Paeds · rheumatology-musculoskeletal-and-sports
Scoliosis and spinal deformity
Also known as adolescent idiopathic scoliosis · AIS · Cobb angle · Risser sign · Sanders maturity · Lenke classification · early-onset scoliosis · congenital scoliosis · neuromuscular scoliosis · Adams forward bend test · scoliometer · BrAIST trial
A fellowship approach to scoliosis and spinal deformity in children and adolescents: scoliosis is a lateral spinal curvature of 10 degrees Cobb or more with vertebral rotation, the adolescent idiopathic curve is common and painless, and the clinical skill is to separate the idiopathic curve managed by the observe-brace-surgery ladder (under 25, 25 to 40, 45 to 50 degrees or more) from the non-idiopathic curve that hides a congenital anomaly, a neural-axis lesion, or a syndrome behind the red flags of age under 10, a left thoracic curve, pain, a neurological deficit, and rapid progression.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A twelve-year-old girl is sent by her school nurse because her right shoulder sits higher than her left and a rib hump appears when she bends forward — the classic painless right thoracic adolescent idiopathic curve, found on screening and managed by the curve magnitude and the remaining growth. A four-year-old boy has a visible spinal curve and a left thoracic prominence with an asymmetric abdominal reflex — a non-idiopathic curve until the magnetic resonance imaging excludes a syrinx. A six-month-old with a hemivertebra on the spine film has a congenital scoliosis that is destined to progress and that carries a renal anomaly until the ultrasound proves otherwise. The task in each is to measure the Cobb angle, stage the maturity, run the red-flag screen, and place the child on the right rung of the management ladder. [2] [12]
The five moves — Screen, Measure, Stage, Decide, Refer
Overview & Definition
Scoliosis is a structural lateral curvature of the spine, and the paediatric clinician holds two ideas at once: most scoliosis in adolescence is idiopathic, common, and painless, and yet every curve is treated as non-idiopathic until the red-flag screen proves otherwise. The formal definition is a lateral curvature measured on a standing radiograph of 10 degrees Cobb or more, with a rotational component — a spinal curvature under 10 degrees is spinal asymmetry, not scoliosis, and it is observed rather than treated. The 10-degree threshold matters because it is the magnitude at which the curve becomes a structural deformity with a measurable rotation, and it is the cut-off that frames every prevalence and progression figure in the literature. [2] [8]
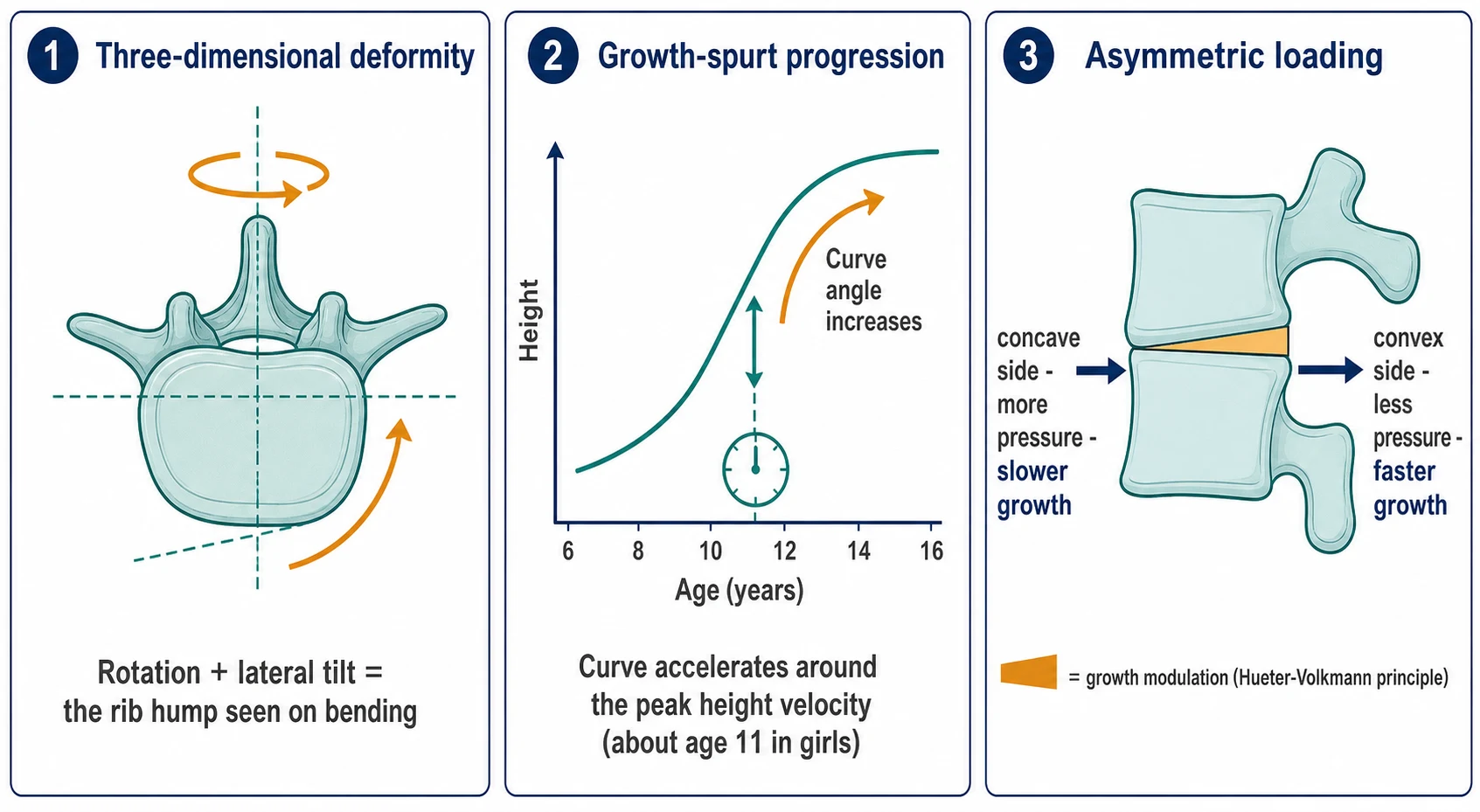
The rotational component is what makes scoliosis a three-dimensional deformity rather than a simple side-bend, and it is the rotation that produces the rib hump the examiner sees on the forward bend. The vertebrae rotate toward the convexity of the curve, the ribs on the convex side bulge posteriorly into a prominence, and the chest wall asymmetry is the visible sign that brings most adolescents to attention. A curve is therefore never fully described by the Cobb angle alone, and the forward-bend examination is as much a part of the assessment as the radiograph. [8] [2]
The clinical weight of scoliosis comes from what an untreated severe curve does to a child over a lifetime, and from what an unnecessary early fusion does to a developing lung. A large thoracic curve restricts the chest and, in the severe curve, the vital capacity. A curve fused in early childhood before the lungs and the thorax have grown leaves the child with a small chest and a restricted lung that no later operation can fully restore. The fellowship task is to identify the curve, measure and stage it, separate the idiopathic from the non-idiopathic, and place the child on the management rung that preserves growth and lung while preventing the deformity from progressing. [3] [7]
Classification
Scoliosis is classified along two axes that together drive the workup and the urgency. The first axis is etiology, and it is the axis that decides whether the curve is managed as a straightforward idiopathic problem or investigated as the sign of a serious underlying condition. The second axis is the curve magnitude and the skeletal maturity, and it is the axis that decides the rung of the management ladder. The fellowship candidate names both axes aloud before naming the plan, because a 35-degree curve in a Risser 5 mature adolescent is watched, while the same 35-degree curve in a Risser 0 pre-menarchal girl is braced. [2] [5]
The etiology axis runs from the idiopathic through the congenital, the neuromuscular, and the syndromic. The idiopathic curve — the commonest, by far — is a diagnosis of exclusion, defined by the absence of an identifiable cause and divided by the age at onset into infantile (onset under 3 years), juvenile (3 to 9 years), and adolescent (10 years and over), with the adolescent the overwhelming majority. The congenital curve is born of a vertebral anomaly — a failure of formation such as a hemivertebra, or a failure of segmentation such as a unilateral bar — and it carries a high rate of associated neural-axis, renal, and cardiac anomalies. The neuromuscular curve accompanies cerebral palsy, spinal muscular atrophy, the myopathies, and the spinal cord lesions, and it tends to a long collapsing C-shape that worsens with the weakness. The syndromic curve is the scoliosis of Marfan, Ehlers-Danlos, neurofibromatosis, and the connective-tissue and skeletal dysplasia disorders. [2] [11]
The Lenke classification is the operative framework for the adolescent idiopathic curve and the one an examiner expects the candidate to name. It assigns each curve a type from 1 to 6 based on which curves are structural (the main thoracic, the double thoracic, the double major, the triple major, the thoracolumbar or lumbar, and the thoracic main with a structural thoracolumbar curve), a lumbar modifier of A, B, or C based on where the centre sacral vertical line falls relative to the lumbar apical vertebra, and a sagittal modifier of minus, N, or plus based on the thoracic kyphosis. The Lenke type drives the surgical plan — which levels to fuse — and it is the language the spinal team speaks. For the early-onset curve, the Williams Classification of Early-Onset Scoliosis (C-EOS) frames the curve by the etiology, the major curve angle, the kyphosis, and the progression, and it guides the growth-friendly strategy. [4] [11]
