Paeds · professional-practice-and-evidence
Shared decision-making and assent in children
Also known as Shared decision making paediatrics · Child assent to treatment · Paediatric assent and dissent · Preference-sensitive decisions in children · Decision aids for parents · Three talk model paediatrics · Supported decision making child
Fellowship-level approach to shared decision-making (SDM) and assent in children: three-talk model, consent versus assent and dissent, AAP seven assent elements, decision aids, child participation, pitfalls and regional frameworks.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent brings you a decision, not just a child. Should we start the stimulant? Should we do the scan? Do we switch to the biologic? Each of these is a fork in the road where evidence, fear, family circumstance and the child's own view must meet. Shared decision-making is the deliberate process of bringing those things together so that the choice fits the person in front of you. [4]
The trap in paediatrics is that you can run a perfectly warm conversation with the parents and forget that there is a small person in the room whose body this is. That child usually cannot give legally binding consent, but they can give assent — a developmentally appropriate affirmative agreement — and they can refuse. The American Academy of Pediatrics Committee on Bioethics frames assent and parental permission as two distinct goods that should both be sought when the child can take part. [1] [2]
In practice the job is to name the decision, share the options honestly, elicit what the family and child actually care about, and land on a choice you write down and revisit. SDM is clinical skill, and like any skill it has a structure you can defend in an exam. [4] [3]
Classification
Sort the concepts first, then sort the decisions. [1]
Three concepts. Consent gives permission and protects from battery; it is given by whoever holds legal authority. Assent respects the developing autonomy of the child who is not yet a legal decision-maker; it has seven elements the AAP asks you to cover. Shared decision-making is the deliberative partnership that should sit underneath both. [1] [3]
Three decision types. Effective decisions are ones where one option is clearly best — give the antibiotics for meningitis, splint the fracture. These need informed consent, not a long deliberation. Preference-sensitive decisions are ones where reasonable people choose differently — stimulant versus behavioural therapy, scan versus watch. These are the natural home of SDM. Emergency decisions are time-critical and proceed under implied consent; you seek assent after the child is stable. [4]
