Paeds · professional-practice-and-evidence
Paediatric consultation with child, young person and family
Also known as Paediatric medical interview · Child and family consultation · Triadic consultation paediatrics · Calgary-Cambridge paediatric consultation · Adolescent interview and HEEADSSS · Paediatric history taking and examination encounter · Communication skills in paediatrics
Fellowship-level approach to the paediatric consultation as a triadic, developmentally-adapted encounter: Calgary-Cambridge structure and the Paediatric Consultation Assessment Tool, age-adapted history and examination, eliciting the child's voice and parental agenda, adolescent confidentiality and HEEADSSS, breaking bad news with SPIKES, family-centred rounds, telehealth, safety-netting and documentation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child walks into the consulting room carrying more than a symptom. The parent carries the history, the timetable and the fear; the child carries the experience and, increasingly with age, the preference. The clinician carries a hypothesis that can be wrong. The paediatric consultation is the structured meeting of all three, and it does two jobs at once: it gathers information and it builds the relationship that lets a plan succeed. [1] [2]
Unlike the adult dyad, the paediatric interview is triadic. The roles shift across childhood. The infant and toddler are observed through play while the parent gives the history; the school-age child becomes a direct informant who can assent; the adolescent is a patient in their own right who needs confidentiality and time alone. Lose sight of the child and you have met the family but not the patient. [1] [10]
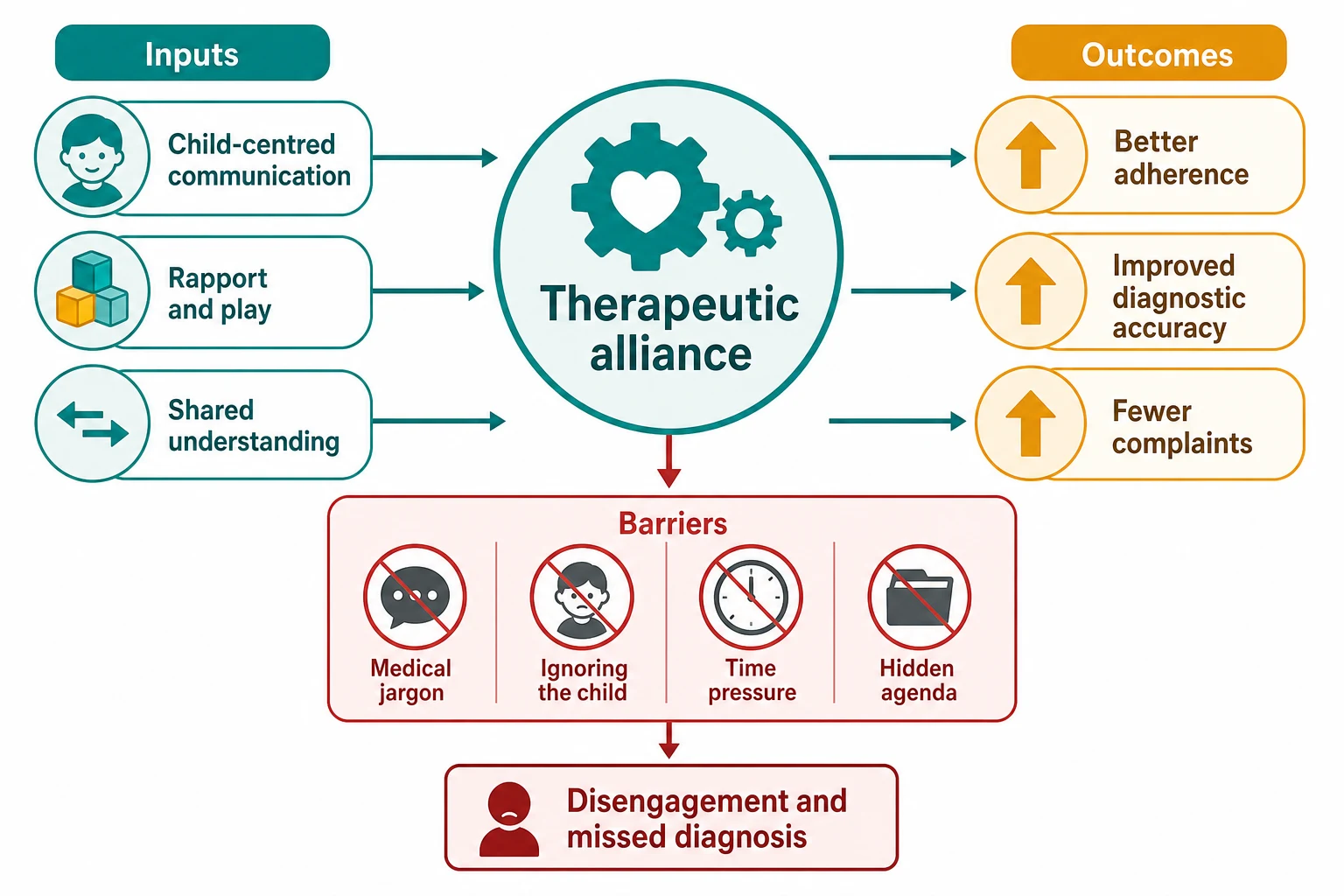
Done well, the consultation is therapeutic in itself. Patients who feel heard disclose more, recall more, adhere more and complain less. Done badly, it is the single most common source of parental complaint and diagnostic error in paediatrics — not a soft skill but a measurable safety intervention. [1] [2]
Classification
Frame the encounter with a structure you can defend in viva, then adapt it to the child in front of you. [2]
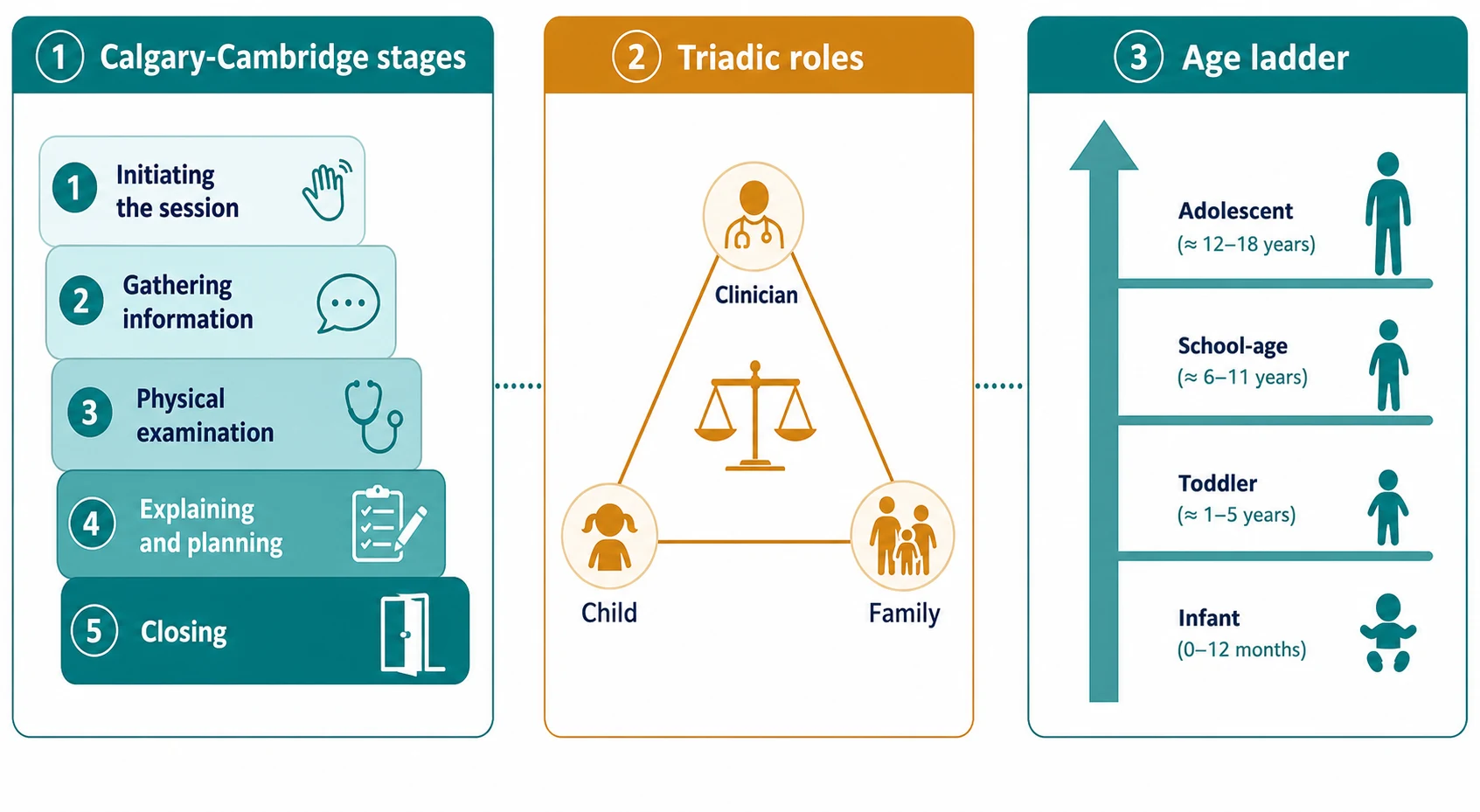
Calgary-Cambridge (adapted for children) is the workhorse framework: initiating the session, gathering information, physical examination, explaining and planning, and closing. The Paediatric Consultation Assessment Tool operationalises these stages for observation and feedback, and it is the framework examiners reach for when they judge a trainee's consultation. [2]
