Paeds · rheumatology-musculoskeletal-and-sports
Back pain in children and adolescents
Also known as paediatric back pain · low back pain in children · spondylolysis · pars interarticularis stress fracture · Scheuermann kyphosis · Scheuermann disease · juvenile kyphosis · discitis · spondylodiscitis · spondylolisthesis · Adams forward bend test
A fellowship approach to back pain in children and adolescents: back pain is uncommon in the pre-school child and a red flag in its own right, and the age-stratified differential runs from discitis in the toddler through spondylolysis in the school-age athlete to Scheuermann kyphosis and lumbar disc herniation in the adolescent — anchored by the red-flag screen that separates the benign mechanical back from the infection, tumour, or neurological compromise that demands urgent imaging and referral.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
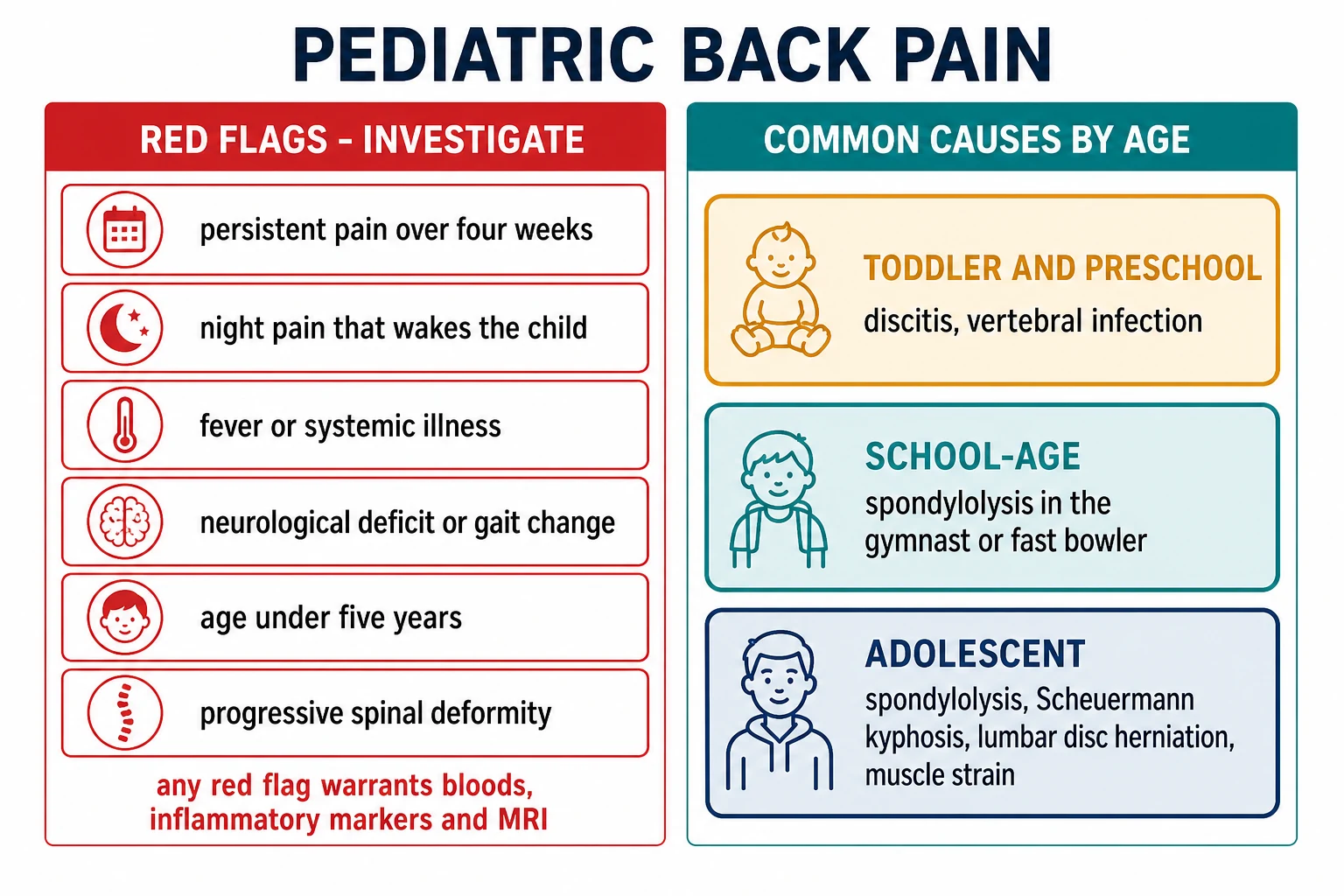
A four-year-old boy refuses to walk and points to his lower back, he is febrile and irritable, and his inflammatory markers are raised — discitis, the classic cause of back pain in the toddler and pre-school child. A thirteen-year-old female gymnast has three weeks of low back pain that worsens with backbends and eases with rest — spondylolysis, a stress fracture of the pars interarticularis that is the commonest identifiable cause of low back pain in the young athlete. A fifteen-year-old boy has an increasing rounded upper-back deformity with an aching thoracic spine that his mother first noticed a year ago — Scheuermann kyphosis, a structural wedging of the vertebral bodies. The task in each is to screen for the red flag, choose the imaging, and separate the diagnosis that needs urgent referral from the one that needs activity modification and follow-up. [1] [9]
The five moves — Screen, Localise, Image, Treat, Follow-up
Overview & Definition
Back pain in children and adolescents is the symptom that most reliably separates the careful clinician from the complacent one, because the paediatric back behaves nothing like the adult back. In adults, low back pain is overwhelmingly mechanical and benign, and the default is reassurance. In children, the opposite holds: back pain is comparatively uncommon, and when it is persistent or severe it carries a much higher probability of an identifiable organic cause. The fellowship candidate holds the two truths at once — most back pain in adolescents is mechanical and self-limiting, but back pain in the younger child, or with any red flag, is a diagnosis waiting to be found. [1] [2]
The red flag is the central concept. A red flag is a clinical feature that raises the probability of a serious underlying cause — infection, tumour, inflammatory disease, fracture, or neurological compromise — to a level that demands investigation rather than observation. The recognised red flags for paediatric back pain are constant or night pain, fever and systemic symptoms, weight loss, neurological deficit or a gait change, age under five years, a progressive or painful deformity, and persistence of the pain beyond roughly four weeks. The absence of every red flag allows the conservative management of a presumed mechanical back; the presence of even one redirects the workup. [1] [11]
The clinical importance comes from what an unrecognised spinal tumour or a discitis does to a child. A vertebral osteosarcoma or an Ewing sarcoma presents with night pain that is dismissed as growing pains, and the delay narrows the window for curative treatment. A discitis in the toddler erodes the disc and the adjacent vertebral endplates and, untreated, leaves a residual deformity. A spondylolysis that is loaded through a competitive season progresses from a stress reaction to a complete pars fracture that may not unite. The fellowship task is to apply the red-flag screen, choose the right imaging, and refer the serious cause early. [3] [7]
Classification
Paediatric back pain is classified along two axes that together drive the differential and the imaging strategy. The first axis is the presence or absence of a red flag: a red-flag back pain points toward infection, tumour, inflammatory disease, fracture, or neurological compromise and demands urgent investigation, while a non-red-flag back pain in an older child points toward a mechanical or developmental cause managed conservatively with a safety-net. The second axis is age, because the differential changes sharply with the developmental stage, and the age at onset is the single most powerful single classifier at the bedside. [1] [11]
The age axis runs from the toddler to the young adult. In the toddler and pre-school child, aged under five years, back pain is uncommon and an organic cause is sought by default — discitis and vertebral infection dominate, with tumour and leukaemia the feared mimics. In the school-age child, aged five to ten years, spondylolysis enters as the athletic child begins organised sport, and discitis is still a consideration at the younger end of the band. In the adolescent, aged ten to eighteen years, the differential broadens to spondylolysis, Scheuermann kyphosis, lumbar disc herniation, spondylolisthesis, and the mechanical muscle-strain back that is the commonest overall explanation. [9] [10]
