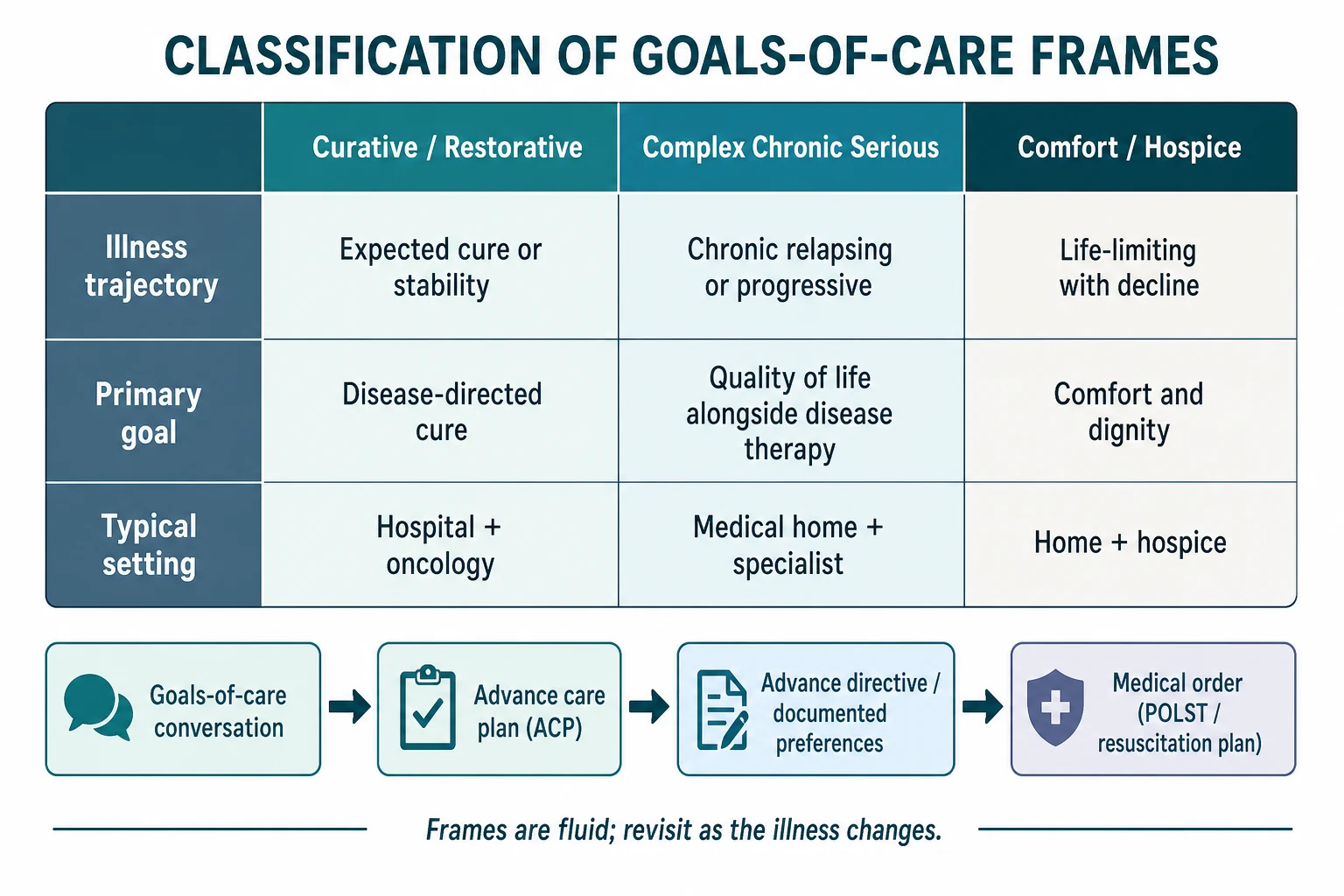
Three goals-of-care frames. Curative or restorative care aims at disease-directed cure or full recovery — the child with first-relapse salvageable disease, the reversible PICU admission. Complex chronic serious care manages an ongoing, often progressive illness where the goal is the best quality of life alongside disease-directed therapy — the technology-dependent child, the neurodegenerative condition. Comfort or hospice care prioritises dignity, symptom control and family presence when disease-directed options have run their course. These frames are fluid, not terminal labels: a child moves between them as the illness changes, and naming the current frame honestly is half the work. [1] [9]
The ACP document ladder. The conversation comes first, and it should happen early. Out of that conversation comes a documented advance care plan that records values, goals and the treatments the family would and would not want. Some of that becomes a formal advance directive or statement of preferences. Where it needs to act in a crisis it is converted into a portable medical order — a resuscitation plan, a POLST-equivalent, or an agreed limitation-of-treatment plan that travels with the child. Each rung depends on the one below it: an order without a conversation is fragile, and a conversation without documentation is invisible. [1] [12]
Life-limiting versus life-threatening. A life-threatening illness is one in which curative treatment may fail and the child may die, but cure remains the aim — much of paediatric oncology sits here. A life-limiting illness is one for which there is no reasonable hope of cure and which will shorten life; comfort care becomes central. The distinction shapes how early and how directly you frame the conversation. [9]
| Aspect | Goals-of-care conversation | Breaking bad news | Informed consent |
|---|---|---|---|
| Question it answers | What should the whole plan aim to achieve? | What has happened to my child? | Do I authorise this specific treatment? |
| Timing | Ongoing, repeated across the illness | At a new diagnosis or a change | Before each specific intervention |
| Output | A documented, disseminated care plan | Understanding and emotional support | Authorisation for one procedure |
| Who decides | Family plus team together over time | Clinician informs, family absorbs | Parent or mature minor |
Epidemiology & Risk Factors
The clearest fact in this area is that the conversation happens too late, too often. Parents of seriously ill children report being asked about their goals and wishes less often and later than they want, and the commonest setting for a first resuscitation decision is an acute deterioration rather than a planned meeting. A scoping review of parent experiences found that families value early, honest, individualised planning and are harmed when it is deferred to a crisis. [8] [9]
