Paeds · respiratory-sleep-and-airway
Croup
Also known as Laryngotracheobronchitis · Viral croup · Acute laryngotracheitis · Spasmodic croup · Barking cough illness
Fellowship guide to croup (viral laryngotracheobronchitis): the parainfluenza-driven subglottic oedema that gives a barking cough, inspiratory stridor and a hoarse voice in a young child; the Westley score; the discriminators from epiglottitis, bacterial tracheitis and foreign body; steroid for every child, nebulised adrenaline for stridor at rest, calm handling, observation and disposition; and the ANZ, UK and North American guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
Overview & Definition
Picture the two-year-old whose parents wake at 2 a.m. to a strange seal-like bark and a high-pitched noise every time she breathes in. She had a runny nose and a low fever yesterday, she is frightened but not toxic, and the noise softens when her mother holds her still. That midnight scene — the barking cough, the inspiratory stridor and the hoarse voice in a well-ish young child with a viral prodrome — is croup, and recognising it quickly is what separates a calm steroid-and-observe pathway from a panicked airway. [1] [2]
Croup is an acute viral infection of the larynx, trachea and (to a lesser extent) the bronchi, so its full name, laryngotracheobronchitis, tells you where the trouble is. The inflammation and oedema concentrate in the subglottis, the narrowest part of a young child's airway, which is why a modest amount of swelling produces a disproportionate amount of noise and obstruction. [1] [9]
Why this matters at fellowship level is that croup is one of the commonest causes of acute upper-airway obstruction in early childhood, it is almost always self-limiting, and the modern evidence base has made it a model of high-value care: a single dose of a cheap steroid changes the trajectory, and the real skill is recognising the small minority who are deteriorating and the mimics that masquerade as croup. [3] [10]
Classification
Croup is best classified two ways at once: by what is causing the airway noise and by how severe the obstruction is right now, because the second drives every treatment decision at the bedside. [1] [2]
By cause, the usual entity is viral croup (laryngotracheobronchitis), overwhelmingly parainfluenza but also influenza, respiratory syncytial virus, adenovirus, human metapneumovirus and SARS-CoV-2. Spasmodic (recurrent) croup describes sudden, often recurrent nocturnal stridor with little or no viral prodrome and rapid resolution, thought to have an allergic or hyper-reactive component and managed the same way acutely. Distinguishing these from the dangerous bacterial airway conditions is the whole point of the differential. [1] [9]
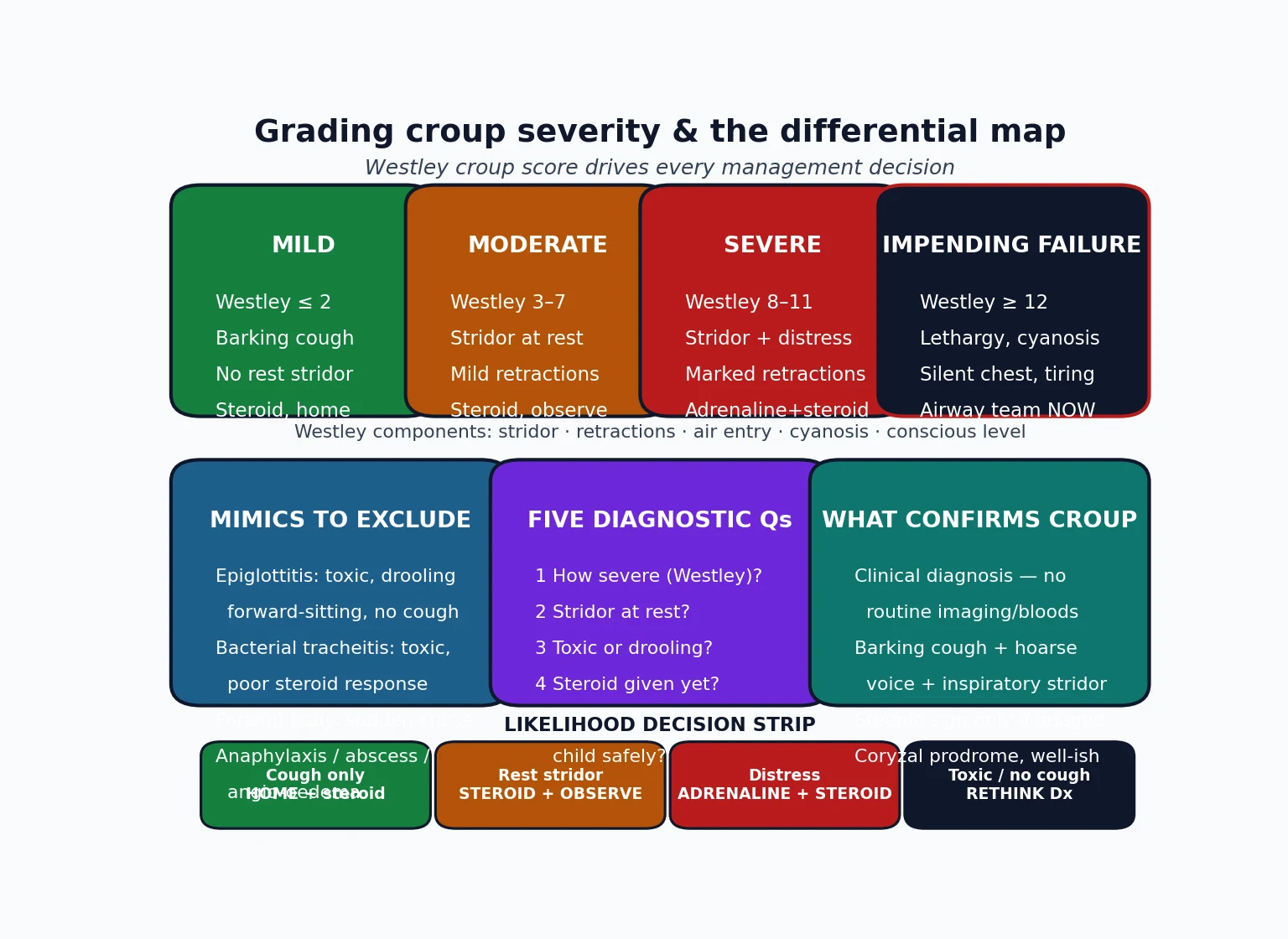