The triadic roles name who is doing what. The clinician guides; the parent is the historian and partner; the child is the patient, the informant and — as capacity grows — the participant. The balance of voice shifts along the age ladder from infant (parent-dominant) through school-age (shared) to adolescent (child-dominant, with parent informed). [1] [10]
Consultation styles and what they miss
HEEADSSS is the structured psychosocial screen for adolescents — home, education and employment, eating, activities, drugs, sexuality, suicide and depression, safety — and it anchors the adolescent private interview. [6]
Epidemiology & Risk Factors
Communication breakdown is not a footnote in paediatric safety; it is a leading driver of parental complaint, litigation and diagnostic error. The consultation is where most preventable harm either begins or is averted. [1] [2]
Several pressures conspire against a good encounter. Time is short, the symptom list is long, and the doctor's hypothesis closes the history early. The child is then talked about rather than talked to. Adolescents disengage the moment they sense no confidentiality and no time alone. Families facing language barriers, low health literacy, neurodiversity or parental distress leave the room understanding less than the clinician assumes. [1] [4]
The hidden agenda is the unspoken fear that drives the visit — a worry about cancer, development, or safety — and it surfaces only when rapport is built. Miss it, and you treat the symptom the parent mentioned while the real reason for coming goes unaddressed. [1] [2]
Pathophysiology
There is no enzyme for rapport, but there is a mechanism. Trust grows when information is honest and timely, and it collapses when a clinician dismisses a worry or hides behind jargon. The therapeutic alliance is the active ingredient: patients who feel heard disclose more, recall more and follow plans more reliably. [1] [2]
Development sets the substrate. Separation and stranger anxiety shape how an infant or toddler tolerates your approach; you examine through play, on a parent's lap, and you leave the threatening parts for last. Cognitive and language development govern how much a child can understand and report — a preschooler thinks concretely and magically, a school-age child wants explanation, an adolescent can reason about risk and confidentiality. [1] [6]
The triadic dynamic is its own physiology. A calm parent steadies a frightened child; an anxious parent transmits alarm. When the clinician partners with the parent rather than performing at them, the child reads the room as safe. Ignore this and even a correct diagnosis lands badly. [1] [10]
Clinical Presentation
