Paeds · respiratory-sleep-and-airway
Behavioural insomnia and circadian rhythm disorders
Also known as Behavioural insomnia of childhood · Bedtime problems and night wakings · Delayed sleep phase syndrome · Delayed sleep-wake phase disorder · Circadian rhythm sleep-wake disorders in children
Fellowship guide to behavioural insomnia of childhood and the circadian rhythm sleep-wake disorders: the sleep-onset association and limit-setting subtypes and their diagnosis on a picture of difficulty sleeping despite adequate sleep opportunity, the two-process and melatonin physiology behind the adolescent phase delay, the sleep history, diary and actigraphy, behavioural treatment as first-line, timed morning bright light and correctly timed low-dose evening melatonin for delayed sleep-wake phase disorder, the special place of melatonin in neurodevelopmental disability, and the families and populations that change the plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Two very different families sit at the exhausted end of most sleep referrals, and the examiner wants them separated at once. The toddler who cannot fall asleep without being rocked, and wakes the household four times a night, has behavioural insomnia of childhood: a learned problem of settling and staying asleep. The teenager who lies awake until two in the morning and cannot be roused for school has a circadian rhythm disorder: a body clock set to the wrong time. [1] [8]
The unifying definition of behavioural insomnia of childhood is difficulty initiating or maintaining sleep that arises from behaviour and learning, occurs despite an adequate opportunity to sleep, and produces daytime consequences for the child or the family. The circadian rhythm sleep-wake disorders, by contrast, are a persistent mismatch between the internal clock and the schedule the child needs to keep. Both are common, both are treatable, and both are frequently mismanaged with a hypnotic instead of the right behavioural or circadian plan. [1] [8]
Classification
The practical split that an examiner expects first is between a learned insomnia and a mistimed clock, because the two are treated in opposite ways. Behavioural insomnia of childhood is the learned group, and it has two named subtypes that describe how the child fails to sleep. Sleep-onset association type is the child who has learned to fall asleep only under certain conditions — rocked, fed, or with a parent present — and who therefore needs those same conditions restored at every normal night waking. [1] [2]
Limit-setting type is the other pattern, seen more in the preschooler than the infant. Here the child resists bedtime, stalls, and produces a stream of requests — the "curtain calls" — that persist when a caregiver does not set or hold consistent limits. Many children show a combined picture with features of both, and naming the subtype matters because it points directly at the behavioural technique that will work. [1] [2]
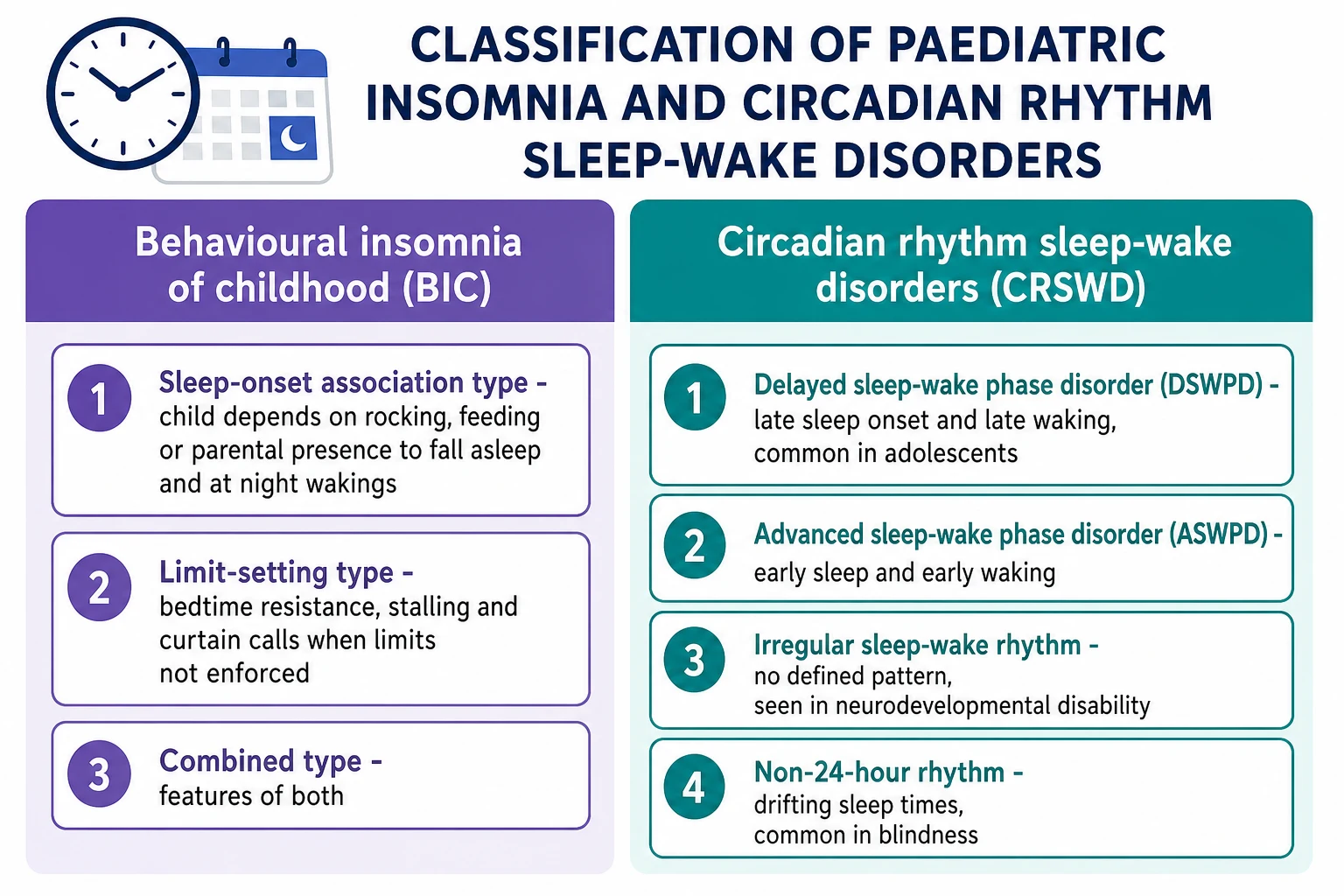
