Paeds · respiratory-sleep-and-airway
Paediatric sleep investigations: polysomnography, sleep-study interpretation and MSLT
Also known as Polysomnography · PSG · Sleep study · Sleep-study interpretation · Apnoea-hypopnoea index · AHI · Obstructive apnoea-hypopnoea index · OAHI · Multiple sleep latency test · MSLT · Overnight oximetry · Sleep-onset REM period · SOREMP
Fellowship guide to paediatric sleep investigations: the polysomnogram that records brain, eye, muscle, airflow, effort, oxygen and carbon dioxide across a night of a child's sleep, the rules that turn those traces into scored events and an apnoea-hypopnoea index, and the multiple sleep latency test that measures daytime sleepiness. The page covers how to choose between attended in-laboratory polysomnography and simpler oximetry or limited studies, how respiratory events are classified as obstructive, central or mixed, how the obstructive apnoea-hypopnoea index grades severity in children rather than adults, how sleep hypoventilation is proven with carbon dioxide, and how the multiple sleep latency test with its sleep-onset REM periods supports a diagnosis of narcolepsy.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent describes a five-year-old who snores every night, stops breathing until she gasps, sleeps restlessly and is impossible in the classroom by mid-morning. The question the sleep study answers is not whether she snores but what her breathing and her brain actually do across a whole night, measured rather than guessed. Polysomnography is that overnight recording: a set of sensors that captures the brain waves, eye movements and muscle tone that stage sleep, alongside the airflow, breathing effort, oxygen and carbon dioxide that reveal how well the child breathes while asleep. [1] [2]
The study earns its status as the reference test because it separates problems that look identical at the bedside. Snoring with obstructive apnoea, snoring without apnoea, central pauses of absent drive, and hypoventilation with a rising carbon dioxide all present as a noisy, unsettled sleeper, yet they demand different treatment. By recording airflow and effort together and adding carbon dioxide, the polysomnogram shows which pattern is present and how severe it is, turning a story into a number that guides the decision to treat. [2] [3]
The multiple sleep latency test answers a different question entirely: not how a child breathes at night but how sleepy she is by day and why. Performed the day after an overnight study, it offers a series of scheduled nap opportunities and times how quickly the child falls asleep and whether she drops straight into rapid-eye-movement sleep. A short latency with repeated sleep-onset rapid-eye-movement periods is the objective signature of narcolepsy, provided the overnight study first excluded simple sleep deprivation or untreated apnoea as the cause. [5] [9]
Classification
Think of the choice of sleep investigation as a ladder from the most complete test to the simplest, and match the rung to the question and the child. Attended in-laboratory polysomnography sits at the top as the reference standard because a technologist watches, the full montage records brain and breathing together, and the study can be salvaged if a sensor fails. Below it lie unattended full studies, limited cardiorespiratory studies without brain channels, and overnight oximetry alone, each cheaper and easier but each blind to more of the picture. [3] [4]
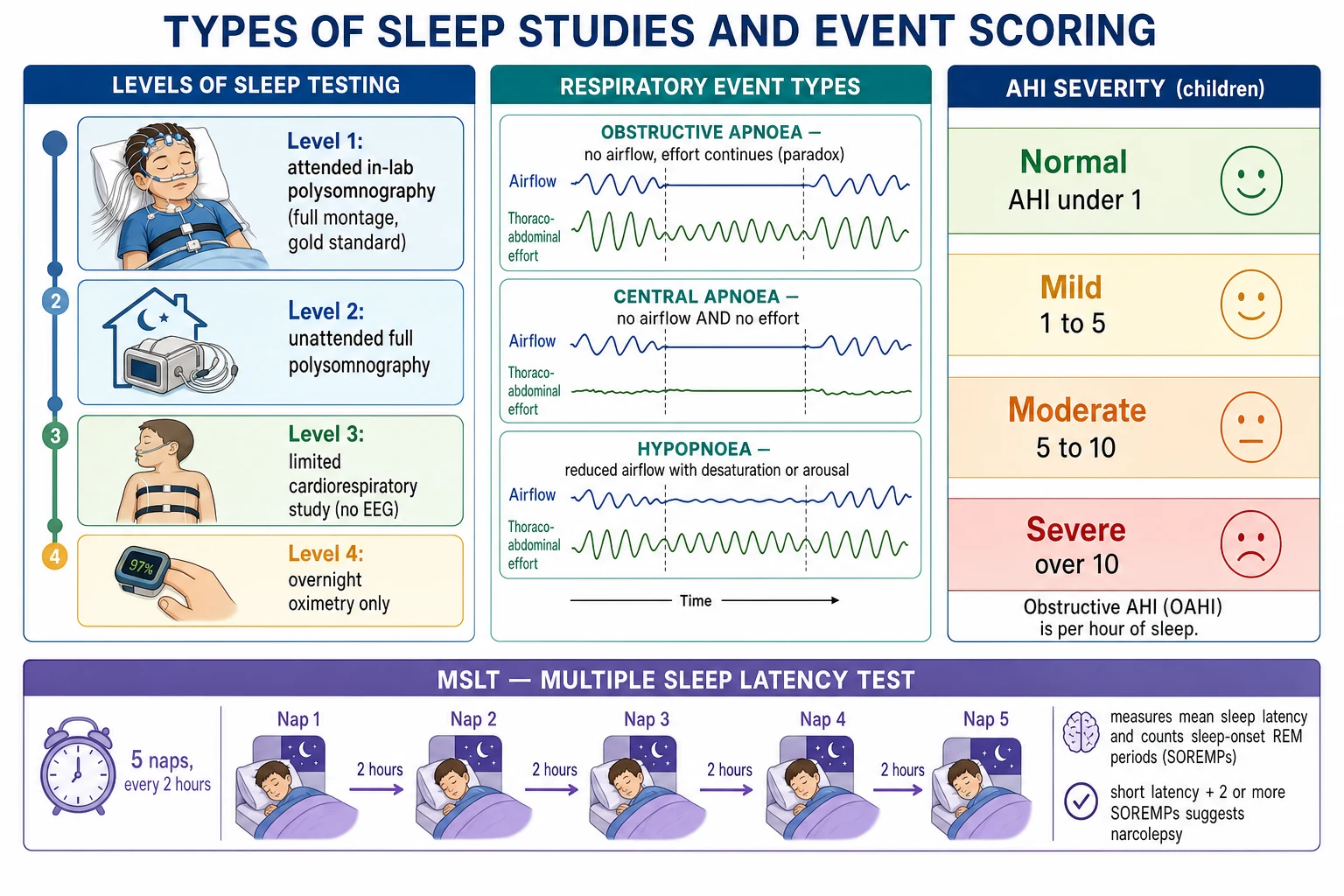
Once a full study is recorded, its events are classified by what airflow and effort do together, because that distinction decides the treatment. An obstructive apnoea shows airflow ceasing while the chest and abdomen keep struggling, often moving paradoxically against a closed airway; a central apnoea shows airflow and effort stopping together because there is no drive; and a mixed event begins central and ends obstructive. A hypopnoea is a partial event, a fall in airflow accompanied by a desaturation or an arousal rather than a complete stop. [7] [2]
Obstructive event
- Airflow falls or stops but effort continues