The mechanism axis further refines the differential within each age band. An extension-related pain in the athlete points to the posterior element stress of spondylolysis. A flexion-related pain with radiculopathy points to a lumbar disc herniation. A progressive postural deformity that does not correct on extension points to the structural kyphosis of Scheuermann disease. A febrile, irritable young child who refuses to walk points to the disc-space infection of discitis. The fellowship answer names the mechanism aloud and uses it to choose the imaging. [5] [8]
Epidemiology & Risk Factors
Back pain becomes steadily more common through childhood and adolescence, and the age-related rise is the epidemiological fact that underpins the red-flag rule. Surveys of school-age children show a prevalence that climbs from a few per cent in the pre-school years to roughly a third of adolescents, and the rise mirrors the increasing mechanical load, the growth spurt, and the organised sport of the teenage years. The corollary is that back pain is uncommon in the young child, and its presence at that age is a red flag in its own right. [1] [2]
The risk factors for an identifiable organic cause cluster around the clinical picture and the activity. The young age, the systemic features of fever and weight loss, the night pain, and the neurological deficit are the individual red-flag risk factors. The repetitive lumbar extension of gymnastics, cricket fast bowling, dance, and the throwing and kicking sports is the risk factor for spondylolysis, and the bilateral pars defect is the risk factor for progression to spondylolisthesis. A high body mass index and deconditioning are the risk factors for the mechanical back, and the male sex and the adolescent growth spurt are the risk factors for Scheuermann kyphosis. [9] [5]
The serious causes are individually uncommon but collectively demand the vigilance this topic teaches. Discitis peaks in the toddler and pre-school years and is the commonest spinal infection of childhood. Spondylolysis is found in roughly one in twenty of the general adolescent population and in a substantially higher proportion of young athletes in extension-loading sports. Scheuermann kyphosis affects roughly one to eight per cent of adolescents, with a male predominance. The vertebral and paraspinal tumours — osteosarcoma, Ewing sarcoma, and leukaemia — are rare but are the diagnoses that the red-flag screen exists to catch. [3] [6]
Pathophysiology
The pathophysiology of paediatric back pain is best understood by the tissue that is diseased, because each tissue generates a distinct clinical pattern and a distinct imaging strategy. The pars interarticularis, the vertebral body and its growth plate, the intervertebral disc, and the neural elements each produce their own pain, and the focused examination seeks the affected tissue through the mechanism of the pain, the site of the tenderness, and the neurological signs. [3] [10]
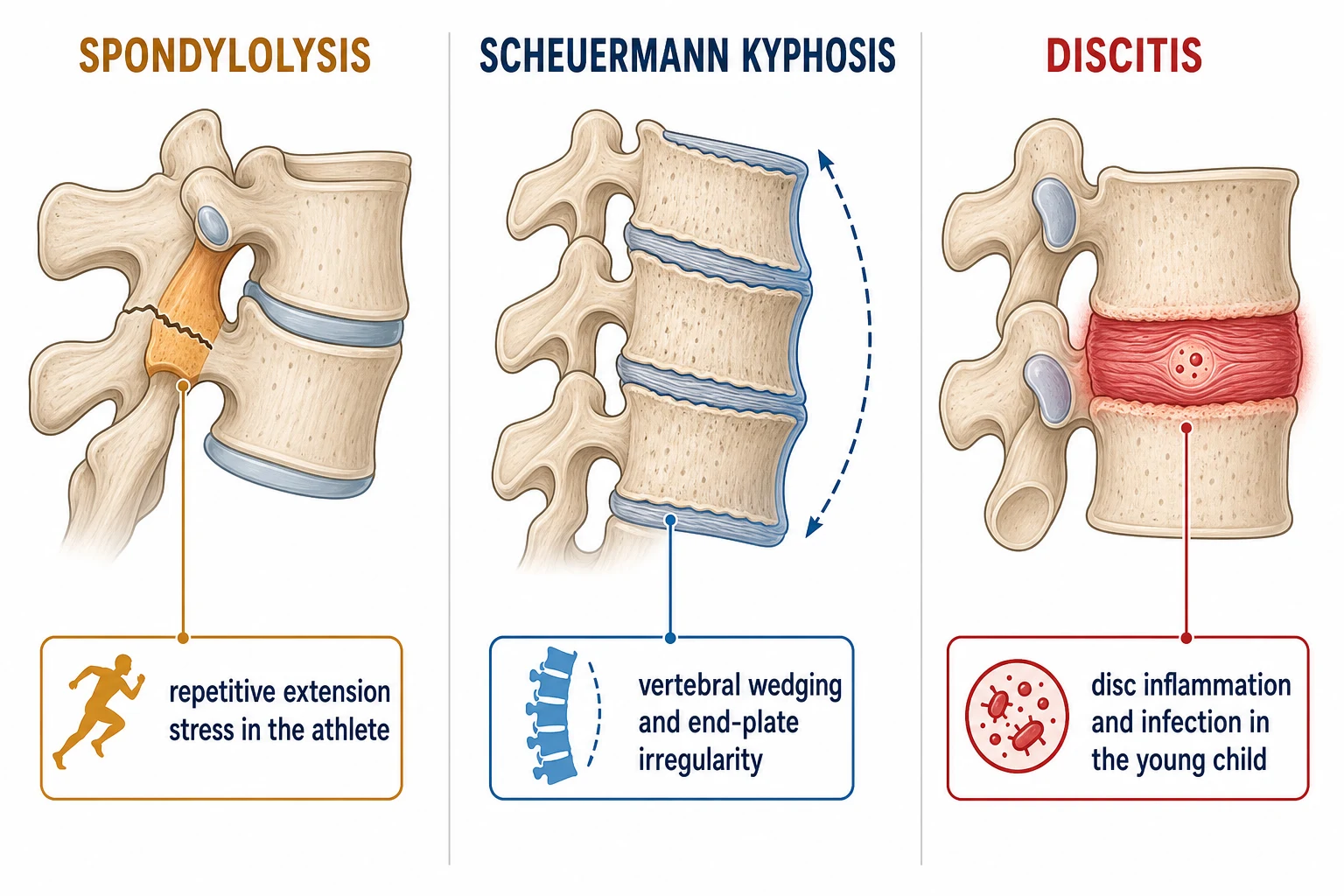
Spondylolysis is a fatigue fracture of the pars interarticularis, the small bridge of bone that connects the superior and the inferior articular facets of a vertebra. The pars is loaded in extension, and the repetitive hyperextension of gymnastics, fast bowling, dance, and the throwing sports concentrates stress at the L4 and L5 levels. The lesion progresses along a continuum from a stress reaction (bone oedema without a cortical break) through an incomplete fracture to a complete fracture, and a bilateral defect detaches the posterior elements and allows the vertebral body to slip forward on the segment below, producing spondylolisthesis. The pathophysiology is mechanical, and the management aims to rest the pars and allow bony union before the defect becomes complete. [3] [4]
Scheuermann kyphosis is a developmental disorder of the vertebral growth plates in which the cartilaginous endplates ossify unevenly, the anterior vertebral body grows more slowly than the posterior elements, and the vertebral bodies wedge anteriorly. The wedging, combined with irregular endplates and a rigid kyphotic curve, produces the characteristic structural thoracic or thoracolumbar deformity that does not correct on extension. The pathophysiology is a growth-plate disorder, and the management aims to brace the spine while the child is skeletally immature to allow more symmetric growth, reserving surgery for the severe rigid curve. [5] [6]
Discitis is an inflammation or low-grade infection of the intervertebral disc and the adjacent vertebral endplates, and it is the archetypal spinal infection of the young child. The immature disc is vascular, and haematogenous seeding or a contiguous spread seeds the disc space, producing an inflammatory and often infective process that erodes the endplates and narrows the disc height. The young child refuses to walk, holds the spine stiff, and may be febrile, and the pathophysiology explains why the MRI, which shows the bone-marrow oedema and the disc-space inflammation, is the definitive investigation while the plain film is initially normal. [7] [8]
Clinical Presentation
