Paeds · rheumatology-musculoskeletal-and-sports
Concussion and return to learn or play
Also known as sport-related concussion · mild traumatic brain injury · concussion · return to learn · return to sport · return to play · SCAT6 · Child SCAT6 · Amsterdam consensus · persistent post-concussive symptoms
A fellowship approach to sport-related concussion in the child and adolescent, anchored by the 2022 Amsterdam Consensus Statement and its tools — the SCAT6 for athletes thirteen years and older and the Child SCAT6 for children six to twelve — built around the two graduated pathways that decide safe recovery: return to learn first, then a six-stage return to sport, with twenty-four to forty-eight hours of relative rest, no prolonged cocoon therapy, and a red-flag screen that sends the deteriorating child to the emergency department.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A fourteen-year-old rugby player is helped off the field after a tackle, dazed and slow to rise, with a headache and a feeling of being foggy — a textbook sport-related concussion recognised at the sideline. An eight-year-old falls from a trampoline and bumps her head, vomits twice on the way to the clinic, and the task is to run the red-flag screen and to decide whether this is an emergency or a graduated recovery. A sixteen-year-old netballer is back at school but still has headaches and poor concentration a month after her injury, and the task is to recognise persistent post-concussive symptoms and to build the multidisciplinary plan. The fellowship skill in each is to assess the child, to place them on the right ladder, and to keep them safe through the recovery. [1] [6]
Two ladders, learn before sport
Overview & Definition
Concussion is the commonest form of traumatic brain injury seen in children and adolescents, and it sits at the centre of paediatric sports medicine because the decisions made in the days after a head knock change the trajectory of recovery. The 2022 Amsterdam Consensus Statement defines a concussion as a traumatic brain injury caused by a direct or an indirect blow to the head, with a short-lived impairment of neurological function that resolves spontaneously, and with symptoms that may or may not involve loss of consciousness. [1] [6] The disturbance reflects a functional brain injury rather than a structural one, and standard structural neuroimaging is normal, which is why the diagnosis is clinical and the imaging is reserved for the red-flag presentation. [8]
The clinical importance comes from what the recognition unlocks. A child whose concussion is missed returns to play, takes a second impact, and risks the rare but catastrophic second impact syndrome, while a child whose concussion is recognised but managed with prolonged strict rest develops the isolation, the deconditioning, and the persistent symptoms that cocoon therapy produces. [12] [5] The fellowship answer holds both risks at once. The child is assessed with the age-appropriate tool, given twenty-four to forty-eight hours of relative rest, returned to learn before sport, and progressed through the six-stage return to sport with a red-flag screen that runs throughout. [1] [4]
Classification
The classification of a concussion runs along two axes that together frame the assessment and the recovery. The first axis is the age band, because the assessment tool is chosen by the age, and the child's brain recovers more slowly than the adult's. The second axis is the symptom domain, because the symptoms cluster into the somatic, the cognitive, the emotional, and the sleep groups, and the pattern and the burden frame the recovery and the risk of persistence. [2] [3]
The tool is age-banded. The SCAT6 is designed for the athlete thirteen years and older, and it carries the symptom evaluation, the cognitive components of orientation, immediate memory, concentration, and delayed recall, and the balance and coordination components. [2] The Child SCAT6 is designed for the child six to twelve years, and it modifies the cognitive and the symptom items for the younger child and adds a parent-report component, because the standard tool overestimates symptoms and underperforms in the younger age group. [3] The on-field recognition before the tool uses the observable signs, the Maddocks questions, the red-flag check, and the Concussion Recognition Tool, and these frame the immediate removal from play. [1]