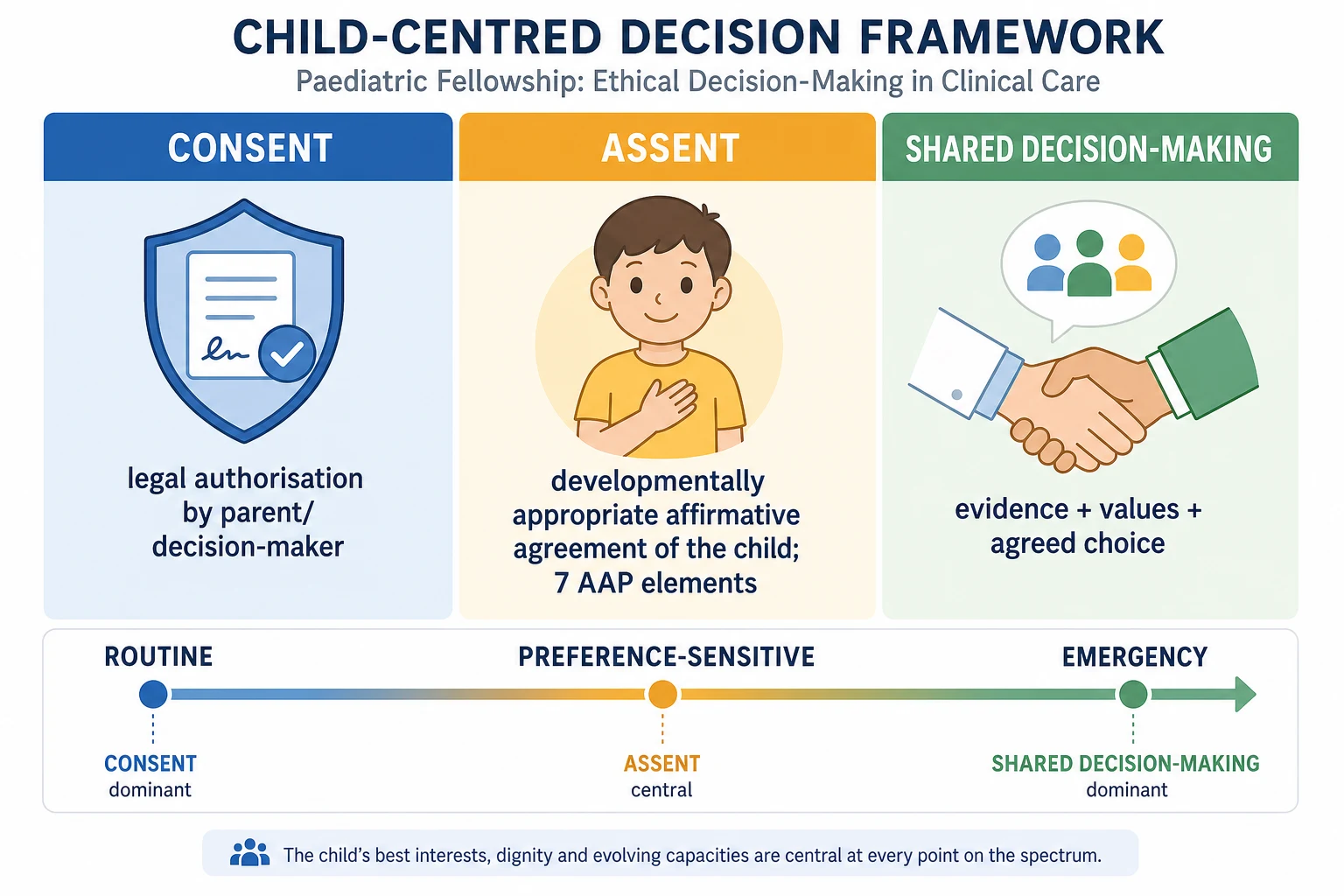
The AAP seven elements of assent. Help the child understand the purpose of the intervention; what they will experience; the main benefits and risks; the reasonable alternatives; that they may refuse; that they may ask questions at any time; and that their agreement is voluntary. You do not read these like a checklist at a five-year-old — you translate them into age-appropriate language and watch for the child's cue. [1] [2]
| Aspect | Consent | Assent | Shared decision-making |
|---|---|---|---|
| Who | Parent or mature minor (legal authority) | Child not yet able to consent | Clinician + parent + child together |
| Function | Authorises treatment; protects autonomy | Respects developing autonomy | Reaches a values-concordant choice |
| Format | Documented legal/ethical agreement | Developmentally appropriate dialogue | Three-talk structured conversation |
| Refusal | Valid refusal usually binds | Dissent is weighed, not absolute | Disagreement triggers ethics/review |
Epidemiology & Risk Factors
SDM is talked about more than it is practised. A systematic review and meta-analysis of paediatric SDM found that interventions improved parents' knowledge but had only modest effects on the actual decisions reached and on child involvement. The gap between knowing the options and sharing the power is real. [4]
Risk factors for a poor SDM encounter cluster around three things: the child, the clinician and the system. Younger children are asked less; sicker children are talked about more than talked with. Clinicians cite time pressure, uncertainty and fear of damaging the relationship as barriers, especially in chronic disease where decisions repeat. Systems reward throughput, not deliberation, so the families who lose out are the ones with language barriers, low health literacy and competing survival pressures. [5] [12]
Parents carry decisional conflict and, later, decision regret on the hard choices — biologics with serious side-effect profiles, surgery, and acute imaging decisions. These are exactly the preference-sensitive moments where a structured conversation earns its keep. [5] [11]
Pathophysiology
There is no enzyme for a good decision, but there is a mechanism. SDM works through information exchange, explicit deliberation, comparison of options and alignment with values. When those steps happen, decisional conflict falls and the choice fits the family. When they are skipped, you get regret, hidden non-adherence and a child who stops trusting the team. [4] [5]