By severity, the validated tool is the Westley croup score, which sums five clinical items — inspiratory stridor, chest-wall retractions, air entry, cyanosis and conscious level — to place a child on a spectrum from mild through moderate and severe to impending respiratory failure. It is more useful as a shared language and a reassessment anchor than as an arithmetic gate, but it disciplines your thinking about who needs adrenaline and who needs the airway team. [8] [1]
The numbers that anchor your viva
Epidemiology & Risk Factors
Croup is a disease of early childhood. It peaks in the second year of life, is uncommon before six months and after six years, and is a little more frequent in boys, with a clear autumn-to-winter seasonality that tracks the circulating parainfluenza and other respiratory viruses. [1] [2]
Most children have a single, self-limiting episode, but a substantial minority have recurrent croup, and repeated or unusually severe episodes should prompt a thought about an underlying anatomical narrowing — subglottic stenosis (especially in an ex-premature infant who was intubated), a subglottic haemangioma, or another fixed airway lesion — that lowers the threshold at which viral oedema causes symptoms. [9] [1]
The risk amplifiers are mostly about airway calibre and access to care. A younger, smaller child obstructs sooner because the subglottis is tiny; a child with a pre-existing airway narrowing needs less oedema to stridor; and a family far from timely reassessment (rural, remote, or without transport) faces more risk from the same illness because the safety net of observation is thinner. [2] [1]
Pathophysiology
The teaching model runs from the virus to the noise you hear, and it hinges on one fact of paediatric anatomy: in a young child the subglottis, ringed by the only complete cartilage of the airway (the cricoid), is the narrowest point, and it cannot expand outward when it swells. [1] [9]
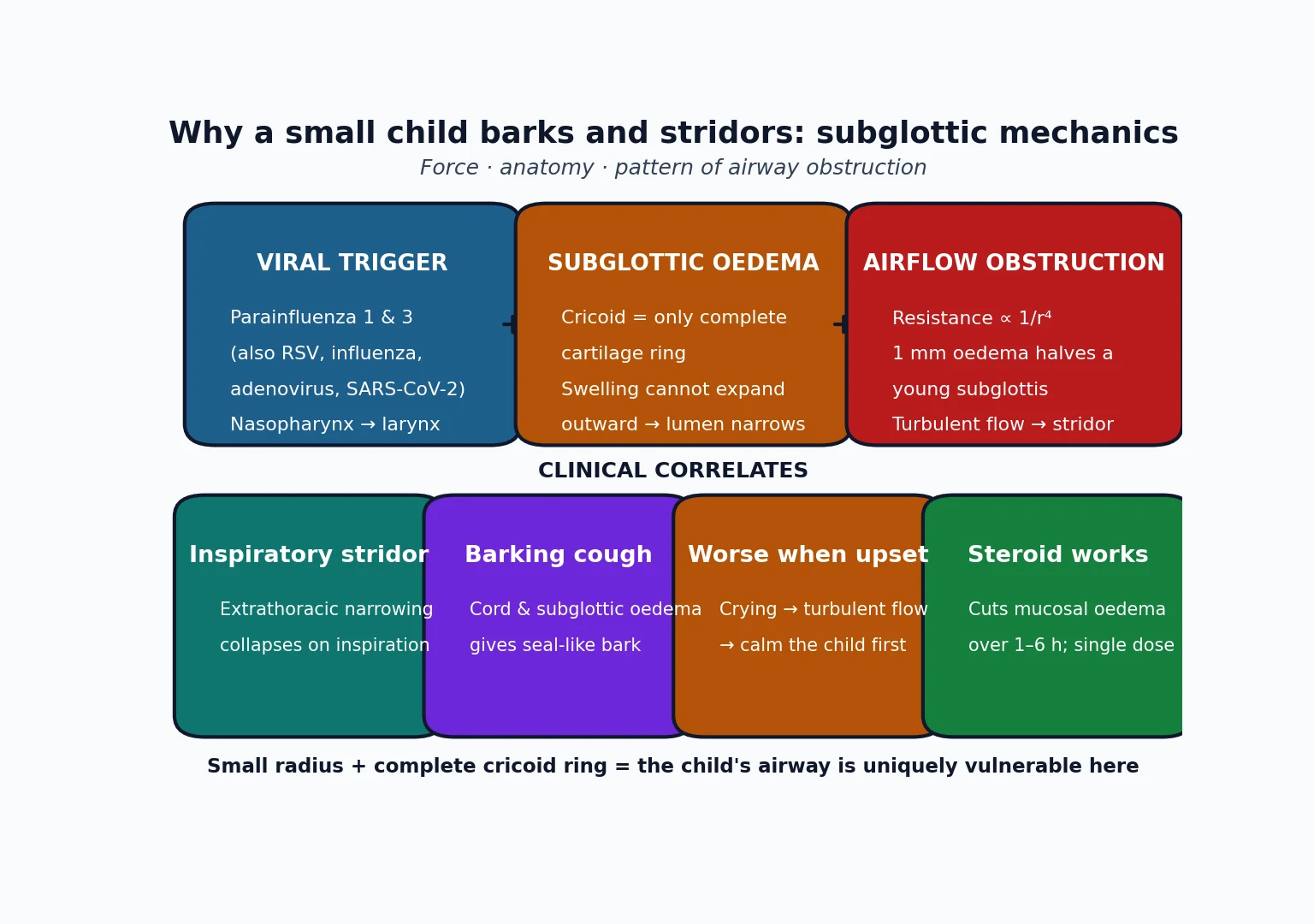
A respiratory virus, most often parainfluenza, infects the nasopharyngeal epithelium and spreads down to the larynx and trachea, producing inflammation, mucosal oedema and increased secretions. Because resistance to airflow rises with the fourth power of the falling radius (Poiseuille's law), even a millimetre of circumferential subglottic swelling markedly narrows a toddler's airway and turns smooth laminar flow into the turbulent flow that we hear as stridor. [1] [9]
The clinical picture then follows directly from the mechanics. Oedema of the vocal cords and subglottis gives the barking, seal-like cough and the hoarse voice; the extrathoracic (upper-airway) narrowing collapses further on inspiration, so the stridor is characteristically inspiratory; and because crying and agitation increase airflow and turbulence, the obstruction — and the child's distress — worsen in a vicious cycle, which is why keeping the child calm is genuine treatment, not just comfort. [1] [2]