You will often meet three stories in one room. The referral and the parental account name the presenting complaint. The child, once engaged, may describe something quite different — where it hurts, what they fear, what they want to avoid. Your own examination will add a fourth. A skilled consultation reconciles them rather than picking one. [1] [2]
Watch for the patterns that signal a consultation in trouble. The silent child who is never asked. The over-anxious parent who overwhelms the timeline. The adolescent who answers in monosyllables because no one guaranteed privacy. The mismatch between the stated concern and the child's behaviour. Each is a cue to slow down and re-engage, not to push on with the checklist. [1] [4]
Some presentations change the tempo of the whole encounter. A seriously ill child shifts you to a rapid, structured assessment. A safeguarding concern — a disclosure, an inconsistent injury story, a withdrawn child — moves you from history-taking to protection. Recognise these and adapt; a rigid script is dangerous. [1] [10]
Differential Diagnosis
When a consultation feels difficult, treat the difficulty itself as a clinical finding with a differential. [1]
| Surface story | Consultation reading | Must-not-miss alternative |
|---|---|---|
| Child won't cooperate | Developmentally normal shyness or stranger anxiety | Undisclosed pain, sensory difference, neurodiversity |
| Parent "rambles" | Health anxiety or hidden fear driving the visit | Genuine serious illness being downplayed |
| Adolescent monosyllabic | No confidentiality framing, no time alone | Depression, abuse, risk the screen will miss |
| Language confusion | Interpreter need or low health literacy | Safeguarding concern lost in translation |
| "Nothing wrong" referral | Tension between parental and clinician agendas | Maltreatment or behavioural change from stress |
Safeguarding is never cancelled by a polite consultation. If the story does not fit the child in front of you, ask, examine, document and escalate according to local child-protection procedure. [1] [10]
Clinical & Bedside Assessment
Open by setting the scene. Greet all three, introduce yourself, confirm consent, and explain what will happen. Then observe before you ask — the child's play, interactions, alertness, colour and work of breathing tell you most of the safety story before a single question. [1] [2]
Take a developmentally-appropriate history. Elicit the child's own words first where possible, then the parental account. Always capture the parental ideas, concerns and expectations — what the family thinks is wrong, what they fear, and what they hope to leave with. These are not soft data; they are the agenda the plan must meet. [1] [2]