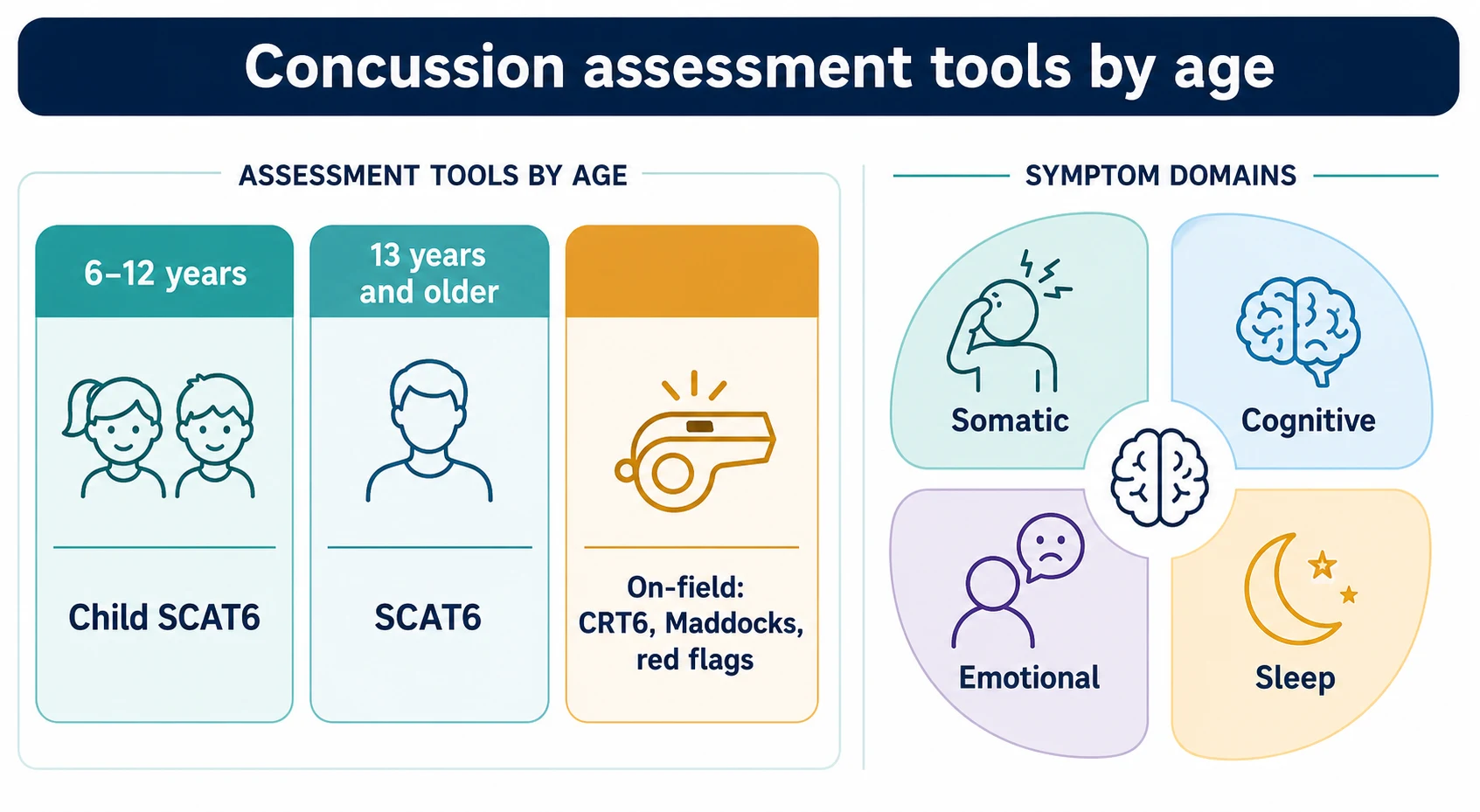
The symptoms cluster into four domains. The somatic symptoms are the headache, the dizziness, the nausea, and the sensitivity to light and noise. The cognitive symptoms are the feeling of being foggy, the poor concentration, and the memory difficulty. The emotional symptoms are the irritability, the sadness, and the anxiety. The sleep symptoms are the drowsiness, the sleeping more or less than usual, and the trouble falling asleep. [1] [7] A higher symptom burden at the first presentation is one of the strongest predictors of a prolonged recovery, and the symptom count frames the risk from the outset. [5] [6]
Epidemiology & Risk Factors
Concussion is among the commonest injuries in paediatric sport, and its epidemiology tracks the collision and the contact sports and the age of the athlete. The sports that carry the highest rates are the collision and the contact sports — the rugby, the Australian-rules football, the soccer, and the ice hockey — and the rates rise through adolescence as the play becomes faster and the forces larger. [7] [6] Girls appear to have higher concussion rates than boys in comparable sports, and the reasons are thought to include the weaker neck strength and the hormonal factors, although the reporting difference may also contribute. [10] [6]
The risk factors for a concussion cluster around the exposure and the individual. A prior concussion raises the risk of a further concussion, and a higher level of competition, a history of migraine, and a learning or an attention disorder each raise the risk and the severity. [5] [7] The risk factors for a prolonged recovery, or for the persistent post-concussive symptoms, are the features the fellowship candidate names at the first visit. The adolescent and the female sex recover more slowly, a high symptom burden at the presentation is the strongest predictor of persistence, and a prior concussion, a migraine history, a mood or an anxiety disorder, and a learning difficulty or an attention deficit each add to the risk. [6] [10]
Loss of consciousness is not a strong predictor of a prolonged recovery, and its absence does not exclude a concussion, which is the common error the history must correct. [1] [7] The cognitive and the emotional symptoms at the presentation, and the sleep disturbance, carry more weight for the prognosis than the single fact of a blackout, and the fellowship answer frames the risk from the symptom burden and the background rather than from the loss of consciousness alone. [5] [6]
Pathophysiology
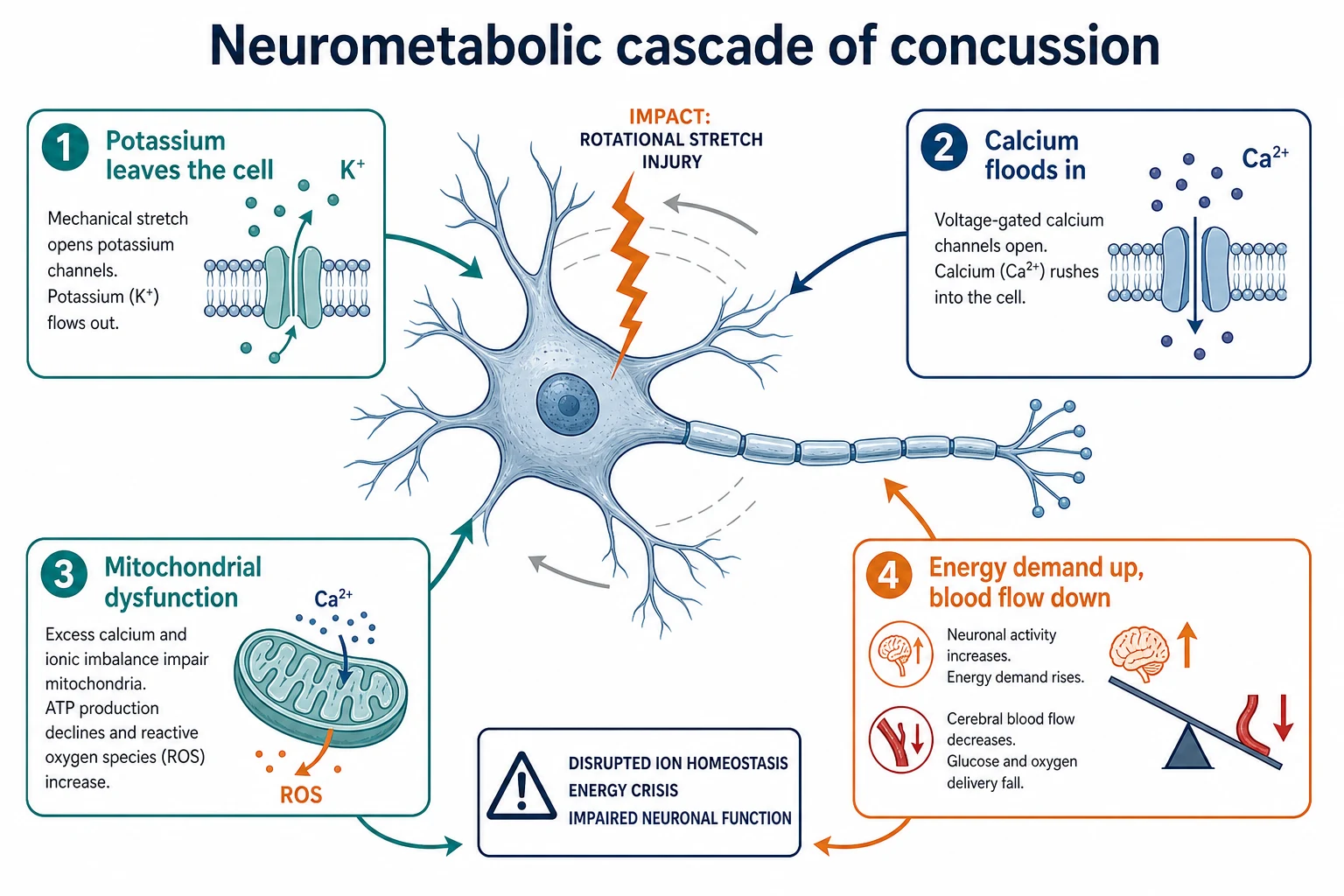
The pathophysiology of a concussion is a functional injury of the brain rather than a structural one, and the mechanism is the stretch of the neurons produced by the rotational acceleration of the head. The blow, whether direct to the head or to the body, accelerates the head and rotates the brain within the skull, and the neurons stretch and the axons deform. [1] [8] The stretch triggers the neurometabolic cascade that underlies the symptoms, and the cascade is a cascade of ion flux, energy demand, and reduced blood flow that leaves the brain in an energy crisis. [9] [8]
The cascade begins with the ion flux. The stretched neurons leak potassium out of the cell and flood calcium in, the ion pumps work hard to restore the balance, and the energy demand of the brain rises sharply at the very moment the cerebral blood flow falls. [9] The mitochondria, overloaded by the calcium, dysfunction, and the mismatch between the raised energy demand and the reduced supply produces the energy crisis that underlies the symptoms and the vulnerability of the brain to a second impact in the early window. [8] [9]
