Paeds · professional-practice-and-evidence
High-value care, stewardship and avoiding low-value interventions
Also known as High-value care in paediatrics · Low-value care and overuse · De-implementation and reducing overuse · Resource stewardship and value-based care · Choosing Wisely and antimicrobial stewardship
Fellowship guide to high-value care and stewardship in paediatrics: defining value, recognising low-value care, overuse and overdiagnosis, the clinician, family and system drivers of overuse, how low-value care harms children through care cascades and opportunity cost, common paediatric low-value practices, and the stepwise de-implementation cycle with its evidence-based levers — framed as good medicine and justice rather than rationing, with ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Stop an overused practice in the right order
Overview & Definition
A mother brings her feverish, snuffling two-year-old and asks for "the antibiotics that worked last time." You are confident this is a viral upper respiratory infection, yet the easy path is to prescribe and move on. This ordinary encounter is where stewardship lives. High-value care is care that maximises a child's benefit relative to the harm, cost and opportunity it consumes, and low-value care is any test, treatment or procedure whose likely harm or cost exceeds its likely benefit. [1] [8]
The discipline rests on three ideas that the examiner will expect you to name. Value is a ratio, not a price: an expensive intervention can be high-value and a cheap one low-value. [8] Overuse — doing too much — is the principal target of stewardship in well-resourced settings, sitting alongside underuse and misuse as the ways care can go wrong. [7] And stewardship is an ethical duty, not a budgetary one: every test or treatment consumes a finite resource and carries a finite risk, so the responsible clinician spends them only where they are likely to help. [2] [8]
This page owns the principles, the harm, the measurement and the de-implementation of low-value care in child health. The statistical machinery for judging whether a therapy works belongs to the evidence-based medicine leaf, and the conversation skills for explaining restraint belong to shared decision-making and risk communication — cross-link them rather than rebuilding their content. [1]
Classification
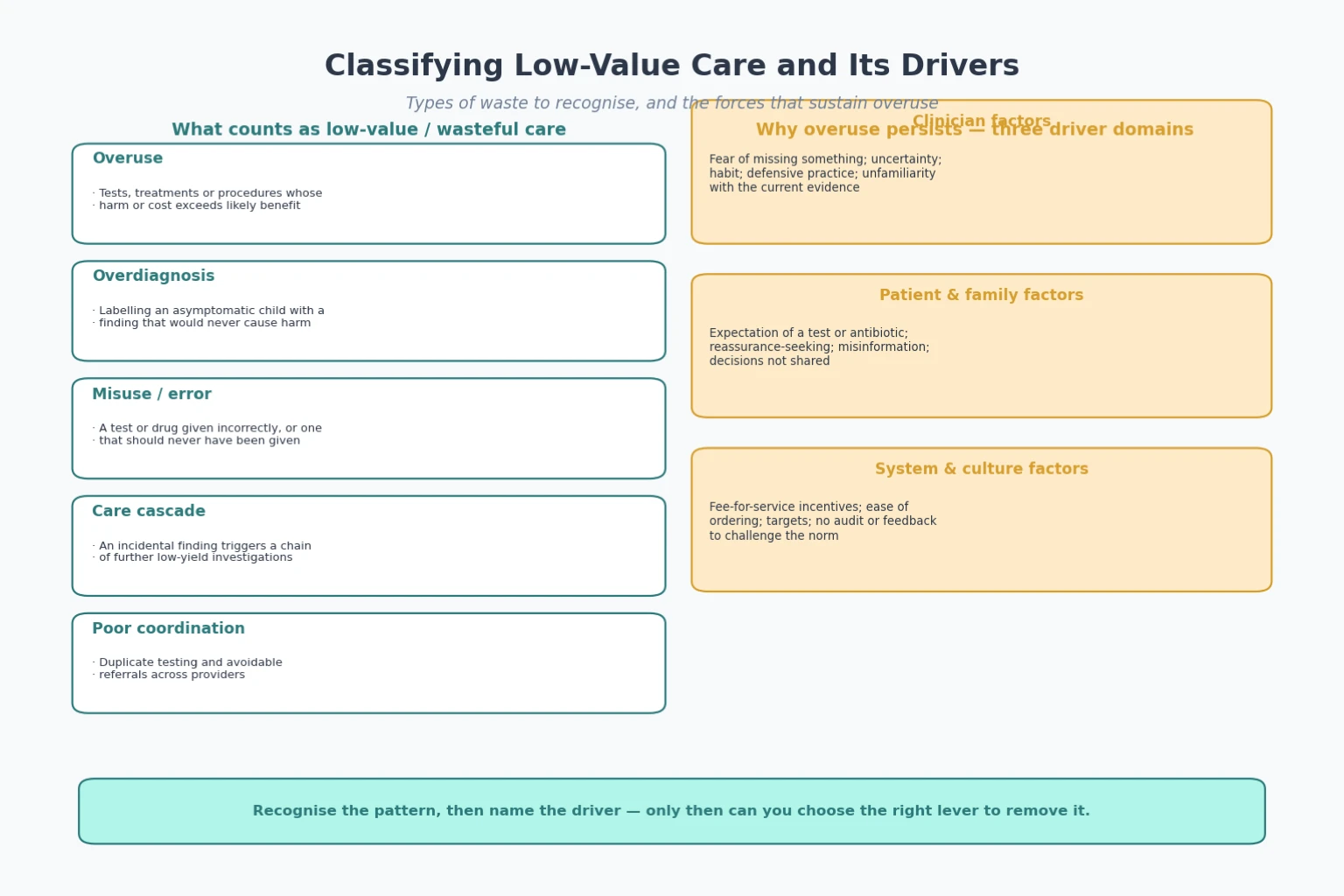