A common misconception is that croup is a lower-airway or "chesty" illness. It is fundamentally an upper-airway obstruction: the abnormal sound is inspiratory stridor, not the expiratory wheeze of asthma or bronchiolitis, and confusing the two leads to the wrong treatment and the wrong disposition. [1] [9]
Clinical Presentation
The classic story is a well or mildly unwell toddler with a one-to-three-day coryzal prodrome who develops, often abruptly and at night, a barking cough, a hoarse voice or cry, and inspiratory stridor. Low-grade fever is common; high fever and a toxic appearance are not typical and should make you think again. [1] [2]
The single most useful bedside skill is to gauge severity from across the room before you touch the child, because the examination itself can precipitate deterioration. Watch for stridor at rest versus only on exertion, the degree of chest-wall and sternal retraction, the respiratory rate and effort, the colour, and the child's alertness and interaction with the carer. [2] [1]
| Severity | Bedside picture | Immediate action |
|---|---|---|
| Mild | Barking cough, hoarse voice, no stridor at rest (or only when upset), no distress | Corticosteroid, reassure, home with a safety-net plan |
| Moderate | Stridor at rest with mild-to-moderate retractions, but alert and interactive | Corticosteroid, keep calm, observe, reassess |
| Severe | Stridor at rest with marked retractions, agitation or distress, poor air entry | Nebulised adrenaline plus corticosteroid, call for help, observe closely |
| Impending failure | Tiring, drowsy or pale child; rising then falling effort; cyanosis; silent chest | Airway team now: senior, anaesthetics, ENT; minimal handling; prepare a difficult airway |
The trap is the quiet, tiring child. A toddler who was noisy and distressed and then becomes still, pale and drowsy with a falling respiratory rate is not getting better — the reduced noise reflects reduced air movement through a critically narrowed airway. A silent chest with poor air entry in a previously stridulous child is a pre-arrest sign. [1] [2]
Croup that is atypical should raise the alarm: high fever with a toxic appearance, drooling and a preference to sit forward, an absent cough, a very rapid onset with choking, an age outside the usual band, or a poor response to standard treatment. Each points away from simple viral croup and toward a mimic you must not miss. [1] [9]
Differential Diagnosis
Sort the differential into three groups: the mimics that kill (bacterial airway emergencies), the mimics that obstruct suddenly (foreign body and anaphylaxis), and the chronic narrowings that present as recurrent croup. The aim is to confirm viral croup confidently while never anchoring on it in the toxic or atypical child. [1] [9]