- Paradoxical chest and abdomen movement, snoring
- Ends with an arousal and a resumed breath
- Points to adenotonsillar or airway obstruction
Central event
- Airflow AND effort stop together: no drive
- No paradox, no snore during the pause
- Think brainstem, prematurity, opioid, heart failure
- Effort belts and capnography make the call
Hypopnoea (partial)
- Airflow reduced, not absent
- Requires linked desaturation or arousal to score
- Classified obstructive or central by effort pattern
- Counts toward the apnoea-hypopnoea index
The apnoea-hypopnoea index then grades severity, and the crucial teaching point is that children are scored against paediatric, not adult, thresholds. In a child an obstructive apnoea-hypopnoea index above one event per hour of sleep is already abnormal, with rough bands of mild, moderate and severe disease guiding treatment, whereas an adult is not considered to have disease until five events per hour. Using the adult cut-off in an adolescent understates real disease, a mismatch shown directly when the two scoring rules are applied to the same recordings. [6] [2]
Epidemiology & Risk Factors
Sleep-disordered breathing is common in childhood, with habitual snoring reported in roughly one in ten children and obstructive sleep apnoea confirmed on polysomnography in a smaller but substantial few per cent, which is why the demand for sleep studies far outstrips the supply of laboratory beds. The peak of obstructive disease falls in the preschool years when the tonsils and adenoids are largest relative to the airway, and a second wave arrives in adolescence driven by obesity. This mismatch between need and capacity shapes every service's rationing of the reference test. [1] [12]
The children most likely to need and to benefit from a formal study cluster in recognisable groups. Adenotonsillar hypertrophy, obesity, craniofacial anomalies such as midface hypoplasia and micrognathia, Down syndrome, neuromuscular disease and the mucopolysaccharidoses all raise the pre-test probability of significant sleep-disordered breathing and often justify polysomnography before surgery. Prematurity, brainstem lesions and syndromes affecting the control of breathing raise the probability of central events and hypoventilation instead. [2] [3]
Daytime sleepiness has its own epidemiology that steers the child toward a different test. Narcolepsy, the main reason to perform a multiple sleep latency test in a child, typically declares itself in later childhood and adolescence, often with cataplexy, and is under-recognised for years. Because insufficient sleep, delayed sleep phase and untreated night-time apnoea are far commoner causes of a sleepy teenager, the multiple sleep latency test is only meaningful after those have been addressed and documented. [9] [8]
Pathophysiology
To read a sleep study you must first understand what the machine is watching. Sleep is not uniform: the electroencephalogram, eye-movement and chin-muscle channels divide the night into non-rapid-eye-movement stages of progressively deeper sleep and rapid-eye-movement sleep, in which the brain is active, the muscles are atonic and dreaming occurs. Obstructive events cluster in rapid-eye-movement sleep because the loss of muscle tone collapses an already vulnerable airway, so a study that captured little rapid-eye-movement sleep may underestimate disease. [1] [12]
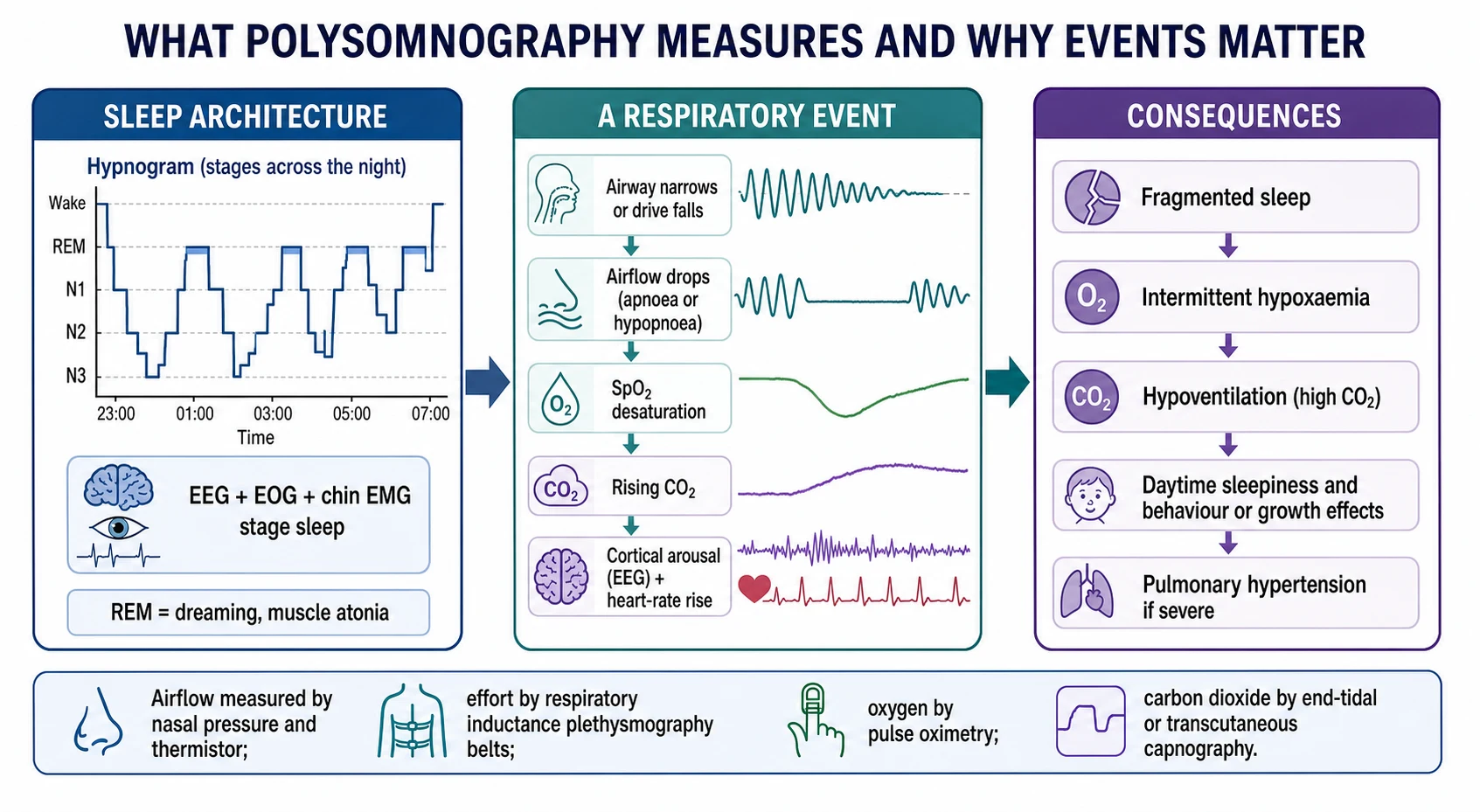
A respiratory event is a small physiological cascade that the study records channel by channel. The airway narrows or the drive to breathe falls, so airflow at the nose drops; the oxygen saturation dips a beat later as the lungs stop refreshing the blood; the carbon dioxide climbs because it is no longer being cleared; and the brain rescues the child with a brief cortical arousal and a surge in heart rate that reopens the airway. Reading these signals in register is exactly how a scorer decides whether an event happened and what type it was. [7] [2]