The presentation of the child with back pain is shaped by the age, and the fellowship candidate holds the age-stratified differential in mind from the moment the child walks, or is carried, into the room. The toddler and pre-school child, aged under five years, rarely localises the pain precisely. The child refuses to walk, or regresses from walking to crawling, holds the spine stiff, and may be irritable or febrile. The parents may report a limp or a refusal to sit, and the child may point to the back or the abdomen. At this age, discitis, vertebral infection, and tumour dominate the differential, and the presentation is investigated, not reassured. [7] [8]
The school-age child, aged five to ten years, presents more precisely. The athletic child describes a low back pain that worsens with extension activities — the backbend, the fast-bowl delivery, the dance arch — and eases with rest, and the pain is often unilateral and low in the lumbar spine. The non-athletic child may describe an aching mid-back or a postural deformity that the family has noticed. The fever and the systemic symptoms, when present, redirect the workup toward infection, and the night pain redirects it toward tumour. The fellowship skill is to ask about the sport, the mechanism, and the temporal pattern in the same breath. [9] [2]
The adolescent, aged ten to eighteen years, presents with the broadest differential. The extension-related low back pain of the athlete is spondylolysis until excluded. The increasing rounded upper-back deformity with an aching thoracic spine is Scheuermann kyphosis. The leg-dominant pain with a positive straight-leg raise is a lumbar disc herniation, which is uncommon in children but occurs in the older adolescent, often after trauma or sport. The mechanical muscle-strain back is activity-related, bilateral, low-grade, and free of red flags. The fellowship answer names the pattern aloud and matches it to the imaging. [5] [10]
Which reassuring-sounding stories must never close the search for serious disease? A child with a mechanical-sounding back pain may also have a red flag, and the screen, not the label, decides the workup. A child with discitis may be afebrile at presentation, and the refusal to walk in the young child is investigated regardless of the temperature. And a child with a spondylolysis may have night pain from the muscle spasm that accompanies the pars stress, so the athletic pain is imaged when it is persistent or severe. The red-flag screen is run on every child, every time. [1] [11]
Differential Diagnosis
The differential diagnosis of paediatric back pain is driven by the red flags and the age. In the toddler and pre-school child, discitis is the leading organic cause, presenting with a refusal to walk, a stiff spine, and a low-grade fever, and it is confirmed by MRI showing the disc-space inflammation and the endplate oedema. Vertebral osteomyelitis presents similarly with more systemic illness and a destructive bone lesion, and it is separated from discitis by the predominant bone rather than disc involvement on MRI. The vertebral and paraspinal tumours — osteosarcoma, Ewing sarcoma, and leukaemia — present with constant night pain, a palpable mass in a minority, and systemic features, and they are confirmed by MRI and biopsy. [7] [8]
In the school-age child, spondylolysis is the leading identifiable cause of low back pain in the athlete, presenting with extension-related pain, a positive one-legged hyperextension test, and a focal lumbar tenderness. The stress reaction and the early pars fracture are radiographically occult, and the imaging strategy progresses from a focused lumbar approach when the suspicion is high. Transient muscle strain and overuse are the mechanical diagnoses, presenting with an activity-related bilateral pain that is free of red flags and resolves with rest, and they are diagnoses of exclusion made after the serious causes are excluded. [9] [12]
In the adolescent, the differential broadens further. Scheuermann kyphosis presents with a rigid thoracic or thoracolumbar kyphosis that does not correct on extension, an aching mid-back, and the characteristic vertebral wedging on the lateral radiograph. Lumbar disc herniation presents with leg-dominant radicular pain, a positive straight-leg raise, and occasionally a neurological deficit, and it is confirmed by MRI. Spondylolisthesis presents when a bilateral pars defect allows the vertebral body to slip forward, with a step-off on palpation and a possible radiculopathy. Inflammatory back pain from enthesitis-related juvenile arthritis presents with insidious onset, morning stiffness, and sacroiliac tenderness. [5] [10]
The treatable mimics must not be missed. A pyelonephritis or a retroperitoneal process may refer pain to the back, and a hip or an abdominal pathology may present as back pain in the young child who cannot localise. A spinal cord lesion — a tethered cord, a syrinx, or a cord tumour — produces a painless or night-dominant pain with neurological signs, and the lower-limb neurological examination and the MRI reveal it. The red-flag screen, the focused spine and neurological examination, and the chosen imaging are the safeguards against the missed diagnosis. [1] [11]
Clinical & Bedside Assessment
