Paeds · rheumatology-musculoskeletal-and-sports
Clubfoot and congenital limb anomalies
Also known as clubfoot · congenital talipes equinovarus · CTEV · Ponseti method · Pirani score · Dimeglio classification · foot abduction brace · percutaneous Achilles tenotomy · fibular hemimelia · tibial hemimelia · polydactyly · syndactyly · amniotic band syndrome
A fellowship approach to the clubfoot (congenital talipes equinovarus) and the broad family of congenital limb anomalies: the four classical deformities (cavus, adductus, varus, equinus), the Ponseti serial casting method as the global gold standard with the percutaneous Achilles tenotomy and the foot-abduction brace to four to five years, the Pirani and Dimeglio severity systems, the idiopathic-versus-syndromic-versus-positional distinction, the relapse and its management, and the longitudinal, transverse, and digital congenital limb deficiencies with their orthopaedic and prosthetic disposition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A newborn boy is found on the routine baby check to have a right foot that is turned inward and downward and that does not correct with gentle passive manipulation — the classic idiopathic clubfoot. His Pirani score is four out of six, the deep medial crease and the rigid equinus raising the hindfoot and the midfoot scores, and the Ponseti casting begins in the first week of life. After five casts and a percutaneous Achilles tenotomy at eight weeks, the foot is plantigrade, and the foot-abduction brace is fitted for twenty-three hours a day. A two-month-old girl presents with a foot that looks identical but corrects to neutral with a thumb and a forefinger — the positional clubfoot, which needs no casting and resolves with stretching. The clinical skill is to read the rigidity, to apply the score, and to begin the Ponseti method early. [2] [7]
CAVE — the four classical deformities of clubfoot
Overview & Definition
Clubfoot, also called congenital talipes equinovarus, is a congenital deformity of the foot present at birth in which the foot is inverted, adducted, and plantarflexed, and in which the deformity is fixed and resists passive correction. The four components — cavus, adductus, varus, and equinus — give the foot its classic appearance: the sole faces inward and the foot points down, the lateral border is curved, and the heel is small and in varus. The deformity is structural, not positional, and the rigidity is the single feature that separates the true clubfoot from the flexible postural foot that resolves with stretching alone. [5] [7]
The clinical importance of clubfoot lies in what an untreated foot does to a child. The child who is not treated walks on the lateral border of the foot or on the dorsum, develops painful calluses, and lives with a permanent limp and a shoe that does not fit. The Ponseti method, developed by Ignacio Ponseti in Iowa in the 1940s and published in its modern form in 1992, transformed the management from the extensive soft-tissue release — with its high rate of stiffness, pain, and arthritis — to a minimally invasive casting method with a percutaneous tenotomy and a brace. The long-term outcome, now documented to thirty years and beyond, is a plantigrade, painless, flexible foot in the great majority of treated children. [1] [2]
The page that follows treats clubfoot as the paediatric generalist encounters it: detected at the newborn baby check, scored at the bedside, treated by the Ponseti method, braced for the first four to five years, and managed through the relapse if and when it comes. It then widens to the broader family of congenital limb anomalies — the longitudinal and transverse deficiencies, and the digital anomalies — that the same newborn examination may reveal, and that share the same early referral and the same family-centred, multidisciplinary care. [5] [7]
Classification
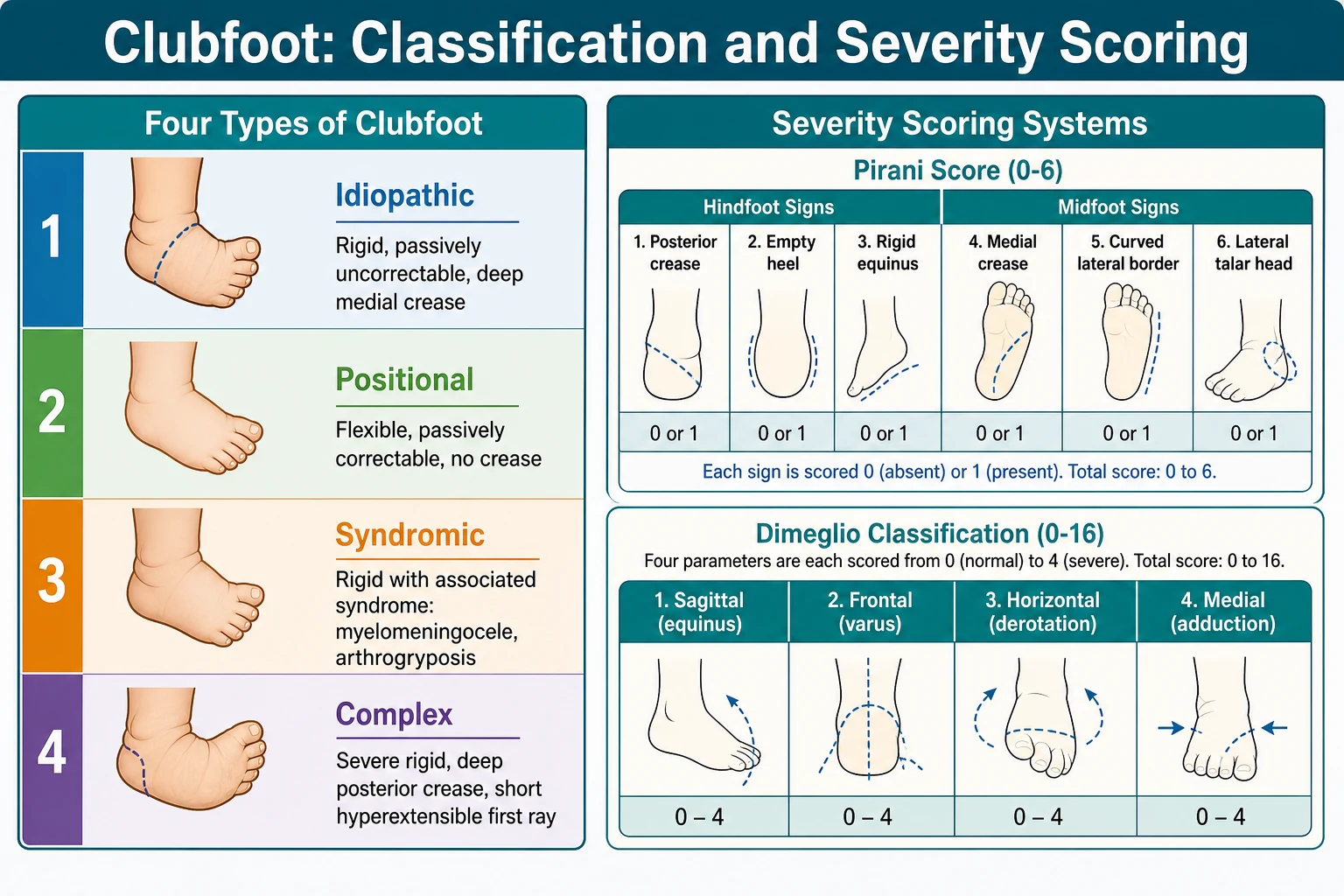
Clubfoot is classified along three axes that together guide the prognosis and the management. The first axis is the aetiology: the idiopathic clubfoot is the isolated deformity in an otherwise normal child, and it is the commonest; the syndromic clubfoot, sometimes called the teratologic or the non-idiopathic clubfoot, is associated with a neural tube defect (myelomeningocele), a neuromuscular disorder (arthrogryposis, distal arthrogryposis), or a skeletal dysplasia (diastrophic dysplasia, Larsen syndrome); and the positional clubfoot is the flexible, passively correctable foot that is a packaging deformity of late gestation, not a true structural deformity. [5] [10]