Viral croup
the usual answer
- Coryzal prodrome, low fever, well-ish
- Barking cough + hoarse voice
- Inspiratory stridor, gradual onset
- Responds to steroid ± adrenaline
Epiglottitis
- Toxic, high fever, rapid onset
- Drooling, muffled voice, no cough
- Sits forward, tripod, distressed
- Do NOT examine throat; airway team
Bacterial tracheitis
- Toxic child, high fever
- Croup-like then deteriorates
- Poor response to adrenaline/steroid
- Thick purulent tracheal secretions
Foreign body / other
- Sudden choke, no prodrome
- Anaphylaxis: urticaria, exposure
- Retropharyngeal abscess, diphtheria
- Recurrent = subglottic stenosis/haemangioma
Epiglottitis is the classic can't-miss: a toxic, febrile child who is drooling, has a muffled ("hot-potato") voice, will not lie down and characteristically has no barking cough. It is now rare where Haemophilus influenzae type b immunisation is high, but it still occurs, and the cardinal rule is to keep the child calm, avoid examining the throat or distressing them, and get the airway team before anything else. [1] [9]
Bacterial tracheitis is the great imitator that starts like croup and then declares itself by toxicity, high fever and a poor response to adrenaline and steroid, with thick purulent tracheal secretions; it needs antibiotics, airway assessment and often intensive care. A foreign body gives sudden onset without a prodrome, often with a witnessed choking episode, and recurrent or unusually severe croup should prompt evaluation for a fixed subglottic narrowing once the acute episode has settled. [9] [1]
Clinical & Bedside Assessment
Assessment is almost entirely clinical and almost entirely observational. Take a focused history — the prodrome, the onset and timing, immunisation status (especially Hib), any previous croup or intubation, and any choking episode — and then assess severity from a distance while the child stays on the carer's lap. [2] [1]
Use the Westley score as your structured tool: score inspiratory stridor (none / with agitation / at rest), retractions (none / mild / moderate / severe), air entry (normal / decreased / markedly decreased), cyanosis (none / with agitation / at rest) and level of consciousness (normal / altered), and let the total anchor your grade and your reassessment. Serial scores tell you the trajectory better than any single number. [8] [1]
Reading the child, not just the score
Severe
Stridor + distress or agitation; poor air entry
Deliberately avoid the things that agitate the child or add nothing: no tongue depressor or throat examination if there is any suspicion of epiglottitis, no routine venepuncture or cannulation in mild-to-moderate croup, and no lying the child flat against their preference. Calm assessment on a parent's knee is both safer and more accurate. [2] [1]