Epidemiology & Risk Factors
Scoliosis becomes measurably common in early adolescence, and the prevalence rises with the curve magnitude and concentrates in the female sex. Roughly two to three per cent of adolescents carry a curve of 10 degrees Cobb or more, but only a small fraction — perhaps two to three per thousand — reach the 40-degree threshold at which surgery is considered, and the female-to-male ratio widens sharply as the curve magnitude grows, so that the severe curve is roughly seven times more common in girls than in boys. A family history raises the risk of a clinically significant curve, and the genetic contribution to the idiopathic curve is well established even though no single gene explains it. [2] [8]
The single most powerful epidemiological risk factor for progression is the combination of a larger curve magnitude with a lower skeletal maturity at presentation — and this is the Lonstein and Carlson insight. A curve of 20 to 29 degrees in a Risser 0 or 1 child (substantial growth remaining) has a high probability of progression, while the same curve in a Risser 4 or 5 child (mature) is essentially stable. The danger window is the period around the peak height velocity, the steep acceleration of spinal growth that occurs around 11 years in girls and 13 in boys, when a curve that has been quiescent can advance several degrees in a few months. The Sanders maturity scale, built from a hand radiograph, refines the prediction further by staging the growth to the peak and the slowing. [5] [6]
The serious and the secondary causes are individually less common but collectively demand the vigilance this topic teaches. The left thoracic curve is the classic red flag, because the idiopathic thoracic curve is overwhelmingly right-sided, and a left thoracic curve carries a meaningfully higher rate of an underlying neural-axis lesion. The painful curve is another, because the idiopathic curve is painless, and pain points to an osteoid osteoma, an infection, a tumour, a spondylolysis, or a cord lesion. The neuromuscular and the syndromic conditions carry a far higher prevalence and a faster progression of scoliosis than the idiopathic curve — in severe cerebral palsy the majority of children develop a clinically significant curve — and the early-onset curve, by definition, threatens the developing lung. [2] [7]
Pathophysiology
Scoliosis is best understood as a three-dimensional deformity in which a lateral curvature and a vertebral rotation reinforce one another, and the pathophysiology explains both the rib hump the examiner sees and the acceleration of the curve through the growth spurt. The vertebrae rotate toward the convexity of the curve, the posterior elements and the ribs on the convex side are thrust backward into the prominence, and the rotational asymmetry is what the Adams forward bend test makes visible. A curve that looks small and benign on the posteroanterior film may carry a substantial rotation, and the forward-bend rib hump is the clinical sign that reveals it. [8] [2]
The growth-spurt acceleration is the heart of the natural history, and the mechanism is the asymmetric loading of a growing vertebra. Once a curve exists, the vertebral bodies on the concave side of the curve carry more compressive load and the bodies on the convex side carry less, and the Hueter-Volkmann principle holds that increased compression slows growth while reduced compression accelerates it. The concave side grows more slowly, the convex side grows faster, the vertebral bodies wedge toward the concavity, and the curve deepens — a self-reinforcing vicious circle that runs fastest when the spine is growing fastest, which is precisely the peak height velocity. This is why a curve that was stable through childhood can advance rapidly across the adolescent growth spurt, and why the maturity staging is as important to the prognosis as the curve magnitude. [8] [6]
The thoracic and the pulmonary consequences follow from the anatomy and the age. A large thoracic curve distorts the ribs and the chest wall and, in the severe curve, restricts the lung and reduces the vital capacity, and the restriction is most pronounced when the deformity begins early and the lung is still developing. This is the central problem of the early-onset curve and the reason for the growth-friendly strategy: a fusion that locks the thoracic spine in a young child prevents the thorax and the lungs from growing, and the resulting small chest and restricted lung — the thoracic insufficiency syndrome — is a far greater burden than the curve itself. The adolescent curve, by contrast, largely spares the lung because the thorax is nearly grown, and the pulmonary concern is reserved for the very large thoracic curve. [7] [11]
The congenital curve has its own pathophysiology, born of a malformation of the vertebral body in early embryonic life. A failure of formation leaves a wedge-shaped or a fully hemi vertebra that grows on one side only and pushes the spine into a progressive curve, while a failure of segmentation leaves a bony bar that tethers one side of the spine and forces the other side to grow around it. Both anomalies are rigid, both tend to progress as the child grows, and the congenital curve carries a high rate of an associated neural-axis anomaly, a renal anomaly, and a cardiac anomaly, which is why the workup at diagnosis includes the magnetic resonance imaging and the screening ultrasound and echocardiogram. [12] [11]
Clinical Presentation
The adolescent with the idiopathic curve presents asymptomatically, and the first sign is usually a visible asymmetry rather than a complaint. The shoulder on the convex side sits higher, the scapula protrudes, the waist crease is asymmetric, and the pelvis may tilt. A rib hump appears only when the child bends forward. The presentation is often the school screening referral, the worried parent who notices the shoulder tilt, or the incidental finding at a routine examination. The painless character is central — the idiopathic curve does not hurt, and any pain reopens the search for a non-idiopathic cause. [2] [8]