The second axis is the severity, graded at the bedside by the two most widely used scoring systems. The Pirani score assigns zero, half, or one point to each of six clinical signs — three hindfoot signs (the posterior crease, the emptiness of the heel, the rigidity of the equinus) and three midfoot signs (the medial crease, the curvature of the lateral border, the palpable lateral part of the head of the talus) — for a total of zero to six. A higher Pirani score predicts a greater number of casts and a higher likelihood of a percutaneous tenotomy. The Dimeglio classification scores four parameters of the range of motion — the equinus in the sagittal plane, the varus in the frontal plane, the derotation of the calcaneopedal block in the horizontal plane, and the adduction of the forefoot in the medial plane — each from zero to four, with four additional one-point severity signs (the posterior crease, the medial crease, the cavus, and the poor muscle condition), for a total of zero to twenty and four severity grades from one (benign) to four (severe). [7]
The third axis is the atypical or the complex clubfoot, the severe rigid deformity with the deep posterior crease above the heel, the short hyperextensible first ray, the tight plantar flexion, and the deep transverse plantar crease. The complex clubfoot, originally described by Ponseti himself, requires a modified casting technique — the two casts for the cavus and the adductus, the peri-talar abduction with a different hand position, and the early percutaneous tenotomy — because the standard Ponseti method applied without modification can produce the rocker-bottom foot. [5] [8]
Idiopathic, positional, syndromic, and complex clubfoot
Idiopathic
Positional
Syndromic
Complex (atypical)
Epidemiology & Risk Factors
Idiopathic clubfoot affects roughly one in one thousand live births worldwide, though the rate varies with ancestry — it is higher in Polynesian and in some South African populations, and lower in Asian populations. Boys are affected about twice as often as girls, and the bilateral involvement is seen in roughly half the cases, with the unilateral cases slightly more common on the right. The male predominance and the bilateral involvement are the two epidemiological facts the fellowship answer holds, because they shape the differential at the newborn baby check and the counselling of the family. [9] [12]
The heritable component is substantial, and it is established by the Wynne-Davies family studies of the 1960s. The recurrence risk for the sibling of an affected child is about three to four percent, and the recurrence risk for the child of an affected parent is about twenty-five to thirty percent. These figures are consistent with a multifactorial inheritance — a polygenic threshold trait combined with an environmental trigger — and they are the numbers the fellowship candidate quotes when the family asks the question that every family asks: "Will it happen again?" [12]
The environmental contributions include the maternal smoking, the oligohydramnios, and the early amniocentesis, all of which raise the risk of clubfoot, and all of which suggest a fetal-packaging component to the deformity. The syndromic clubfoot, in myelomeningocele and in arthrogryposis, follows a different epidemiology — it is the foot manifestation of a primary neural or a neuromuscular disorder — and it responds differently to the Ponseti method, with a higher rate of relapse and a greater need for the modified technique. The complex clubfoot, with its deep crease and its short hyperextensible first ray, is a clinical phenotype within the idiopathic group that carries a more guarded prognosis and a longer casting course. [10] [8]
Pathophysiology
The pathophysiology of the idiopathic clubfoot combines an intrauterine malposition, a contracture of the posterior and the medial soft tissues, and a malrotation of the talonavicular and the calcaneocuboid joints. The talus is small and plantarflexed, the navicular is medially displaced and rotated to face the medial aspect of the talus, the calcaneus is inverted and plantarflexed beneath the talus, and the cuboid is medially displaced on the calcaneus. The posterior tibialis, the gastrocnemius-soleus, and the long toe flexors are shortened and contracted, and the posterior and the medial ankle and the subtalar capsules are thickened. The result is the four classical deformities: the cavus from the plantarflexion of the first ray, the adductus from the medial displacement of the navicular and the cuboid, the varus from the inversion of the calcaneus, and the equinus from the plantarflexion contracture of the ankle. [1] [5]
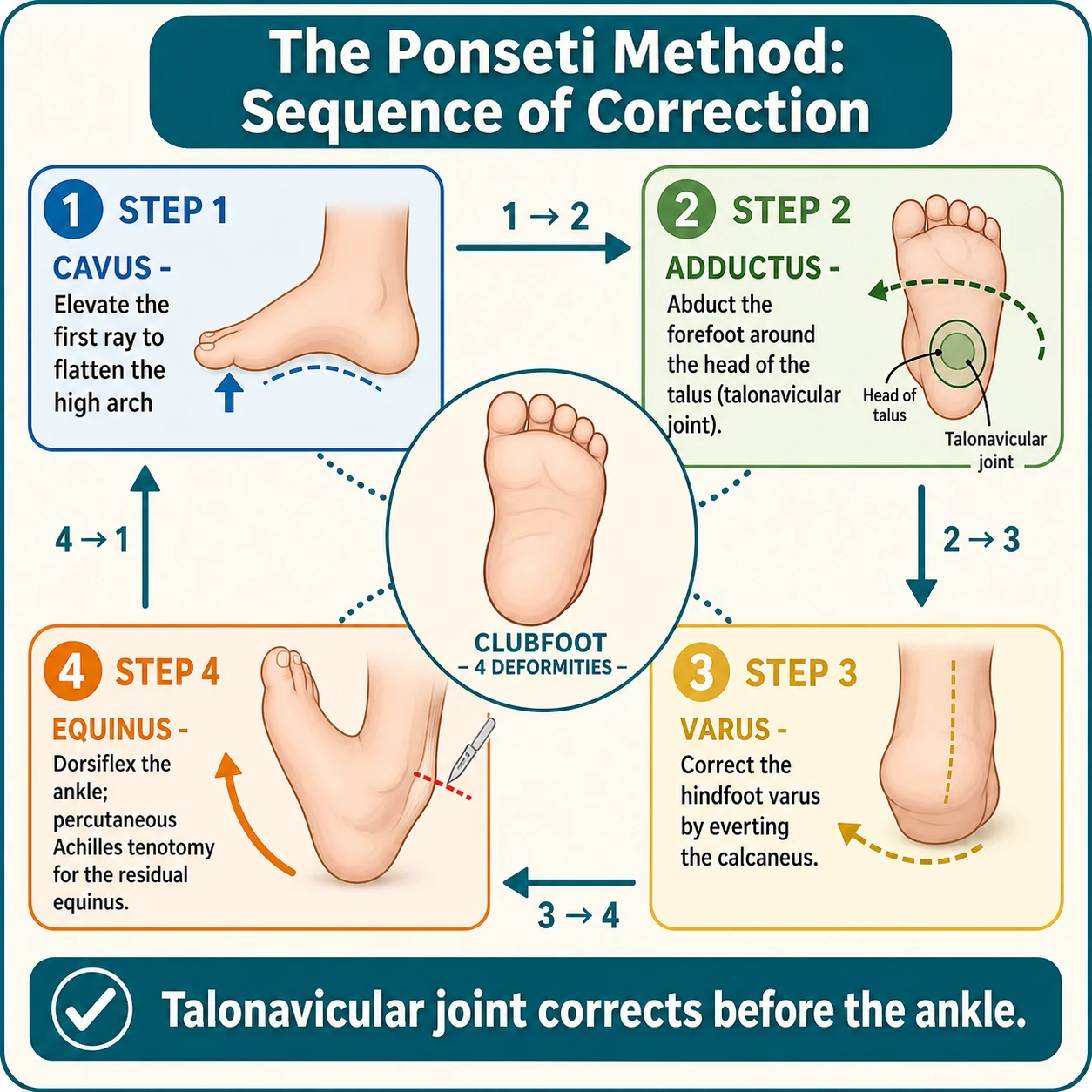
The genius of the Ponseti method is the way it exploits the viscoelastic creep of the immature ligament and the cartilage to correct the deformities in a defined sequence. The cavus is corrected first by elevating the first ray, aligning the forefoot with the hindfoot. The adductus and the varus are corrected next, together, by abducting the foot around the head of the talus — the fulcrum of the correction — while applying a counter-pressure on the lateral aspect of the talar head. As the foot abducts, the navicular reduces onto the head of the talus, the calcaneus everts beneath the talus, and the cuboid aligns on the calcaneus. The equinus is corrected last, by dorsiflexing the ankle, and in most cases a percutaneous Achilles tenotomy is needed to release the residual tightness of the tendon that the casts cannot overcome. The sequence is biomechanical, not arbitrary: the talonavicular joint corrects before the ankle, because the abduction of the foot around the talus must precede the dorsiflexion, and a premature dorsiflexion against a tight posterior capsule produces the rocker-bottom foot. [1] [7]