The circadian rhythm sleep-wake disorders form the second family, defined by when sleep happens rather than by settling behaviour. Delayed sleep-wake phase disorder is the adolescent who sleeps and wakes hours later than required and cannot shift; advanced sleep-wake phase disorder is the mirror image of early sleep and early waking; irregular sleep-wake rhythm has no consolidated pattern and is seen in neurodevelopmental disability; and non-24-hour rhythm, in which sleep drifts progressively later, is classically a problem of the blind child. [8] [10]
Epidemiology & Risk Factors
Bedtime problems and night wakings are among the commonest concerns raised by parents of young children, reported in roughly a fifth to a third of infants and toddlers depending on how they are defined. Their frequency is one reason the topic is so heavily examined: this is everyday general paediatrics rather than a rarity, and confident behavioural advice is expected of any candidate. [1] [3]
The behavioural insomnias cluster around how sleep has been taught. Inconsistent routines, a parent who lies down with the child until sleep comes, reactive co-sleeping introduced to end a battle, and a temperamentally difficult child all raise the risk. None of these are moral failings; they are learned patterns, which is exactly why they respond to relearning rather than to medication. [1] [2]
Delayed sleep-wake phase disorder rises sharply through adolescence and is the most common circadian disorder of the teenage years. The risk is driven by the biology of puberty, which delays the internal clock, and then amplified by modern life: bright evening light and screens, caffeine, weekend sleep-ins that push the clock later, and academic and social demands that erode the morning. Comorbid anxiety, depression, ADHD and autism all add risk, and the blind child is specifically prone to a non-24-hour rhythm. [9] [10]
Pathophysiology
Sleep timing is governed by two systems working together, and holding this "two-process model" in mind explains almost every treatment in the topic. Process S is the homeostatic sleep pressure that builds the longer a child is awake and discharges during sleep. Process C is the circadian alerting signal generated by the suprachiasmatic nucleus of the hypothalamus, which promotes wakefulness during the day and permits sleep at night. Sleep comes easily when high sleep pressure meets a falling circadian alerting signal. [9] [10]
The circadian clock is set to the outside world chiefly by light. Retinal light exposure signals the suprachiasmatic nucleus, which in turn controls the pineal secretion of melatonin — the hormone that rises in the evening to signal biological night. The onset of melatonin secretion under dim light, the dim light melatonin onset, is the best marker of a person's internal clock time and is the reference point for timing treatment. [8] [10]
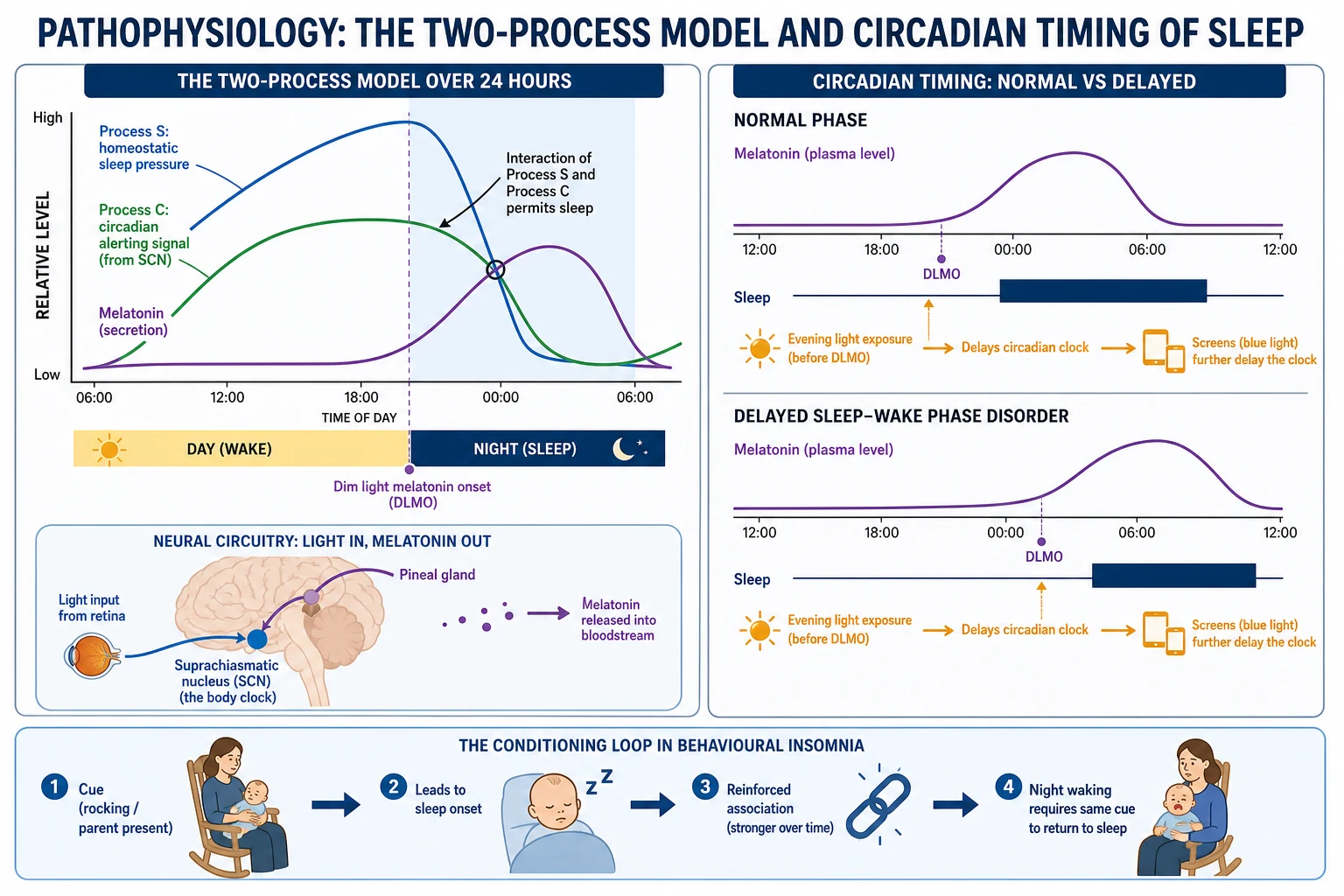
Adolescent delay is best understood as a "perfect storm". The pubertal clock naturally shifts later, homeostatic sleep pressure builds more slowly so the teenager is not sleepy at the old bedtime, and the environment — light, screens, late social life and early school starts — pushes the same way. The result is a stable, biologically driven late phase rather than wilful lateness. Behavioural insomnia has a different mechanism: a cue such as rocking becomes conditioned to sleep onset, so the child cannot bridge normal night arousals without it and signals for the caregiver instead. [9] [10]