The children who most need an advance care plan cluster in recognisable groups: oncology patients with relapsed or refractory disease; children with severe neurological impairment and complex chronic conditions; those with progressive neuromuscular and metabolic disease; technology-dependent children with tracheostomies, ventilators or long-term ventilation; and children who have survived a critical PICU admission but face an uncertain trajectory. [1] [7]
The barriers are not mysterious. Clinicians fear taking away hope, feel untrained for the conversation, and work under prognostic uncertainty. Families fear that talking about death will make it happen, or that a comfort frame means abandonment. Systems reward throughput and fragmentation, so a plan made in oncology is not found in the emergency department. These are the failure modes an examiner expects you to name and plan around. [10] [12]
Pathophysiology
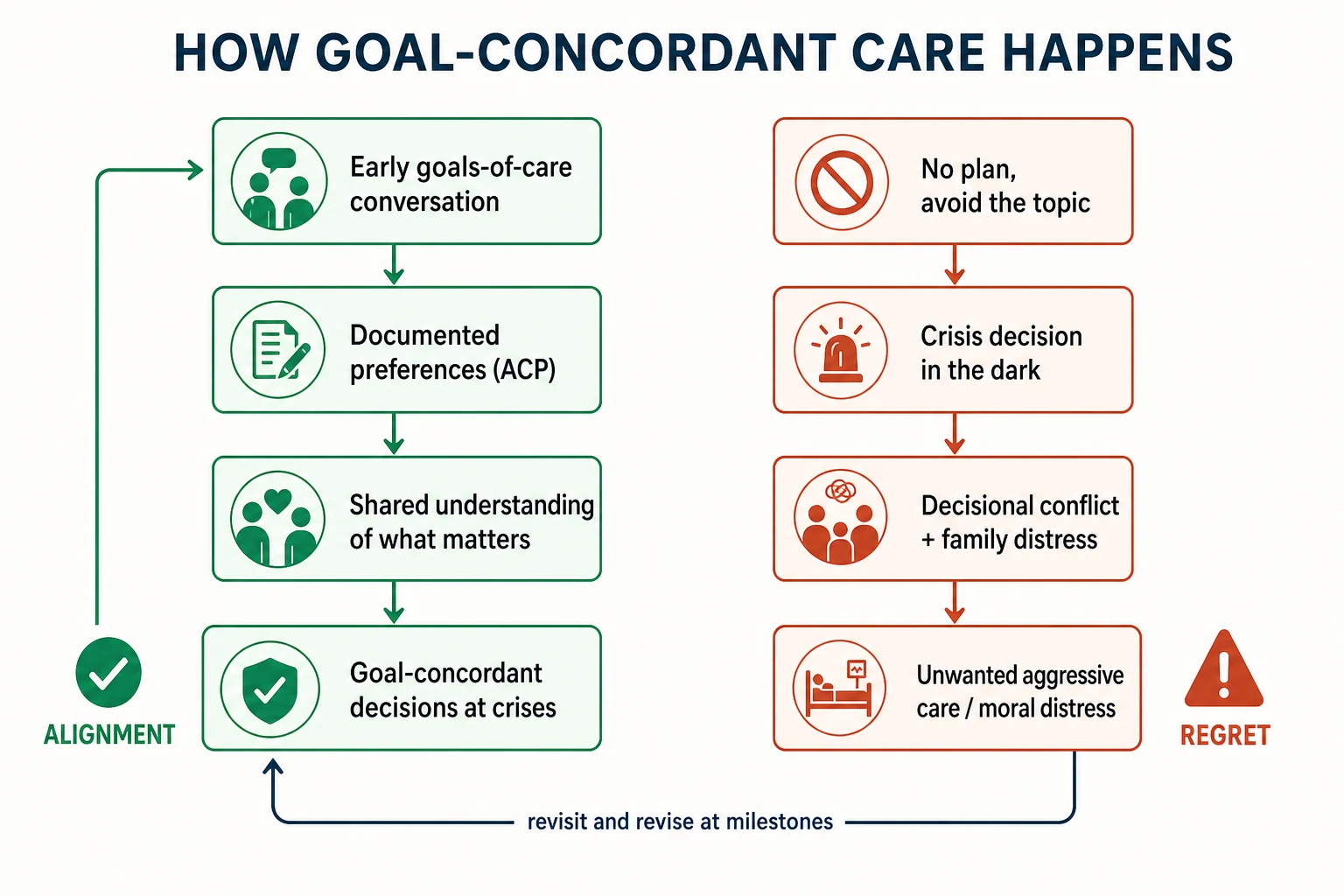
There is no enzyme for a good goals-of-care plan, but there is a mechanism, and it runs on information and trust. An early conversation surfaces what the family knows and what they fear; honest prognostic sharing corrects false expectations; the resulting documented preferences give the team a shared map. When the next deterioration arrives, the decision is made against that map instead of in the dark, and the family has already done the hardest emotional work. [1] [2]
The measurable output is congruence — the degree to which the adolescent and the family agree on what treatments they would and would not want at the end of life. Family-centred ACP for teens with cancer was built specifically to raise and sustain that congruence, and the randomised trial evidence shows it does, both at the time of the intervention and months later. That matters because incongruence at a crisis is the engine of decisional conflict, unwanted aggressive care, and family regret. [3] [6]
The failure pathway mirrors the success pathway in reverse. When the conversation is avoided, no preferences are documented; when a crisis hits, a frightened family is asked to choose without preparation; the default is to do everything; and the result is high-intensity care the child may not have wanted and moral distress for the team that delivers it. A plan that is written but never disseminated, or never revisited, fails the same way. [1] [8]
Clinical Presentation
You will usually recognise a goals-of-care conversation is due before anyone asks for one. The triggers are a new diagnosis of a life-limiting condition, disease relapse or progression, a cluster of repeated admissions, a clear decline in function or quality of life, or a planned high-risk intervention whose outcomes include death or major morbidity. Each of these is a fork where the frame may need to shift. [1] [9]