The foot-abduction brace maintains the corrected foot in the abducted, dorsiflexed position and prevents the relapse that occurs when the medial and the posterior contractures recur in the growing child. The brace holds the foot at seventy degrees of external rotation (sixty to seventy for the affected foot, and thirty to forty for the unaffected foot in the unilateral case), with fifteen degrees of dorsiflexion, and the long-term brace compliance — not the casting, and not the tenotomy — is the single greatest determinant of whether the correction lasts. [3] [4]
The broader family of the congenital limb anomalies follows the same embryological logic. The longitudinal deficiencies — the fibular hemimelia, the tibial hemimelia, the proximal femoral focal deficiency — arise from a failure of formation of a part of the limb bud across the long axis. The transverse deficiencies — the congenital amputation, the amniotic band syndrome — arise from a failure of formation across the short axis, or from a constriction band that compromises the distal limb in utero. The digital anomalies — the polydactyly, the syndactyly — arise from a failure of separation or a duplication of the digital rays. Each pattern tells the examiner something about the aetiology and the management, and the classification of Frantz and O'Rahilly — the four types of failure of formation, failure of differentiation, duplication, and overgrowth — is the framework the paediatric orthopaedic surgeon applies. [5] [7]
Clinical Presentation
The newborn with the idiopathic clubfoot is detected on the routine baby check, often in the first twenty-four to forty-eight hours of life. The foot is inverted, the sole faces inward, the foot is plantarflexed, and the lateral border is curved rather than straight. The heel is small and in varus, the deep medial crease runs from the heel to the sole, and the deformity does not correct with gentle passive manipulation. The bilateral clubfoot presents with both feet in the same posture, and the unilateral clubfoot presents with the affected foot in the deformity and the calf atrophy that is the subtle sign of the long-standing intrauterine position. The child is otherwise well, with no other anomaly, and the spine and the hips are normal. [5] [7]
The positional clubfoot presents with the same external appearance but with a foot that corrects to neutral with gentle passive manipulation. There is no deep crease, the heel is of normal size, the calf is normal, and the deformity is the consequence of a packaging in late gestation rather than a structural contracture. The positional clubfoot resolves with stretching by the parents or, rarely, with a few serial casts, and it does not require the full Ponseti method. The skill at the bedside is to test the rigidity: a foot that corrects to neutral with a thumb and a forefinger is positional; a foot that resists is structural. [5] [7]
The syndromic clubfoot presents with the rigid foot and the features of the underlying syndrome. The child with a myelomeningocele has an open spinal lesion, the absent lower-limb movement, and the paralytic clubfoot that is often bilateral and severe. The child with arthrogryposis has the rigid contractures of multiple joints, the internally rotated shoulders, the extended elbows, and the clubfoot that is one of several fixed deformities. The child with a distal arthrogryposis has the clubfoot and the hand contractures. The syndromic clubfoot is more rigid, more resistant to the Ponseti method, and more likely to relapse, and the workup must include the spine, the genetics, and the multidisciplinary team. [10]
The complex clubfoot, within the idiopathic group, presents with the severe rigid deformity, the deep posterior crease above the heel, the short hyperextensible first ray, the tight plantar flexion, and the deep transverse plantar crease. The foot is short and stubby, the toes are flexed, and the standard Ponseti method, applied without modification, can produce the rocker-bottom foot. The complex clubfoot is the phenotype that demands the modified technique and the early recognition. [5] [8]
The congenital limb anomalies present at the same newborn examination. The fibular hemimelia presents with the short lower limb, the absent lateral rays, the valgus ankle, and the leg-length discrepancy that declares in the growing child. The tibial hemimelia presents with the short lower limb, the varus ankle, and the flexed knee with the absent or the deficient tibia. The proximal femoral focal deficiency presents with the short thigh, the flexed and the abducted hip, and the leg-length discrepancy. The amniotic band syndrome presents with the constriction ring around a limb or a digit, with the distal oedema and the threatened ischaemia. The polydactyly presents with the extra digit — the postaxial on the ulnar or the fibular side, the preaxial on the radial or the tibial side, the central between the rays. The syndactyly presents with the fused digits, the simple (soft-tissue only) or the complex (with the bony fusion). Each anomaly is detected on inspection, and each demands the early referral. [5]