The pathophysiology explains the two pillars of the management. The energy crisis explains why twenty-four to forty-eight hours of relative rest helps in the acute window, because the recovering brain needs a reduced load. The same crisis explains why prolonged strict rest harms, because the deconditioning, the isolation, and the loss of the routine worsen the symptoms and the mood, and the early sub-symptom-threshold aerobic exercise aids the recovery by restoring the cerebral autoregulation and the blood flow. [5] [11] The fellowship candidate uses the pathophysiology to justify the short rest and the early activity, and to reject the cocoon therapy that older practice taught. [1] [6]
Clinical Presentation
The presentation is driven by what the child and the witnesses describe, and the chief complaint after a head knock is a change in the way the child feels, thinks, or behaves rather than a structural sign. The somatic symptoms are the headache, the dizziness, the nausea, and the sensitivity to light and noise, and these are the commonest of the early symptoms. [7] [1] The cognitive symptoms are the feeling of being in a fog, the poor concentration, the slowed thinking, and the memory difficulty, and the child may say that they cannot follow the lesson or that they feel behind. [2] [6]
The emotional and the sleep symptoms complete the picture. The child may be irritable, sad, or more emotional than usual, and the sleep may be disturbed with the drowsiness, the sleeping more than usual, or the trouble falling asleep. [7] [1] Loss of consciousness occurs in only a minority of concussions, and the absence of a blackout never excludes the diagnosis, which is the error the history must correct. The onset is immediate in most cases, although some symptoms evolve over the first hours, and the red-flag screen is run at every encounter to separate the concussion from the evolving intracranial injury. [8] [1]
The presentation of the persistent case is the symptoms that fail to resolve. A child with persistent post-concussive symptoms has the headache, the poor concentration, the fatigue, and the mood change that persist or worsen beyond the expected four-week window, and the school performance often declines because the cognitive load of the classroom exceeds the recovering brain. [5] [6] The history at this stage elicits the risk factors — the high initial symptom burden, the prior concussion, the migraine, the anxiety, and the learning difficulty — and frames the multidisciplinary plan that the persistent case needs. [10] [6]
Differential Diagnosis
The differential diagnosis of the acute head-injury presentation is the fork between the uncomplicated concussion and the evolving intracranial injury, and the red-flag screen decides it. The uncomplicated concussion has the symptoms described and a normal examination, and the management is the graduated recovery. [1] [8] The evolving intracranial injury — the intracranial bleed, the cerebral oedema, or the skull fracture — declares itself through the red flags of the deteriorating consciousness, the repeated vomiting, the severe or the worsening headache, the seizure, the focal neurological deficit, and the unequal pupils, and the pathway is the emergency assessment and the imaging. [8] [9]
The cervical spine injury is the differential that the assessment must never miss. A child with a neck pain or a midline cervical tenderness after a head injury may have a cervical spine injury, and the management is the spinal precautions, the immobilisation, and the imaging of the spine before any further assessment or any movement. [8] [1] The fellowship candidate states aloud that the cervical spine is cleared before the child is moved, because the missed cervical injury is the harm that the assessment prevents. [8] [7]
The differential of the persistent symptoms is the set of the mimics and the contributors. The post-traumatic headache may coexist with a pre-existing migraine, the dizziness may reflect a vestibular or a cervicogenic component, and the mood and the sleep disturbance may reflect an anxiety or a depression that the injury has uncovered. [5] [6] The persistent symptoms may also signal a missed intracranial injury or a post-traumatic seizure in the rare case, and the persistent or the atypical course is the trigger for the imaging and the specialist review that the straightforward recovery never needs. [9] [10]