Investigations
Croup is a clinical diagnosis and needs no routine tests. The default in a typical case is no bloods, no imaging and no viral swabs — investigations are reserved for when the diagnosis is in doubt or a complication or mimic is suspected. [1] [10]
Neck radiographs are not required to diagnose croup and can dangerously delay care or distress the child; when a film is obtained for another reason it may show the "steeple sign" of subglottic narrowing on the frontal view, but its absence does not exclude croup and its presence does not confirm severity. Imaging belongs to the workup of an atypical presentation — a suspected radio-opaque foreign body, a retropharyngeal abscess, or an uncertain diagnosis — not to routine croup. [1] [9]
Pulse oximetry is reasonable and unobtrusive, but remember that hypoxaemia is a late sign in upper-airway obstruction: a child can be working very hard with a normal saturation, so oximetry never overrides the clinical picture of increasing distress or fatigue. [1] [2]
Management — Resuscitation
For the small number of children in severe croup or impending respiratory failure, the priority is a calm, staged airway approach delivered by the right team, not a scramble. Minimise handling, let the child stay with the parent, give oxygen gently if tolerated (blow-by if a mask distresses them), and summon senior paediatric, anaesthetic and ENT support early. [1] [2]
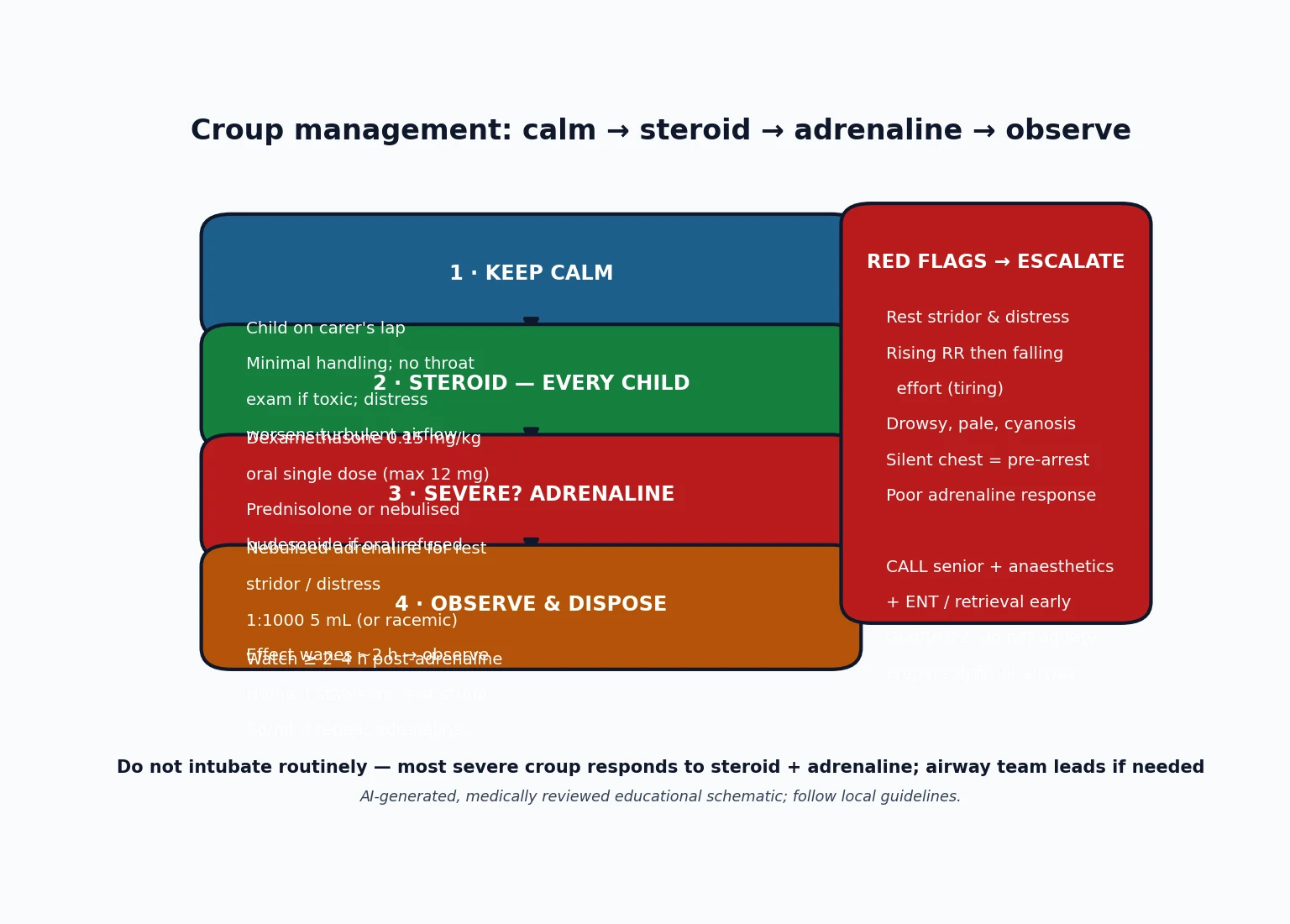
Give nebulised adrenaline immediately for stridor at rest with distress: adrenaline (epinephrine) 1:1000 (1 mg/mL) 0.5 mL/kg up to a maximum of 5 mL nebulised, or nebulised racemic adrenaline where available, alongside a corticosteroid. It works within minutes by vasoconstricting the oedematous mucosa, but its effect wanes over about two hours, so the child must be observed for rebound after each dose rather than sent home on the strength of a good initial response. [7] [8]
Acute airway drugs in severe croup
Intubation is rarely needed and is not a routine step even in severe croup — most children respond to steroid plus adrenaline and buy the time the medicine needs to work. When an airway is genuinely failing, it is managed by the most experienced airway operator available, using a tube smaller than predicted for age because the subglottis is narrowed, with a plan for a surgical airway as a last resort. [1] [2]
Management — Definitive & Stepwise
The definitive management of croup is elegantly simple: a corticosteroid for every child, adrenaline for those with stridor at rest or distress, calm supportive care throughout, and disposition by response and severity. [3] [1]