Low-value care wears several faces, and naming the pattern tells you which lever to pull. The simplest split is into three failures of care: overuse, where we do too much; misuse, where we do the right thing the wrong way; and underuse, where we do too little of an effective intervention. [7] Overuse is the dominant problem in well-resourced child health and the primary focus of this page, but a stewardship drive that cuts overuse must guard against widening underuse of high-value care. [8]
A sharper distinction separates overuse from overdiagnosis. Overuse is an action that should not have happened; overdiagnosis is a true finding that should not have mattered. [5] When a borderline incidentaloma on a scan is labelled and treated, the diagnosis is real but clinically irrelevant, and the harm — anxiety, surveillance, intervention — is real too. [5] [10]
A useful way to think about waste, set out by Berwick and refined by others, groups it into overtreatment, failures of care delivery, failures of care coordination, and administrative complexity. [2] [3] For a child, the practical categories are simpler: an unnecessary test, an unnecessary treatment, a duplicate test no one coordinated, and the cascade that follows when any of these throws up a stray finding. [14]
Epidemiology & Risk Factors
The scale of low-value care is large and is documented in every well-resourced system. A substantial fraction of routine care brings little or no benefit, and estimates of total waste in health spending run to a quarter or more. [2] [3] Paediatric overuse is common enough to be tracked systematically, with regular reviews cataloguing tests and treatments whose use exceeds the evidence. [4]
Three families of forces sustain overuse, and the candidate should be able to name a driver from each. Clinician factors include fear of missing a diagnosis, diagnostic uncertainty, ingrained habit, defensive practice and simple unfamiliarity with current evidence. [9] [11] Family factors include the expectation of a test or an antibiotic, reassurance-seeking, misinformation, and decisions that were never shared. [9] System factors include fee-for-service incentives, the ease of ordering a test, target-driven cultures, and the absence of audit and feedback to challenge the norm. [13]
Children are exposed to these forces in particular ways. The evidence base is thinner and more often extrapolated from adults, parents act as proxy decision-makers whose anxiety can amplify demand, and a "do everything" instinct is strongest when the patient is young. [4] [5] Recognising these child-specific pressures is the first step to resisting them.