The adolescent component is mandatory from puberty onward. Guarantee confidentiality and its limits, then offer time alone with the young person. Run the HEEADSSS psychosocial screen to surface home, education, eating, activities, substance use, sexuality, mood and safety risks that no parent-accompanied history will reveal. [6] [4]
Examine while you engage. Use distraction, play and a parent's lap; explain what you are doing in language the child can follow; and sequence from least to most invasive, leaving ears and throat until last. A child who has trusted you through the easy parts will let you do the hard ones. [1] [2]
The age-adapted consultation
Investigations
You cannot order a blood test for consultation quality. The instruments here are structured observation and documentation, not the laboratory. [2]
The Paediatric Consultation Assessment Tool and Calgary-Cambridge observation checklists let a supervisor score a trainee's consultation stage by stage — initiating, gathering, examination, explaining and planning, closing — and they are how communication skills are taught and measured. [2]
Document the child's reported words and the parental agenda verbatim, not only your own summary. In adolescents, a structured psychosocial tool such as HEEADSSS — increasingly delivered digitally, for example through composite screeners — turns the private interview into reliable, comparable data. [6]
Finally, use teach-back (closing the loop) as a diagnostic test of understanding: ask the family to tell you back the plan in their own words before you close. If they cannot, the explanation failed, not the listener. [1] [2]
Management — Resuscitation
When the child is seriously ill or acutely distressed, the consultation changes shape. Stabilise the child first. Build rapid rapport, control pain early, and name one calm spokesperson so the family hears a single, consistent voice. [1] [11]
De-escalate the frightened child with parental presence, comforting positioning, distraction and plain language. The goal is cooperation without restraint, because a traumatising encounter poisons every future visit. [1]
If a safeguarding concern emerges, the safety of the consultation is paramount. Do not interrogate; listen, document exactly, and follow local child-protection pathways. In any crisis, give honest information the same day and stop contradictory team advice before it reaches the family. [1] [10]
Management — Definitive & Stepwise
Use a repeatable sequence you can defend in viva and reproduce under pressure. [2]
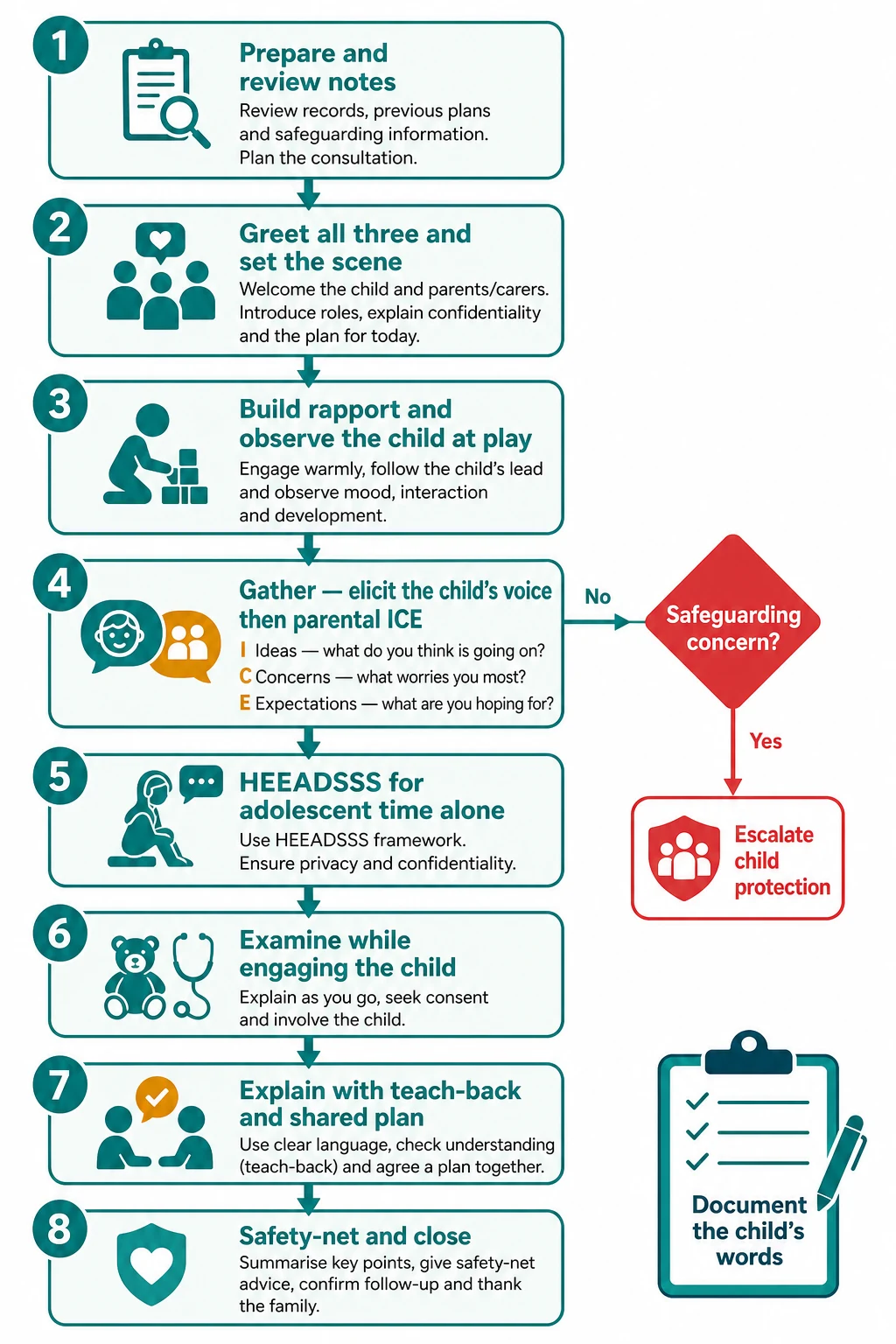
The structured paediatric consultation
Prepare: review the referral and notes, decide who must be present
Set the scene: greet all three, introduce, confirm consent and confidentiality