Parents give cues that the time is right. They ask what to expect, or what the future holds; they ask about their child's suffering; they say they want to do whatever is best; or they begin to pull back from another round of aggressive therapy without quite saying so. An adolescent may ask directly about dying, refuse further treatment, or want to talk about what they hope for. Reading these cues and offering the conversation — rather than waiting for a formal request — is the skill. [8] [11]
The high-yield clinical finding is the seriously ill child who has been admitted repeatedly yet has no documented goals-of-care plan. That gap is itself a problem to solve, not a neutral absence. [1]
Differential Diagnosis
When a goals-of-care conversation feels stuck or a family seems to want "everything," diagnose the obstacle before pushing the frame. [1] [8]
| Surface story | Real obstacle | What to do |
|---|---|---|
| "They want everything done" | Fear of abandonment, not preference for intervention | Reassure you will not leave them; separate comfort from giving up |
| "They are in denial" | Information gap or a different pace of processing | Re-assess understanding; share prognosis in graded, honest steps |
| "They will not decide" | Decisional conflict, not apathy | Add structure: options, values, a written plan and time |
| "The team disagrees" | Moral distress or a genuine best-interests conflict | Convene a goals-of-care meeting; involve palliative care and ethics |
| "They keep changing their minds" | Illness or values changing over time | Expected — plan to revisit, not a failure |
Keep two mimics in mind. First, breaking bad news is delivering a diagnosis or a poor result; it is emotionally heavy but it is information delivery, not the ongoing alignment of treatments with goals. Second, informed consent authorises a single intervention and is bounded by that intervention. Both may overlap with a goals-of-care conversation, but confusing them produces a single-event form where an ongoing process belongs. [1] [2]
Safeguarding can also distort a family preference: a child pushed toward, or away from, comfort care for reasons that are not their own. If the decision smells of coercion, your duty to protect operates alongside the partnership — you clarify who holds parental responsibility and you do not let a goals-of-care frame legitimise neglect. [1]
Clinical & Bedside Assessment
Diagnose the readiness before you run the meeting. Is the prognosis clear enough to share honestly? Who should be in the room — both parents, a grandparent, an adolescent, a trusted nurse? What does the family already know, and what have they said they want to know? Is there a language or cultural need that requires an interpreter or a cultural broker? Answering these in advance is what separates a meeting that lands from one that detonates. [1] [12]
Then assess the participants. How developmentally able is the child to take part, and what role do they and their parents want them to have? What is the family's caregiving burden and psychological state — a parent in acute distress cannot absorb a full prognostic disclosure in one sitting. Screen for decisional conflict, for spiritual or religious framing that will shape the goals, and for the sibling and extended-family needs that are so often missed. [4] [8]