Clinical Presentation
The behavioural insomnia story is told by the exhausted parent. In sleep-onset association type the complaint is repeated night wakings: the infant settles only when rocked or fed and then signals loudly at each normal arousal until that condition is restored. In limit-setting type the complaint is the bedtime battle: prolonged resistance, stalling, repeated requests for water or stories, and settling only when an adult finally stays or gives in. The child usually sleeps well once asleep, and daytime problems are irritability and behavioural difficulty. [1] [2]
Delayed sleep-wake phase disorder presents very differently, and its hallmark is the discrepancy between school days and free days. The adolescent cannot fall asleep until the early hours despite trying, then cannot wake for school and is profoundly sleepy in the morning. Given the chance — at weekends or in holidays — the same young person sleeps soundly and for a normal length on their own late schedule and feels refreshed. That preserved sleep on a delayed timetable is the feature that points to a clock problem rather than to insomnia. [8] [9]
The consequences are what bring families to help and what examiners probe. Chronic behavioural insomnia wears down parental mental health and can strain the whole household. Delayed phase in a teenager produces school lateness and absence, falling grades, low mood and conflict at home, and the sleepiness itself carries real risk in a young person who drives. Recognising these downstream harms justifies active treatment rather than watchful waiting. [3] [9]
Differential Diagnosis
The first thing to exclude is not a disorder at all but a schedule. Insufficient sleep from an inadequate opportunity to sleep — a packed timetable, a chaotic home, or simply a bedtime too late for the child's needs — mimics both families and is corrected by protecting time in bed rather than by any specific therapy. Confirming adequate sleep opportunity is therefore the opening move of the differential. [1] [8]
Organic sleep disorders must then be actively sought, because they masquerade as behavioural problems. A snoring, gasping child may have obstructive sleep apnoea; a child who cannot keep still at bedtime and describes an urge to move the legs may have restless legs syndrome or periodic limb movements; and dramatic night-time events may be parasomnias. In the adolescent, delayed sleep-wake phase disorder must be distinguished from primary psychophysiological insomnia and from depression and anxiety — while remembering these conditions frequently coexist and reinforce each other. [8] [10]
Clinical & Bedside Assessment
The assessment is a history, and a good one is largely diagnostic. It maps the whole 24 hours: the bedtime routine and environment, exactly how the child falls asleep and what conditions are needed, the number and handling of night wakings, and the timing of sleep and wake on both school and free days. It then measures daytime function — mood, behaviour, school attendance and sleepiness — and screens deliberately for snoring, restless legs, anxiety, low mood and ADHD. [1] [8]