The younger child with the early-onset curve presents differently, and the age band is itself the red flag. The infantile curve, onset under 3 years, is uncommon and often resolves spontaneously, but the juvenile curve, onset from 3 to 9 years, is the one that worries the clinician, because it sits in the window of the developing thorax and the lung and because it carries a higher rate of an underlying neural-axis lesion. The early-onset curve is non-idiopathic by default until the red-flag screen and the imaging prove otherwise, and the magnetic resonance imaging is obtained more liberally than in the adolescent. [2] [11]
The presentations that must never close the search for a serious cause are the very reason the red-flag screen exists. The painful scoliosis — a child with back pain and a curve — is a different animal from the painless idiopathic curve, and the differential includes the osteoid osteoma, the discitis, the osteomyelitis, the tumour, and the spondylolysis, each of which demands its own imaging. The left thoracic curve raises the concern for a syringomyelia or a Chiari malformation, and the neurological deficit — however subtle — signals a cord lesion. The rapid progression, the curve that advances through a brace, and the skin stigmata over the spine each redirect the workup from the idiopathic ladder to the investigation of the underlying cause. [2] [3]
The neuromuscular child presents with a long, collapsing, often C-shaped curve that affects the sitting balance and, in the severe case, the breathing and the ease of care. The child with severe cerebral palsy develops a pelvic obliquity and a windswept posture that makes sitting painful and feeding difficult, and the curve progresses with the growth and the weakness. The syndromic child — Marfan, neurofibromatosis, the connective-tissue disorders — carries a curve that is often early, rapidly progressive, and atypical in pattern, and the associated cardiac and ocular disease shapes the perioperative risk. [2] [11]
Differential Diagnosis
The idiopathic curve is distinguished from the others by the absence of a cause, and the distinction is made by the history, the examination, and the selective imaging. The first fork is structural versus non-structural: a non-structural or postural curve corrects when the underlying cause is removed — when a leg-length inequality is levelled, when a muscle spasm settles, or when an acute pain resolves — while a structural curve persists and carries the rotation. The idiopathic curve is the commonest structural curve, and it is named only after the others are excluded. [8] [2]
The congenital curve is distinguished on the radiograph by the vertebral anomaly — the hemivertebra, the wedge vertebra, the unilateral bar — and the distinction matters because the congenital curve is rigid, progressive, and associated with the neural-axis and the visceral anomalies. A magnetic resonance imaging of the spine is obtained at diagnosis to define the cord and the neural elements, a renal ultrasound to screen for the urologic anomaly that accompanies roughly a fifth of congenital spinal anomalies, and an echocardiogram for the associated cardiac defect. The McMaster classification frames the prognosis by the anomaly type, and the unilateral failure of segmentation carries the worst progression. [12] [11]
The neuromuscular and the syndromic causes are identified by the associated condition. The cerebral palsy, the spinal muscular atrophy, the myelomeningocele, and the myopathies each carry their characteristic collapsing curve, and the muscular dystrophies carry a curve that progresses rapidly once the child loses ambulation. The syndromes — Marfan, Ehlers-Danlos, neurofibromatosis, the skeletal dysplasias — present with early, atypical, and rapidly progressive curves, and the workup includes the cardiac and the ocular assessment that the syndrome demands. The Scheuermann kyphosis is the differential of the sagittal plane — a rigid structural round back rather than a lateral curve — and it is distinguished by the wedging on the lateral radiograph. [2] [8]
The painful scoliosis carries its own differential, and it is the differential that demands the urgent imaging. The osteoid osteoma is the classic cause of a painful curve in the older child, with night pain relieved by non-steroidal anti-inflammatory drugs. The discitis and the osteomyelitis present with fever and raised inflammatory markers in the younger child. The osteoid osteoma, the osteoblastoma, the eosinophilic granuloma, and the malignant tumour are the bony causes, and the spondylolysis presents with the extension-related low back pain of the young athlete. The neural-axis lesion — the syringomyelia, the Chiari, the tethered cord, the spinal cord tumour — produces the painful or the neurologically abnormal curve, and it is the lesion that the magnetic resonance imaging is designed to find. [2] [3]
Clinical & Bedside Assessment
The recognition move is the Adams forward bend test, performed on every child with a suspected curve and at every screening opportunity. The child stands and bends forward at the waist with the arms hanging and the knees straight, and the examiner inspects the back from behind at the level of the trunk. A scoliotic curve produces an asymmetric rib prominence — the rib hump on the convex side — because the vertebral rotation thrusts the ribs and the posterior elements backward. The scoliometer is placed on the most prominent part of the hump, perpendicular to the trunk, and the angle of trunk rotation is read. A trunk-rotation angle of 7 degrees or more is the conventional trigger for the standing radiograph, because it correlates with a curve of roughly 20 degrees Cobb and it captures the curves worth investigating while sparing the minor asymmetries. [2] [10]
The standing inspection is the first half of the assessment, and it is performed with the pelvis levelled — a leg-length inequality must be corrected with a block under the short leg before the curve is read, because a tilted pelvis produces a compensatory non-structural curve that disappears when the pelvis is level. The examiner looks for the shoulder symmetry, the scapular prominence, the waist-crease asymmetry, the trunk shift, and the pelvic tilt, and notes the direction of any curve. The forward bend completes the assessment, and the scoliometer quantifies the rotation. A thorough assessment also palpates the spine for a focal tenderness, inspects the skin over the spine for a dimple, a hair tuft, or a sinus, and examines the lower limbs for a leg-length difference. [2] [8]