Minimum pre-meeting assessment: [1] [9]
- Confirm the prognostic picture with the treating team and identify what is and is not reversible. [1]
- Identify the legal decision-makers and the child's capacity and preferred role. [9]
- Ask the family what they already understand and how much they want to be told. [8]
- Arrange language, cultural and spiritual support and a private space. [12]
- Decide who will run the meeting, who will scribe, and when it will be reviewed. [1]
Investigations
There is no blood test for a goals-of-care plan. The "investigations" here are the validated tools and documents that make the conversation reproducible and the record findable. [1] [2]
- Paediatric Serious Illness Conversation Guide — the structured, teachable script that adapts the Ariadne Labs serious illness approach to children, with a paediatric feasibility study showing it can be delivered by trained clinicians. [2] [10]
- Family-centred (FACE) advance care planning — the Lyon-developed, RCT-tested intervention for adolescents with serious illness that raises and sustains preference congruence. [3] [6]
- Voicing My CHOiCES — an age-appropriate advance care planning document for adolescents and young adults with cancer and other serious conditions, modelled on the adult Five Wishes. [11]
- Documentation that records the goals-of-care frame, the values elicited, the treatments wanted and not wanted, resuscitation status, preferred place of care and death, and named surrogate decision-makers. [1] [9]
A scoping review of guidelines and frameworks confirms that the common thread across regions is the same: the conversation must be structured, documented, disseminated and revisited. [12]
Management — Resuscitation
In a true emergency, life-sustaining treatment proceeds under implied consent while the goals-of-care conversation is urgently convened. You do not run a structured family meeting during an active resuscitation, and you do not demand a documented plan before treating a child who is arresting and has none. [1] [9]
What you do is treat the child, stabilise them, and then — the same day if possible — convene the senior clinician, the family and palliative care to establish the goals-of-care frame and to decide what should happen at the next deterioration. The resuscitation status is a medical order that flows out of that frame; it is never decided in isolation, and it is never the first or only thing discussed. [1]
When a family refuses life-sustaining treatment in an emergency, or when the team believes continued treatment is not in the child's best interests, escalate at once to the senior clinician, clinical ethics and the local legal pathway. Do not abandon the relationship while you resolve the disagreement. [1]
Management — Definitive & Stepwise