Differential Diagnosis
The differential of the inverted foot at birth is the first decision the general paediatrician makes. The metatarsus adductus is the forefoot adduction with a normal hindfoot, and it is distinguished from the clubfoot by the normal heel and the flexible forefoot that abducts to neutral with passive manipulation. The calcaneovalgus foot is the dorsiflexed and the externally rotated foot — the opposite of the clubfoot — and it resolves spontaneously with stretching. The congenital vertical talus is the rigid rocker-bottom foot, with the convex plantar surface and the irreducible dislocation of the talonavicular joint, and it is the diagnosis that demands the surgical reduction rather than the Ponseti casting. The skew foot, the combination of the metatarsus adductus and the hindfoot valgus, is rarer and is managed by the paediatric orthopaedic surgeon. [5] [7]
The inverted foot at birth — the differential
Idiopathic clubfoot
Metatarsus adductus
Calcaneovalgus foot
Congenital vertical talus
The differential of the syndromic clubfoot, when a rigid foot is associated with other anomalies, is the workup that the general paediatrician begins. The myelomeningocele is identified by the open spinal lesion and the neurological deficit. The arthrogryposis is identified by the multiple joint contractures. The distal arthrogryposis is identified by the hand and the foot contractures with the characteristic hand positioning. The Larsen syndrome is identified by the multiple joint dislocations. The diastrophic dysplasia is identified by the short stature, the hitchhiker thumb, and the cystic ear swelling. The myotonic dystrophy, the congenital form, is identified by the hypotonia and the family history. Each syndrome carries its own prognosis and its own modification of the Ponseti method. [10] [5]
Clinical & Bedside Assessment
The examination of the newborn foot begins with the inspection. The foot is observed at rest, in the inverted, the adducted, and the plantarflexed posture. The deep medial crease, the posterior crease, the small heel in varus, the curved lateral border, and the calf atrophy are the inspection findings that raise the clubfoot. The deep posterior crease above the heel, the short hyperextensible first ray, and the deep transverse plantar crease are the findings that raise the complex clubfoot. The absence of the creases and the normal calf raise the positional clubfoot. [7]
The rigidity is then tested. The examiner grasps the foot and attempts to correct the deformity with gentle passive manipulation: the forefoot is abducted, the heel is everted, and the ankle is dorsiflexed. A foot that corrects to neutral is positional; a foot that resists is structural. The range of the dorsiflexion, with the knee flexed, estimates the equinus, and the rigidity of the equinus is a key hindfoot sign of the Pirani score. The head of the talus is palpated just in front of the lateral malleolus, and the prominence of the lateral part of the talar head is the midfoot sign that reflects the medial displacement of the navicular. [7] [5]
The Pirani score is then applied. The three hindfoot signs — the posterior crease, the emptiness of the heel, and the rigidity of the equinus — and the three midfoot signs — the medial crease, the curvature of the lateral border, and the palpable lateral part of the head of the talus — are each scored zero (normal), half (moderate), or one (severe), for a total of zero to six. A Pirani score above four predicts a greater number of casts, and a hindfoot score above one at the end of the casting predicts the need for the percutaneous tenotomy. The Dimeglio classification is applied in parallel: the four parameters of the range of motion (the sagittal equinus, the frontal varus, the horizontal derotation, the medial adduction) are each scored zero to four, the four pejorative signs (the posterior crease, the medial crease, the cavus, the poor muscle condition) are each scored zero or one, and the total of zero to twenty gives the Dimeglio grade from one (benign) to four (severe). [7]
The spine is examined for a myelomeningocele scar, a hairy patch, a lipoma, or a sacral dimple, because the syndromic clubfoot of a neural tube defect is the diagnosis that changes the management. The hips are examined for the developmental dysplasia, with the Barlow and the Ortolani manoeuvres, because the hip and the foot may coexist. The upper limbs are examined for the contractures of the arthrogryposis, and the facial features are observed for the syndrome. The general examination is the safeguard that prevents the idiopathic label being applied to a syndromic foot. [10] [5]