The neurological examination is mandatory and often skipped, and its omission is the classic error. Every child with a curve is examined for the lower-limb tone, power, reflexes, and sensation, and for the gait, because a subtle deficit is the sign of the underlying cord lesion. The abdominal reflexes are tested, and an asymmetric abdominal reflex — present on one side and absent on the other — is a recognised sign of a syringomyelia and the trigger for the magnetic resonance imaging. The straight-leg raise and the focal spinal tenderness are assessed when the curve is painful. The fellowship candidate who performs and documents the neurological examination of every scoliosis earns the mark the complacent candidate loses. [2] [3]
The findings that must never be dismissed are the red flags, and they are the gate to the magnetic resonance imaging. The left thoracic curve, the painful curve, the early-onset curve, the rapidly progressive curve, the neurological deficit, the asymmetric abdominal reflex, and the skin stigmata over the spine each demand the imaging and the search for the underlying cause. The examination is also the moment to screen the systems that the syndromic curve implicates — the cardiac murmur of Marfan, the cafe-au-lait patches of neurofibromatosis, the joint hypermobility of the connective-tissue disorders — and to assess the developmental and the psychosocial context that will shape the management and the consent. [2] [8]
Investigations
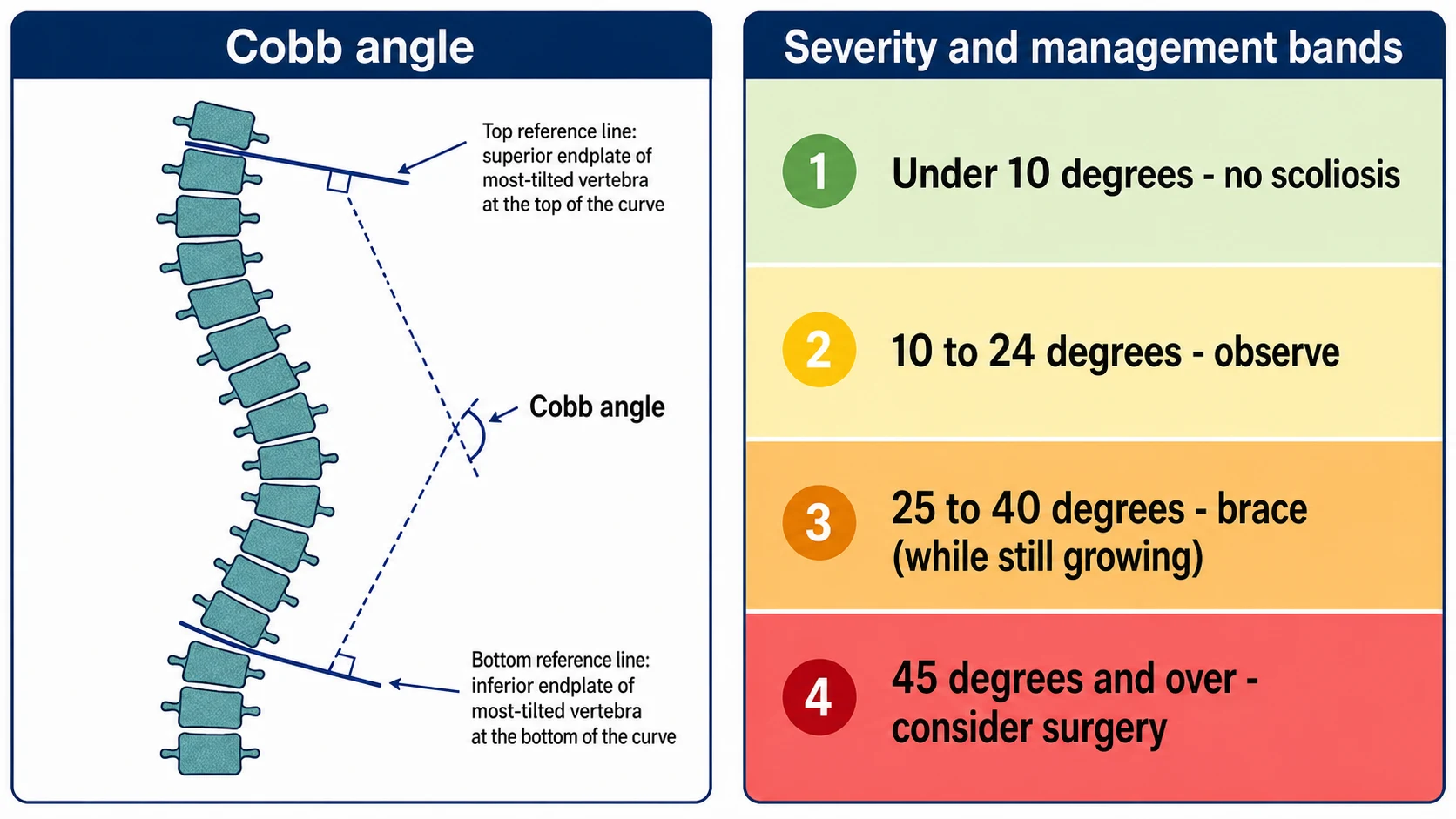
The standing posteroanterior radiograph of the spine is the central investigation, and the Cobb angle is the measurement that flows from it. The Cobb angle is measured by drawing a line along the superior endplate of the most-tilted vertebra at the top of the curve and a line along the inferior endplate of the most-tilted vertebra at the bottom of the curve, and the angle between the perpendiculars to these two lines is the Cobb angle. The most-tilted vertebrae — the end vertebrae — are identified as those whose endplates are most tilted toward the curve concavity, and the angle is read to the nearest degree. The posteroanterior projection is used rather than the anteroposterior to reduce the radiation dose to the breast, and a single well-centred standing film, including the cervical spine to the pelvis, is the study that frames the curve. [2] [8]
The maturity is staged from the same film and from a hand radiograph when needed. The Risser sign grades the ossification of the iliac apophysis from 0 (no ossification, substantial growth remaining) through 1 to 4 (progressive ossification) to 5 (full fusion, skeletal maturity), and it is read directly from the posteroanterior spine film. The Sanders maturity scale, built from a left-hand radiograph, stages the skeletal maturity from 1 to 9 and refines the prediction of the peak height velocity and the remaining growth, and it is the staging that the modern spinal service uses to time the bracing and the surgery. The two maturities are reported together with the Cobb angle, because the management is built on the magnitude and the remaining growth in combination. [5] [6]
The magnetic resonance imaging of the neural axis is the investigation that separates the idiopathic from the non-idiopathic curve, and it is obtained for the atypical and the high-risk presentation. The indications are the left thoracic curve, the early-onset curve (especially the juvenile curve under 10), the painful curve, the rapid progression, any neurological deficit or the asymmetric abdominal reflex, the congenital scoliosis, and routinely before the surgical instrumentation of an atypical curve. The imaging excludes the syringomyelia, the Chiari malformation, the tethered cord, the diastematomyelia, and the spinal cord tumour, and the finding redirects the management from the brace to the neurosurgical and the spinal intervention. [2] [3]
The serial radiograph is the investigation of observation, and the reproducibility of the measurement defines the progression. A child on observation has a standing posteroanterior film repeated at 4 to 6 month intervals through the growth, and a curve is judged to have progressed when it advances by 5 degrees or more on a reproducible film — a smaller change is within the measurement error and does not, by itself, justify a change in management. The bone scan, the computed tomography, and the low-dose biplanar (EOS) imaging are reserved for the specific question — the painful curve, the pre-operative planning, the radiation minimisation in the serial follow-up — and the renal ultrasound and the echocardiogram complete the workup of the congenital curve. [9] [11]
Management — Resuscitation
Scoliosis is, for the most part, an elective and an outpatient problem, and the management ladder is applied in the clinic rather than the emergency department. The resuscitation framing matters for the small number of curves that present as a clinical emergency, and the fellowship candidate names the emergency presentations aloud because they redirect the whole pathway. The rapidly progressive early-onset curve that threatens the thorax and the lung, the neurological deficit that signals a cord compromise, and the congenital curve with an associated neural-axis or a visceral anomaly are the presentations that demand an urgent imaging and a referral rather than a routine clinic visit. [2] [11]
The painful scoliosis with a neurological deficit is the clearest emergency, and the pathway is the urgent magnetic resonance imaging followed by the neurosurgical and the spinal referral. A syringomyelia that has produced a deficit, a spinal cord tumour that is progressing, and a congenital anomaly with a cord tethering are the lesions that the imaging finds and that the neurosurgical team addresses, and the bracing and the elective fusion wait until the cord is secured. The syndrome that compromises the cardiac or the respiratory function — the severe Marfan with the aortic root dilation, the muscular dystrophy with the cardiomyopathy and the failing respiratory muscles — is the medical emergency that precedes the spinal management. [2] [3]