Build rapport and observe the child at play before any question or examination
Gather: elicit the child's voice, then the parental ideas, concerns and expectations
Adolescent: guarantee confidentiality, offer time alone, run HEEADSSS
Examine while engaging the child — least invasive to most invasive, last
Explain findings and a shared plan in plain language with teach-back
Safety-net explicitly and close: what to watch for, when, where to return
Breaking bad news uses SPIKES — setting, perception, invitation, knowledge, emotions, strategy and summary. Adapt it to the child's developmental level: tell the truth, in words they can hold, and keep the dialogue open rather than delivering a single devastating sentence. Palliative and serious-illness consultations extend this into ongoing, family-centred planning. [3] [11]
Family-centred ward rounds and the medical home carry the consultation into systems. Structured rounds that engage nurse and family in plain language improve understanding and safety climate, and the medical home coordinates care for children with complex needs around the family rather than around clinic silos. [10]
Specific Subtypes & Scenarios
Infant and toddler. The parent is the primary historian. Examine on a lap and through play, watch attachment and tone, and manage stranger anxiety with short, concrete reassurance and a toy to hand. [1]
School-age child. Question the child directly at their level, seek assent, and explain what you will do before you do it. Drawing and telling can surface worries a verbal history misses. [1] [2]
Adolescent. Frame confidentiality and its limits, offer time alone, and run HEEADSSS. Respect emerging autonomy and capacity; a participatory style raises visit satisfaction and engagement, and pre-visit prompts can increase the young person's question-asking. [4] [6] [8] [9]
Breaking bad news. Adapt SPIKES to the family and the child's developmental stage. Truth-telling builds trust; deception erodes it permanently. Palliative-care consultation extends this into goals, symptoms and advance planning. [3] [11]
Telehealth and remote consultation. Rapport is harder and examination is mediated through the parent as co-examiner. Be explicit about what you can and cannot assess remotely, and have a low threshold to bring the child in. [1]
Complications & Pitfalls
- Talking only to the parents and treating the child as scenery. [1]
- Closing the history before the hidden agenda and the parental ICE are exposed. [2]
- Using jargon and never checking understanding with teach-back. [1]
- Building rapport too late, so a frightened child refuses the examination. [1] [2]
- Breaching adolescent confidentiality without a clear, explained threshold of risk. [4]