The bedside assessment begins with the gait and the general appearance, observed before the child is on the couch. Watch the child walk, because a refusal to walk, an antalgic gait, or a wide-based gait with a neurological quality redirects the workup immediately. The young child who is carried in and refuses to weight-bear is investigated for discitis or infection regardless of the temperature, and the adolescent with a foot drop or an abnormal gait is investigated for a neurological cause. [1] [7]
The history is structured around the red-flag screen and the mechanism. Ask about the onset, the site, the radiation, and the aggravating and relieving factors, and ask explicitly about night pain, fever, weight loss, and neurological symptoms. Ask about the sport, the training load, and the extension activities, because the mechanism points to the pars. Ask about the duration, because a pain persisting beyond four weeks is a red flag. Ask about the past history, the family history of spinal disease, and the developmental history, and ask about the systemic features that point to infection or malignancy. [1] [11]
The spine examination proceeds from inspection through palpation to movement and a neurological screen. Inspect the spine from behind for a scoliosis, a kyphosis, and an asymmetry of the skin creases, and inspect the skin for a midline defect such as a sacral dimple, a hair tuft, or a haemangioma that suggests an occult spinal dysraphism. Ask the child to bend forward — the Adams forward bend test reveals a scoliotic rotational prominence, and the persistence of a kyphotic curve on full extension suggests a structural Scheuermann deformity. Palpate the spine for focal tenderness, and percuss for the deep tenderness of an infection or a tumour. Move the spine through flexion, extension, and lateral flexion, and perform the one-legged hyperextension test for a pars stress. [5] [9]
The neurological examination is performed on every child and documented carefully. Test the gait, the tone, the power, the reflexes, and the sensation in the lower limbs, and examine for a Babinski sign and clonus. Test the straight-leg raise for radicular pain, and check for the saddle anaesthesia and the bladder and bowel function that signal a cord or cauda equina compromise. A neurological deficit is a red flag that demands urgent MRI, and the documentation of a normal examination is the safeguard that allows the conservative pathway. [1] [10]
Which findings must never be dismissed? A focal spinal tenderness with a fever is an infection until the MRI proves otherwise. A progressive or a painful deformity is a structural lesion until imaged. And any neurological deficit, however subtle, is a cord or nerve-root compromise that demands urgent imaging and referral. The child with a normal examination and no red flags is managed conservatively with a clear safety-net, and the safety-net is the instruction to return if the pain persists beyond four weeks or if any red flag emerges. [11] [8]
Investigations
The investigation of the child with back pain is guided by the red-flag screen and the suspected diagnosis. In the child with no red flags and a mechanical pattern, the conservative pathway is observation, activity modification, and a safety-net review, and routine imaging is avoided because it is low-yield and exposes the child to radiation. In the child with a red flag, the investigation is targeted at the suspected serious cause, and the imaging is chosen to reveal it. [1] [11]
Bloods are taken when an infection, an inflammatory disease, or a malignancy is suspected. A full blood count, a C-reactive protein, and an erythrocyte sedimentation rate frame the inflammatory and the infective picture and provide the baseline for tracking the response. A blood culture is drawn when the child is febrile, and a myeloid screen is considered when a leukaemia is suspected. The inflammatory markers are the single most useful blood test for discitis and vertebral osteomyelitis, and a markedly raised ESR or CRP in a febrile child with back pain is the trigger for urgent MRI. [7] [8]
Imaging is selected by the suspected diagnosis, and the ACR Appropriateness Criteria for back pain in the child frame the choice. A plain radiograph of the spine is the first-line imaging for a suspected deformity such as Scheuermann kyphosis, revealing the vertebral wedging, the irregular endplates, and the kyphotic angle on the lateral view, and it may reveal a destructive lesion or a spondylolisthesis. Magnetic resonance imaging is the investigation of choice for a suspected infection, a tumour, or a neurological compromise, because it reveals the bone-marrow oedema, the disc-space inflammation, the soft-tissue mass, and the cord or nerve-root involvement that the plain film and the bone scan miss. A focused lumbar imaging strategy is used for the suspected spondylolysis, progressing from the initial plain films to the modality that reveals the early pars lesion. [2] [11]
The bone scan and the computed tomography have a selective role. The bone scan, once the mainstay of the occult spondylolysis, is sensitive for the stress reaction and the early fracture, and it screens the whole spine for the multifocal lesion. The computed tomography defines the bony anatomy of an established pars defect and grades the spondylolisthesis, and the recent radiology review confirms its role in characterising the chronic lesion. The choice among these is made with the radiologist and the orthopaedic team, and the principle is to reveal the diagnosis at the lowest radiation dose that is adequate. [2] [12]