The congenital curve is screened for the associated anomalies at diagnosis, and the screening is part of the early management. The renal ultrasound is obtained for the urologic anomaly that accompanies roughly a fifth of congenital spinal anomalies, the echocardiogram for the associated cardiac defect, and the magnetic resonance imaging for the neural-axis anomaly, because the congenital curve is a multisystem finding and the spinal team is not the only team involved. The neuromuscular curve that compromises the sitting balance and the breathing is referred for the growth-friendly assessment before the thoracic insufficiency is established, and the early-onset curve that is progressing is referred before the curve becomes rigid and the lung is fixed. [12] [7]
The rapidly progressive early-onset curve is the presentation that the growth-friendly strategy is designed to rescue, and the timing of the referral is the intervention. A young child whose curve is advancing toward the severe range is referred for the growth-friendly implants — the traditional growing rods, the magnetically controlled growing rods, the vertebral body tether, or the vertical expandable prosthetic titanium rib (VEPTR) — that expand the chest and the spine through the growth and delay the definitive fusion until the thorax and the lung are mature. The resuscitation of the early-onset curve is the prevention of the thoracic insufficiency syndrome, and the window is the growth. [7] [11]
Management — Definitive & Stepwise
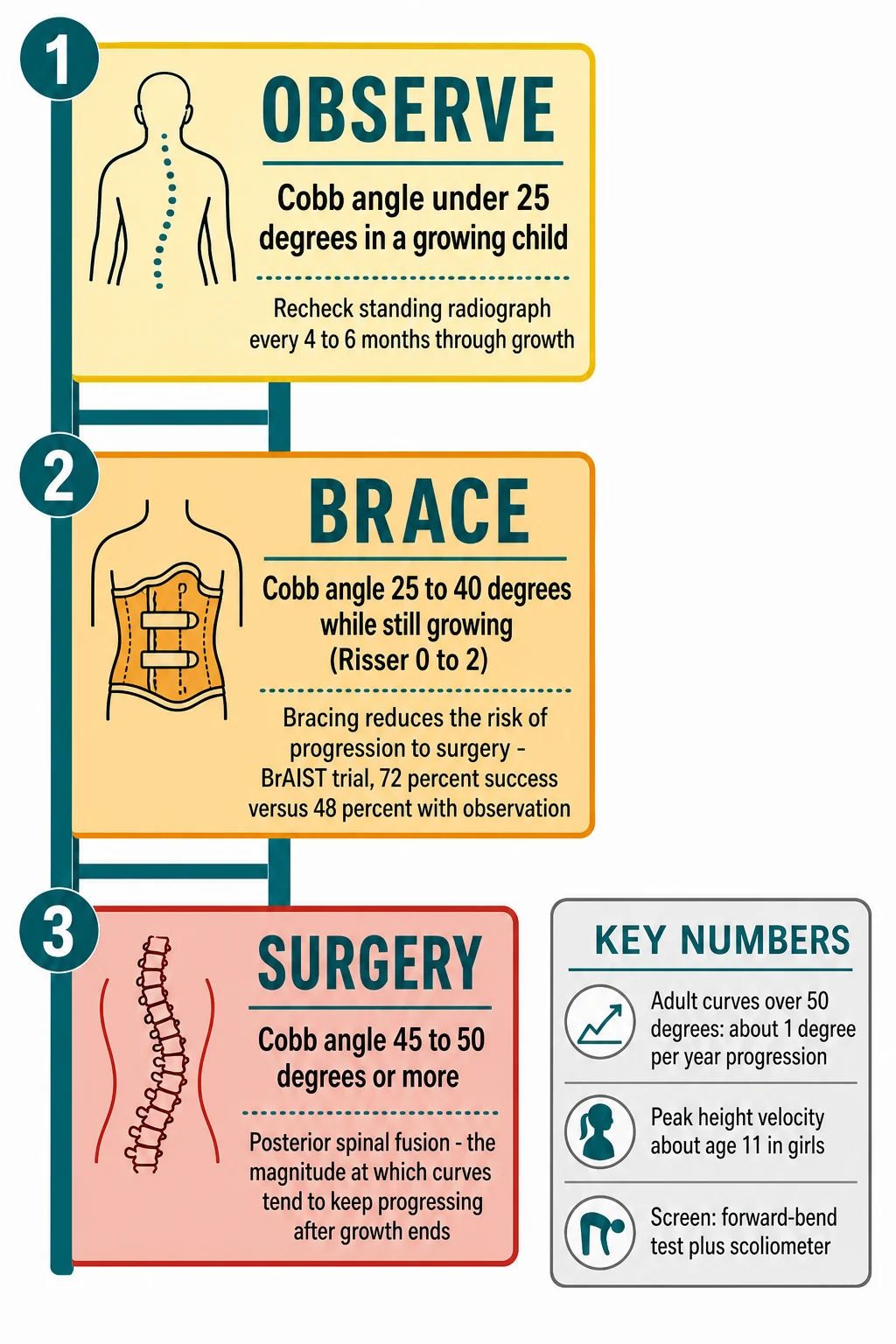
The definitive management of the idiopathic curve is the ladder of observe, brace, and consider surgery, and each rung is set by the two numbers — the curve magnitude and the skeletal maturity. A curve under 25 degrees in a growing child is observed, with a standing radiograph repeated at 4 to 6 months through the growth. A curve of 25 to 40 degrees in a skeletally immature child (Risser 0 to 2, or substantial growth remaining) is braced, and a curve of 45 to 50 degrees or more is considered for the surgical fusion, because it is the magnitude at which the curve tends to keep progressing after the growth ends. The maturity modifies each rung — a 30-degree curve in a mature adolescent is watched, while the same curve in a pre-menarchal Risser 0 girl is braced — and the two numbers are always reported together. [1] [2]
Observation is the management of the small curve, and it is an active rather than a passive strategy. The child returns at 4 to 6 month intervals through the growth, the standing radiograph is repeated, and the curve is tracked for the 5-degree change that defines the progression. A curve that progresses from the observe range into the brace range is braced. A curve that holds steady through the growth is discharged at maturity with the reassurance and the safety-net. The observation is paired with the counselling of the family — the natural history, the importance of the follow-up, and the signs that warrant an earlier return — and the documentation of the safety-net is part of the management. [9] [8]
Bracing is the management of the moderate curve in the growing child, and the BrAIST trial is the evidence that established its efficacy. The Bracing in Adolescent Idiopathic Scoliosis Trial randomised skeletally immature children with a 25 to 40 degree curve to bracing or to observation, and it was stopped early for efficacy: bracing raised the rate of successful treatment — defined as the curve not reaching 50 degrees — to 72 percent, against 48 percent with observation, with a number needed to treat of 3. The benefit was greatest in the higher-risk curves and the compliant wearers, and the trial settled a long-standing controversy over whether bracing altered the natural history. The orthosis is worn full-time (18 to 23 hours a day) for the thoracic and the thoracolumbar curves, with the part-time brace an option for the selected curve, and the wear continues until the skeletal maturity. [1] [9]
The surgery is the posterior spinal fusion with the segmental instrumentation, and it is offered for the curve of 45 to 50 degrees or more, because it is the magnitude at which the curve tends to keep progressing after the growth ends — the natural history of the untreated 50-degree curve is a roughly 1-degree-per-year progression into adult life. The fusion straightens the curve with the rods and the screws, decorticates the posterior elements, and locks the vertebrae of the curve into a solid bony fusion. The levels are chosen by the Lenke classification, and the selective fusion spares the mobile lumbar segments when the lumbar curve is non-structural. The alternatives for the young and the selective curve are the growing rod and the vertebral body tether, which are designed to correct the curve while preserving the growth and the motion. [1] [4]
The physiotherapeutic scoliosis-specific exercises are an adjunct to the observation and the bracing, and they sit within the SOSORT guidelines as a part of the conservative management. The exercises — the auto-correction, the asymmetrical stabilisation, and the curve-pattern-specific training — are performed under the supervision of a trained physiotherapist, and the evidence supports their role as an adjunct that may improve the brace compliance and the muscular support, although they are not a standalone substitute for the bracing of a progressive curve. The fellowship answer names the exercises as part of the conservative package and refers the child to the physiotherapist as part of the multidisciplinary team. [9] [8]
Specific Subtypes & Scenarios
The adolescent idiopathic curve is the commonest subtype, and its management is the ladder applied to the magnitude and the maturity. The natural history of the untreated curve is the long arc of the Weinstein fifty-year study: the curve that reaches 50 degrees at skeletal maturity tends to progress at roughly 1 degree per year through adult life, the larger thoracic curve may restrict the vital capacity, and the visible deformity carries the cosmetic and the psychosocial burden, although the untreated curve is not, in the long run, the cause of the severe back pain or the early mortality that was once feared. The management aims to prevent the progression and the deformity, and the bracing and the selective fusion are the tools. [3] [2]