Pathophysiology
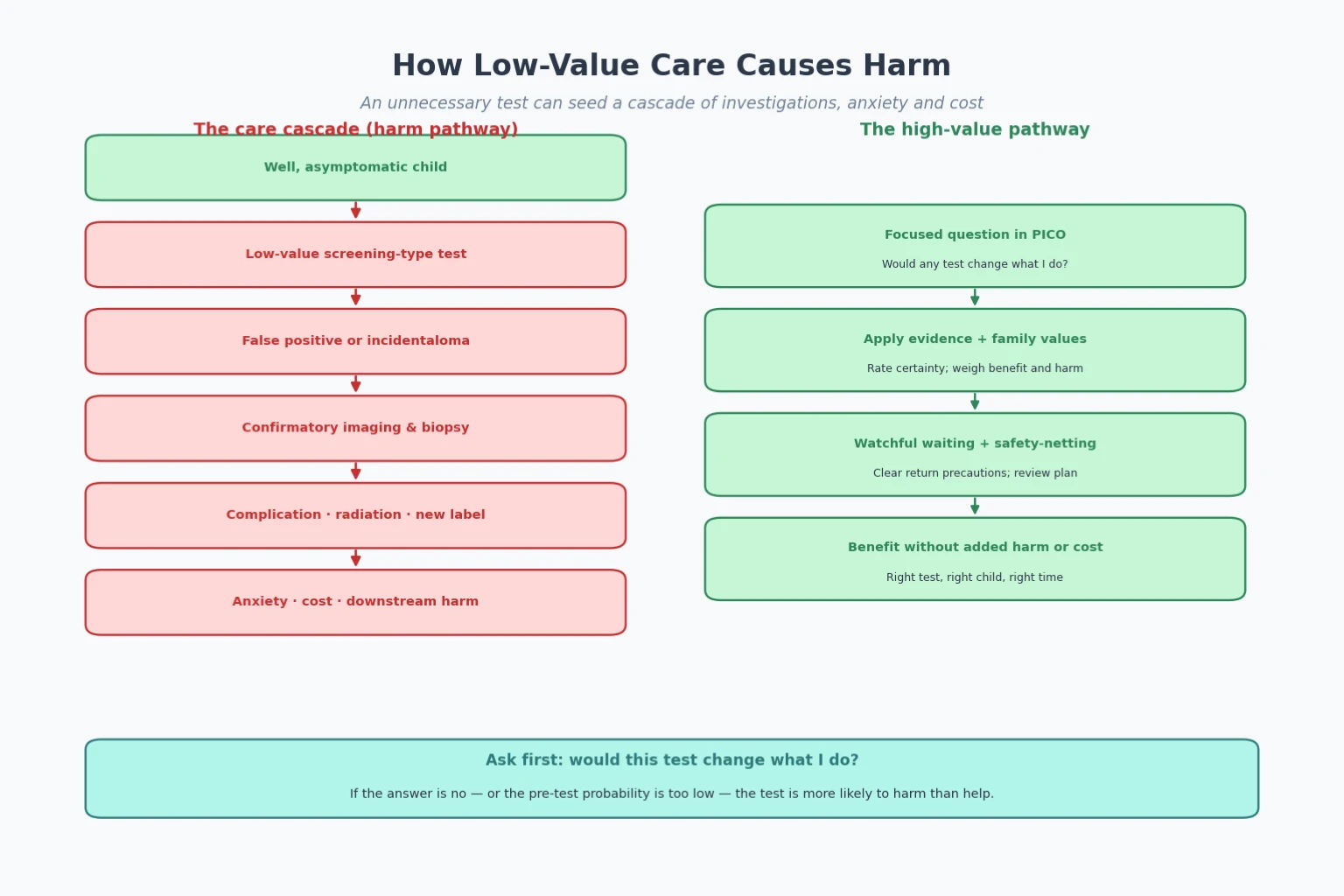
How does a test ordered for a good child with a low probability of disease end up causing harm? The mechanism is the care cascade. A screen applied to a low-risk population throws up more false positives than true positives, and each positive prompts confirmatory imaging, biopsy and further intervention. [14] The downstream burden — radiation, sedation, complications, days off school, family anxiety and cost — can dwarf the original problem and may never resolve it. [14]
Overdiagnosis is the quiet companion of the cascade, and it harms without any error. A real but clinically irrelevant finding is detected, labelled and treated, and the child carries a diagnosis that would never have become apparent. [5] [10] Because the finding is genuine, the harm is easy to overlook; because the surveillance and treatment are real, the harm is real too. [10]
Unnecessary antimicrobials travel their own harm pathway. Each prescription that is not needed adds to selection pressure for resistance, risks an adverse drug reaction, and disturbs the developing microbiome. [16] At the level of the system, every low-value intervention carries an opportunity cost: the money, time and attention spent on it are then unavailable for the high-value care that genuinely helps. [2] [8]
The clinician's own mind sustains these pathways. Availability bias makes the vivid missed diagnosis loom large, commission bias favours action over inaction, and the fear of complaint tilts the decision toward the test that "covers" the clinician rather than the one that helps the child. [9] [11] Naming these biases is not an excuse; it is the first defence against them.