Clinical & Bedside Assessment
The assessment begins at the sideline and continues in the clinic, and the first task is the red-flag screen that separates the concussion from the emergency. Check the level of consciousness, the pupil size and the reactivity, the cervical spine for the pain and the tenderness, and the limbs for the focal weakness. [8] [1] A deteriorating consciousness, a drowsiness that cannot be roused, a repeated vomiting, a severe or a worsening headache, a seizure, a focal deficit, or an unequal pupil is the red flag that sends the child to the emergency department and the imaging, and the absence of these is the licence to proceed with the concussion assessment. [8] [9]
The tool is then chosen by the age. The SCAT6 is used for the athlete thirteen years and older, and the Child SCAT6 is used for the child six to twelve, and the tool frames the symptom evaluation, the cognitive testing, and the balance and the coordination. [2] [3] The cognitive components assess the orientation, the immediate memory, the concentration, and the delayed recall, and the balance components use the modified Balance Error Scoring System and the tandem gait. [2] The Child SCAT6 modifies these for the younger child and adds the parent report, and the right tool avoids the over- and the under-diagnosis that the wrong tool produces. [3]
Which findings must never be dismissed? The child who is dazed, who has a blank or a vacant look, who is slow to respond, or who shows the poor balance or the slurred speech is removed from play and not returned the same day, because the same-day return risks the second impact. [1] [12] The neurological examination of the cranial nerves, the limbs, and the cervical spine is performed on every child, the cervical spine is cleared before the child is moved, and the cognitive and the symptom assessment is repeated because the recovery is tracked against the baseline of the first assessment. [8] [6]
Investigations
The investigation of the straightforward concussion is the clinical assessment, because the diagnosis is clinical and the imaging is normal and therefore unhelpful. A child with the typical symptoms, a normal examination, and a negative red-flag screen needs no computed tomography, no magnetic resonance imaging, and no blood test, and the imaging in this setting exposes the child to radiation and the family to anxiety without changing the management. [1] [8] The imaging is reserved for the child in whom an intracranial injury is suspected. [9] [8]
A computed tomography of the head is the first-line imaging when an intracranial injury is suspected, and it is taken for the deteriorating consciousness, the repeated vomiting, the severe headache, the seizure, the focal deficit, the suspected skull fracture, or the dangerous mechanism. [8] [9] The computed tomography reveals the intracranial bleed, the cerebral oedema, and the skull fracture that the red flags point to, and a normal scan in the presence of the typical symptoms confirms the concussion and frames the graduated recovery. [8] [1]
The magnetic resonance imaging is reserved for the persistent or the atypical case. A child whose symptoms persist beyond the expected window, or whose course is atypical, may have the magnetic resonance imaging to exclude the rare structural cause, and the persistent case is the trigger for the specialist review and the neuropsychology. [5] [6] The fellowship answer reserves the imaging for the red-flag and the persistent presentations, and it never images the straightforward concussion, because the stewardship of the consultation is to match the investigation to the clinical picture. [9] [8]
Management — Resuscitation
Resuscitation is rarely the task in the child with a straightforward concussion, because the airway, the breathing, and the circulation are intact and the threat is functional rather than structural. The rare exception is the child who presents with an evolving intracranial injury or a cervical spine injury, and in whom the priority is the airway, the breathing, the circulation, the cervical spine immobilisation, and the urgent imaging. [8] [9] The fellowship candidate states aloud that the resuscitation is run on the deteriorating child while the emergency team and the neurosurgical team are called, and that the straightforward concussion moves straight to the graduated recovery. [1] [8]