Investigations
The diagnosis of the clubfoot is clinical, and no imaging is required in the typical idiopathic newborn. The history and the examination — the rigid foot, the deep creases, the Pirani and the Dimeglio scores, and the normal spine and the hips — are sufficient to make the diagnosis and to begin the Ponseti method. The radiograph, the ultrasound, and the magnetic resonance imaging are reserved for the atypical, the syndromic, and the complex presentations. [5] [7]
The spinal ultrasound or the magnetic resonance imaging is indicated when a syndromic clubfoot raises the suspicion of an occult spinal dysraphism. A hairy patch, a lipoma, a sacral dimple, or a haemangioma over the spine, in a child with a clubfoot, is the skin marker that prompts the imaging, and the magnetic resonance imaging reveals the tethered cord, the diastematomyelia, or the lipoma that may accompany the foot deformity. The spinal imaging is the workup that prevents the missed neural tube defect. [10]
The anteroposterior and the lateral radiographs of the foot are indicated when the congenital vertical talus is suspected — the rigid rocker-bottom foot with the convex plantar surface — because the radiograph reveals the vertical talus and the dislocated talonavicular joint that demand the surgical reduction. The radiographs are also useful in the older child with the neglected clubfoot, where the bone architecture informs the surgical plan, and in the complex clubfoot, where the casts may need to be adapted. The talocalcaneal angle on the anteroposterior view is reduced in the clubfoot (the parallelism of the talus and the calcaneus), and it increases as the correction proceeds. [7] [5]
The hip ultrasound is indicated when a syndrome raises the risk of the developmental dysplasia of the hip, or when the hip examination is abnormal, because the hip and the foot may coexist in the same child. The prenatal ultrasound, at the twenty-week scan, often detects the clubfoot before the birth, and the isolated finding on the scan carries a good prognosis, whereas the finding in the context of other anomalies raises the syndromic and the chromosomal workup. The counselling of the family, when the clubfoot is detected prenatally, is the opportunity to set the expectations and to plan the early referral. [5] [10]
Management — Resuscitation
The management of the clubfoot does not, in the typical case, demand a resuscitation. The newborn with the idiopathic clubfoot is well, and the management is the prompt referral for the Ponseti method in the first one to two weeks of life. The early initiation of the casting is the resuscitative principle, because the immature ligaments and the cartilage are most responsive in the first weeks, and the delay makes the correction harder and the relapse more likely. [1] [3]
The urgent action is reserved for the syndromic and the complex presentations. The newborn with the myelomeningocele and the clubfoot requires the neurosurgical closure of the spinal lesion as the priority, with the Ponseti casting begun thereafter, once the wound is healed. The newborn with the amniotic band and the threatened distal ischaemia requires the urgent surgical release of the constriction band. The newborn with the complex clubfoot requires the modified Ponseti method, with the recognition of the atypical features and the adaptation of the casting. [10] [8]
The multidisciplinary referral is the resuscitative safeguard. The syndromic clubfoot is referred to the paediatric orthopaedic surgeon, the neurosurgeon (for the myelomeningocele), the geneticist, and the physiotherapist, for the integrated management of the underlying syndrome alongside the foot. The family is referred to the peer-support network, because the counselling by another family who has lived through the Ponseti method is a powerful aid to the brace compliance. The general paediatrician is the coordinator of the multidisciplinary care, and the early referral is the action that prevents the late and the neglected presentation. [5]
Management — Definitive & Stepwise
The Ponseti method is the global gold standard of the clubfoot management, endorsed by the World Health Organization and the Paediatric Orthopaedic Society of North America, and delivered through the international Ponseti programmes in over one hundred countries. The method corrects the deformities in the same cavus-adductus-varus-equinus sequence that the deformities appear, and it uses the viscoelastic creep of the immature ligament to achieve the correction without the extensive surgery. [1] [3]
The Ponseti method — the five steps
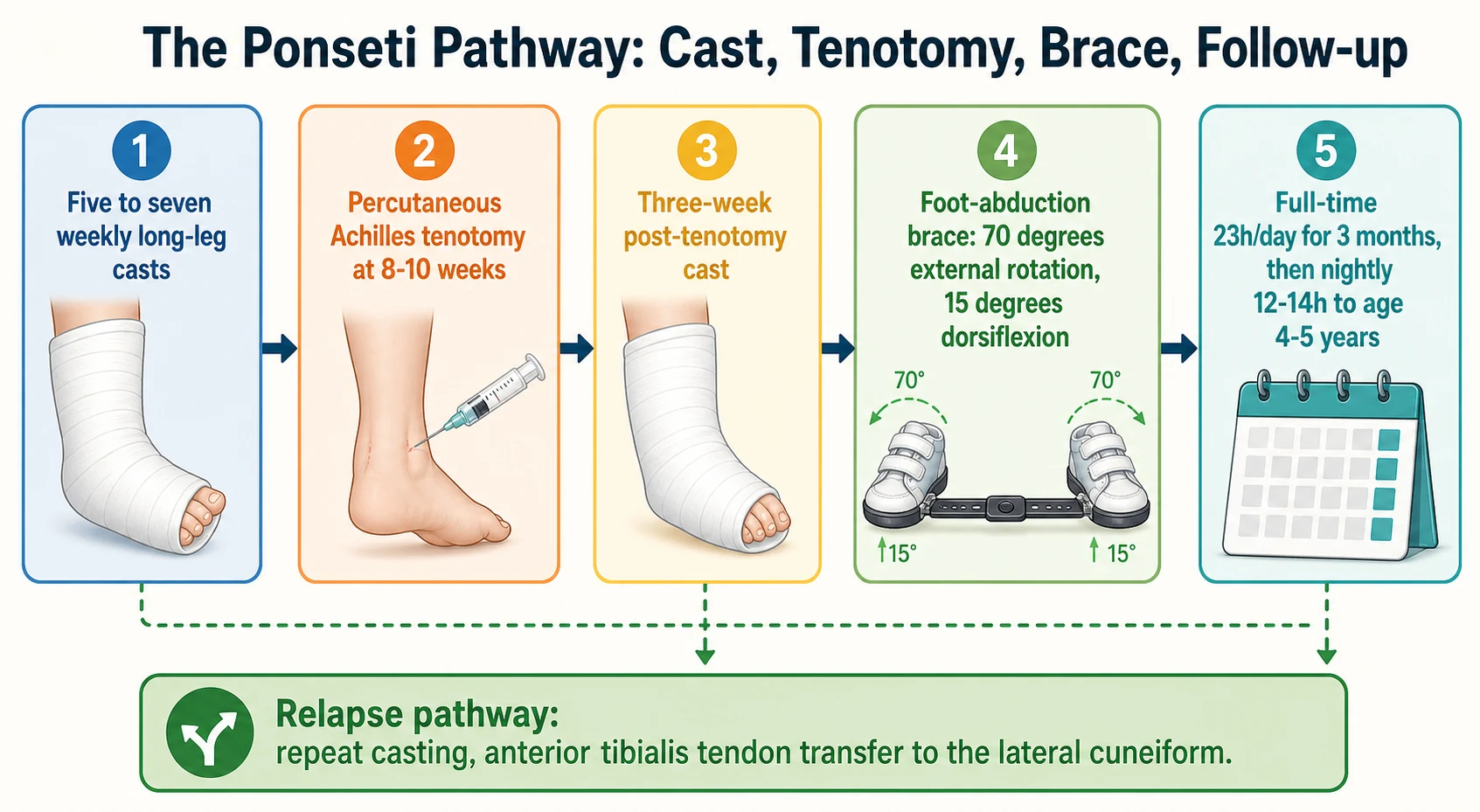
Cast one to cast five to seven: long-leg above-knee casts, changed weekly, correcting cavus (cast one), then adductus and varus together (casts two to four or five), with the foot abducted around the head of the talus and the counter-pressure on the lateral talar head.