- Failing to safety-net or to document the plan, the safety-net and the child's words. [1]
- Overlooking a safeguarding concern beneath a routine symptom. [1] [10]
Prognosis & Disposition
A well-structured consultation is not just pleasant; it changes outcomes. Patients and families who feel heard disclose more, recall the plan more accurately, adhere better and complain less. Structured consultation-skills teaching and feedback measurably improve performance. [1] [2]
Disposition is never "see GP". Name the key contact, write the plan in plain language, give an explicit safety-net, and schedule review. When the consultation reveals serious illness or a safeguarding risk, escalate, refer, and ensure a safe handover rather than an open-ended reassurance. [1] [10]
Special Populations
Adolescents. Confidentiality, time alone, HEEADSSS and respect for emerging autonomy are the non-negotiables. Minor-consent provisions in many jurisdictions let young people consent to specific care independently, which changes how you frame the encounter. [4] [6]
Children with disability, neurodiversity or who are non-verbal. Adapt communication to the child, use augmentative tools, and treat trusted caregivers and support people as essential informants without letting them silence the child. [1]
Culturally and linguistically diverse families. Use trained interpreters and cultural humility. Never press a child into service as the family interpreter, and check understanding explicitly. [5]
Out-of-home-care, refugee and youth-justice populations. Clarify who holds consent, take a trauma-informed approach, and do not assume prior services have done your partnership work for you. [5] [10]
Evidence, Guidelines & Regional Differences
Landmark anchors for this topic: the AAP policy on communicating with children and families from everyday interaction to distressing information; the Calgary-Cambridge framework and the Paediatric Consultation Assessment Tool for structured, observable consultation skills; the SPIKES protocol for delivering bad news, adapted from adult oncology into paediatrics; the evidence on adolescent minor consent and confidentiality; and trials of interventions that raise youth engagement and question-asking in clinic. [1] [2] [3] [4] [7] [8] [9]
Controversies you must handle calmly: how much time alone an adolescent should have and whether the parent stays; the limits of confidentiality when risk is disclosed; whether a telehealth consultation can substitute for in-person assessment; and how honestly to tell a seriously ill child the truth without cruelty. Each is a judgement under rights and evidence, not a rule to recite. [1] [6]