Use a structure you can recite under viva pressure. The Serious Illness Conversation Guide gives you five steps — set up, assess, share, align, plan — and the paediatric version adapts them for families and for the child's developmental stage. [2] [10]
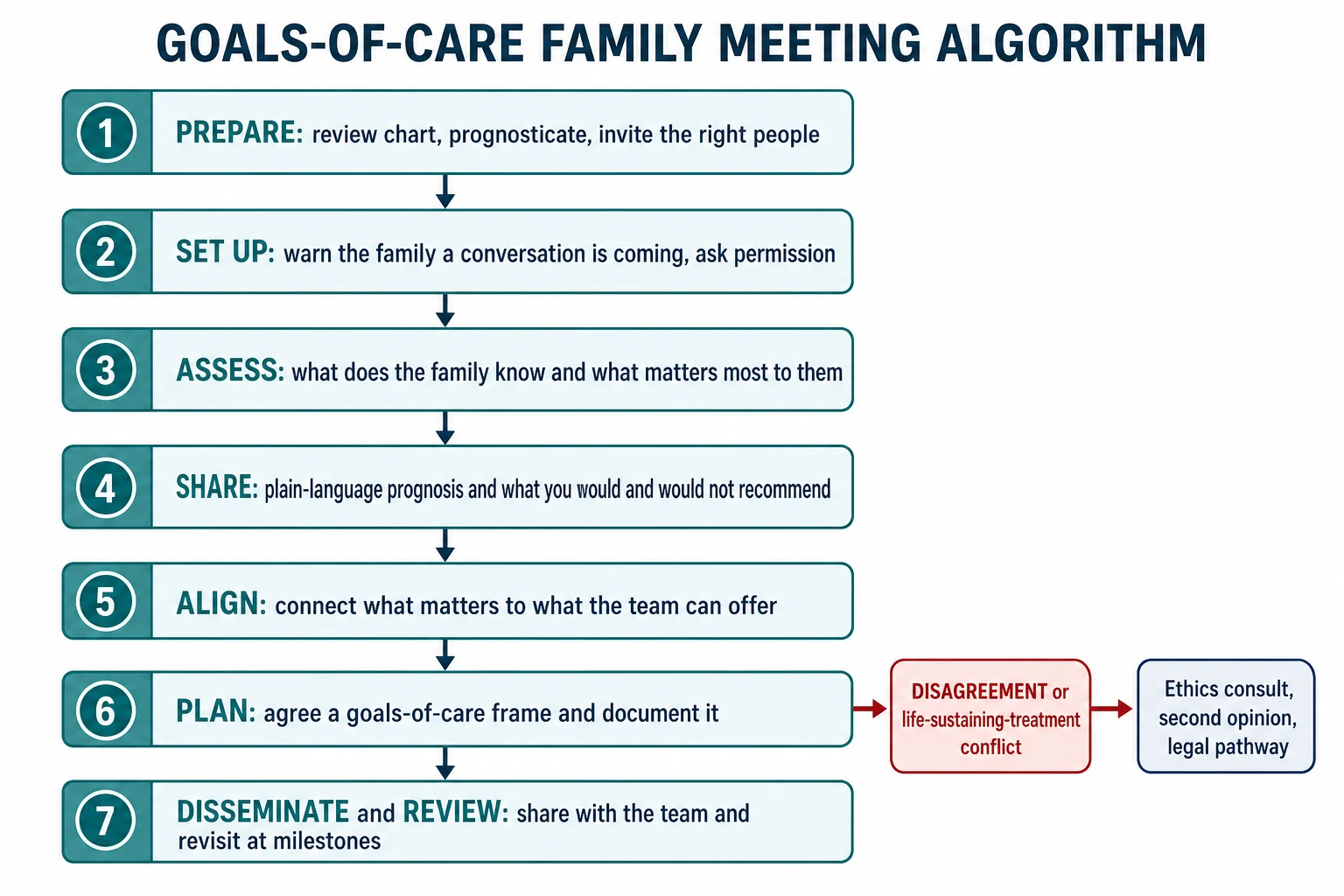
Goals-of-care family meeting algorithm
Prepare: review the chart, prognosticate with the team, invite the right people and a quiet space
Set up: warn the family a conversation is coming and ask permission to talk honestly
Assess: elicit what they know, how much they want to know, and what matters most to them
Share: give plain-language prognosis and what you would and would not recommend
Align: connect what matters to what the team can offer and name the goals-of-care frame
Plan: agree the frame, record treatments wanted and not wanted, and write the medical order
Disseminate and review: share with the whole team, family and primary care; revisit at milestones
Share prognosis honestly, with compassion. The evidence is clear that honest prognostic disclosure does not destroy hope or cause depression in this population; it lets families prepare and reframe hope from cure toward comfort, legacy and presence. Use plain language, pause for emotion, and respond with the NURSE statements — name, understand, respect, support, explore — rather than racing on. [8] [11]
Tailor to age and capacity. For a developmentally able adolescent, use Voicing My CHOiCES or the family-centred ACP structure so their voice is captured directly, not mediated entirely through their parents. For a non-verbal or pre-verbal child, elicit comfort cues and treat parents as the surrogates who know the child best. A plan built only from the adult's perspective fails the child who can take part. [3] [11]
Document, disseminate, review. A usable plan records the goals-of-care frame, the values behind it, the specific interventions agreed and declined, the resuscitation status, the preferred place of care and death, and the named decision-makers. It lives in the medical record, is summarised for the family and primary care, is converted to a portable order that retrieval and emergency services can find, and carries a review date. A plan that cannot be found at a crisis is no plan. [1] [12]
Escalate when stuck. When the family and team cannot reach agreement, or when a life-sustaining-treatment decision is contested, escalate to palliative care, a clinical ethics consult, a second opinion, and — where the dispute cannot be resolved — the local legal pathway. Best interests is a structured weighing of the child's welfare, not a slogan to end the conversation. [1] [9]
Specific Subtypes & Scenarios
Adolescent oncology. The strongest evidence sits here. Family-centred ACP for teens with cancer, developed and tested by the Lyon group across a programme of randomised trials, raised and sustained adolescent-family congruence on end-of-life preferences, improved family positive caregiving appraisals, and supported adolescent preparedness and quality of life. This is the scenario an examiner wants you to evidence with trials, not platitudes. [3] [4] [5] [6]