The acute care at the sideline is the removal from play, the red-flag screen, and the avoidance of the same-day return. A child who is suspected of a concussion is removed from play, assessed, and not returned to the game the same day, because the second impact in the vulnerable window risks the second impact syndrome. [12] [1] The child is observed, given the advice on the relative rest, and the family is given the safety-net for the red flags that would bring them back to the emergency department. [8] [7]
Management — Definitive & Stepwise
The definitive management of the concussion is the twenty-four to forty-eight hours of relative rest followed by the early symptom-limited activity, and the evidence is clear that the prolonged strict rest harms the recovery. The child is advised the relative rest for the first twenty-four to forty-eight hours, with the reduced physical and the cognitive load, and then the early and the gradual return to the activity that does not worsen the symptoms. [1] [5] The cocoon therapy — the prolonged rest in a dark room — is rejected, because it increases the isolation, the deconditioning, the anxiety, and the persistent symptoms, and the contemporary evidence frames the short rest and the early activity as the standard. [5] [11]
The first ladder is the return to learn, and it precedes the return to sport. The child begins with the light daily activity, moves to the schoolwork at home, then returns to school part-time, then full-time with the accommodations, and then the full school without the accommodations. [4] [1] The accommodations are the reduced cognitive load — the shorter days, the extra time, the reduced screen time, the quiet space, and the breaks — and they are tapered as the symptoms ease. The return to learn is the priority, because the cognitive recovery is the foundation of the safe return to sport, and the child who is back at school tolerating the cognitive load is the child who is ready to begin the sport ladder. [6] [4]
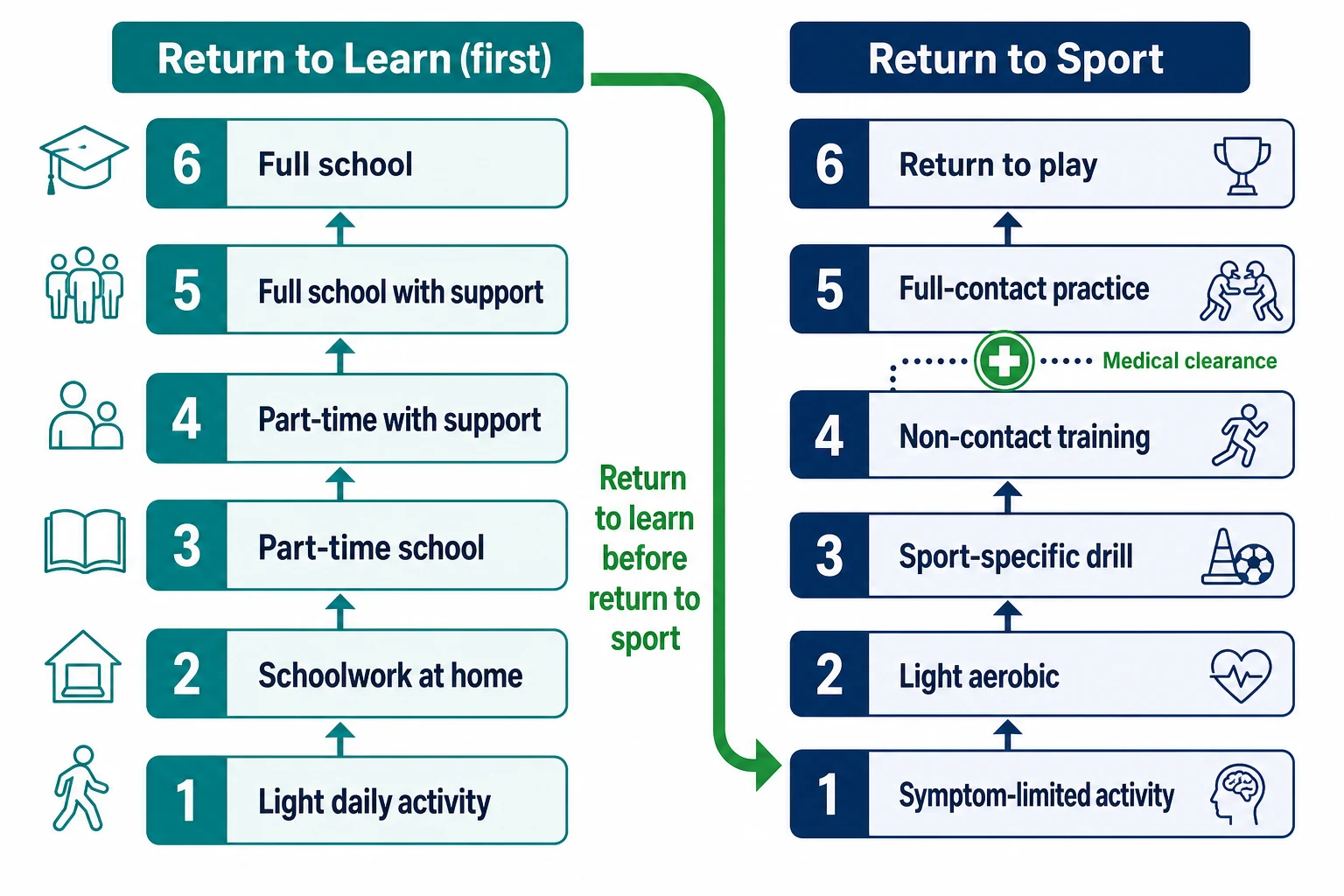
The second ladder is the six-stage return to sport, and it begins only after the child has returned to learn. The first stage is the symptom-limited activity, the second is the light aerobic, the third is the sport-specific drill, the fourth is the non-contact training, the fifth is the full-contact practice after the medical clearance, and the sixth is the return to play. [1] [4] Each stage is held for at least twenty-four hours, the child drops back a stage if the symptoms worsen, and no child moves to the full-contact practice without the medical clearance from a healthcare professional. The progression is symptom-led, and the early sub-symptom-threshold aerobic exercise aids the recovery in the child whose symptoms persist. [11] [5]
The six stages of the return to sport
Specific Subtypes & Scenarios
The adolescent with the persistent symptoms is the subtype that tests the fellowship candidate. A sixteen-year-old whose headaches and the poor concentration persist beyond four weeks has the persistent post-concussive symptoms, and the risk factors are often present — the high initial symptom burden, the female sex, the migraine history, and the anxiety. [6] [5] The management shifts from the graduated recovery to the structured multidisciplinary plan, with the targeted therapies for the headache, the vestibular or the cervicogenic dizziness, and the mood, and the sub-symptom-threshold aerobic program that the evidence supports. [11] [5]
The younger child is the subtype that needs the right tool. A seven-year-old is assessed with the Child SCAT6 rather than the SCAT6, because the standard tool overestimates the symptoms and underperforms in the younger age group, and the parent report is added. [3] [6] The younger child recovers more slowly than the adult, and the return to learn is the priority, with the close liaison with the school and the teacher to titrate the cognitive load and the accommodations as the symptoms ease. [10] [4]