The reason events matter is the harm they do when repeated hundreds of times a night. Fragmented sleep from constant arousals produces daytime sleepiness, inattention and behavioural disturbance; intermittent hypoxaemia and the swings in intrathoracic pressure strain the cardiovascular system and, when severe, drive pulmonary hypertension; and sustained hypoventilation, marked by a carbon dioxide that stays high rather than dipping transiently, injures the child through chronic hypercapnia. The study quantifies each of these harms through the arousal index, the oxygen nadir and the carbon dioxide summary. [12] [1]
Daytime sleepiness has its own mechanism that the multiple sleep latency test exploits. In narcolepsy the loss of hypocretin-producing neurons destabilises the boundary between wake and rapid-eye-movement sleep, so the child not only falls asleep abnormally fast but slips almost immediately into rapid-eye-movement sleep. The nap test makes this visible by measuring how short the sleep latency is and by counting how often rapid-eye-movement sleep appears at sleep onset. [9] [8]
Clinical Presentation
The presentations that bring a child to a sleep study fall into two broad stories, and knowing which one you are in decides which test to order. The night-time story is of noisy, obstructed breathing: habitual snoring, witnessed pauses that end in a gasp or snort, restless sleep with unusual postures and sweating, mouth-breathing and sometimes secondary enuresis. This picture, especially with large tonsils, points toward obstructive sleep apnoea and toward an overnight study to confirm and grade it. [1] [2]
The daytime story is of sleepiness or its behavioural mask. Younger children more often show hyperactivity, irritability, poor concentration and impaired school performance than obvious drowsiness, so a "difficult" child can be a tired one. Older children and adolescents may describe frank excessive daytime sleepiness, unrefreshing sleep and, in narcolepsy, sudden sleep attacks and cataplexy. When sleepiness dominates and is not explained by short or disrupted sleep, the investigation shifts toward the multiple sleep latency test. [9] [8]
Certain presentations demand a study rather than a trial of treatment. A child being considered for adenotonsillectomy who has obesity, a craniofacial or neuromuscular condition, Down syndrome or a discrepancy between mild-looking tonsils and severe symptoms benefits from pre-operative polysomnography to confirm the diagnosis and gauge the peri-operative risk. A child with a suspected disorder of the control of breathing, or with neuromuscular weakness, presents with hypoventilation that only a study with carbon dioxide will reveal. [2] [10]
Differential Diagnosis
The first differential the study resolves is why a child is a poor sleeper or a poor breather at night. Primary snoring without significant apnoea, obstructive sleep apnoea, central sleep apnoea and sleep-related hypoventilation all produce disturbed nights but need different responses, and only the simultaneous recording of airflow, effort and carbon dioxide reliably distinguishes them. A limited study or oximetry can suggest the answer but cannot separate these confidently, which is why a negative simple test never overrules a strong clinical story. [4] [2]
Obstructive sleep apnoea
- Snoring, witnessed apnoea, effortful obstructed breaths
- Obstructive events dominate; worse in REM
- Graded by the obstructive apnoea-hypopnoea index
- Often adenotonsillar or obesity-related
Central or hypoventilation
- Central pauses with no effort, or a high sleep carbon dioxide
- Little snoring; child may not look distressed
- Needs effort belts and capnography to detect
- Think brainstem, neuromuscular, prematurity
Daytime sleepiness
- Insufficient sleep and delayed sleep phase first
- Untreated apnoea before labelling narcolepsy
- Multiple sleep latency test, not overnight AHI
- Short latency plus 2 or more SOREMPs in narcolepsy