RACP and the Bright Futures-influenced health-supervision model frame the consultation around family partnership and developmental surveillance. Confidentiality and minor-consent provisions operate within state law; HEEADSSS is a standard part of adolescent care, increasingly delivered through digital screeners. [4] [6]
Exam Pearls
PATIENTS
References
- [1]Levetown M and American Academy of Pediatrics Committee on Bioethics Communicating with children and families: from everyday interactions to skill in conveying distressing information. Pediatrics, 2008.PMID 18450887
- [2]Howells RJ, Davies HA, Silverman JD, Archer JC, Mellon AF Assessment of doctors' consultation skills in the paediatric setting: the Paediatric Consultation Assessment Tool. Archives of disease in childhood, 2010.PMID 19019880
- [3]Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. The oncologist, 2000.PMID 10964998
- [4]Ford CA, Skiles MP, English A, Cai J, Agans RP, Stokley S, Markowitz L, Koumans EH Minor consent and delivery of adolescent vaccines. The Journal of adolescent health, 2014.PMID 24074605
- [5]Waterston T, Yilmaz G Child Rights and Health Care: International Society for Social Pediatrics and Child Health (ISSOP) Position Statement. Child: care, health and development, 2014.PMID 24588351
- [6]Ho J, Fong CK, Iskander A, Towns S, Steinbeck K Digital psychosocial assessment: An efficient and effective screening tool. Journal of paediatrics and child health, 2020.PMID 31883286
- [7]Coyne I, Sleath B, Surdey J, Pembroke S, Hilliard C, Chechalk K, Rafferty S, Rogerson S, Hughes MM, Murphy M, Cody D, Roche E Intervention to promote adolescents' communication and engagement in diabetes clinic encounters: A pilot randomized controlled trial. Patient education and counseling, 2024.PMID 38772095
- [8]Sleath B, Beznos B, Carpenter D, Thomas K, Annis I, Tudor G, Garcia N, Adjei A, Anastopoulos A, Leslie L, Coyne I A pre-visit video/question prompt list intervention to increase youth question-asking about attention deficit hyperactivity disorder during pediatric visits. Patient education and counseling, 2024.PMID 38851012
- [9]Sleath B, Thomas KC, Carpenter DM, Annis IE, Tudor G, Coyne I, Garcia N, Adjei AA, Leslie LK Provider use of a participatory decision-making style with youth with ADHD and their caregivers and visit satisfaction. Patient education and counseling, 2025.PMID 40020479
- [10]COMMITTEE ON HOSPITAL CARE and INSTITUTE FOR PATIENT- AND FAMILY-CENTERED CARE Patient- and family-centered care and the pediatrician's role. Pediatrics, 2012.PMID 22291118
- [11]Moore D, Sheetz J Pediatric palliative care consultation. Pediatric clinics of North America, 2014.PMID 25084721