Management — Resuscitation
Resuscitation is rarely the primary need in the child with back pain, because most causes are not immediately life-threatening. The exceptions are the child with a spinal cord or cauda equina compromise, in whom the priority is airway, breathing, and circulation, followed by urgent MRI and neurosurgical referral, and the child with discitis or vertebral osteomyelitis who is septicaemic, in whom intravenous access, fluid resuscitation if shocked, and empirical intravenous antibiotics after blood culture are the immediate steps. The spinal emergency is managed by the imaging and the specialist referral, not by the bedside manoeuvre. [7] [8]
The child with a suspected spinal cord compromise is kept flat and immobilised, and the urgent MRI is arranged with the neurosurgical team involved from the outset. The child with a suspected discitis or vertebral infection receives empirical intravenous antibiotics that cover the common organisms once the blood culture is drawn. Staphylococcus aureus is the commonest organism in the spinal infections of childhood, and the choice of antibiotic follows local guidelines and is guided by the culture result. The duration is typically two to four weeks intravenously and then an oral step-down, guided by the clinical and the inflammatory-marker response. [8] [7]
The child with a painful spondylolysis or a Scheuermann kyphosis is managed as an elective outpatient, and the general paediatrician's role is to make the diagnosis, arrange the imaging, control the pain, and refer to the orthopaedic team. The pain is controlled with simple analgesia and activity modification, and the child is prepared for the bracing or the surgical fixation that the orthopaedic team guides. The resuscitation principle is that the serious diagnosis is identified before the deterioration, and the harm is prevented by the early imaging and the early referral. [9] [6]
Management — Definitive & Stepwise
The definitive management of the mechanical back is activity modification, simple analgesia, and a strengthening programme, and the condition resolves within four to six weeks in the great majority of adolescents. The child is reviewed at four to six weeks, because a pain that fails to resolve is itself a red flag and demands escalation to imaging. The key management decision is the one made at the outset: the red-flag screen that excludes the serious cause and allows the safe, conservative pathway. [1] [11]
The definitive management of spondylolysis is activity cessation, an anti-lordotic brace in the symptomatic or the high-grade lesion, and a core-stabilisation physiotherapy programme, with the goal of bony union of the pars before the defect becomes complete. The review of over two hundred young athletes confirmed that the conservative approach achieves union or a symptom-free state in the great majority, and the graded return to sport is guided by the resolution of the pain and the imaging. The surgical repair is reserved for the refractory symptomatic lesion that fails a thorough conservative programme, and the bilateral defect with a progressive spondylolisthesis is monitored closely and fixed when the slip progresses. [9] [4]
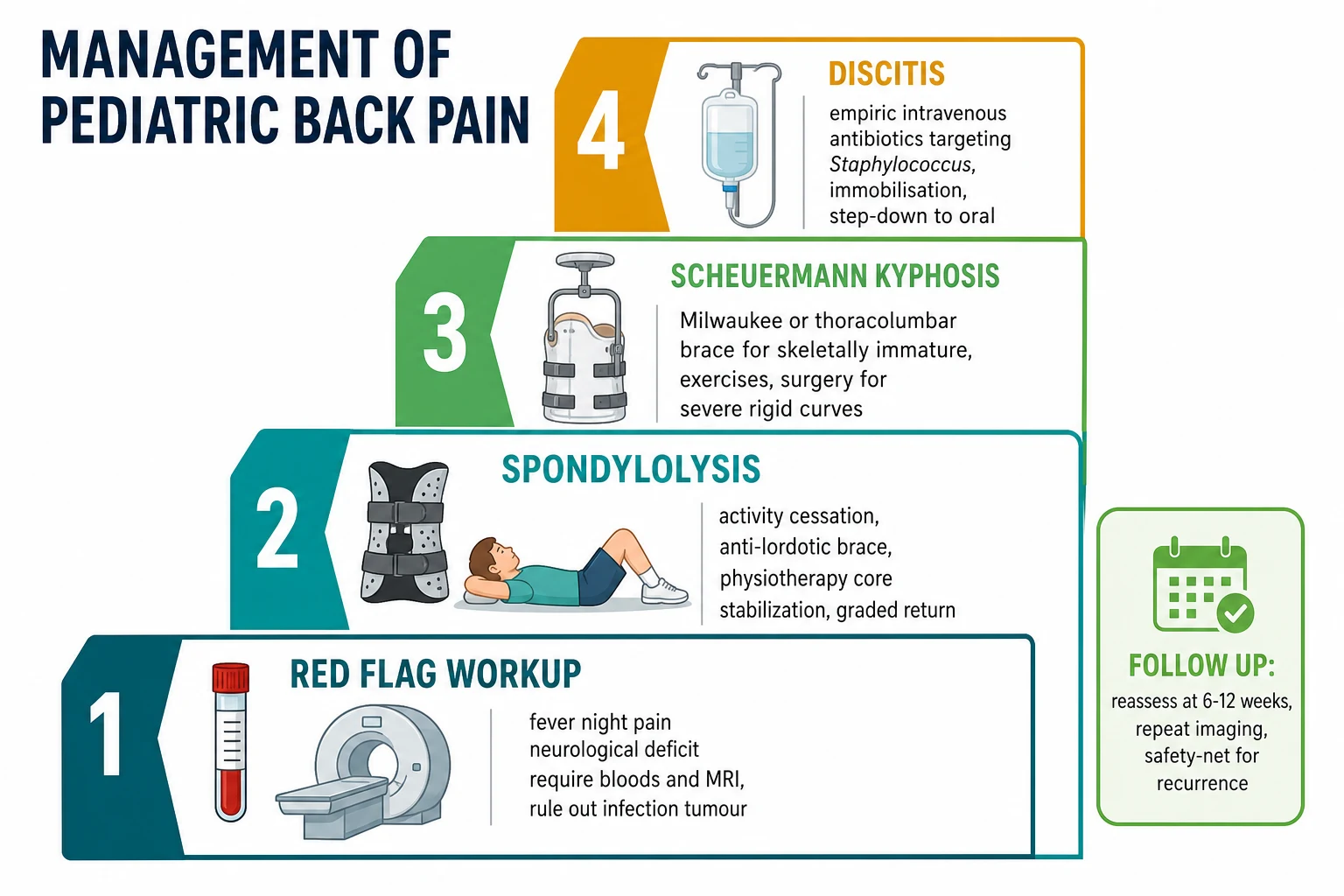
The definitive management of Scheuermann kyphosis depends on the skeletal maturity and the severity of the curve. The skeletally immature adolescent with a moderate curve is managed with a Milwaukee or a thoracolumbar brace and a posture-and-strengthening programme, with the aim of allowing more symmetric vertebral growth while the growth plates remain open. The severe rigid curve, typically a kyphosis above seventy degrees with an unacceptable deformity or persistent pain, is managed with a posterior spinal fusion, and the evidence-based review frames the brace and the surgery as complementary rather than competing. The fellowship answer names the threshold and refers to the orthopaedic team for the decision. [5] [6]
The definitive management of discitis is empirical intravenous antibiotics targeting Staphylococcus aureus, immobilisation for comfort, and a step-down to oral therapy guided by the clinical and the inflammatory-marker response. The systematic review of paediatric spondylodiscitis confirmed the role of the targeted antibiotic course and the immobilisation, with surgical intervention reserved for the abscess, the neurological deficit, or the progressive deformity. The lumbar disc herniation in the adolescent is managed conservatively in the great majority, with surgical microdiscectomy reserved for the persistent radiculopathy, the neurological deficit, or the cauda equina syndrome. [8] [7]
The age-stratified diagnoses and their first management
Specific Subtypes & Scenarios