Complex chronic neurological impairment. Technology-dependent children with severe neurodisability and conditions such as severe cerebral palsy, neurodegenerative or metabolic disease need ACP that weighs the burden of interventions (surgery, recurrent admissions, escalation to PICU) against their benefit for the child's experienced quality of life. The family is usually the best informant on what the child's baseline looks like. [1] [7]
PICU and withdrawal of life-sustaining treatment. When a critically ill child will not recover, the goals-of-care frame shifts to comfort, and the plan may include withdrawal of life-sustaining treatment with the family present, symptom control, and structured bereavement support. The conversation that should have happened earlier often has to happen here — run it with the same structure, and lean on palliative care. [1] [9]
Neonatal and perinatal. When a life-limiting diagnosis is made antenatally or at birth, advance care planning begins with antenatal counselling that sets realistic expectations and agrees a resuscitation and comfort plan for delivery. These conversations are longitudinal and often span pregnancy, birth and the neonatal unit. [1]
Adolescents and young adults and transition. As capacity matures, the young person moves from being represented toward representing themselves. Voicing My CHOiCES captures their wishes directly, and transition planning must hand the documented plan and the decision-making over to adult services rather than losing it at the boundary. [11] [12]
Complications & Pitfalls
- Deferring the conversation until a crisis, when the family is least able to decide. [1] [8]
- Treating a one-off resuscitation decision as the goals-of-care process. [9]
- Sharing prognosis so bluntly that you crush hope, or so evasively that you give false hope. [8] [11]
- Writing a plan that no one on the team can locate at the next admission. [1] [12]
- Failing to revisit the plan as the illness, the values or the child's capacity change. [7]
- Excluding a developmentally able child from the conversation about their own care. [3] [11]
- Letting symptom control, sibling needs and bereavement support fall through the cracks. [1]
- Reading disagreement as non-compliance instead of a values or trust gap. [8] [10]
Prognosis & Disposition
The honest evidence is that structured paediatric ACP changes the right outcomes. It increases and sustains adolescent-family preference congruence, improves family positive caregiving appraisals and preparedness, and supports adolescent quality of life and preparedness. [3] [4] [5]
A defensible point at viva: advance care planning does not cause depression, does not take away hope, and does not hasten death. Families who are offered it report feeling more, not less, supported. The fear that naming the possibility of dying will harm the child is the commonest reason the conversation is delayed, and it is not borne out by the evidence. [8] [11]