A prospective sleep diary kept for one to two weeks turns the history into a pattern and is the workhorse of the topic. It reveals the true sleep and wake times, the weekday–weekend gap that betrays a delayed phase, and the frequency of wakings, and it doubles as a baseline to judge treatment. Where available, actigraphy — a wrist-worn movement monitor worn for one to two weeks — provides an objective record of the sleep-wake rhythm and is especially useful for confirming a circadian disorder. [8] [3]
Investigations
For most children this is a clinical diagnosis and no laboratory test is needed. The history and the sleep diary establish behavioural insomnia or a circadian disorder directly, and the examiner rewards a candidate who states plainly that routine polysomnography is not required for uncomplicated behavioural or circadian sleep problems. Investigation is reserved for when an organic disorder is suspected or the picture does not fit. [8] [1]
Actigraphy is the most useful objective investigation when one is wanted, documenting the sleep-wake pattern over one to two weeks and confirming a delayed or irregular rhythm. In specialist practice the timing of the dim light melatonin onset can be measured to establish the internal clock time precisely and to guide when melatonin should be given, although this is not needed for everyday management. Polysomnography is the test to add when obstructive sleep apnoea, periodic limb movements or an atypical hypersomnia is suspected. [8] [10]
Management — Resuscitation
These conditions are not medical emergencies, but a small number of situations need urgent, prioritised action rather than a routine clinic plan. The clearest is dangerous daytime sleepiness — the adolescent who is driving, or a child so sleep-deprived that safety and functioning are threatened — which requires prompt schedule correction and same-visit safety advice. The urgency is about the consequence of the sleep loss, not the sleep disorder itself. [8] [9]
The second priority is the adolescent whose delayed phase presents as entrenched school refusal with low mood. Circadian disruption and depression drive each other, so an active screen for depression, anxiety and suicidal ideation is mandatory, and a positive screen changes the plan to include mental health care alongside the sleep intervention. In severe behavioural insomnia, an exhausted and overwhelmed family may be in crisis, and the right first response is early structured behavioural support — not a sedative to buy quiet. [3] [9]
Management — Definitive & Stepwise
Behavioural intervention is the definitive first-line treatment for behavioural insomnia of childhood, and the evidence for it is strong. Mindell and colleagues' review and the accompanying American Academy of Sleep Medicine practice parameter found consistent, durable benefit from behavioural methods for bedtime problems and night wakings, and Meltzer and Mindell's meta-analysis confirmed their efficacy across paediatric insomnia. The techniques are chosen to match the subtype and the family. [1] [2] [3]
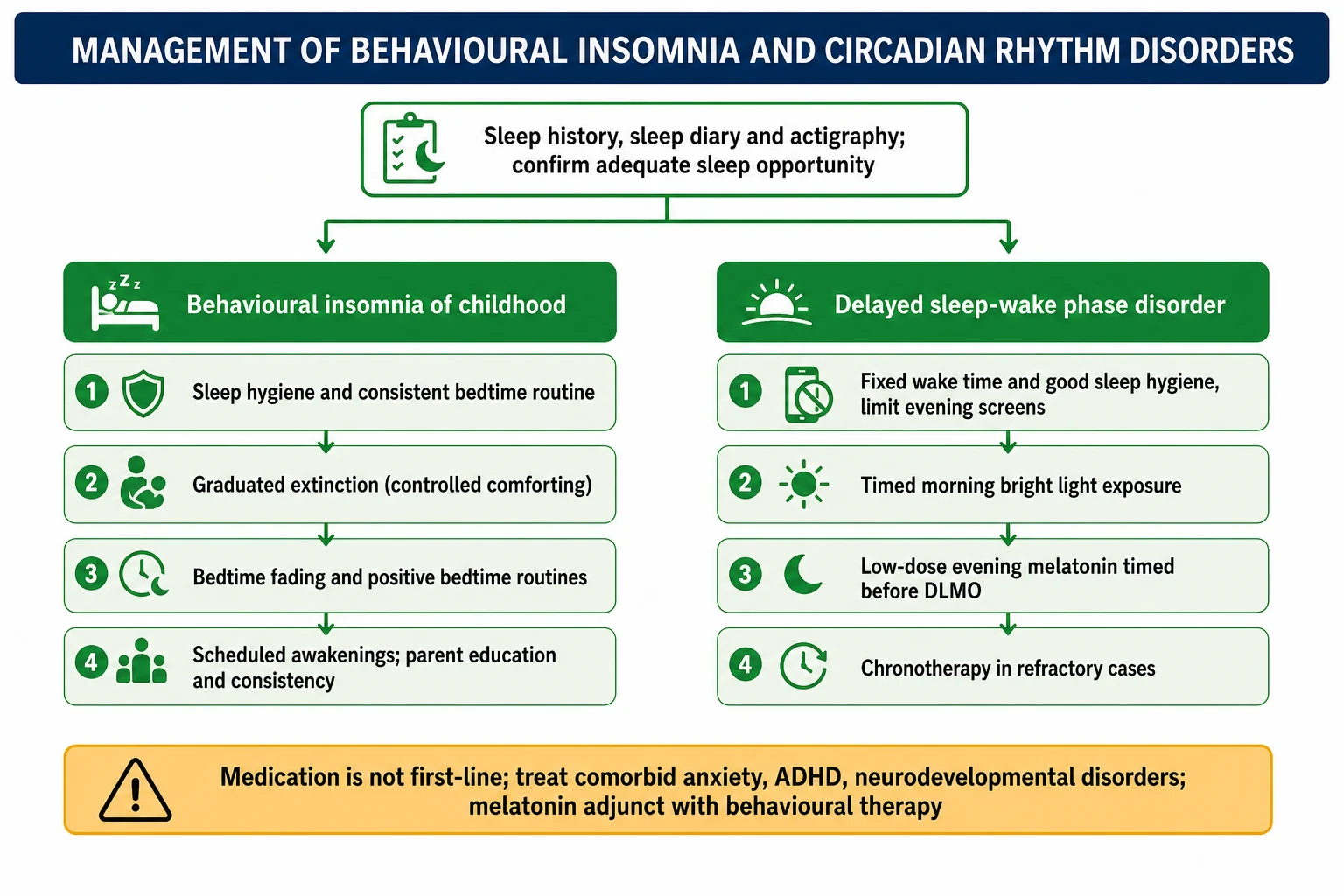