Assent works through respect. The United Nations Convention on the Rights of the Child treats the right to be heard as weighty, scaled to evolving capacity. A child who is invited into a decision — even one they cannot legally make — learns that their body and their voice matter, and that is protective for every future encounter. Token assent, by contrast, is corrosive: if the child works out the agreement was theatre, trust does not recover quickly. [1] [10]
Decision aids are tools, not the whole process. They reduce decisional conflict by structuring information about options, benefits, harms and uncertainties — but only when the clinician still does the values work. A decision aid shown without anyone asking what the family cares about is just a fancier information dump. [4] [9]
Clinical Presentation
You will recognise an SDM opportunity by listening for a fork. A parent says "what would you do, doctor?" on a question where reasonable clinicians genuinely differ. An adolescent says "nobody asked me" about a treatment that reshapes their daily life. A family is handed a single path as if there were no other, then asked to sign. [4] [12]
The high-yield presentations are the preference-sensitive ones: starting an ADHD medication, choosing observation over imaging after a minor head injury, weighing a biologic against its side-effect burden, deciding on surgery for a chronic condition, and any life-limiting-illness choice. Each is a place where the decision belongs to the family once they understand the options. [7] [9] [5]
Differential Diagnosis
When a decision feels stuck or a family seems "non-compliant," diagnose the obstacle before pushing harder. [4] [12]
| Surface story | Real obstacle | What to do |
|---|---|---|
| "They won't decide" | Decisional conflict, not apathy | Add structure: options, values, a decision aid |
| "Child won't engage" | Fear, development, or genuine dissent | Assess capacity; respect dissent if non-emergency |
| "They refused everything" | Values gap or trust gap, not stubbornness | Revisit values; offer time and a second opinion |
| "There's only one option" | Clinician has collapsed the choice | Re-list reasonable alternatives honestly |
| "Adolescent wants control" | Evolving autonomy, not defiance | Capacity assessment; supported decision-making |
Safeguarding can masquerade as a "choice" the child is being pushed into or out of. If the decision smells of coercion or the child's safety is at stake, your obligation to protect overrides the partnership frame — but partnership is how you deliver the protection, not an alternative to it. [1] [3]
Clinical & Bedside Assessment