Disposition is a living plan, not a form. It is a documented goals-of-care frame, disseminated across every setting the child may enter, reviewed at milestones, and accompanied by symptom control and bereavement support for the family when a child dies. The outcome ACP is designed to achieve is goal-concordant care — that the treatment a child receives at the end matches what they and their family wanted. [1] [2]
Special Populations
Adolescents and young adults. Assess evolving capacity for the specific decision, offer confidential time, use Voicing My CHOiCES to capture their voice, and plan the transition of both decision-making and care to adult services. [11] [12]
Children with complex chronic neurological impairment. Rely on parents as expert surrogates for the child's baseline quality of life, anchor decisions in the child's best interests, and weigh the burden of each intervention against its realistic benefit. [1] [7]
Culturally and linguistically diverse families. Use professional interpreters and cultural brokers, and respect frameworks around truth-telling and who may decide that differ from your own. A plan that assumes a Western disclosure model can fail a family it was meant to serve. [8] [12]
Pre-verbal and non-verbal children. Elicit comfort cues directly and treat parents as the surrogates who know the child's baseline suffering and enjoyment of life best. [1]
Out-of-home care and safeguarding. Clarify who holds parental responsibility and legal authority before the conversation, and ensure the goals-of-care frame does not mask neglect or coercion. [1]
Evidence, Guidelines & Regional Differences
Practice anchors: the Rapoport overview of goals-of-care conversations and ACP for seriously ill children; the DeCourcey and Wolfe feasibility study of the Pediatric Serious Illness Conversation Program; the Doherty implementation evidence on clinician experience after training; and the Lyon programme of family-centred ACP randomised trials in adolescent oncology. [1] [2] [3] [4] [5] [10]
The reviews fill the frame: the Michiels systematic review on age-appropriate ACP, the Bennett scoping review of parent experiences, the Loeffen and Verhagen guidance on individualised ACP, the Wiener work on Voicing My CHOiCES, and the Linane scoping review of guidelines and frameworks for adolescents and young adults. [6] [7] [8] [9] [11] [12]
Controversies to handle calmly: when exactly to hold the first conversation; how to balance hope and honesty without collapsing into one; how far adult serious-illness tools generalise to children and to non-oncology conditions; and how to close the equity gap so that access to paediatric palliative care does not depend on postcode, language or socioeconomic status. [7] [12]