The child with the learning difficulty or the attention disorder is the subtype at the higher risk. A child with the pre-existing learning difficulty or the attention deficit has a higher risk of the concussion and a higher risk of the prolonged recovery, and the management integrates with the existing education and the health plan. [5] [7] The child in the rural or the remote setting is the subtype that tests the access. The telehealth and the shared care with the local team bridge the distance, the safety-net is reinforced, and the family is given the clear criteria for the emergency return. [8] [6]
Complications & Pitfalls
The complications of the concussion are the harms on both sides of the line. The harm of the prolonged rest is the cocoon therapy that the older practice taught, and it costs the child the isolation, the deconditioning, the anxiety, the depressive symptoms, and the persistent symptoms that the prolonged inactivity produces. [5] [11] The contemporary evidence frames the twenty-four to forty-eight hours of relative rest and the early activity as the standard, and the stewardship of the consultation is to remove the prolonged rest from the management of the typical child. [1] [6]
The harm of the under-management is the missed second-impact risk and the missed persistent symptoms. A child who returns to the contact sport before the recovery takes a second impact, and the second impact in the vulnerable window risks the rare but catastrophic second impact syndrome with the diffuse cerebral swelling. [12] [1] The safeguard is the no-same-day return, the medical clearance before the full-contact stage, and the symptom-led progression through the six stages. The missed persistent case is the related harm, and the safeguard is the structured multidisciplinary review at the four-week mark for the child whose symptoms have not resolved. [5] [6]
The pitfall of the wrong tool is the error that the age-banded assessment prevents. A younger child assessed with the SCAT6 rather than the Child SCAT6 is over-diagnosed with the symptoms and under-served by the cognitive items, and the wrong tool distorts the assessment from the outset. [3] [6] The pitfall of the imaging over-use is the computed tomography applied to the straightforward concussion, and the safeguard is the red-flag screen that reserves the imaging for the evolving injury. [9] [8]
Prognosis & Disposition
The prognosis of the straightforward concussion is excellent, and the resolution within four weeks is the rule for most children and adolescents. The symptoms peak in the first days, ease with the twenty-four to forty-eight hours of relative rest, and the child returns to learn within days and to sport within about four weeks through the six-stage pathway. [1] [4] A minority of the children — those with the high initial symptom burden, the adolescent age, the female sex, the prior concussion, and the migraine or the mood background — develop the persistent post-concussive symptoms, and the prognosis for these improves with the structured multidisciplinary care and the sub-symptom-threshold aerobic exercise. [11] [5]
The prognosis of the second-impact case is the rare but the severe one. The second impact syndrome carries a high mortality and morbidity, and it is prevented by the no-same-day return, the symptom-led progression, and the medical clearance before the full contact. [12] [1] The fellowship candidate names the second-impact risk as the reason for the caution, and frames the graduated pathway as the safeguard that removes it. [8] [6]
The disposition is shared between the general paediatrician, the sports-medicine physician, and the school. The general paediatrician or the sports-medicine physician owns the assessment, the tool, the graduated pathway, and the medical clearance, and the school owns the return-to-learn accommodations through the liaison with the teacher and the family. [4] [6] The persistent case is referred to the multidisciplinary concussion service, with the neurology, the neuropsychology, the physiotherapy for the vestibular and the cervicogenic components, and the psychology for the mood. The fellowship answer names the right specialist for the right stage and never holds a deteriorating child in the graduated pathway. [5] [8]