Clinical Presentation
Low-value care announces itself in the everyday, not the dramatic. A parent requests an antibiotic or a scan for a self-limiting viral illness, framing last time's prescription as the cure. [16] A well child booked for day surgery is added to the "routine pre-operative bloods and chest radiograph" list by default. [15] A borderline incidental finding on an imaging study triggers a chain of further, low-yield investigations and a spiral of family anxiety. [14]
The request for more is the most common presentation, and it is usually well-meaning. Families want certainty, reassurance and a sense that everything has been done, and a clinician who simply refuses risks looking dismissive or cost-driven. [9] The skill is to validate the concern, explain why non-doing is the higher-value choice, and offer a clear safety-net. [13]
A third presentation is the service that wants to change. A department notices it orders far more viral panels or bronchodilators for bronchiolitis than its peers, and asks how to do better. This is de-implementation at the system level, and it calls for the same cycle as an individual decision, scaled up with measurement and feedback. [13] [6]
Differential Diagnosis
When you face a proposed test or treatment, the real diagnostic question is whether it will help this child. The first fork is between a test that will change management and one that will merely reassure or cascade. [14] A test whose result will not alter your plan is a candidate for omission regardless of its accuracy.
The second fork separates a genuinely indicated treatment from an overused one sustained by habit or demand. Antibiotics for a clear viral illness, imaging for a minor head injury that meets a low-risk rule, and routine pre-operative testing in a fit child all fall on the low-value side. [4] [15]
The third and most important fork guards against harm in both directions. Evidence-based restraint must be distinguished from harmful under-investigation, and from rationing. [8] When you are unsure, ask whether you are withholding a high-value intervention to save money, or omitting a low-value one to protect the child — only the second is stewardship.
Restraint, rationing and underuse — keeping them apart
Clinical & Bedside Assessment
At the bedside, stewardship begins with a single question asked before every order: will this test or treatment change what I do, or help this child? [1] If the answer is no, the default is to wait, watch and safety-net rather than to test. The pre-test probability is the key variable: when disease is unlikely, even a good test yields more false positives than true ones and the cascade begins. [14]
Weigh the certainty and applicability of the evidence before you adopt an intervention, not only its headline benefit. A therapy that halves a rare complication may still be low-value if the absolute benefit is tiny, the harms are real, and the trial population does not match your patient. [8] This is the appraisal skill owned by the evidence-based medicine leaf, applied here to the decision to do less.
Where a target practice has been chosen for reduction, assess it with a validated overuse measure. [6] [12] Quantifying how often the practice is used, in which patients, and with what downstream effect turns a vague impression into a tractable problem. [6]
Finally, elicit the family's understanding, fears and expectations. A parent who expects an antibiotic is not an obstacle to stewardship; they are its first partner. When you understand what they are hoping the treatment will achieve, you can offer a higher-value way to meet that need. [9]
Investigations
Investigations are the heartland of low-value care, so the investigative section of a stewardship answer is mostly about what not to do. Make "do I need any test to change what I do" the default screen before any order, and apply a validated decision rule where one exists. [4] Rules such as PECARN for minor paediatric head injury are designed precisely to spare children unnecessary computed tomography while not missing the rare significant injury.