The second differential concerns the sleepy child, and here the danger is mislabelling. Insufficient sleep from late nights and early school starts, a delayed sleep phase in an adolescent whose clock runs late, and untreated night-time apnoea are all commoner than narcolepsy and all cause daytime sleepiness. Each must be identified and corrected, with the recent sleep pattern documented, before a multiple sleep latency test is interpreted, because sleep deprivation itself shortens the sleep latency and can even produce sleep-onset rapid-eye-movement periods. [5] [9]
A third set of pitfalls are technical mimics that masquerade as disease or as health. A study with too little total sleep or too little rapid-eye-movement sleep can miss obstructive disease, artefactual signal loss can be misread as apnoea, and a periodic breathing pattern normal for a young infant can be over-interpreted. Recognising an inadequate or artefact-laden study, and repeating it when the clinical suspicion is high, is part of the diagnostic discipline. [3] [4]
Clinical & Bedside Assessment
Before any study, the bedside assessment does the work of choosing the right test and interpreting its result. A focused sleep history quantifies the snoring, the witnessed pauses, the restlessness and the daytime consequences, and screens for the daytime sleepiness, cataplexy and disrupted schedule that point instead toward hypersomnolence. Growth is charted, since both failure to thrive and obesity accompany sleep-disordered breathing, and a sleep diary or actigraphy over one to two weeks documents how much the child actually sleeps. [1] [9]
The examination looks for the causes and the consequences that the study will corroborate. Enlarged tonsils, adenoidal facies and mouth-breathing suggest upper-airway obstruction; a crowded oropharynx, retrognathia or midface hypoplasia point to craniofacial contributors; and obesity, hypotonia or neuromuscular weakness broaden the differential toward hypoventilation. Signs of the downstream harm — systemic or pulmonary hypertension, a loud pulmonary second sound or right heart strain — raise the urgency and the pre-test probability of severe disease. [2] [12]
For the sleepy child specifically, the bedside preparation determines whether a multiple sleep latency test can even be interpreted. The two weeks beforehand should show adequate, regular sleep on the diary or actigraphy, rapid-eye-movement-suppressing drugs such as many antidepressants should have been withdrawn where safe, and the immediately preceding overnight study should confirm at least six hours of sleep and exclude another cause. Only then does a short nap latency with sleep-onset rapid-eye-movement periods carry its narcolepsy meaning. [5] [8]
Investigations
Attended in-laboratory polysomnography is the definitive investigation, and its value lies in recording everything at once so that events can be typed and quantified. The standard montage stages sleep with the electroencephalogram, electro-oculogram and chin electromyogram, and measures breathing with nasal pressure and thermistor airflow, chest and abdominal effort belts, pulse oximetry, carbon dioxide and the electrocardiogram, usually with synchronised video and leg electromyography. From these the scorer derives the apnoea-hypopnoea index, the obstructive and central event counts, the oxygen nadir, the arousal index and the carbon dioxide summary. [3] [1]
The carbon dioxide channel deserves its own emphasis because it detects a problem oxygen saturation misses. Sleep hypoventilation is defined by a carbon dioxide that stays elevated for a substantial proportion of sleep rather than dipping in discrete events, and it is the hallmark of central, neuromuscular and syndromic sleep-disordered breathing. A study without capnography can therefore report a normal saturation while missing dangerous hypoventilation, which is why carbon dioxide monitoring is built into the standard paediatric montage and into home studies for at-risk children. [10] [7]
When laboratory polysomnography is unavailable, simpler tests are used with their limitations understood. Overnight oximetry and limited cardiorespiratory studies can confirm significant obstructive disease when clearly positive, and home polysomnography with transcutaneous carbon dioxide performs well in selected children such as those with neuromuscular disease, but a negative simple study does not exclude apnoea in a symptomatic child. Where obstruction persists after adenotonsillectomy or the site of collapse is unclear, drug-induced sleep endoscopy visualises the dynamic airway to direct further surgery. [4] [11]