Special Populations
Children with the developmental disabilities and the neurodiversity present particular challenges in the concussion assessment. A child with the autism or the intellectual disability may report the symptoms differently, the baseline behaviour may complicate the assessment, and the tool is used with the adaptation and the caregiver report. [6] [3] The threshold for the specialist review is lower, and the return-to-learn plan is integrated with the existing education plan, because the cognitive and the sensory load of the classroom may be harder for the recovering child with the neurodiversity. [5] [7]
The socioeconomically disadvantaged child faces the additional burden of the access. The graduated pathway needs the close follow-up, the school liaison, and the clear safety-net, and the disadvantaged setting may limit the access to the clinic, the sports-medicine physician, and the multidisciplinary service. [8] [6] The telehealth and the shared care bridge the gap, the safety-net is reinforced, and the public-health messaging on the recognition and the management is the population-level intervention that the fellowship answer acknowledges. [7] [8]
The Indigenous and the remote child carries the combined considerations. The higher rates of the injury in some settings, the reduced access to the specialist services, and the cultural and the linguistic factors shape the assessment and the plan, and the family is engaged with the cultural respect and the interpreter where needed. [6] [8] The fellowship candidate does not close the concussion assessment at the sideline, because the follow-up and the graduated pathway are the management, and the access and the equity frame the delivery. [4] [7]
Evidence, Guidelines & Regional Differences
The evidence base for the paediatric concussion rests on the 2022 Amsterdam Consensus Statement and its accompanying systematic reviews. The consensus statement, from the sixth International Conference on Concussion in Sport, updated the definition, the tools, and the graduated pathways, and it formalised the rejection of the prolonged strict rest and the endorsement of the early symptom-limited activity. [1] [6] The systematic review of the clinical recovery from concussion by Putukian and Purcell framed the return to school and the return to sport, and the review of the targeted interventions by Schneider confirmed that the early sub-symptom-threshold exercise aids the recovery while the prolonged rest harms it. [4] [5]
The tool evidence rests on the SCAT6 and the Child SCAT6. Echemendia introduced the SCAT6 for the athlete thirteen years and older, with the updated symptom, cognitive, and balance components, and Davis introduced the Child SCAT6 for the child six to twelve, with the age-appropriate modification and the parent report. [2] [3] The paediatric-specific recommendation from the Amsterdam consensus, published by Davis in Pediatrics, translated the consensus for the child and the adolescent, and it is the single best reference for the fellowship answer. [6]
The guideline evidence rests on the American Academy of Pediatrics and the Centers for Disease Control. The AAP clinical report on the sport-related concussion in the children and the adolescents framed the management for the primary care, and the CDC guideline on the mild traumatic brain injury in the children, with its accompanying systematic review, set the diagnostic and the management standards across the age range. [7] [8] The exercise evidence rests on the Leddy group, and the Chizuk study confirmed that the adolescents who adhered to the aerobic exercise prescription recovered faster, framing the sub-symptom-threshold exercise as the active treatment. [11] [5]
The regional differences are modest but real. The rates of the concussion vary with the sport and the latitude, the access to the sports-medicine physician and the multidisciplinary service varies with the setting, and the school-return policies vary with the jurisdiction. [6] [4] The Amsterdam consensus and the CDC guideline are adopted broadly across the regions, and the fellowship answer names the local guideline and the local access without pretending that a single algorithm resolves every consultation. [1] [8]