Use Choosing Wisely, EVOLVE and society "do-not-do" recommendations to identify low-value practices specific to children. [1] [15] These clinician-led lists name common practices whose evidence does not support them, and they give a defensible starting point for any de-implementation effort.
Before changing practice, audit the baseline rate of the target practice in your own setting. [6] Knowing the starting point lets you set a tractable goal, choose the right lever, and demonstrate improvement to a sceptical team. Pair the count of the practice itself with a measure of its downstream effect — the cascade, the cost, the days of school missed. [14]
When you do investigate, prefer the test with the highest yield and the lowest cascade risk, and build the safety-net into the plan so that non-doing never becomes abandonment. [8]
Management — Resuscitation
Stewardship has an acute face, and the candidate should be able to describe it. A child may come to harm directly from an unnecessary intervention: a complication of a procedure that should not have been performed, an adverse reaction to an inappropriately prescribed antibiotic, or a prescribing cascade in which the side effect of one unnecessary drug is mistaken for a new condition and treated with another. [16]
The resuscitation priorities are unchanged — airway, breathing, circulation — but the disclosure is not. Once the child is stabilised, the team must honestly acknowledge that the harm arose from an unnecessary intervention, report it through local incident systems, and feed the lesson back into a de-implementation effort so that the next child is spared. [2]
A cascade of incidental findings generating repeated invasive testing is an emergency of a different kind, demanding that the team pause, review the pre-test probability, and stop the chain rather than add another link. [14] Stopping a cascade is itself a resuscitative act for the family's wellbeing.
Management — Definitive & Stepwise
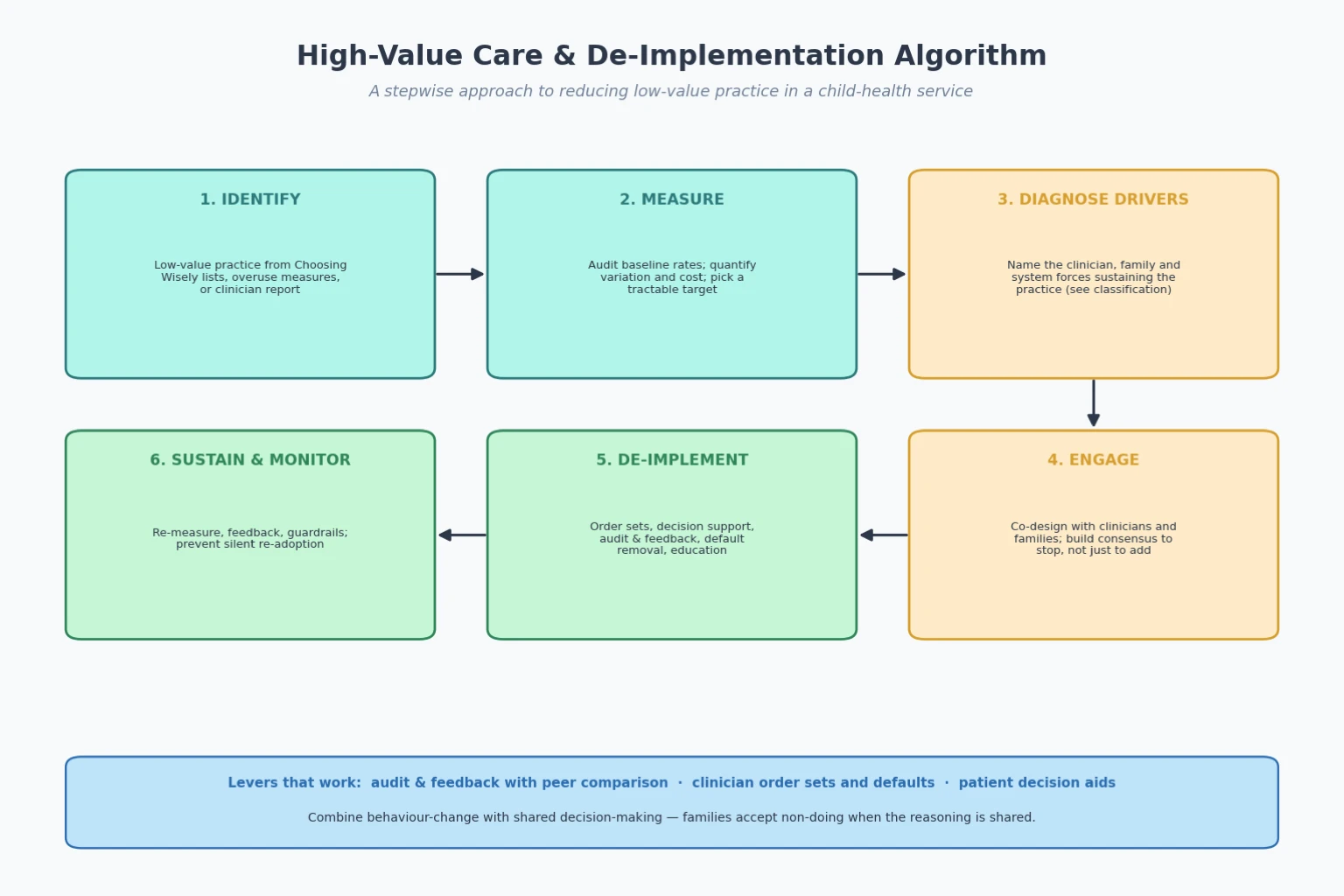