The multiple sleep latency test is the key investigation for the sleepy child, performed the day after an adequate overnight study. It offers four to five nap opportunities at two-hourly intervals and measures the mean time to fall asleep and the number of naps that reach rapid-eye-movement sleep. A short mean sleep latency with two or more sleep-onset rapid-eye-movement periods, one of which may come from the preceding night, supports narcolepsy, but only once sleep deprivation, circadian disorders and rapid-eye-movement-suppressing drugs have been excluded. [5] [9]
Management — Resuscitation
Most sleep investigations are elective, but the report can reveal physiology that needs immediate action rather than a clinic letter. A study showing severe desaturation, prolonged apnoeas, marked hypercapnia or evidence of cor pulmonale identifies a child who should not wait months for treatment, and the finding is escalated the same day to arrange urgent airway or ventilatory support. The principle mirrors acute care everywhere: treat the physiology the study exposes, not the position in the outpatient queue. [2] [1]
Where hypoventilation rather than obstruction is the danger, the resuscitative principle is to support ventilation rather than merely oxygenate. A child with neuromuscular weakness or a central disorder whose study reveals a sustained high carbon dioxide needs assisted ventilation that clears carbon dioxide, with supplemental oxygen added only on top of adequate ventilation, because oxygen alone can normalise the saturation while the carbon dioxide climbs. Continuous carbon dioxide monitoring, not the pulse oximeter alone, guides the adequacy of that support. [10] [7]
Around any acute intervention, the study itself informs safety. A child with severe obstructive sleep apnoea is at heightened risk of airway compromise and opioid sensitivity around anaesthesia and adenotonsillectomy, so a severe pre-operative study prompts inpatient post-operative monitoring rather than day-case discharge. Recognising this from the report prevents the avoidable respiratory deterioration that can follow surgery in the most affected children. [1] [2]
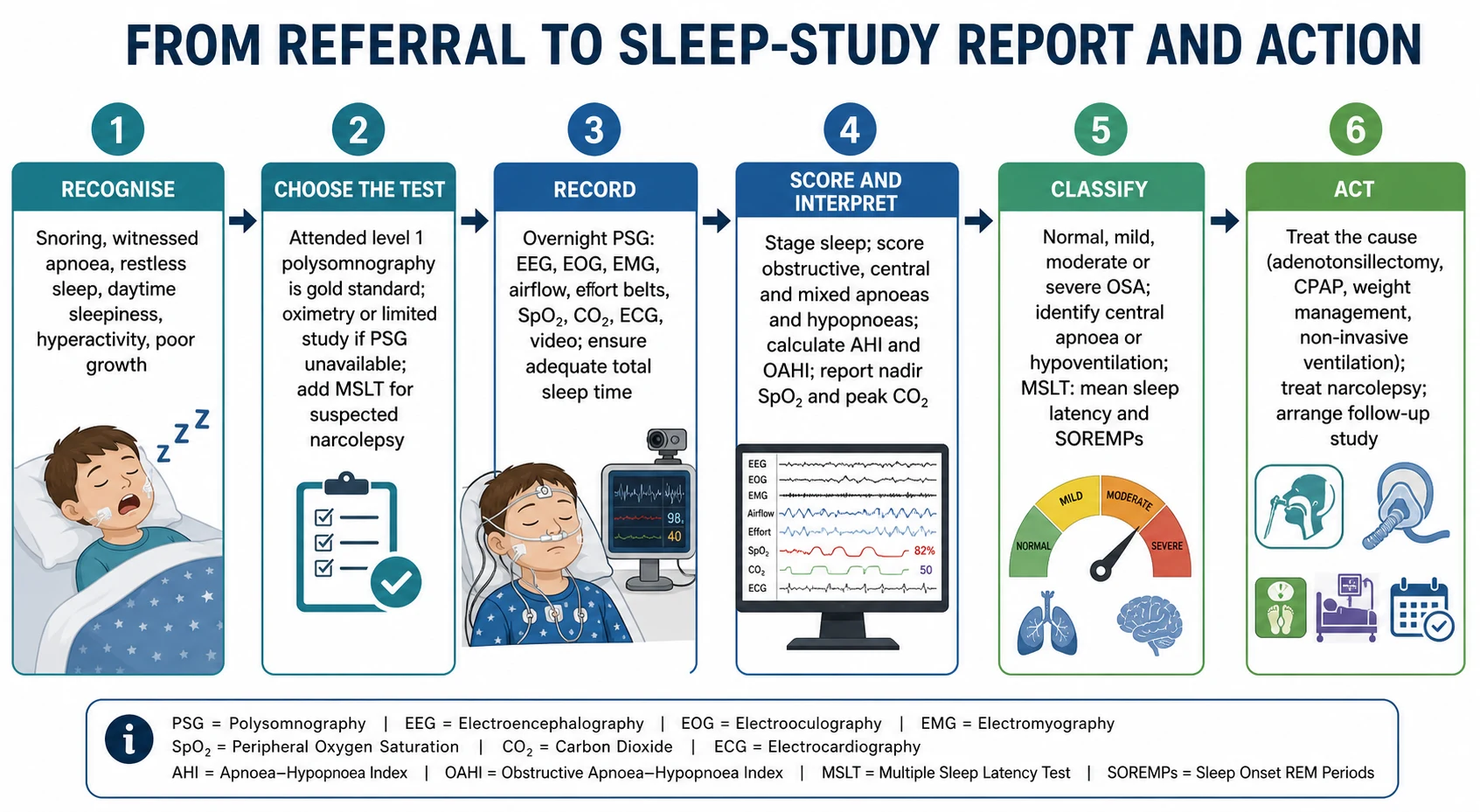
Management — Definitive & Stepwise
The definitive value of a sleep study is that it converts a symptom into a graded diagnosis that directs a specific treatment. The report is read in a fixed order — confirm the study was adequate, classify the events as obstructive, central or hypoventilation, grade the severity, and note the oxygen and carbon dioxide load — and that reading points to the corresponding pathway. The figure sets out this journey from recognising the child at the bedside through choosing and recording the test to acting on the interpreted result. [2] [3]
For confirmed obstructive sleep apnoea the study grades the response. Adenotonsillectomy is the first-line treatment where adenotonsillar hypertrophy is the driver, and the severity on the pre-operative study predicts both the likelihood of cure and the peri-operative risk. Continuous positive airway pressure treats residual or non-surgical obstruction and is titrated, ideally on a study, to the pressure that abolishes events. Weight management, intranasal corticosteroids for milder disease, and orthodontic or craniofacial approaches fill out the ladder, with a follow-up study confirming resolution in children who had severe disease or persistent symptoms. [1] [2]
For the sleepy child, the multiple sleep latency test result drives management once mimics are excluded. A confirmed narcolepsy is managed with scheduled naps and sleep hygiene alongside pharmacological treatment of the sleepiness and any cataplexy, following disorder-of-hypersomnolence guidance, and with attention to the psychosocial and school impact of a lifelong condition. When the test instead points to insufficient sleep or a delayed sleep phase, the treatment is behavioural and circadian rather than a stimulant, underlining why the test is interpreted so carefully. [8] [9]