Diagnose the decision before you diagnose the child. Is this preference-sensitive? Who is the legal decision-maker? What is the time frame? Those three questions stop you from running a thirty-minute conversation in a resuscitation, and from skipping one in a clinic where it matters. [4]
Then assess the participants. How old and how capable is the child of understanding the options? What role does the parent want — collaborative, clinician-led, or family-led? What is the family's health literacy and language need? These shape how you deliver the same content. [1] [12]
Minimum SDM and assent assessment: [1] [4]
- Identify the decision and whether it is preference-sensitive or effective. [4]
- Assess the child's developmental capacity to assent and their preferred role. [1] [10]
- Elicit values and what matters most before presenting options. [4] [11]
- Check understanding with teach-back of the options, not just the plan. [3]
- Screen for decisional conflict when the choice is hard. [11]
Record what the child said, not only what the adults decided. [10]
Investigations
You do not order a blood test for shared decision-making. The "investigations" here are structured tools and documentation that make the conversation visible and repeatable. [4] [9]
- Decision aids for specific preference-sensitive choices (head CT after minor head injury, ADHD treatment) when a validated instrument exists. [9] [7]
- Decisional conflict scale (Ottawa) to quantify difficulty and flag a family that needs more support. [11]
- Capacity assessment using the mature-minor standard when an adolescent wants to consent to or refuse a non-emergency treatment independently. [1] [2]
- Documentation of the options discussed, the values elicited, the child's assent or dissent, and the agreed choice with a review date. [1] [10]
Management — Resuscitation
In the emergency or resuscitation setting, life-saving treatment proceeds under implied consent. You do not pause a time-critical intervention to run a deliberative SDM conversation, and you do not demand assent before an emergency procedure from a child who cannot give it. [1] [3]
What you do is explain afterwards, at a developmentally appropriate level, what happened and why, and seek assent for the next steps once the child is stable. Parents are told the options for any genuine fork even in an emergency — for example a procedural approach with a real alternative — but in a compressed, honest form. [3] [1]
Management — Definitive & Stepwise
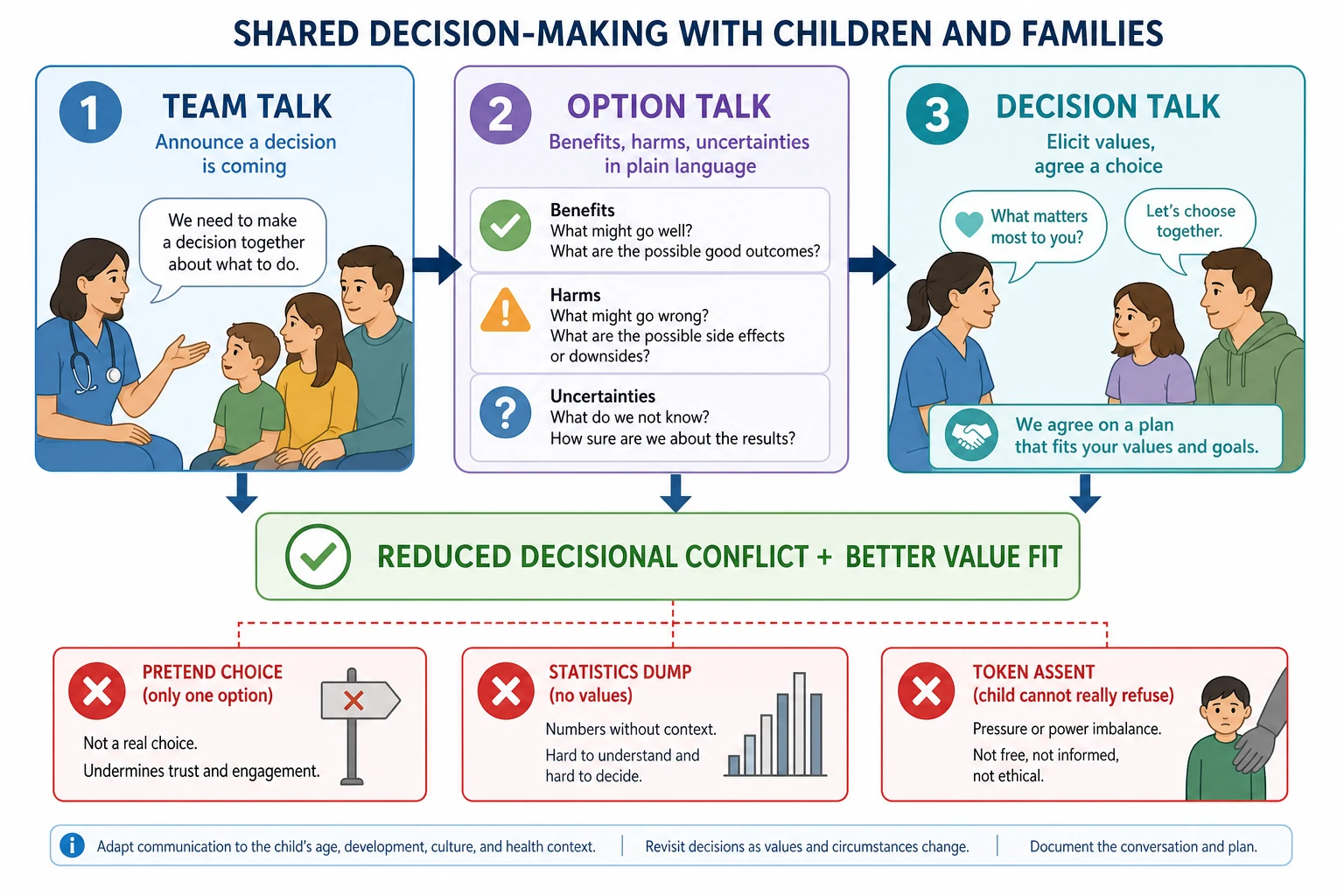
Use a structure you can recite under viva pressure. The three-talk model is the cleanest scaffold: team talk, option talk, decision talk, with assent threaded through. [4]
SDM and assent algorithm
Diagnose the decision: preference-sensitive? who decides? time frame?