Discitis is the subtype that defines the pre-school back. The child is typically under five years, presents with a refusal to walk or a regression in mobility, holds the spine stiff, and may be febrile or irritable. The inflammatory markers are raised, the plain film is initially normal, and the MRI shows the disc-space inflammation and the adjacent endplate oedema. The management is empirical intravenous antibiotics targeting Staphylococcus aureus, immobilisation, and a step-down to oral, and the outcome is excellent with prompt treatment. The fellowship skill is to investigate the young child with back pain, not to reassure, because the diagnosis is missed when the temperature is normal and the refusal to walk is attributed to a minor injury. [7] [8]
Spondylolysis is the subtype that defines the school-age athletic back. The child plays an extension-loading sport and describes a low back pain that worsens with hyperextension and eases with rest. The one-legged lumbar hyperextension test reproduces the pain, and the focal lumbar tenderness on palpation supports the suspicion. The imaging strategy progresses from the initial films to the modality that reveals the early pars lesion, and the management is activity cessation, an anti-lordotic brace, and a core-stabilisation programme with the goal of bony union. The recent radiology review confirms that the computed tomography characterises the chronic defect and grades the spondylolisthesis when the slip is suspected. [9] [12]
Scheuermann kyphosis is the subtype that presents with a deformity. The adolescent, often male, has an increasing rounded upper back that the family noticed first, an aching thoracic spine, and a rigid kyphotic curve that does not correct on extension. The lateral radiograph reveals the anterior vertebral wedging, the irregular endplates, and the kyphotic angle, and the management is bracing in the skeletally immature and surgery in the severe rigid curve. The fellowship answer frames the long timeline, the role of the brace while the growth plates are open, and the threshold for the orthopaedic referral. [5] [6]
Lumbar disc herniation is the subtype that presents with leg pain. The older adolescent, often after trauma or sport, describes a leg-dominant radicular pain with a positive straight-leg raise, and occasionally a neurological deficit. The MRI confirms the disc protrusion and the nerve-root compression, and the management is conservative in the great majority with a microdiscectomy reserved for the persistent radiculopathy or the deficit. Spondylolisthesis presents when a bilateral pars defect allows the vertebral body to slip forward, with a step-off on palpation and a possible radiculopathy, and the high-grade slip is monitored and fixed surgically when it progresses. [10] [4]
Complications & Pitfalls
The complications of a delayed or missed diagnosis span the spine and the child's future. A discitis that is treated late leaves a residual disc-space narrowing and a vertebral deformity, and a vertebral osteomyelitis may progress to a chronic infection or an epidural abscess with a neurological deficit. A spondylolysis that is loaded through a competitive season progresses from a stress reaction to a complete fracture that may not unite, and a progressive spondylolisthesis may compress the nerve roots and require a fusion. A spinal tumour that is dismissed as growing pains narrows the window for curative treatment. The harm is preventable by the red-flag screen and the early imaging. [7] [4]
The pitfall of the reassuring label is the error that delays the diagnosis of the serious cause. An adolescent with a mechanical-sounding back pain is sent home with analgesia, and the spondylolysis or the early tumour is missed until the pain persists and the red flag emerges. The safeguard is the rule that the red-flag screen is run on every child, and that a pain persisting beyond four weeks is imaged rather than reassured. The pitfall of the normal initial radiograph in the early discitis or the occult tumour is the related error, and the safeguard is the MRI when the clinical suspicion is high and the plain film is normal. [1] [11]
The pitfall of the over-investigated mechanical back is the lesser harm, but it is a harm nonetheless. An adolescent with a straightforward muscle strain is swept into unnecessary imaging and specialist referral, exposing the child to radiation, the family to anxiety, and the system to cost. The safeguard is the disciplined application of the red-flag screen: a normal examination with no red flags is managed conservatively with a clear safety-net, and the imaging is reserved for the pain that persists or the red flag that emerges. [1] [2]
The pitfall of the missed non-accidental injury or the psychosomatic pain is the error that the broad assessment catches. A toddler with a vertebral fracture and an inconsistent story raises the question of abuse, and the safeguard is the careful history and the child-protection involvement. An adolescent with a disabling, persistent back pain and a normal workup may have a pain-amplification syndrome, and the safeguard is the recognition of the biopsychosocial pattern and the referral to the pain-medicine or the psychology team. The fellowship answer holds the physical and the psychosocial frames together. [11] [8]
Prognosis & Disposition