Corticosteroid for everyone is the central, evidence-based step. A single dose of dexamethasone 0.15 mg/kg orally is the standard first choice, effective across the whole severity range and supported by the Cochrane review of glucocorticoids for croup; doses up to 0.6 mg/kg are used and are no more effective than 0.15 mg/kg for most children, so the lower dose is preferred. Where oral dexamethasone is not tolerated, options are oral prednisolone, intramuscular dexamethasone, or nebulised budesonide 2 mg. [3] [6]
The stepwise pathway
Assess severity by observation (Westley) with the child calm on the carer's lap.
Give a corticosteroid to every child — dexamethasone 0.15 mg/kg oral single dose is first-line.
If stridor at rest or distress: add nebulised adrenaline 0.5 mL/kg (max 5 mL) of 1:1000.
Keep the child calm; give gentle oxygen only if needed; escalate early if deteriorating.
Observe after adrenaline for rebound (usually ≥ 2–4 hours) and reassess severity.
Dispose by response: home with safety-net advice, or admit if repeated adrenaline, poor response, or an unsafe home situation.
Nebulised adrenaline is the rescue for moderate-to-severe disease; it is not a treatment for mild croup, where steroid alone suffices. After adrenaline, a period of observation is mandatory because of the two-hour wane; a child who remains well after that window, with no stridor at rest, can usually go home, whereas one who needs repeated adrenaline or does not improve should be admitted and reassessed for a mimic. [7] [8]
Steam and humidified air, long a folk remedy, have not been shown to help in controlled studies and can distress or scald the child; the effective, high-value interventions are the steroid, adrenaline when indicated, and a calm environment. Distraction, a familiar carer and minimal intervention do more for a mild-to-moderate child than any inhaled mist. [1] [10]
CROUP-Rx
Specific Subtypes & Scenarios
Spasmodic (recurrent) croup presents as sudden nocturnal stridor with little or no viral prodrome, often recurring and settling quickly. Acutely it is managed exactly like viral croup — assess severity, give steroid, add adrenaline if there is stridor at rest — but a pattern of frequent recurrence warrants a thought about atopy and about an underlying airway narrowing once the child is well. [1] [9]
The child with recurrent or persistent stridor deserves a deliberate outpatient airway evaluation after the acute episode. Repeated croup, croup outside the usual age band, or stridor that never fully clears can be the surface sign of subglottic stenosis (classically in an ex-premature infant who was intubated) or a subglottic haemangioma, both of which change management. [9] [1]
Bjornson 2004 — N Engl J Med (PMID 15385657)
Randomised, double-blind, placebo-controlled trial in children with mild croup
Key finding
Children given dexamethasone had fewer return visits for medical care and faster resolution than placebo, establishing benefit even at the mild end of the spectrum.