The core techniques are practical and teachable. A consistent, soothing bedtime routine and good sleep hygiene set the foundation. Graduated extinction — "controlled comforting", checking on the child at gradually lengthening intervals — treats sleep-onset association type by letting the child learn to self-settle. Bedtime fading temporarily moves bedtime later to match the child's actual sleep onset and then advances it. Positive bedtime routines and consistent limit-setting resolve limit-setting type, and scheduled awakenings can pre-empt habitual night wakings. [1] [2]
Delayed sleep-wake phase disorder is treated by resetting and holding the clock. The plan combines a fixed, realistic wake time every day, good sleep hygiene with reduced evening light and screens, timed morning bright light to advance the clock, and a low dose of melatonin given in the early evening — several hours before habitual sleep onset — to act as a chronobiotic. The American Academy of Sleep Medicine circadian guideline supports strategically timed melatonin, and a randomised trial by Saxvig and colleagues showed that bright light and melatonin improve sleep in delayed phase; chronotherapy, progressively delaying bedtime around the clock, is reserved for refractory cases. [8] [11]
Stepwise management by problem
Take a sleep history and a one to two week sleep diary; confirm adequate sleep opportunity
Exclude organic sleep disorders and screen for anxiety, ADHD and low mood
For behavioural insomnia: sleep hygiene and a consistent bedtime routine
Add graduated extinction or bedtime fading for sleep-onset association type; consistent limits and positive routines for limit-setting type
For delayed sleep-wake phase disorder: set a fixed daily wake time and reduce evening light and screens
Add timed morning bright light to advance the clock
Add low-dose evening melatonin timed hours before habitual sleep onset (chronobiotic)
Reserve chronotherapy and specialist referral for refractory or complex cases; treat comorbidities
Melatonin (paediatric sleep-onset insomnia and delayed sleep-wake phase disorder)
Loading dose
Delayed sleep-wake phase disorder: low dose (about 0.5 mg) timed several hours before habitual sleep onset to advance the clock (chronobiotic effect)
Maintenance dose
Chronic sleep-onset insomnia: immediate-release melatonin, commonly 2–3 mg 30–60 minutes before the desired bedtime, titrated to effect (dose-finding: van Geijlswijk 2010)
Specific Subtypes & Scenarios
The rocked-to-sleep infant is the archetypal sleep-onset association case. A baby who is fed or rocked until asleep has learned that this is how sleep begins, so at every light arousal overnight — which every infant has — the same help is demanded. Graduated extinction and bedtime fading break the association by teaching the child to fall asleep independently, and parents are coached that a brief increase in protest is expected before improvement. [1] [2]
The stalling preschooler is the archetypal limit-setting case. Bedtime becomes a negotiation of one more story, one more drink, and the parent who eventually stays inadvertently rewards the resistance. Treatment is a calm, consistent bedtime with clear limits, a positive routine the child looks forward to, and reward for staying in bed. The adolescent with a delayed clock and mounting school absence is the third recurring scenario, needing the fixed wake time, morning light and timed melatonin combination plus liaison with the school about attendance. [1] [8]