The prognosis of paediatric back pain is generally excellent when the serious causes are identified and treated promptly. The mechanical back resolves within four to six weeks with activity modification in the great majority of adolescents. Spondylolysis, rested early, achieves bony union or a symptom-free state in the great majority of young athletes, and the outcome worsens when the defect is bilateral, chronic, or associated with a progressive spondylolisthesis. Discitis treated promptly with antibiotics resolves with a minimal residual deformity, and the prognosis worsens with a delay in treatment or a neurological deficit at presentation. [9] [7]
Scheuermann kyphosis has a prognosis that depends on the skeletal maturity and the curve severity at the time of the bracing, with the skeletally immature and the moderate curve doing well with the brace. The severe rigid curve carries a higher burden of deformity and pain, and the surgical fusion corrects the curve and stabilises the spine. The lumbar disc herniation in the adolescent resolves conservatively in the great majority, with a microdiscectomy reserved for the persistent or the deficit case, and the outcome is comparable to the adult series in the carefully selected surgical candidate. [5] [6]
The disposition is shared between the general paediatrician, the orthopaedic surgeon, the neurosurgeon, and the infectious-diseases team. The general paediatrician owns the initial assessment, the red-flag screen, the decision to image, and the safety-net review. The orthopaedic surgeon owns the spondylolysis that fails conservative care, the Scheuermann kyphosis, and the spondylolisthesis. The neurosurgeon owns the cord or cauda equina compromise and the disc herniation with a deficit. The infectious-diseases team owns the discitis and the vertebral osteomyelitis. The fellowship answer names the right specialist for the right diagnosis and never holds a child with a red flag in the outpatient clinic when the urgent pathway is indicated. [1] [10]
Special Populations
Children with developmental disability and neurodiversity present particular challenges in the back-pain assessment. A child with cerebral palsy may have a pre-existing scoliosis or a postural deformity that masks a new pain, and a child with limited communication may not localise the pain, so the assessment relies on observing the change from the baseline, the refusal to move, and the physiological signs of distress. The threshold for imaging and bloods is lower when the history is uncertain, and the red-flag screen is adapted to the child's abilities and baseline. [11] [8]
Indigenous, remote, and socioeconomically disadvantaged children face the additional burdens of access and equity. The incidence of osteoarticular infection, including discitis and vertebral osteomyelitis, is higher in many remote Indigenous communities, and the distance to MRI and specialist review delays the diagnosis and the antibiotic course. A newly arrived migrant or refugee child may have an undocumented history and a higher prevalence of tuberculosis-related spinal disease, and the workup may need to consider the unusual organism and the local epidemiology. The fellowship answer acknowledges these inequities and builds the rapid-referral pathways that close the gap. [7] [8]
The child in out-of-home care and the adolescent with psychosocial adversity are the special populations that demand the broad assessment. A toddler with a vertebral injury and an inconsistent history raises the question of non-accidental injury, and the safeguard is the careful history and the child-protection involvement. An adolescent with a persistent, disabling back pain and a normal workup may have a pain-amplification syndrome driven by the psychosocial context, and the safeguard is the recognition of the biopsychosocial pattern and the multidisciplinary referral. The fellowship candidate does not close the back-pain assessment after the spine is dealt with. [1] [11]
Evidence, Guidelines & Regional Differences
The evidence base for the paediatric back-pain assessment rests on the algorithmic studies from Feldman and colleagues. The 2000 paper established the role of the bone scan in the investigation of the back pain that the plain film misses, and the 2006 paper evaluated an algorithmic approach that combines the clinical assessment, the red-flag screen, and the staged imaging. These studies frame the fellowship task: screen for the red flags, image the suspected serious cause, and follow up the conservative case. The ACR Appropriateness Criteria for back pain in the child, updated in 2024, formalise the imaging strategy and confirm the MRI as the modality for the infection, the tumour, and the neurological compromise. [1] [11]
The evidence for spondylolysis rests on the natural-history studies and the athletic reviews. The Fredrickson 1984 paper and the Beutler 2003 forty-five-year follow-up established the natural history of the pars defect and the spondylolisthesis, framing the conservative management and the monitoring. The Choi review of over two hundred young athletes confirmed the success of the activity cessation, the brace, and the core programme in achieving union or a symptom-free state, and the Rambo radiology review characterised the computed-tomography features of the lesion. The Cetik review framed the combined management of the sagittal-plane pathologies that coexist in the child. [3] [9]