Practice change
Give a corticosteroid to every child with croup, not only the moderate or severe — the lesson that steroid is universal, not selective.
The remote or telehealth presentation is a common exam scenario: a child with croup a long way from a hospital. The priorities are to gauge severity remotely as best you can, ensure a steroid dose is actually given, arrange transfer if there is stridor at rest or any deterioration, and give the family explicit, concrete return advice — because the safety net of easy reassessment is exactly what geography removes. [2] [3]
Croup superimposed on a fixed narrowing (known subglottic stenosis or haemangioma) obstructs at a lower threshold and may respond less completely to standard treatment; these children need earlier senior and ENT involvement and a lower threshold for admission and airway assessment. [9] [1]
Complications & Pitfalls
Serious complications of viral croup are uncommon because the illness is self-limiting and the treatment is effective, but they do happen: progression to respiratory failure needing intubation in a very small minority, secondary bacterial infection (bacterial tracheitis), and, rarely, the sequelae of severe hypoxia if obstruction is missed. [1] [9]
The dominant pitfalls are diagnostic and dispositional. The first is missing a mimic — treating a toxic, drooling child as croup instead of recognising epiglottitis or bacterial tracheitis, or attributing a sudden choking presentation to croup rather than a foreign body. The discriminators are toxicity, absence of the barking cough, drooling, sudden onset, and a poor response to standard croup treatment. [1] [9]
The second pitfall is misreading the quiet child as improving when the reduced noise actually signals reduced air movement and impending failure; the third is discharging too early after adrenaline, before the two-hour wane has been observed, so a child rebounds at home. Each is avoided by the same discipline: reassess the child, not the clock, and grade the trajectory. [7] [1]
[10]A quieter pitfall is over-treatment and low-value care: routine neck films, blood tests, viral swabs, antibiotics for a viral illness, and humidified air all add cost, distress and delay without benefit in typical croup. High-value care is the steroid, adrenaline when indicated, calm observation and clear advice. [1] [10]
Prognosis & Disposition
The prognosis of viral croup is excellent. The great majority of children improve within a day or two, fewer than one in twenty need admission, and intubation is needed in well under one per cent even of those with severe disease; recurrence during childhood is common but the long-term outlook is normal. [1] [2]
Disposition is decided by severity and response, not by a fixed rule. A child with mild croup, or one whose moderate croup settles after steroid with no stridor at rest, can go home with clear safety-net advice; a child who needed adrenaline should be observed for the rebound window and admitted if they need it repeated or fail to improve; and any child with severe or deteriorating disease, or an unsafe route back to care, should be admitted. [3] [2]
Safety-net advice is part of the treatment and must be concrete: return urgently if the stridor is present at rest, if breathing becomes harder with in-drawing of the chest, if the child becomes pale, drowsy or blue, or if you are worried — and be explicit that the illness can flare again the next night. Give a plan the family can act on, not a vague reassurance. [2] [10]
Special Populations
The ex-premature infant with a history of intubation carries a real risk of subglottic stenosis, so viral croup in this child can obstruct sooner and respond less completely; involve senior and ENT teams earlier and keep a lower threshold for admission and airway evaluation. [9] [1]
Children with an underlying airway or neuromuscular condition — subglottic haemangioma, laryngomalacia, Down syndrome (with a naturally narrower subglottis), or reduced airway-protective reflexes — have less reserve, and a standard viral insult can produce disproportionate obstruction; they warrant closer observation and earlier escalation. [1] [9]
Indigenous, rural and remote families face the same illness with a thinner safety net: longer distances to reassessment, and in some communities a higher burden of respiratory illness. The key equity intervention is to ensure the steroid is actually given, to arrange retrieval promptly for moderate-to-severe disease, and to give unambiguous return advice suited to the family's circumstances. [2] [3]