Percutaneous Achilles tenotomy: performed at eight to ten weeks, when the cavus, adductus, and varus are corrected but the equinus persists (a Pirani hindfoot score above one), under local anaesthesia, with a small ophthalmic scalpel or a tenotomy needle, through a medial approach at the insertion or one centimetre above.
Post-tenotomy cast: the foot is dorsiflexed to fifteen degrees and held in the long-leg cast for three weeks, allowing the tendon to heal in the lengthened position.
Foot-abduction brace: the shoes-and-bar device, holding the affected foot at seventy degrees of external rotation (sixty to seventy for the affected, thirty to forty for the unaffected in the unilateral case) and fifteen degrees of dorsiflexion, worn full-time (twenty-three hours a day) for the first three months.
Nightly bracing: twelve to fourteen hours a day (night and nap), to the age of four to five years, with the brace reviewed at each clinic visit for the fit and the compliance.
The percutaneous Achilles tenotomy is performed in roughly eighty to ninety percent of the idiopathic clubfeet, and it is the step that releases the residual equinus that the casts cannot overcome. The tenotomy is a minor procedure, performed in the clinic or the theatre, under the local anaesthetic or the sedation, and the complications — the bleeding, the infection, the neurovascular injury — are rare. The post-tenotomy cast is worn for three weeks, and the foot is then transitioned to the foot-abduction brace. The early recognition of the residual equinus — by the Pirani hindfoot score above one at the end of the casting — is the trigger for the tenotomy. [1] [3]
The foot-abduction brace is the cornerstone of the long-term success. The brace holds the foot in the overcorrected position — the seventy degrees of external rotation and the fifteen degrees of dorsiflexion — and the brace compliance, not the casting and not the tenotomy, is the single greatest determinant of whether the correction lasts. The brace is worn full-time (twenty-three hours a day) for the first three months after the last cast, then nightly (twelve to fourteen hours a day, at the night and the nap) to the age of four to five years. The brace compliance is the issue that the fellowship candidate must address, because the non-compliance is the commonest cause of the relapse, and the family-centred counselling — the explanation of the rationale, the peer support, and the regular review — is the safeguard. [3] [4]
The management of the relapsed clubfoot follows a defined ladder. The relapse is most often the signature of the brace non-compliance, and the first step is the repeat Ponseti casting, with the five to seven casts and, often, a repeat percutaneous tenotomy. The dynamic supination — the foot that supinates on the swing phase of the gait, from the overpull of the anterior tibialis — is the relapse pattern that responds to the anterior tibialis tendon transfer, typically to the lateral cuneiform, performed at the age of two and a half to five years. The more extensive procedures — the posterior release, the posteromedial release, the talectomy — are reserved for the resistant few, the neglected clubfoot in the older child, and the severe syndromic foot, and they carry the higher risk of the stiffness and the arthritis that the Ponseti method was designed to prevent. [8] [6]
The management of the congenital limb anomalies is the domain of the paediatric orthopaedic surgeon and the prosthetist, and the general paediatrician's role is the early referral and the coordination of the multidisciplinary care. The fibular hemimelia is managed by the limb-lengthening (the Ilizarov or the Taylor spatial frame) in the mild to the moderate, and by the amputation (the Syme or the Boyd) and the prosthetic fitting in the severe. The tibial hemimelia is managed by the amputation and the prosthetic fitting, or by the knee reconstruction and the limb-lengthening in the selected cases. The proximal femoral focal deficiency is managed by the limb-lengthening, the rotationplasty, or the prosthetic fitting, depending on the severity. The amniotic band syndrome is managed by the urgent release of the constriction band when the distal ischaemia is threatened, and by the elective release of the band and the reconstruction of the soft-tissue defect. The polydactyly is managed by the excision of the supernumerary digit, with the reconstruction of the ligaments and the tendons, in the first one to two years of life. The syndactyly is managed by the surgical separation, with the full-thickness skin grafts, between the ages of six and eighteen months, with the border digits (the thumb-index and the ring-little) separated earlier to prevent the tethering and the deformity. [5]
Specific Subtypes & Scenarios
The idiopathic clubfoot is the commonest scenario, and it responds to the standard Ponseti method with five to seven casts, a percutaneous tenotomy in eighty to ninety percent, and a brace to four to five years. The long-term outcome, documented in the Cooper and Dietz thirty-year follow-up, is a plantigrade, painless, flexible foot in over ninety percent, with only minor strength deficits compared with the unaffected side. The patient functions normally — walks, runs, plays sport — and the only residual is the calf atrophy and the slightly smaller foot that are the legacy of the intrauterine deformity. [2] [5]
In Australia and Aotearoa New Zealand, the idiopathic clubfoot is managed through the paediatric orthopaedic services in the major centres, with the regional and the remote children supported by the outreach clinics and the telehealth. The international Ponseti programmes, run by the Ponseti International Association and the MiracleFeet charity, deliver the method in over one hundred countries, with the serial casting delivered by a trained health worker and the tenotomy by a visiting surgeon. [4] [11]
The complex clubfoot, with the deep crease and the short hyperextensible first ray, requires the modified Ponseti method. The two casts for the cavus and the adductus, the peri-talar abduction with a different hand position (the thumb on the medial malleolus rather than the lateral talar head), the early percutaneous tenotomy, and the longer casting course are the modifications. The complex clubfoot is the phenotype that the examiner rewards the candidate for recognising, because the standard Ponseti method, applied without modification, can produce the rocker-bottom foot. [5] [8]
The syndromic clubfoot of myelomeningocele, documented in the Gerlach 2009 study, responds to a modified Ponseti method that accommodates the paralytic foot and the open spinal lesion. The neurosurgical closure of the myelomeningocele is performed first, and the Ponseti casting is begun thereafter, once the wound is healed. The syndromic clubfoot is more rigid and more resistant to the casting, with a higher rate of the relapse and a greater need for the additional surgery, but the Ponseti method is still the best first-line, and the modified technique achieves the correction in the majority. [10]
The neglected clubfoot in the older child or the adolescent, presenting after years without the treatment, is the scenario that the fellowship candidate must address with the realism. The prolonged Ponseti casting may achieve a partial correction in the younger neglected child, but the older child and the adolescent more often need the extensive soft-tissue release, the talectomy (the removal of the talus), or the triple arthrodesis (the fusion of the subtalar, the talonavicular, and the calcaneocuboid joints) to achieve the plantigrade foot. The functional outcome is determined by the residual deformity and the arthritis, and the Ponseti method, even in the neglected case, is the worth-while first attempt. [5] [8]
Complications & Pitfalls
The most common complication of the clubfoot management is the relapse, seen in twenty to thirty percent of the idiopathic cases, and most often the consequence of the brace non-compliance. The relapse presents as the recurrence of the equinus, the adductus, and the varus, often within the first two to three years after the last cast. The safeguard is the family-centred brace counselling — the explanation of the rationale, the peer support, and the regular review — and the management is the repeat Ponseti casting, the repeat percutaneous tenotomy, and the anterior tibialis tendon transfer for the dynamic supination. [8] [4]