Specific Subtypes & Scenarios
The pre-operative adenotonsillectomy assessment is the commonest scenario in which a study changes practice. Guidelines recommend polysomnography before surgery in children whose risk or complexity is raised — those with obesity, Down syndrome, craniofacial or neuromuscular conditions, or a mismatch between symptoms and tonsil size — because the study confirms the diagnosis, grades severity to plan peri-operative monitoring, and provides a baseline against which to judge the need for a post-operative study. [2] [1]
The child with neuromuscular disease or a syndrome affecting the control of breathing is the scenario where carbon dioxide, not the apnoea-hypopnoea index, is the key output. In Duchenne muscular dystrophy, spinal muscular atrophy, the mucopolysaccharidoses and similar conditions, nocturnal hypoventilation appears before daytime respiratory failure, and a study with capnography detects it and triggers non-invasive ventilation. Home polysomnography with transcutaneous carbon dioxide is a validated option that brings the test to children for whom a laboratory night is difficult. [10] [7]
The sleepy adolescent evaluated for narcolepsy is the defining multiple sleep latency test scenario. The sequence is fixed: document adequate sleep for two weeks, withdraw rapid-eye-movement-suppressing drugs where safe, perform an adequate overnight study to exclude apnoea and confirm sufficient sleep, then run the nap test the next day. A short mean sleep latency with two or more sleep-onset rapid-eye-movement periods supports narcolepsy, corroborated where needed by cataplexy and cerebrospinal fluid hypocretin. [5] [9]
Complications & Pitfalls
The complications of getting the investigation wrong are complications of the underlying disease left untreated. A missed or underestimated obstructive sleep apnoea allows the neurocognitive, behavioural, growth and cardiovascular harms to continue, and missed hypoventilation permits chronic hypercapnia and its consequences. Because access to laboratory studies is limited, the pressure to rely on simpler tests is real, and the corresponding risk is a false-negative simple study that falsely reassures in a symptomatic child. [4] [12]
The interpretive pitfalls cluster around a few recurring errors. Applying adult apnoea-hypopnoea index thresholds to a child understates disease; trusting a study with too little total or rapid-eye-movement sleep as representative underestimates obstruction; reading a normal saturation as normal ventilation misses hypoventilation when carbon dioxide was not recorded; and mislabelling central events as obstructive, or the reverse, sends the child down the wrong treatment road. Each is avoided by a disciplined, checklist-driven reading of the report. [6] [7]
The multiple sleep latency test carries its own characteristic pitfalls. Performing it on a sleep-deprived child, or one on a rapid-eye-movement-suppressing antidepressant, or without a preceding overnight study to exclude apnoea and confirm sleep, produces uninterpretable or falsely positive results, since sleep debt alone shortens the latency and can generate sleep-onset rapid-eye-movement periods. Interpreting the test outside these conditions is the classic way to over-diagnose narcolepsy. [5] [8]
Prognosis & Disposition
The prognosis attached to a sleep study is really the prognosis of the condition it diagnoses, made better by the accuracy of the diagnosis. Obstructive sleep apnoea from adenotonsillar hypertrophy often resolves with surgery, and the pre-operative study both predicts the response and flags the children who need a follow-up study to confirm cure, particularly those with severe disease, obesity or complex comorbidity. Untreated, the same disease carries measurable neurocognitive, behavioural and cardiovascular costs, which is the case for investigating and treating it properly. [1] [12]