Once the acute situation is controlled, the lasting management of low-value care is de-implementation, and it follows a cycle the candidate should be able to recite. [9] [13] Each step has a clear purpose, and skipping one is the commonest reason a campaign stalls.
First, identify a low-value practice using Choosing Wisely lists, validated overuse measures, or clinician and family report. [15] Second, measure the baseline rate, quantify the variation and the cost, and choose a tractable, measurable target. [6] Third, diagnose the drivers sustaining the practice across the clinician, family and system domains, because the lever must match the driver. [9]
Fourth, engage clinicians, families and consumers to co-design the change and build consensus to stop, not merely to add. [13] Fifth, de-implement with combined levers rather than a single memo: clinician order sets that change the default, embedded decision support, audit and feedback with peer comparison, patient decision aids that reduce demand, and targeted education. [13] [16]
Sixth, sustain and monitor by re-measuring, feeding back, and installing guardrails that prevent silent re-adoption. [6] The single best-evidenced lever is audit and feedback paired with peer comparison, which shifts the social norm as well as the individual decision. [13] [16]
The size of the problem and the leverage of feedback
Specific Subtypes & Scenarios
Antibiotics for viral respiratory infection are the most common paediatric low-value practice and the archetype of de-implementation. Delayed or backup prescriptions, point-of-care decision support, and family decision aids together reduce prescribing while preserving satisfaction, and outpatient antimicrobial stewardship has been shown to cut broad-spectrum use in a randomised trial. [16] This is the scenario the examiner will reach for most often.
Imaging after minor head injury illustrates the disciplined use of a validated rule. PECARN and similar tools identify children so low-risk that computed tomography is more likely to harm than to help, sparing radiation and cascades without missing significant injury. [4] The rule is not a barrier to imaging; it is the evidence-based threshold for it.