Assess capacity: child's developmental ability to assent; parental style and health literacy
Team talk: announce a decision is coming and offer a partnership role
Option talk: present reasonable options with benefits, harms and uncertainties in plain language
Seek assent: invite and record the child's view, including dissent
Decision talk: elicit values, check understanding, agree a choice
Document and review: written plan, follow-up date, revisit at milestones and transition
Use a decision aid where one exists. For well-appearing children with minor head trauma, the head CT choice decision aid was tested in a cluster-randomised trial and reduced CT use without an increase in missed injuries; it also reached potentially vulnerable parents. That is the kind of evidence an examiner wants to hear, not a vague "decision aids help." [9] [11]
Tailor to the scenario. In ADHD care, shared decision-making tools improve engagement and parental knowledge, and they make the choice between stimulant, non-stimulant and behavioural options explicit rather than defaulted. [7] [8] In chronic disease, physicians name time, uncertainty and relationship-protection as the main barriers; planning around those barriers is the management. [5] In oncology and cystic fibrosis, the evidence base on how best to promote the child's own participation is still thin — a Cochrane review found few studies — so you default to good three-talk practice and document it. [6]
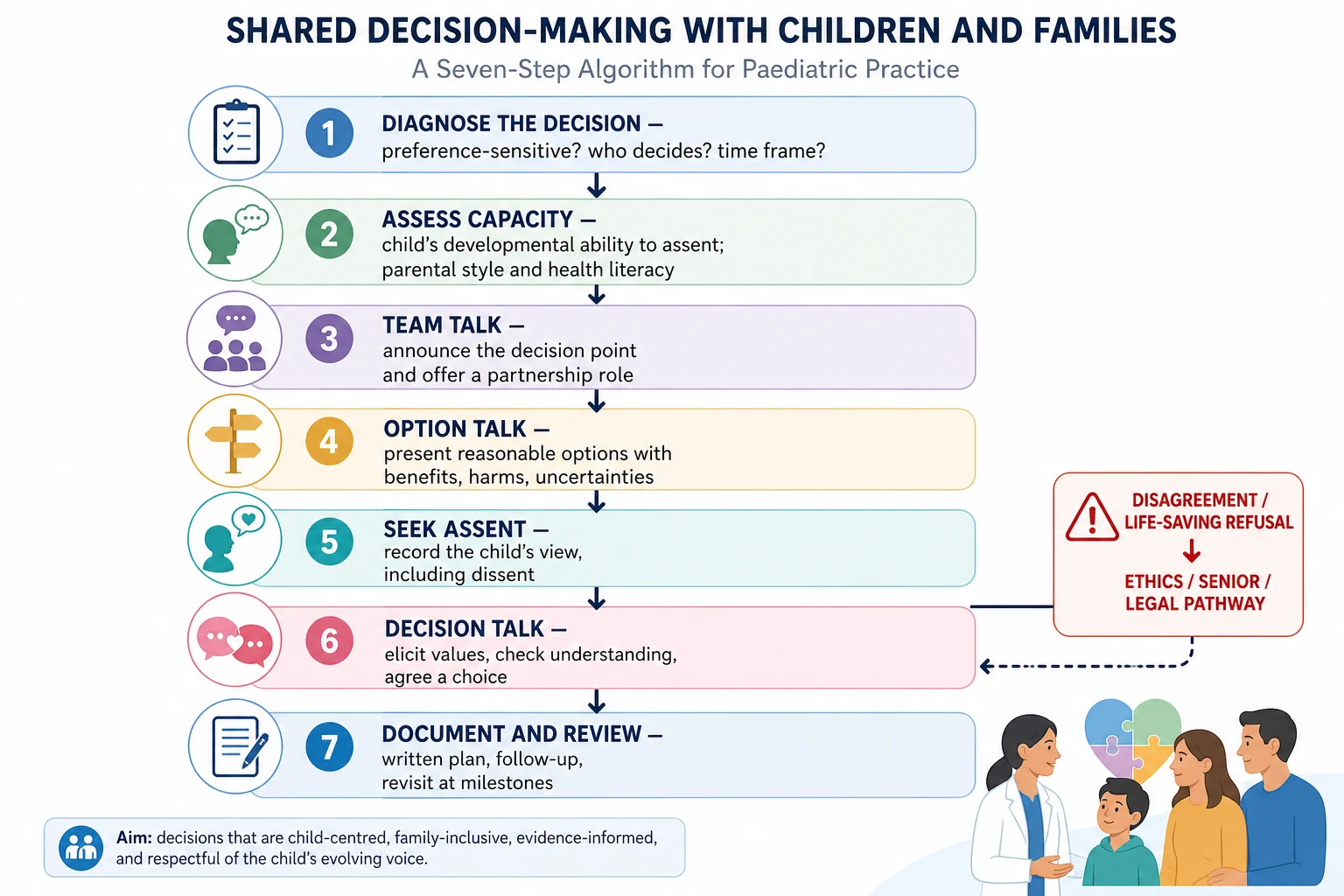
Best-interests and disagreement. When parents disagree with each other, with the adolescent, or with the team on a preference-sensitive choice, return to values and options before escalation. If the disagreement is irreconcilable or a life-saving treatment is refused, escalate to clinical ethics, a second opinion and the local legal pathway. Best interests is a structured weighing of the child's welfare, not a slogan to end the conversation. [1] [2]
Specific Subtypes & Scenarios
ADHD treatment choice. After a multi-informant assessment confirms the diagnosis, the stimulant-versus-behavioural-versus-combined choice is preference-sensitive. SDM tools help parents and children weigh side effects, school timing and family routines rather than default to the first option offered. [7] [8]
Minor head injury imaging. For well-appearing children, the head CT choice decision aid supports parents to choose observation over imaging, reducing radiation without missing clinically important injuries. It is a model of a decision aid that genuinely shifts practice. [9] [11]
Chronic disease biologics and surgery. Repeated high-stakes choices over years favour a longitudinal SDM approach: revisit the decision as the disease and the child's capacity change, and keep the adolescent central as transition approaches. [5] [12]
Oncology and cystic fibrosis. These children live inside repeated decisions; promote their participation at a level matched to capacity, and accept that the evidence on the best way to do that is still developing. [6]