The complications of the untreated or the poorly treated clubfoot are the rigid, the painful, and the deformed foot, the limp, the callus on the lateral border, and the lifelong disability. The Ponseti method prevents these complications, and the early referral and the brace compliance are the safeguards. The overcorrected foot — the valgus and the calcaneus deformity from an extensive release — is the complication of the surgical era that the Ponseti method was designed to prevent, and it is the reason the casting and the tenotomy are preferred to the extensive release. [6] [2]
The pitfall of the persistent equinus after the casts is the failure to perform the percutaneous tenotomy when indicated. The Pirani hindfoot score above one at the end of the casting is the trigger for the tenotomy, and the foot that is dorsiflexed against the residual equinus, without the tenotomy, is the foot that develops the rocker-bottom deformity. The safeguard is the Pirani-guided tenotomy. [1] [7]
The pitfall of the missed syndromic clubfoot is the idiopathic label applied to a child with a myelomeningocele or an arthrogryposis. The safeguard is the full general examination — the spine, the hips, the upper limbs, and the facial features — at the newborn baby check, and the multidisciplinary referral when the syndromic features are present. The missed syndrome changes the management and the prognosis, and the spinal ultrasound or the magnetic resonance imaging is the workup that prevents the error. [10]
Prognosis & Disposition
The prognosis of the idiopathic clubfoot treated by the Ponseti method is excellent. The plantigrade, painless, flexible foot is achieved in over ninety percent of the idiopathic cases, and the thirty-year follow-up in the Cooper and Dietz study showed the normal function, the normal activity, and only the minor strength deficits compared with the unaffected side. The patient walks, runs, and plays sport without the limitation, and the only residual is the calf atrophy and the slightly smaller foot. The key determinant of the long-term success is the brace compliance, and the family-centred counselling is the safeguard. [2] [5]
The prognosis of the syndromic clubfoot is more guarded, with the higher rate of the relapse and the greater need for the additional surgery. The myelomeningocele clubfoot, in the Gerlach 2009 study, achieved the correction with the modified Ponseti method, but the higher relapse rate and the underlying neurological deficit shaped the long-term function. The arthrogryposis clubfoot is more rigid and more resistant, with a greater need for the extensive surgery. The Ponseti method, even in the syndromic foot, is the best first-line, and the realistic counselling of the family is the safeguard. [10]
The prognosis of the complex clubfoot is good when the modified Ponseti method is followed, with a longer casting course and a higher rate of the tenotomy, but with a good long-term outcome. The prognosis of the relapsed clubfoot is good when the repeat casting and the anterior tibialis tendon transfer are applied, with the extensive release reserved for the resistant few. The prognosis of the neglected clubfoot is determined by the residual deformity and the arthritis, and the functional outcome is the realistic measure. [8] [5]
The disposition is shared. The general paediatrician owns the newborn baby check, the referral, and the family counselling. The paediatric orthopaedic surgeon owns the casting, the tenotomy, and the surgery. The physiotherapist owns the brace fitting and the follow-up. The prosthetist and the orthotist own the congenital limb anomalies and the brace fabrication. The geneticist owns the syndromic workup. The general paediatrician is the coordinator of the multidisciplinary care, and the long-term follow-up — to the age of four to five years for the brace, and to the skeletal maturity for the growth and the relapse — is the safeguard. [5] [7]
Special Populations
The Ponseti method is adapted for the newborn with the open myelomeningocele. The neurosurgical closure of the spinal lesion is performed first, and the Ponseti casting is begun thereafter, once the wound is healed. The modified technique accommodates the paralytic foot, with the gentler manipulation, the longer casting course, and the higher rate of the tenotomy. The multidisciplinary spina bifida service coordinates the orthopaedic, the neurosurgical, the urological, and the developmental care, and the family is counselled on the realistic prognosis. [10]
The Ponseti method is adapted for the child in the low-resource or the remote setting. The serial casting is delivered by a trained health worker — the nurse, the physiotherapist, or the community health worker — and the percutaneous tenotomy is performed by a visiting surgeon. The foot-abduction brace is fabricated locally, from the affordable materials, and the follow-up is supported by the telehealth. The international Ponseti programmes, run by the Ponseti International Association and the MiracleFeet charity, deliver the method in over one hundred countries, and the low-cost, the high-impact nature of the method is the reason it is the global standard. [4] [11]
The congenital limb anomaly in the Indigenous or the socioeconomically disadvantaged child is managed with the culturally safe, the family-centred care. The higher prevalence of certain conditions, the barriers to the prosthetic fitting and the follow-up, and the geographical distance from the specialist centre are the challenges that the outreach clinics, the telehealth, and the peer-support networks address. The early referral and the coordination of the multidisciplinary care are the safeguards. [5]
The counselling of the family of the child with the clubfoot or the congenital limb anomaly is approached with the plain language, the realistic prognosis, and the long-term plan. The family is told that the clubfoot is a treatable condition, that the Ponseti method is the gold standard, and that the brace is the key to the permanent correction. The family is told that the congenital limb anomaly is managed by the multidisciplinary team, that the prosthetic fitting and the follow-up are the long-term commitment, and that the child will walk and function. The peer-support networks — the clubfoot support groups, the limb-difference associations — are the powerful aid, and the counselling by another family who has lived through the journey is the safeguard. [5] [3]
Evidence, Guidelines & Regional Differences
The Ponseti 1992 paper, "Treatment of congenital club foot" in the Journal of Bone and Joint Surgery, established the method of the serial casting and the percutaneous tenotomy that became the global gold standard. The paper codified the biomechanical sequence — the cavus first, then the adductus and the varus together, then the equinus last — and it reported the outcomes that overturned the assumption of the surgical era. The problem the paper solved was the high rate of the stiffness, the pain, and the arthritis that followed the extensive soft-tissue release, and the solution was the minimally invasive casting method that corrected the deformities by the viscoelastic creep. [1]
The Cooper and Dietz 1995 thirty-year follow-up paper showed that the patients treated by the Ponseti method had the near-normal function, the painless feet, and only the minor strength deficits at thirty years. The paper overturned the assumption that the early results would not last, and it established the Ponseti method as the durable, the long-term solution. The Morcuende 2004 paper showed the radical reduction in the rate of the extensive posterior and the posteromedial release when the Ponseti method was adopted at the Iowa centre — from the high rate of the surgery to the very low rate — and it changed the standard of care. [2] [3]
Cooper & Dietz 1995 — 30-year follow-up of the Ponseti method
Retrospective review of 45 patients (71 feet) treated by the Ponseti method, with the mean follow-up of 34 years, compared with the age-matched controls.