Routine pre-operative testing in otherwise healthy children before low-risk surgery is a third classic. Blood tests, electrocardiograms and chest radiographs in a fit, asymptomatic child rarely change management and carry their own burden, and Choosing Wisely in paediatric hospital medicine names them among its opportunities for improved value. [15]
Antimicrobial stewardship deserves special mention as the model programme. Blending formulary restriction, prospective audit with feedback, and education, it has reduced resistance, adverse events and cost while protecting outcomes, and it shows what a mature de-implementation system looks like. [16]
Finally, there is the conversation scenario: a family who expects "everything" must be helped to see restraint as good medicine. Here the tool is shared decision-making — eliciting values, presenting the absolute benefit and harm honestly, and offering a clear safety-net — so that non-doing is understood as care, not denial. [9] [13]
Antimicrobial stewardship as the archetypal de-implementation programme
Formulary restriction and pre-authorisation for targeted agents
Prospective audit of prescribing with direct feedback to the prescriber
Guideline-based order sets and decision support embedded in the record
Education on indication, duration and the local resistance pattern
Ongoing measurement of use, resistance and adverse events, fed back to the team
Complications & Pitfalls
The complications of low-value care are the harms described in the pathophysiology section made concrete: a false positive and its cascade, an overdiagnosed label and its surveillance, an adverse drug event from an unnecessary prescription, and the quiet opportunity cost of care not given. [5] [14] [16]
The pitfalls live in how we try to fix it. Ordering a test for reassurance that instead generates a cascade is the original mistake dressed as kindness. [14] Equating restraint with rationing, and so withholding high-value care, is the mirror-image error that turns a steward into a barrier. [8] Assuming a practice will fade on its own, without measurement or system change, ignores how entrenched habit and incentive are. [11]
Two pitfalls deserve special care. Blaming overuse solely on parent demand is both unfair and ineffective, because clinician habit and system incentives are usually the larger drivers and the ones a campaign can actually move. [9] [11] And de-implementing a practice without engaging families invites complaints and erodes the trust on which all stewardship depends. [13]
Prognosis & Disposition
The prognosis for a well-run de-implementation effort is good, provided it is measured. The marker of success is a sustained fall in the targeted low-value practice, with no compensatory rise in underuse of high-value care and no rise in adverse outcomes. [6] [8] A campaign that shows only a fall in the target, with no eye on underuse or harm, has not yet proven itself.
When to pause: if monitoring signals unintended underuse or harm, stop, re-engage stakeholders, and adjust the intervention before pushing on. [8] When to escalate: if a practice is entrenched by strong financial or cultural incentives, bring in leadership, consumers and governance so the change is owned by the system rather than imposed by a lone enthusiast. [13]
Disposition is documentation. Record the stewardship aim, the measured outcome, and the plan to sustain and re-audit, so that the gain outlives the individuals who made it. [6]
Special Populations
Neonates and infants are doubly exposed: the evidence base is thinner and more often extrapolated, and the youngest children are most vulnerable to overdiagnosis and drug harm, so a high threshold for testing and treatment is warranted. [4] [5] Children with medical complexity and technology dependence sit at the junction of overuse and underuse, and stewardship here must be aligned with the goals of care rather than applied uniformly. [8]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children carry a particular equity consideration: a stewardship drive must be co-designed with community and must not widen existing gaps in high-value care. [8] Migrant, refugee and asylum-seeking families may face language and health-literacy barriers that make restraint feel like denial unless it is carefully explained with interpreter support.
The equity argument runs in stewardship's favour for families in poverty. The out-of-pocket cost of low-value care — a needless scan, a needless prescription, a needless day off work — falls hardest on those with least, so reducing it is itself an act of distributive justice. [2] [8]
Evidence, Guidelines & Regional Differences
The evidence base for stewardship draws on three streams. The first defines the problem: Berwick and Hackbarth, and later Shrank and colleagues, estimate the large share of health spending that is waste, while Brownlee and colleagues document overuse of services worldwide. [2] [3] [7] The second explains the mechanism and the barrier: Coon and colleagues review paediatric overuse and overdiagnosis, and Cabana and colleagues show why clinicians fail to follow guidelines even when they know them. [4] [5] [11]
The third stream shows what works. Elshaug and colleagues set out the levers for addressing underuse and overuse, and Morgan and colleagues frame overuse through the patient-clinician interaction. [8] [9] Colla summarises the practical interventions, and Bhatia and colleagues provide the framework for measuring a campaign's effect. [13] [6] Two paediatric anchors round out the set: Quinonez and colleagues name five opportunities for improved value in paediatric hospital medicine, and Gerber and colleagues demonstrate that outpatient antimicrobial stewardship reduces broad-spectrum prescribing in a randomised trial. [15] [16]
Regional differences are mostly in framing, not principle. Choosing Wisely and its equivalents operate across ANZ, the United Kingdom and North America, and antimicrobial stewardship is a near-universal hospital requirement. [1] The candidate should cite the principle and name the jurisdiction, rather than quoting local cost figures or statutory wording.