The evidence for Scheuermann kyphosis rests on the Lowe evidence-based analysis and the O'Donnell current-concepts review. The Lowe 2007 analysis framed the bracing and the surgery as complementary, and the O'Donnell 2023 review updated the current concepts and the management. The evidence for discitis rests on the Brown clinical series and the Lashkarbolouk systematic review, which confirmed the role of the targeted antibiotic course and the immobilisation, with the surgical intervention reserved for the complication. [5] [8]
The regional differences are modest but real. The imaging strategy and the antibiotic choice for discitis follow the local microbiology and the resistance pattern, and the threshold for the MRI varies by the access and the distance in the rural and the remote setting. The prevalence of the tuberculosis-related spinal disease is higher in the migrant and the refugee population, and the workup considers the atypical organism in the right clinical context. The bracing and the surgical thresholds for Scheuermann kyphosis are broadly consistent across the regions, and the fellowship answer names the local guideline without pretending that a single algorithm resolves every judgement call. [7] [10]
Exam Pearls
The fellowship answer turns on five facts. Back pain in a child under five is itself a red flag, and the pre-school back is investigated for discitis and infection. The red-flag screen — night pain, fever, weight loss, neurological deficit, age under five, and persistence beyond four weeks — separates the back that demands urgent imaging from the one managed conservatively. The age-stratified differential runs from discitis in the toddler through spondylolysis in the school-age athlete to Scheuermann kyphosis and lumbar disc herniation in the adolescent. The athletic extension-related low back pain is a spondylolysis until imaging excludes it. And the MRI is the modality for the infection, the tumour, and the neurological compromise that the plain film and the bone scan miss. [1] [9]
The examiner probes three traps. The first is the pre-school child with back pain who is reassured as a minor injury — discitis is missed when the temperature is normal and the refusal to walk is attributed to a fall, and the MRI is the safeguard. The second is the adolescent athlete whose extension-related low back pain is dismissed as muscle strain — the spondylolysis is missed until the defect is complete or the spondylolisthesis progresses, and the focused lumbar imaging is the safeguard. The third is the child with the night pain who is dismissed as growing pains — the tumour is missed until the pain is constant and the mass is palpable, and the red-flag screen is the safeguard. [7] [12]
The examiner rewards the candidate who frames the back-pain assessment as a clinical reasoning exercise, not a list. The red-flag screen is run, the age-stratified differential is held, the imaging is chosen for the suspected diagnosis, the right specialist is called, and the conservative case is followed up with a safety-net. A candidate who shows this breadth and this safety demonstrates the systems thinking that the fellowship demands. [1] [11]
References
- [1]Feldman DS, Straight JJ, Badra MI, Mohaideen A, Madan SS. Evaluation of an algorithmic approach to pediatric back pain. J Pediatr Orthop, 2006.PMID 16670548
- [2]Feldman DS, Hedden DM, Wright JG. The use of bone scan to investigate back pain in children and adolescents. J Pediatr Orthop, 2000.PMID 11097256
- [3]Fredrickson BE, Baker D, McHolick WJ, Yuan HA, Lubicky JP. The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am, 1984.PMID 6373773
- [4]Beutler WJ, Fredrickson BE, Murtland A, Sweeney CA, Grant WD, Baker D. The natural history of spondylolysis and spondylolisthesis: 45-year follow-up evaluation. Spine (Phila Pa 1976), 2003.PMID 12768144
- [5]Lowe TG, Line BG. Evidence based medicine: analysis of Scheuermann kyphosis. Spine (Phila Pa 1976), 2007.PMID 17728677
- [6]O'Donnell JM, Wu W, Youn A, Mann A, Swarup I. Scheuermann Kyphosis: Current Concepts and Management. Curr Rev Musculoskelet Med, 2023.PMID 37615931
- [7]Brown R, Hussain M, McHugh K, Novelli V, Jones D. Discitis in young children. J Bone Joint Surg Br, 2001.PMID 11245515
- [8]Lashkarbolouk N, Mazandarani M, Ilharreborde B, Nabian MH. Understanding the management of pediatric spondylodiscitis based on existing literature; a systematic review. BMC Pediatr, 2023.PMID 37980513
- [9]Choi JH, Ochoa JK, Lubinus A, Timon S, Lee YP, Bhatia NN. Management of lumbar spondylolysis in the adolescent athlete: a review of over 200 cases. Spine J, 2022.PMID 35504566
- [10]Cetik RM, Latalski M, Yazici M. Management of low back pain accompanying sagittal plane pathologies in children: Spondylolysis/spondylolisthesis and Scheuermann's disease. J Child Orthop, 2023.PMID 38050599
- [11]Expert Panel on Pediatric Imaging, Dahmoush H, Gaddam DS, Ho ML, Bauer DF, Bosemani T. ACR Appropriateness Criteria® Back Pain-Child: 2024 Update. J Am Coll Radiol, 2025.PMID 40409897
- [12]Rambo AJ, Sheffer BW, Hajek B, Almatari A, Suit P, Rhodes LN. Lumbar Spondylolysis in the Pediatric Population: A Retrospective CT Review With Radiology Rereview. J Am Acad Orthop Surg, 2025.PMID 40233349