The early-onset scoliosis, onset before 10 years, is the subtype that threatens the lung, and its management is the growth-friendly strategy rather than the early fusion. The goal is to allow the thorax and the lung to grow while controlling the curve, because a fusion in the young child locks the thorax and produces the thoracic insufficiency syndrome — the small chest, the restrictive lung, and the respiratory failure that no later operation fully reverses. The growth-friendly implants are the traditional growing rods, lengthened at planned operations. The magnetically controlled growing rods, lengthened non-invasively in the clinic. The vertebral body tether, a compressive implant on the convex side that modulates the growth and corrects the curve, and the vertical expandable prosthetic titanium rib (VEPTR), which expands the thorax for the chest-wall and the rib-anomaly curve. The definitive fusion is delayed until the thorax and the lung are mature. [7] [11]
The congenital scoliosis is managed by the anomaly type and the progression, and the management is often surgical and early. The hemivertebra, the wedge vertebra, and the unilateral bar are rigid and progressive, and the curve that is destined to progress is better addressed before the deformity becomes severe and rigid — the prophylactic hemivertebra excision or the in-situ fusion of the unilateral bar is offered to the young child to prevent the large structural curve. The associated anomalies are screened and managed in parallel — the neural-axis lesion by the neurosurgery, the renal anomaly by the urology, the cardiac defect by the cardiology — and the spinal team coordinates the long surveillance. The McMaster classification frames the prognosis, and the unilateral failure of segmentation carries the worst outlook for progression. [12] [11]
The neuromuscular scoliosis is managed to preserve the sitting balance, the pulmonary function, and the ease of care, and the timing and the extent of the fusion differ from the idiopathic curve. The child with severe cerebral palsy develops a pelvic obliquity and a long C-shaped curve that makes sitting painful and care difficult, and the fusion to the pelvis is offered when the curve compromises the function rather than at a fixed magnitude threshold. The muscular dystrophies carry a curve that progresses rapidly once the ambulation is lost, and the timing of the fusion is set by the declining pulmonary function, because the surgery must be performed while the vital capacity is still adequate for the anaesthetic. The syndromic scoliosis — Marfan, neurofibromatosis, the connective-tissue disorders — is managed with the attention to the cardiac and the ocular associations that raise the perioperative risk. [2] [8]
Complications & Pitfalls
The complications of the untreated severe curve are the reason the management exists. A large thoracic curve restricts the chest and, in the severe case, the vital capacity. A curve that reaches 50 degrees at maturity tends to progress at roughly 1 degree per year into adult life, and the visible deformity carries the cosmetic and the psychosocial burden, with the effect on the body image, the self-esteem, and the social participation of the adolescent. The pulmonary restriction is the chief medical concern of the very large thoracic curve and the early-onset curve, and the prevention of the progression and the deformity is the aim. [3] [7]
The complications of the early thoracic fusion are the reason the growth-friendly strategy exists, and the Karol study is the evidence that frames them. A fusion of the thoracic spine in a young child prevents the thorax and the lung from growing, and the children fused early in life are left with a smaller chest and a reduced vital capacity, with the impairment greatest in those fused youngest and over the longest span. The thoracic insufficiency syndrome — the inability of the thorax to support the normal respiration and the lung growth — is the syndrome that the growth-friendly implants are designed to prevent, and the avoidance of the early definitive fusion in favour of the lengthening strategy is the principle that the modern service applies. [7] [11]
The surgical complications of the posterior spinal fusion are the risks that the consent addresses. The neurological injury is the feared complication, and the spinal cord monitoring and the wake-up test are the safeguards. The infection, the implant failure, the pseudarthrosis, and the crankshaft phenomenon (the continued anterior growth of the spine behind a posterior fusion in the very immature child, which distorts the result) are the recognised complications. The pulmonary and the transfusion risks of the major surgery are quantified, and the anaesthetic and the intensive-care support are part of the perioperative pathway. The fellowship candidate names the complications and the safeguards when the consent is examined. [2] [4]
The pitfalls are the errors that the red-flag screen and the disciplined follow-up prevent. The reassuring normal radiograph in the early curve is a trap, because the small curve is real and progressive, and the serial standing film safeguards the diagnosis. The missed non-idiopathic cause — the syringomyelia braced as idiopathic, the congenital anomaly overlooked, the tumour dismissed — is the error that the magnetic resonance imaging and the red-flag screen catch. The over-called idiopathic curve, braced unnecessarily, is the lesser harm, but the disciplined screen and the shared decision safeguard against it. The non-compliance with the brace is the pitfall that the counselling and the follow-up address, because a brace worn inadequately does not work. [1] [2]
Prognosis & Disposition
The natural history of the untreated curve is the long arc of the Weinstein fifty-year follow-up, and it is the evidence that frames the prognosis. The curve that reaches 50 degrees at skeletal maturity tends to progress at roughly 1 degree per year through adult life, the larger thoracic curve may restrict the vital capacity, and the visible deformity carries the cosmetic and the psychosocial burden — but the untreated curve is not, in the long run, the cause of the severe back pain, the cardiopulmonary disease, or the early mortality that was once feared, and the modern management aims to prevent the progression and the deformity rather than to avert a catastrophic outcome. [3] [2]