Across Australia, New Zealand and the United Kingdom the model is the same: behavioural sleep problems and delayed phase are managed chiefly in primary and general paediatric care, with written behavioural plans, sleep diaries and parent education, and referral to sleep or mental health services reserved for refractory or complex cases. Melatonin is widely used for paediatric insomnia — particularly in children with neurodevelopmental disorders — and prescribing frameworks emphasise behavioural therapy first and correct timing. In the ANZ context, access to sleep clinics and actigraphy is uneven, social disadvantage and crowded housing can undermine routines, and culturally appropriate advice and telehealth follow-up help bridge the gap for rural, remote and Indigenous families. [6] [8]
The child with autism or ADHD and chronic insomnia is a scenario in its own right and a favourite of examiners. Insomnia is very common in these children, behavioural strategies still come first but often need adaptation, and melatonin has its strongest evidence here: Gringras and colleagues' randomised trial showed that melatonin improved sleep onset in children with neurodevelopmental disorders. Treating the underlying condition and any coexisting anxiety is part of the sleep plan rather than separate from it. [7] [6]
Complications & Pitfalls
Untreated sleep-timing problems do real harm. Chronic sleep restriction impairs daytime behaviour, mood, attention and learning, and in the adolescent it drives school absence and academic decline. The family cost is substantial too: persistent behavioural insomnia is strongly linked to parental exhaustion, stress and depression, which is one of the reasons effective treatment improves the wellbeing of the whole household. [3] [9]
The pitfalls cluster around shortcuts and mislabelling. The commonest is reaching for melatonin or a sedative before a behavioural or circadian plan. The next is mistaking a delayed clock for ordinary insomnia and simply telling the teenager to go to bed earlier, which fails because the clock, not the willpower, is late. A third is timing melatonin wrongly — too large a dose too close to bedtime — so it sedates rather than shifts the phase. Missing an organic disorder such as obstructive sleep apnoea is the quiet, dangerous error. [6] [8]
Prognosis & Disposition
The outlook for behavioural insomnia of childhood is good, and this optimism should be conveyed to families. Consistent behavioural treatment produces durable improvement in settling and night wakings, with measurable benefits to the child's daytime behaviour and to parental mood and stress. The main threat to success is inconsistency, so much of the clinician's work is supporting the family to persevere through the first difficult nights. [1] [3]
Delayed sleep-wake phase disorder can be corrected with combined light and melatonin therapy, but it is prone to relapse whenever the routine slips — a run of late nights or weekend sleep-ins lets the clock drift back. The prognosis therefore depends on maintenance: a protected wake time, ongoing sleep hygiene and, where needed, continued timed melatonin. Most children in both families are managed entirely in primary or general paediatric care with a written plan and diary review. [8] [11]