Key finding
The treated patients had the near-normal function, the painless feet, and only the minor strength deficits (an average of about 15 percent less calf strength and 10 percent less foot mobility) compared with the controls. No patient had the limitation of the activity, and the satisfaction was high.
The Jowett 2011 systematic review and the Ganesan 2017 systematic review confirmed the high initial correction rate of the Ponseti method — over ninety percent in the idiopathic clubfoot — and the importance of the brace compliance for the long-term success. The relapse rate, when the brace is not worn, rises to the eighty percent, and the relapse rate, when the brace is worn, falls to the twenty to thirty percent. The Smith 2014 comparison of the Ponseti method with the comprehensive release showed the better long-term outcome of the Ponseti method, with the less stiffness and the less pain. [4] [11] [6]
The controversies — the accelerated versus the standard Ponseti casting (the casts changed every five days rather than weekly, with the similar outcomes), the early versus the late tenotomy (the tenotomy guided by the Pirani hindfoot score), the role of the botulinum toxin as an adjunct to the tenotomy (the variable evidence), the anterolateral tibialis transfer at the time of the relapse (the dynamic supination) — are the questions that the fellowship answer names without resolving. The Canavese and Dimeglio 2021 review and the Masrouha 2021 relapsed-clubfoot review are the contemporary references that guide the practice, and the Zionts 2017 sex-and-laterality study informs the severity assessment. [7] [8] [9]
The Ponseti method is endorsed by the World Health Organization and the Paediatric Orthopaedic Society of North America, and it is delivered through the international Ponseti programmes in over one hundred countries. The method is low-cost, high-impact, and culturally adaptable, and it is the global standard of the clubfoot management. The MiracleFeet brace, the affordable foot-abduction brace, has expanded the access to the brace in the low-resource settings. [3] [11]
Exam Pearls
The fellowship answer turns on five facts. The first is the CAVE mnemonic — the cavus, the adductus, the varus, and the equinus — the four deformities in the order the Ponseti method corrects them. The second is the Ponseti method as the gold standard — the five to seven weekly long-leg casts, the percutaneous tenotomy at eight to ten weeks, and the foot-abduction brace to four to five years. The third is the brace compliance as the single greatest determinant of the long-term success, and the relapse as the signature of the non-compliance. The fourth is the relapse managed by the repeat casting and the anterior tibialis tendon transfer. The fifth is the Pirani and the Dimeglio scores as the bedside severity systems. [1] [7]
The three examiner traps are the following. The first is the positional clubfoot taken for the idiopathic — the flexible, passively correctable foot that needs no casting, distinguished from the rigid structural foot by the rigidity test. The second is the syndromic clubfoot missed for the idiopathic — the myelomeningocele, the arthrogryposis, the diastrophic dysplasia — distinguished by the full general examination and the spinal imaging. The third is the rocker-bottom foot produced by the incorrect casting sequence — the dorsiflexion forced before the varus is corrected — distinguished by the convex plantar surface and prevented by the correct sequence. [5] [8]
What is the single most important determinant of long-term success in the Ponseti method?
The foot-abduction brace compliance. The brace is worn twenty-three hours a day for the first three months after the last cast, then nightly to the age of four to five years, and the non-compliance is the commonest cause of the relapse. The family-centred counselling, the peer support, and the regular review are the safeguards. [3] [4]
References
- [1]Ponseti IV. Treatment of congenital club foot. Journal of Bone and Joint Surgery. American Volume, 1992.PMID 1548277
- [2]Cooper DM, Dietz FR. Treatment of idiopathic clubfoot. A thirty-year follow-up note. Journal of Bone and Joint Surgery. American Volume, 1995.PMID 7593056
- [3]Morcuende JA, Dolan LA, Dietz FR, Ponseti IV. Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics, 2004.PMID 14754952
- [4]Jowett CR, Morcuende JA, Ramachandran M. Management of congenital talipes equinovarus using the Ponseti method: a systematic review. Journal of Bone and Joint Surgery. British Volume, 2011.PMID 21911524
- [5]Chu A, Lehman WB. Treatment of Idiopathic Clubfoot in the Ponseti Era and Beyond. Foot and Ankle Clinics, 2015.PMID 26589078
- [6]Smith PA, Kuo KN, Graf AN, Krzak J. Long-term results of comprehensive clubfoot release versus the Ponseti method: which is better? Clinical Orthopaedics and Related Research, 2014.PMID 24249539
- [7]Canavese F, Dimeglio A. Clinical examination and classification systems of congenital clubfoot: a narrative review. Annals of Translational Medicine, 2021.PMID 34423009
- [8]Masrouha K, Chu A, Lehman W. Narrative review of the management of a relapsed clubfoot. Annals of Translational Medicine, 2021.PMID 34423014
- [9]Zionts LE, Jew MH, Ebramzadeh E, Sangiorgio SN. The Influence of Sex and Laterality on Clubfoot Severity. Journal of Pediatric Orthopaedics, 2017.PMID 26214324
- [10]Gerlach DJ, Gurnett CA, Limpaphayom N, Alaee F, Zhang Z, Porter K, Kirchhofer M, Smyth MD, Dobbs MB. Early results of the Ponseti method for the treatment of clubfoot associated with myelomeningocele. Journal of Bone and Joint Surgery. American Volume, 2009.PMID 19487512
- [11]Ganesan B, Luximon A, Al-Jumaily A, Balasankar SK, Naik GR. Ponseti method in the management of clubfoot under 2 years of age: A systematic review. PLoS One, 2017.PMID 28632733
- [12]Wynne-Davies R. Family studies and the cause of congenital club foot. Talipes equinovarus, talipes calcaneo-valgus and metatarsus varus. Journal of Bone and Joint Surgery. British Volume, 1964.PMID 14216453