The prognosis of the braced curve depends on the curve magnitude, the skeletal maturity, and the brace compliance, and the BrAIST trial frames the success rate. Bracing raised the rate of successful treatment — the curve not reaching 50 degrees — to 72 percent against 48 percent with observation, with the number needed to treat of 3, and the benefit was greatest in the higher-risk curves and the compliant wearers. The brace that is worn for the prescribed hours, through the remaining growth, and with the regular follow-up, gives the child the best chance of avoiding the surgery, and the non-compliance is the chief threat to the outcome. The prognosis of the surgical fusion is generally excellent, with a well-corrected and a solidly fused curve, and the return to the activity in the months that follow. [1] [9]
The prognosis of the early-onset curve is tied to the thoracic and the lung development, and the prevention of the thoracic insufficiency syndrome is the central goal. The growth-friendly strategy preserves the growth and the lung function, and the definitive fusion is delayed until the maturity. The child managed well through the early years reaches the adolescence with a larger chest and a better lung than the child fused early. The prognosis of the congenital curve depends on the anomaly type and the progression, with the unilateral failure of segmentation carrying the worst outlook. The prognosis of the neuromuscular curve is intertwined with the underlying condition, and the management aims to preserve the comfort, the sitting, and the pulmonary function. [7] [12]
The disposition is shared across the multidisciplinary team, and the general paediatrician is the coordinator. The orthopaedic spinal surgeon leads the bracing, the surgery, and the growth-friendly strategy. The physiotherapist delivers the scoliosis-specific exercises and the post-operative rehabilitation. The orthotist fits and adjusts the brace and monitors the compliance. The respiratory physician and the intensivist support the perioperative and the neuromuscular curve, and the cardiology and the renal teams manage the associated anomalies of the congenital and the syndromic curve. The family is counselled on the diagnosis, the natural history, the treatment options, the safety-net, and the importance of the follow-up, and the psychosocial support — the body image, the school, the peer network — is part of the management of the adolescent. [2] [8]
Special Populations
The child with the neuromuscular disorder — the cerebral palsy, the spinal muscular atrophy, the muscular dystrophy, the myelomeningocele — carries a scoliosis that is more prevalent, more rapidly progressive, and more functionally consequential than the idiopathic curve. The management balances the sitting balance, the comfort, the ease of care, and the pulmonary function against the surgical risk, and the decision to fuse to the pelvis is made when the curve compromises the function rather than at a fixed magnitude threshold. The perioperative pathway addresses the nutrition, the anticonvulsants, the respiratory support, and the pain, and the family-centred decision weighs the quality of life alongside the radiograph. [2] [8]
The child with the syndrome — Marfan, neurofibromatosis, the Ehlers-Danlos, the skeletal dysplasias — carries a curve that is often early, atypical, and rapidly progressive, and the associated cardiac, ocular, and vascular disease shape the workup and the perioperative risk. The Marfan syndrome demands the echocardiogram for the aortic root, the neurofibromatosis the assessment for the plexiform neurofibroma and the hypertension, and the connective-tissue disorders the vascular and the wound considerations. The scoliosis is one part of a multisystem condition, and the management is coordinated with the cardiology, the ophthalmology, and the genetics teams. [2] [3]
The adolescent with the developmental disability or the neurodiversity experiences the brace and the surgery through the lens of the capacity and the sensory profile, and the assessment and the consent adapt. The explanation is tailored to the developmental level, the brace is introduced gradually with the desensitisation, the carers are engaged in the wear and the care, and the capacity for the consent is assessed and documented. The shared decision includes the family and the carers, and the best-interest framework is applied when the capacity is limited. The psychosocial impact of the visible deformity and the brace weighs on every adolescent, and the mental-health support and the peer network are part of the management. [9] [8]
The Indigenous, the remote, and the socioeconomically disadvantaged children present later with larger curves, because the access to the screening, the imaging, and the follow-up is shaped by the distance, the cost, and the service availability. The telehealth and the outreach clinics, the coordination of the travel and the accommodation, and the cultural safety of the service are part of the access, and the fellowship answer names the equity of the access as a determinant of the outcome. The migrant and the refugee child raises the consideration of the late presentation and the unfamiliarity with the service, and the interpreter and the cultural support are part of the assessment. [2] [8]
Evidence, Guidelines & Regional Differences
The BrAIST trial is the landmark that established the efficacy of the bracing, and the fellowship candidate knows its result. The Bracing in Adolescent Idiopathic Scoliosis Trial randomised the skeletally immature child with a 25 to 40 degree curve to the bracing or the observation, and it was stopped early for the efficacy: the bracing raised the rate of the successful treatment — the curve not reaching 50 degrees — to 72 percent, against 48 percent with the observation, with a number needed to treat of 3. The benefit was greatest in the higher-risk curves and the compliant wearers, and the trial settled the long-standing question of whether the bracing altered the natural history. [1] [2]
The Weinstein fifty-year natural history study and the Lancet seminar frame the long-term outcome of the untreated curve, and they are the evidence that calibrates the modern management. The fifty-year follow-up showed that the untreated curve carried the cosmetic and the psychosocial burden and the curve progression, and that the very large thoracic curve might restrict the vital capacity, but that the untreated curve was not the cause of the severe back pain, the cardiopulmonary disease, or the early mortality that was once feared — a finding that places the management in its proportion and that frames the shared decision. The Lonstein and Carlson progression model and the Sanders maturity study frame the prediction of the curve and the timing of the intervention. [3] [5]