For central and hypoventilation disorders detected on a study, the disposition is a structured, often lifelong programme of ventilatory support and surveillance rather than a single procedure. These children move into home ventilation pathways with regular re-studies to adjust support as they grow, and the sleep study becomes a repeated monitoring tool rather than a one-off diagnostic test. The prognosis improves markedly when hypoventilation is detected early by capnography and supported before organ injury accrues. [10] [7]
Narcolepsy diagnosed by the multiple sleep latency test is a lifelong condition, but one whose prognosis is substantially improved by recognition and treatment. Scheduled naps, good sleep hygiene, pharmacological control of sleepiness and cataplexy, and support at school allow most young people to function well, and making the diagnosis correctly — neither missed for years nor over-called in a sleep-deprived teenager — is what determines whether that support arrives. Disposition is to ongoing sleep-medicine follow-up. [8] [9]
Special Populations
Children with Down syndrome are a population in whom sleep-disordered breathing is so common, and clinical prediction so poor, that guidelines recommend a screening polysomnogram regardless of symptoms in the early years. Midface hypoplasia, glossoptosis, hypotonia and obesity combine to produce obstruction that parents often do not report, and a study frequently uncovers significant disease in a child thought to be sleeping well. The same logic of low clinical predictive value applies to other craniofacial syndromes. [2] [1]
Children with neuromuscular disease and technology dependence are the population for whom carbon dioxide monitoring and repeated studies matter most. Nocturnal hypoventilation is the earliest sign of respiratory decline in conditions such as Duchenne muscular dystrophy and spinal muscular atrophy, and serial studies with capnography guide the timing and titration of non-invasive ventilation. Home polysomnography with transcutaneous carbon dioxide extends access for children for whom travel to a laboratory is burdensome or medically difficult. [10] [7]
Access and equity shape sleep investigation for infants, for rural and remote families and for Indigenous communities. Infants require specialised scoring and interpretation because their sleep and breathing differ from older children, laboratory beds are scarce everywhere, and long distances make an in-laboratory night impractical for many families, widening reliance on home and limited studies. Building equitable pathways — validated home testing, telehealth review and prioritised access for the highest-risk children — is an explicit service responsibility rather than an afterthought. [4] [10]
Evidence, Guidelines & Regional Differences
The framework for paediatric sleep investigation rests on a small number of authoritative documents. The American Academy of Pediatrics clinical practice guideline positions polysomnography as the reference standard for diagnosing childhood obstructive sleep apnoea and sets the diagnostic and management approach, while the European Respiratory Society statement provides a complementary, staged diagnostic pathway for obstructive sleep-disordered breathing in two- to eighteen-year-olds. Together they anchor the indications, the interpretation and the treatment thresholds used internationally. [1] [2]
The technical rules and indications come from the American Academy of Sleep Medicine. Its practice parameters and evidence review define the respiratory indications for polysomnography in children, its parameters for non-respiratory indications set out when and how to perform the multiple sleep latency test, and its scoring manual and validation studies establish the paediatric event definitions and the reason paediatric rather than adult thresholds must be used. The guideline on central disorders of hypersomnolence frames the diagnosis and treatment of narcolepsy that the nap test supports. [3] [5] [8]