Disposition is matched to complexity. The straightforward child is managed with parent education, a behavioural plan and diary follow-up, often by telehealth. Referral to a sleep service or mental health team is reserved for treatment failure, diagnostic doubt, significant comorbidity, or the complex child with neurodevelopmental disability. Equitable access to these services, and to actigraphy where it is needed, is part of good disposition planning in the ANZ setting. [6] [8]
Special Populations
Children with autism spectrum disorder and ADHD carry a very high burden of insomnia, and they are the special population most examined. Behavioural strategies remain first-line but usually need tailoring to the child's communication and sensory profile, and melatonin has its best evidence in this group, improving sleep onset in the randomised trial by Gringras and colleagues. Coexisting anxiety and the effect of stimulant medication on sleep must both be addressed as part of the plan. [7] [6]
Adolescents as a group are prone to delayed sleep-wake phase disorder because puberty itself delays the clock, and early school start times collide with that biology. Understanding this "perfect storm" reframes the sleepy, late teenager as biologically driven rather than simply lazy, and supports interventions aimed at the clock and, at a policy level, at school timing. The blind child is a distinct special case, prone to a free-running non-24-hour rhythm that timed melatonin can entrain. [9] [8]
Social and cultural context shapes both risk and treatment. Crowded or disrupted housing, shift-working parents and socioeconomic disadvantage make consistent routines harder to keep, and sleep advice must be realistic for the family's circumstances rather than idealised. In the ANZ context, culturally safe advice, attention to equity of access to sleep services, and telehealth follow-up matter for rural, remote and Indigenous families who face the greatest barriers. [6] [3]
Evidence, Guidelines & Regional Differences
The behavioural evidence base is the backbone of the topic. Mindell and colleagues' 2006 review and the American Academy of Sleep Medicine practice parameter by Morgenthaler and colleagues established behavioural interventions as effective, well-supported first-line treatment for bedtime problems and night wakings. Meltzer and Mindell's 2014 meta-analysis reinforced this, confirming the efficacy of behavioural interventions across paediatric insomnia and giving the candidate a citable evidence summary. [1] [2] [3]
For the circadian disorders, the American Academy of Sleep Medicine 2015 clinical practice guideline by Auger and colleagues is the reference, supporting strategically timed melatonin and light for delayed sleep-wake phase disorder and defining the other circadian diagnoses. The melatonin literature is anchored by van Geijlswijk's dose-finding trial and long-term safety follow-up, by Bruni and colleagues' clinical recommendations for paediatric neurology, and by Gringras and colleagues' randomised trial in neurodevelopmental disorders, while Crowley and Micic explain the adolescent phase delay and the aetiology of delayed sleep phase disorder. [4] [6] [7] [8]