The immunisation-incomplete child shifts your differential: where Hib coverage is low or unknown, keep epiglottitis higher on the list for a toxic child, and where diphtheria immunisation is incomplete, remember membranous ("true") croup as a rare but dangerous mimic. [1] [9]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | Steroid emphasis | Notes |
|---|---|---|---|
| ANZ | RCH Melbourne and state CPGs | Dexamethasone 0.15 mg/kg oral for all; budesonide if oral refused | Adrenaline for moderate-to-severe; observe for rebound |
| UK | NICE / CKS | Single-dose oral dexamethasone or prednisolone even for mild | Admission by severity, response and social factors |
| North America | AAP-aligned and Cochrane evidence | Dexamethasone 0.15–0.6 mg/kg; single dose | Nebulised adrenaline then observation before discharge |
| Low-resource | WHO-aligned approaches | Ensure a steroid dose is given | Access to observation and transfer is the limiting factor |
The evidence backbone you should be able to name starts with the Cochrane reviews of glucocorticoids for croup (Russell 2011, updated by Gates 2018), which established that steroids reduce symptom severity, return visits, length of stay and the need for adrenaline across the severity range. The Bjornson 2004 NEJM trial extended the benefit to mild croup, and the Dobrovoljac and Geelhoed Australian data supported the 0.15 mg/kg dexamethasone dose as effective. [3] [4] [5] [6]
For adrenaline, the Cochrane review of nebulised epinephrine (Bjornson 2013) confirmed a real but transient benefit that mandates observation, and the historical Westley 1978 study both introduced nebulised racemic adrenaline and gave us the severity score that still bears the name. The Fernandes 2019 safety review reassures that short-course corticosteroids in young children with acute respiratory illness are safe, supporting the universal-steroid approach. [7] [8] [11]
The live areas of nuance are the choice of steroid preparation and dose (dexamethasone versus prednisolone; 0.15 versus 0.6 mg/kg), the exact observation window after adrenaline, and the recognition that humidified air, once standard, is not supported by the evidence — a good example of guidelines catching up with trials. [1] [10]
Exam Pearls
The single move that keeps children safe is the disciplined one: grade the severity from across the room, give the steroid to everyone, rescue the severe with adrenaline and observe them, and keep a low index of suspicion for the mimics in the toxic or atypical child. [1] [3]
And when you teach croup, teach it as a model of high-value care — a cheap single steroid dose, calm handling, careful observation and clear advice — while never letting the routine of a common illness dull your alertness to the rare child whose airway is failing. [2] [9]
References
- [1]Bjornson CL, Johnson DW. Croup. Lancet, 2008.PMID 18295000
- [2]Bjornson CL, Johnson DW. Croup in children. CMAJ, 2013.PMID 23939212
- [3]Gates A, Gates M, Vandermeer B, et al. Glucocorticoids for croup in children. Cochrane Database Syst Rev, 2018.PMID 30133690
- [4]Russell KF, Liang Y, O'Gorman K, et al. Glucocorticoids for croup. Cochrane Database Syst Rev, 2011.PMID 21249651
- [5]Bjornson CL, Klassen TP, Williamson J, et al. A randomized trial of a single dose of oral dexamethasone for mild croup. N Engl J Med, 2004.PMID 15385657
- [6]Dobrovoljac M, Geelhoed GC. 27 years of croup: an update highlighting the effectiveness of 0.15 mg/kg of dexamethasone. Emerg Med Australas, 2009.PMID 19682017
- [7]Bjornson C, Russell K, Vandermeer B, et al. Nebulized epinephrine for croup in children. Cochrane Database Syst Rev, 2013.PMID 24114291
- [8]Westley CR, Cotton EK, Brooks JG. Nebulized racemic epinephrine by IPPB for the treatment of croup: a double-blind study. Am J Dis Child, 1978.PMID 347921
- [9]Petrocheilou A, Tanou K, Kalampouka E, et al. Viral croup: diagnosis and a treatment algorithm. Pediatr Pulmonol, 2014.PMID 24596395
- [10]Johnson DW. Croup. BMJ Clin Evid, 2014.PMID 25263284
- [11]Fernandes RM, Wingert A, Vandermeer B, et al. Safety of corticosteroids in young children with acute respiratory conditions: a systematic review and meta-analysis. BMJ Open, 2019.PMID 31375615