Regional differences are practical rather than conceptual. The definitions of events, the paediatric thresholds and the indications are broadly consistent across guidelines, but access to attended in-laboratory polysomnography, to carbon dioxide monitoring, to the multiple sleep latency test and to drug-induced sleep endoscopy varies widely between and within countries. In Australia and New Zealand, as elsewhere, studies are concentrated in tertiary paediatric centres, waiting lists are long, and validated home and limited studies plus telehealth interpretation are increasingly used to extend equitable access to rural, remote and Indigenous families. [10] [4]
Exam Pearls
Hold the framework for the viva in one breath: choose the test from the question, where an overnight polysomnogram answers a breathing problem and a multiple sleep latency test answers a sleepiness problem, then read the study in a fixed order — adequacy, event type, severity, and oxygen and carbon dioxide load. Attended in-laboratory polysomnography is the reference standard, a negative simple study never overrules a strong clinical story, and carbon dioxide, not saturation, is what proves hypoventilation. [1] [3]
State the numbers correctly, because examiners test them. In a child an obstructive apnoea-hypopnoea index above one event per hour is abnormal, unlike the adult cut-off of five. An obstructive event shows airflow absent but effort continuing, a central event shows airflow and effort absent together, and a hypopnoea is a partial fall in airflow with a desaturation or arousal. Sleep hypoventilation is a sustained high carbon dioxide, not a transient dip. On the multiple sleep latency test, a short mean sleep latency with two or more sleep-onset rapid-eye-movement periods supports narcolepsy. [6] [7] [5]
The high-yield pairings do the exam's work. Snoring with large tonsils and an abnormal obstructive index points to adenotonsillectomy; a normal saturation with a rising carbon dioxide points to hypoventilation and non-invasive ventilation, never oxygen alone; a sleepy teenager needs insufficient sleep, delayed sleep phase and apnoea excluded before the nap test is believed; and a complex or high-risk child — Down syndrome, obesity, neuromuscular disease — needs a study before adenotonsillectomy and post-operative monitoring. Read the study, then treat the child. [2] [8] [10]
References
- [1]Marcus CL; Brooks LJ; Draper KA; et al Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics, 2012.PMID 22926173
- [2]Kaditis AG; Alonso Alvarez ML; Boudewyns A; et al Obstructive sleep disordered breathing in 2- to 18-year-old children: diagnosis and management. Eur Respir J, 2016.PMID 26541535
- [3]Aurora RN; Zak RS; Karippot A; et al Practice parameters for the respiratory indications for polysomnography in children. Sleep, 2011.PMID 21359087
- [4]Wise MS; Nichols CD; Grigg-Damberger MM; et al Executive summary of respiratory indications for polysomnography in children: an evidence-based review. Sleep, 2011.PMID 21359088
- [5]Aurora RN; Lamm CI; Zak RS; et al Practice parameters for the non-respiratory indications for polysomnography and multiple sleep latency testing for children. Sleep, 2012.PMID 23115395
- [6]Accardo JA; Shults J; Leonard MB; et al Differences in overnight polysomnography scores using the adult and pediatric criteria for respiratory events in adolescents. Sleep, 2010.PMID 21061855
- [7]Berry RB; Ryals S; Wagner MH Use of Chest Wall EMG to Classify Hypopneas as Obstructive or Central. J Clin Sleep Med, 2018.PMID 29734977
- [8]Maski K; Trotti LM; Kotagal S; et al Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med, 2021.PMID 34743789
- [9]Kotagal S; Chopra A Pediatric sleep-wake disorders. Neurol Clin, 2012.PMID 23099134
- [10]Withers A; Pettigrew G; Filmer K; et al Comparing home polysomnography with transcutaneous CO2 monitoring to laboratory polysomnography in children with neuromuscular disorders. J Clin Sleep Med, 2025.PMID 39663926
- [11]Kirkham EM Pediatric Drug-Induced Sleep Endoscopy. Otolaryngol Clin North Am, 2022.PMID 36371133
- [12]Jadhav U; Bhanushali J; Sindhu A; et al A Comprehensive Review of Pediatric Obstructive Sleep Apnea: From Assessment to Intervention. Cureus, 2025.PMID 40013169