Exam Pearls
In a viva, lead with the definition: value is benefit relative to harm and cost, and low-value care is not the same as cheap care. [8] Then name the mechanism of harm — the cascade, overdiagnosis, antimicrobial resistance and opportunity cost — before you reach for solutions. [5] [14]
Recite the de-implementation cycle as a clean sequence: identify, measure, diagnose drivers, engage, de-implement, sustain and monitor. [9] [13] Name audit and feedback with peer comparison as the best-evidenced single lever, and antimicrobial stewardship as the archetypal successful programme. [13] [16]
Above all, hold the ethical line. Stewardship is good medicine and justice, never rationing; the test of a good campaign is that high-value care is protected and the family trusts the restraint. [8]
References
- [1]Cassel CK, Guest JA Choosing wisely: helping physicians and patients make smart decisions about their care JAMA, 2012.PMID 22492759
- [2]Berwick DM, Hackbarth AD Eliminating waste in US health care JAMA, 2012.PMID 22419800
- [3]Shrank WH, Rogstad TL, Parekh N Waste in the US Health Care System: Estimated Costs and Potential for Savings JAMA, 2019.PMID 31589283
- [4]Coon ER, Young PC, Quinonez RA, et al. 2017 Update on Pediatric Medical Overuse: A Review JAMA pediatrics, 2018.PMID 29582079
- [5]Coon ER, Quinonez RA, Moyer VA, et al. Overdiagnosis: how our compulsion for diagnosis may be harming children Pediatrics, 2014.PMID 25287462
- [6]Bhatia RS, Levinson W, Shortt S, et al. Measuring the effect of Choosing Wisely: an integrated framework to assess campaign impact on low-value care BMJ quality & safety, 2015.PMID 26092165
- [7]Brownlee S, Chalkidou K, Doust J, et al. Evidence for overuse of medical services around the world Lancet, 2017.PMID 28077234
- [8]Elshaug AG, Rosenthal MB, Lavis JN, et al. Levers for addressing medical underuse and overuse: achieving high-value health care Lancet, 2017.PMID 28077228
- [9]Morgan DJ, Leppin AL, Smith CD, et al. A Practical Framework for Understanding and Reducing Medical Overuse: Conceptualizing Overuse Through the Patient-Clinician Interaction Journal of hospital medicine, 2017.PMID 28459906
- [10]Moynihan R, Doust J, Henry D Preventing overdiagnosis: how to stop harming the healthy BMJ, 2012.PMID 22645185
- [11]Cabana MD, Rand CS, Powe NR, et al. Why don't physicians follow clinical practice guidelines? A framework for improvement JAMA, 1999.PMID 10535437
- [12]Schwartz AL, Landon BE, Elshaug AG, et al. Measuring low-value care in Medicare JAMA internal medicine, 2014.PMID 24819824
- [13]Colla CH Swimming against the current--what might work to reduce low-value care? New England Journal of Medicine, 2014.PMID 25271601
- [14]Ganguli I, Lupo C, Mainor AJ, et al. Assessment of Prevalence and Cost of Care Cascades After Routine Testing During the Medicare Annual Wellness Visit JAMA network open, 2020.PMID 33306120
- [15]Quinonez RA, Garber MD, Schroeder AR, et al. Choosing wisely in pediatric hospital medicine: five opportunities for improved healthcare value Journal of hospital medicine, 2013.PMID 23955837
- [16]Gerber JS, Prasad PA, Fiks AG, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians: a randomized trial JAMA, 2013.PMID 23757082