Adolescents and transition. As capacity matures, move from assent toward supported autonomous decision-making. Confidential adolescent time and a mature-minor assessment sit naturally alongside SDM, not in competition with it. [1] [2]
Procedures. Seek assent from the able child, explain what they will feel, and build comfort hold, distraction and topical anaesthesia into the plan so cooperation is genuine rather than forced. [3] [1]
Complications & Pitfalls
- Token or coerced assent the child cannot meaningfully refuse. [1] [10]
- Presenting a single option as a "shared decision" — pretend choice. [4]
- Equating assent with consent and ignoring the legal decision-maker. [1]
- Overwhelming families with statistics without ever eliciting values. [5] [11]
- Ignoring adolescent dissent on a non-emergency, preference-sensitive choice. [1]
- Failing to revisit a chronic-disease decision as capacity and disease evolve. [5]
- Confusing a decision aid with the SDM conversation itself. [9]
Prognosis & Disposition
Good SDM reliably improves parents' knowledge and reduces decisional conflict; its effect on hard clinical outcomes is more modest because it is designed to fit values, not to change physiology. The honest framing for an examiner is that SDM is about decision quality and trust, not a mortality benefit. [4] [11]
Authentic child participation builds engagement with care that pays off across future encounters, especially in chronic disease and transition. [10] [12]
Disposition is a documented decision: the options discussed, the values that drove the choice, the child's assent or dissent, the agreed plan in plain language, and a named review date. Escalate to clinical ethics, a second opinion or the legal pathway when disagreement cannot be resolved or life-saving treatment is refused. [1] [4]
Special Populations
Pre-verbal infants and toddlers. Parents act as surrogates; assent is not possible, so watch distress signals and prioritise comfort. Surrogate decisions should track what the family believes is best for this child. [1] [3]
School-age children. Give concrete, age-appropriate assent for procedures and treatments; the seven AAP elements translated into language the child can use. [1]
Adolescents. Assess capacity for the specific decision; offer confidential time; support movement toward autonomous choice and transition planning. [1] [2]
Children with intellectual or developmental disability. Use supported decision-making adapted to capacity, and never assume incapacity from diagnosis alone. [1] [10]
Families with language barriers or low health literacy. Use professional interpreters, plain language and teach-back; SDM that only reaches articulate, English-fluent families widens inequity rather than closing it. [12] [3]
Evidence, Guidelines & Regional Differences
Practice anchors: the AAP Committee on Bioethics framework on informed consent and assent; Levetown's communication guidance; the Wyatt systematic review and meta-analysis of paediatric SDM; the Coyne Cochrane review on children's participation in cancer decisions; the Hess head CT choice cluster-randomised trial and its vulnerable-parents follow-up; and the Brinkman and Lipstein programmes of work on ADHD and chronic-disease SDM. [1] [3] [4] [5] [6] [9]