Exam Pearls
The fellowship answer turns on five facts. A concussion is a mild traumatic brain injury with the short-lived neurological symptoms and the normal imaging, and the diagnosis is clinical. The SCAT6 is for the athlete thirteen years and older and the Child SCAT6 is for the child six to twelve. Twenty-four to forty-eight hours of relative rest is followed by the early symptom-limited activity, and the prolonged strict rest is rejected. The child returns to learn before the return to sport, and the return to sport is the six stages that end in the full return to play after the medical clearance. And the red flags — the deteriorating consciousness, the repeated vomiting, the severe headache, the seizure, the focal deficit, the unequal pupils, and the cervical pain — send the child to the emergency department. [1] [6]
The examiner probes three traps. The first is the prolonged-rest trap — a child placed in the cocoon therapy that the evidence rejects, and the safeguard is the twenty-four to forty-eight hours of relative rest and the early activity. [5] [11] The second is the missed second-impact risk — an athlete returned to the contact sport before the recovery, and the safeguard is the no-same-day return and the medical clearance before the full contact. [12] [1] The third is the missed persistent case — a child whose symptoms at four weeks are dismissed as the slow recovery, and the safeguard is the structured multidisciplinary review at the four-week mark. [6] [5]
The examiner rewards the candidate who frames the concussion as a safety exercise rather than a list. The child is assessed with the age-appropriate tool, the red-flag screen is run, the relative rest and the early activity begin, the return to learn precedes the return to sport, and the six-stage pathway ends in the medical clearance. A candidate who shows this safety and this stewardship — the recognition, the graduated recovery, and the vigilant red-flag screen — demonstrates the systems thinking that the fellowship demands. [1] [4]
References
- [1]Patricios JS, Schneider KJ, Dvorak J, et al. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport-Amsterdam, October 2022. Br J Sports Med, 2023.PMID 37316210
- [2]Echemendia RJ, Brett BL, Broglio S, et al. Sport concussion assessment tool - 6 (SCAT6). Br J Sports Med, 2023.PMID 37316203
- [3]Davis GA, Echemendia RJ, Ahmed OH, et al. Introducing the Child Sport Concussion Assessment Tool 6 (Child SCAT6). Br J Sports Med, 2023.PMID 37316202
- [4]Putukian M, Purcell L, Schneider KJ, et al. Clinical recovery from concussion-return to school and sport: a systematic review and meta-analysis. Br J Sports Med, 2023.PMID 37316183
- [5]Schneider KJ, Critchley ML, Anderson V, et al. Targeted interventions and their effect on recovery in children, adolescents and adults who have sustained a sport-related concussion: a systematic review. Br J Sports Med, 2023.PMID 37316188
- [6]Davis GA, Schneider KJ, Anderson V, et al. Pediatric Sport-Related Concussion: Recommendations From the Amsterdam Consensus Statement 2023. Pediatrics, 2024.PMID 38044802
- [7]Halstead ME, Walter KD, Moffatt K, et al. Sport-Related Concussion in Children and Adolescents. Pediatrics, 2018.PMID 30420472
- [8]Lumba-Brown A, Yeates KO, Sarmiento K, et al. Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children. JAMA Pediatr, 2018.PMID 30193284
- [9]Lumba-Brown A, Yeates KO, Sarmiento K, et al. Diagnosis and Management of Mild Traumatic Brain Injury in Children: A Systematic Review. JAMA Pediatr, 2018.PMID 30193325
- [10]Davis GA, Anderson V, Babl FE, et al. What is the difference in concussion management in children as compared with adults? A systematic review. Br J Sports Med, 2017.PMID 28455361
- [11]Chizuk HM, Willer BS, Cunningham A, et al. Adolescents with Sport-Related Concussion Who Adhere to Aerobic Exercise Prescriptions Recover Faster. Med Sci Sports Exerc, 2022.PMID 35482774
- [12]McCrory P. Does second impact syndrome exist? Clin J Sport Med, 2001.PMID 11495318