The screening is the area of the regional and the evidentiary difference, and the US Preventive Services Task Force 2018 statement is the reference. The Task Force issued an I statement — the evidence is insufficient to assess the balance of the benefits and the harms of the routine screening of the asymptomatic adolescent for the idiopathic scoliosis — citing the uncertainty over the harms of the over-diagnosis, the unnecessary bracing, and the radiation, set against the benefit of the earlier detection. The Scoliosis Research Society and the paediatric bodies recommend the screening, and the ANZ and the UK practice screen at the school and the clinic with the Adams forward bend test and the scoliometer, using the 7-degree angle of trunk rotation as the trigger for the radiograph. The fellowship candidate names the controversy and the local practice. [10] [2]
The SOSORT 2016 guidelines frame the conservative management — the observation, the physiotherapeutic scoliosis-specific exercises, and the bracing — and they are the international reference for the non-operative pathway. The guidelines place the exercises as an adjunct to the observation and the bracing, with the evidence supporting their role in the muscular support and the brace compliance, and they frame the bracing as the primary conservative treatment for the progressive moderate curve. The areas of the remaining controversy — the optimum hours of the brace wear, the role of the part-time bracing, the patient selection for the vertebral body tether, and the long-term outcome of the growth-friendly implants — are the open questions that the modern evidence continues to address. [9] [1]
Exam Pearls
The five facts the examiner rewards are the 10-degree Cobb definition of the scoliosis, the observe-brace-surgery ladder of under 25, 25 to 40, and 45 to 50 degrees or more, the BrAIST 72 versus 48 percent with the number needed to treat of 3, the red-flag screen that separates the idiopathic from the non-idiopathic curve, and the Adams forward bend test with the scoliometer at the 7-degree threshold. A candidate who opens with the definition and the two numbers — the Cobb angle and the maturity — and then runs the red-flag screen before naming the rung of the ladder, has the framework the examiner is listening for. [2] [1]
The three traps the examiner probes are the reassured painful curve, the dismissed left thoracic curve, and the early fusion that sacrifices the lung. The painful scoliosis is not idiopathic until the imaging excludes the cause. The left thoracic curve carries the neural-axis lesion until the magnetic resonance imaging proves otherwise, and the fusion of the young thoracic spine produces the thoracic insufficiency syndrome that the growth-friendly strategy is designed to prevent. The candidate who reaches for the brace before the red-flag screen, or who offers the early fusion to the young child without the growth consideration, has fallen into the trap. [2] [7]
The examiner rewards the candidate who names the maturity before naming the management, because the maturity is the second number and the modifier of every rung. A 35-degree curve in a Risser 0 pre-menarchal girl is braced. The same curve in a Risser 5 mature adolescent is observed, and the candidate who reports the Risser sign or the Sanders scale alongside the Cobb angle, and who explains the peak height velocity as the danger window, has the depth the fellowship viva tests. The Cobb angle is measured from the most-tilted end vertebrae on the standing posteroanterior film, the posteroanterior projection is used to spare the breast, and the progression is the 5-degree change on the reproducible film. [5] [6]
The scoliometer is the bridge between the clinic and the radiograph, and the 7-degree angle of trunk rotation is the threshold that triggers the standing film. The screening is the school and the clinic examination with the Adams forward bend test, the US Preventive Services Task Force issued the I statement on the balance of the benefits and the harms, and the local practice screens with the forward-bend test and the scoliometer. The candidate who knows the threshold, the screening controversy, and the local practice, and who frames the scoliosis as a clinical reasoning exercise with the red-flag screen and the shared decision, has the answer the examiner rewards. [10] [2]
References
- [1]Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med, 2013.PMID 24047455
- [2]Weinstein SL, Dolan LA, Cheng JCY, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet, 2008.PMID 18456103
- [3]Weinstein SL, Dolan LA, Spratt KF, Peterson KK, Spoonamore MJ, Ponseti IV. Health and function of patients with untreated idiopathic scoliosis: a 50-year natural history. JAMA, 2003.PMID 12578488
- [4]Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am, 2001.PMID 11507125
- [5]Lonstein JE, Carlson JM. The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am, 1984.PMID 6480635
- [6]Sanders JO, Browne RH, McConnell SJ, Margraf SA, Cooney TE, Finegold DN. Maturity assessment and curve progression in girls with idiopathic scoliosis. J Bone Joint Surg Am, 2007.PMID 17200312
- [7]Karol LA, Johnston C, Mladenov K, Schochet P, Walters P, Browne RH. Pulmonary function following early thoracic fusion in non-neuromuscular scoliosis. J Bone Joint Surg Am, 2008.PMID 18519321
- [8]Parent S, Newton PO, Wenger DR. Adolescent idiopathic scoliosis: etiology, anatomy, natural history, and bracing. Instr Course Lect, 2005.PMID 15948477
- [9]Negrini S, Donzelli S, Aulisa AG, et al. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord, 2018.PMID 29435499
- [10]US Preventive Services Task Force. Screening for adolescent idiopathic scolatitis: US Preventive Services Task Force recommendation statement. JAMA, 2018.PMID 29318284
- [11]Williams BA, Matsumoto H, McCalla DJ, et al. Development and initial validation of the Classification of Early-Onset Scoliosis (C-EOS). J Bone Joint Surg Am, 2014.PMID 25143496
- [12]McMaster MJ. Prognosis for congenital scoliosis due to a unilateral failure of vertebral segmentation. J Bone Joint Surg Am, 2013.PMID 23780534