Controversies to handle calmly: how much weight to give a child's dissent when the family wants to proceed; how far decision aids generalise beyond the setting they were built in; whether SDM widens or closes equity gaps depending on who receives it; and how to practise SDM under genuine time pressure without reducing it to a checkbox. [5] [11]
In Australia and Aotearoa New Zealand, capacity is decision-specific and the mature-minor principle allows a competent young person to consent independently; local statute and hospital policy govern operational thresholds. Use children's healthcare charters and rights frameworks to ground the child's voice alongside parental authority. [1]
Exam Pearls
OPTIONS
References
- [1]COMMITTEE ON BIOETHICS Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456514
- [2]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [3]Levetown M, American Academy of Pediatrics Committee on Bioethics Communicating with children and families: from everyday interactions to skill in conveying distressing information. Pediatrics, 2008.PMID 18450887
- [4]Wyatt KD, List B, Brinkman WB, Prutsky Lopez G, Asi N, Erwin P, Wang Z, Domecq Garces JP, Montori VM, LeBlanc A Shared Decision Making in Pediatrics: A Systematic Review and Meta-analysis. Academic pediatrics, 2015.PMID 25983006
- [5]Dodds CM, Britto MT, Denson LA, Lovell DJ, Saeed S, Lipstein EA Physicians' Perceptions of Shared Decision Making in Chronic Disease and Its Barriers and Facilitators. The Journal of pediatrics, 2016.PMID 26817588
- [6]Coyne I, O'Mathuna DP, Gibson F, Shields L, Leclercq E Interventions for promoting participation in shared decision-making for children with cancer. Cochrane Database of Systematic Reviews, 2016.PMID 27898175
- [7]Brinkman WB, Hartl Majcher J, Poling LM, Shi G, Zender M Shared decision-making to improve attention-deficit hyperactivity disorder care. Patient education and counseling, 2013.PMID 23669153
- [8]Brinkman WB, Hartl J, Rawe LM, Sucharew H, Britto MT Physicians' shared decision-making behaviors in attention-deficit/hyperactivity disorder care. Archives of pediatrics & adolescent medicine, 2011.PMID 22065181
- [9]Hess EP, Homme JL, Kharbanda AB, Tzimenatos L Effect of the Head Computed Tomography Choice Decision Aid in Parents of Children With Minor Head Trauma: A Cluster Randomized Trial. JAMA network open, 2018.PMID 30646167
- [10]Quaye AA, Coyne I, Soderback M, Hallstrom IK Children's active participation in decision-making processes during hospitalisation: An observational study. Journal of clinical nursing, 2019.PMID 31430412
- [11]Skains RM, Kuppermann N, Homme JL, Kharbanda AB What is the effect of a decision aid in potentially vulnerable parents? Insights from the head CT choice randomized trial. Health expectations, 2020.PMID 31758633
- [12]Giambra BK, Haas SM, Britto MT, Lipstein EA Exploration of Parent-Provider Communication During Clinic Visits for Children With Chronic Conditions. Journal of pediatric health care, 2018.PMID 28866436