In Australia and Aotearoa New Zealand, paediatric advance care planning is supported by national palliative care frameworks and by state-based portable resuscitation and goals-of-care order schemes. Local hospital policy governs how a plan is documented and how it travels with the child across services and during retrieval. [1]
Exam Pearls
PLAN-AHEAD
References
- [1]Rapoport A Goals of care conversations and advance care planning for paediatric patients living with serious illness. Paediatr Child Health, 2024.PMID 39539786
- [2]DeCourcey DD, Bernacki RE, Nava-Coulter B, Lach S, Xiong N, Wolfe J Feasibility of a Serious Illness Communication Program for Pediatric Advance Care Planning. JAMA Netw Open, 2024.PMID 39058485
- [3]Needle JS, Friebert S, Thompkins JD, Grossoehme DH, Baker JN, Jiang J, Wang J, Lyon ME Effect of the Family-Centered Advance Care Planning for Teens with Cancer Intervention on Sustainability of Congruence About End-of-Life Treatment Preferences: A Randomized Clinical Trial. JAMA Netw Open, 2022.PMID 35819787
- [4]Thompkins JD, Needle J, Baker JN, Briggs L, Cheng YI, Wang J, Friebert S, Lyon ME Pediatric Advance Care Planning and Families' Positive Caregiving Appraisals: An RCT. Pediatrics, 2021.PMID 33958436
- [5]Friebert S, Trujillo Rivera EA, Baker JN, Thompkins JD, Grossoehme D, Needle J, Lyon ME Pediatric Advance Care Planning and Adolescent Preparedness and Quality of Life: An RCT. Pediatrics, 2025.PMID 39821687
- [6]Lyon ME, Jacobs S, Briggs L, Cheng YI, Wang J Family-centered advance care planning for teens with cancer. JAMA Pediatr, 2013.PMID 23479062
- [7]Brunetta J, Fahner J, Legemaat M, van den Bergh E, Krommenhoek K, Prinsze K, Kars M, Michiels E Age-Appropriate Advance Care Planning in Children Diagnosed with a Life-Limiting Condition: A Systematic Review. Children (Basel), 2022.PMID 35740767
- [8]Bennett HE, Duke S, Richardson A Paediatric advance care planning in life-limiting conditions: scoping review of parent experiences. BMJ Support Palliat Care, 2023.PMID 37201934
- [9]Loeffen EAH, Tissing WJE, Schuiling-Otten MA, de Kruiff CC, Kremer LCM, Verhagen AAE Individualised advance care planning in children with life-limiting conditions. Arch Dis Child, 2018.PMID 29127099
- [10]Doherty M, Gujral P, Frenette M, Lusney N, van Breemen C The Pediatric Serious Illness Conversation Program: Understanding challenges and experiences for clinicians after advance care planning training. Palliat Support Care, 2024.PMID 37288722
- [11]Wiener L, Bedoya S, Battles H, Sender L, Zabokrtsky K, Donovan KA, Thompson LMA, Lubrano di Ciccone BB, Babilonia MB, Fasciano K, Malinowski P, Lyon M, Thompkins J, Heath C, Velazquez D, Long-Traynor K, Fry A, Pao M Voicing their choices: Advance care planning with adolescents and young adults with cancer and other serious conditions. Palliat Support Care, 2022.PMID 35876450
- [12]Linane H, Tanjavur B, Sullivan L A scoping review of guidelines and frameworks for advance care planning for adolescents and young adults with life-limiting or life-threatening conditions. Palliat Med, 2024.PMID 38600067