The regional differences are pragmatic rather than conceptual. High-resource systems agree that behavioural therapy comes first and that melatonin is an adjunct, but the availability of sleep clinics, actigraphy and dim light melatonin onset testing varies, and prescribing rules for melatonin differ between countries. The ANZ context adds an equity dimension: uneven access to specialist sleep services, the impact of disadvantage on the feasibility of routines, and the value of telehealth and culturally appropriate advice for rural, remote and Indigenous families. [6] [8]
Exam Pearls
Manage the sleepless child — 'SETTLE'
References
- [1]Mindell JA; Kuhn B; Lewin DS; Meltzer LJ; Sadeh A Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep, 2006.PMID 17068979
- [2]Morgenthaler TI; Owens J; Alessi C; Boehlecke B; Brown TM; Coleman J; et al Practice parameters for behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep, 2006.PMID 17068980
- [3]Meltzer LJ; Mindell JA Systematic review and meta-analysis of behavioral interventions for pediatric insomnia. J Pediatr Psychol, 2014.PMID 24947271
- [4]van Geijlswijk IM; van der Heijden KB; Egberts ACG; Korzilius HPLM; Smits MG Dose finding of melatonin for chronic idiopathic childhood sleep onset insomnia: an RCT. Psychopharmacology (Berl), 2010.PMID 20668840
- [5]van Geijlswijk IM; Mol RH; Egberts TCG; Smits MG Evaluation of sleep, puberty and mental health in children with long-term melatonin treatment for chronic idiopathic childhood sleep onset insomnia. Psychopharmacology (Berl), 2011.PMID 21340475
- [6]Bruni O; Alonso-Alconada D; Besag F; Biran V; Braam W; Cortese S; et al Current role of melatonin in pediatric neurology: clinical recommendations. Eur J Paediatr Neurol, 2015.PMID 25553845
- [7]Gringras P; Gamble C; Jones AP; Wiggs L; Williamson PR; Sutcliffe A; et al Melatonin for sleep problems in children with neurodevelopmental disorders: randomised double masked placebo controlled trial. BMJ, 2012.PMID 23129488
- [8]Auger RR; Burgess HJ; Emens JS; Deriy LV; Thomas SM; Sharkey KM Clinical Practice Guideline for the Treatment of Intrinsic Circadian Rhythm Sleep-Wake Disorders: Advanced Sleep-Wake Phase Disorder (ASWPD), Delayed Sleep-Wake Phase Disorder (DSWPD), Non-24-Hour Sleep-Wake Rhythm Disorder (N24SWD), and Irregular Sleep-Wake Rhythm Disorder (ISWRD). An Update for 2015: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med, 2015.PMID 26414986
- [9]Crowley SJ; Wolfson AR; Tarokh L; Carskadon MA An update on adolescent sleep: New evidence informing the perfect storm model. J Adolesc, 2018.PMID 29908393
- [10]Micic G; Lovato N; Gradisar M; Ferguson SA; Burgess HJ; Lack LC The etiology of delayed sleep phase disorder. Sleep Med Rev, 2016.PMID 26434674
- [11]Saxvig IW; Wilhelmsen-Langeland A; Pallesen S; Vedaa O; Nordhus IH; Bjorvatn B A randomized controlled trial with bright light and melatonin for delayed sleep phase disorder: effects on subjective and objective sleep. Chronobiol Int, 2014.PMID 24144243